#lung transplant procedure
Text
#Lung Transplant in Chennai#Lung Transplant Program#heart-lung transplantation#Lung Transplantation#Kauvery Hospitals#Lung Transplant procedure#Transplant Pulmonologist#Transplant Surgeons#Types of Lung Transplant
0 notes
Text

The pre-transplant assessment before a lung transplant employs a collaborative approach involving a range of healthcare professionals. It consists of the following key elements:
1. Medical Evaluation:
• Pulmonary Function Analysis: Spirometry and diffusion capacity tests provide critical insights into lung disease severity, assisting clinicians in determining transplant eligibility.
• Radiological Examination: Chest X-rays and CT scans generate detailed lung images, aiding surgical planning and patient suitability assessment.
• Cardiac Assessment: Given the heart-lung connection, cardiac function evaluation is essential, often involving stress tests or echocardiograms.
• Laboratory Assessments: Comprehensive blood tests detect infections, assess liver and kidney function, and provide a holistic health overview, identifying underlying issues needing management pre-transplant.
2. Psychological Appraisal:
• Mental Health Evaluation: Psychologists conduct a thorough analysis of mental and emotional well-being, seeking signs of anxiety, depression, or other concerns, and providing coping strategies.
• Social Support Review: The patient's support system is examined to ensure a robust network of family and friends for emotional and practical support during lung transplantation.
3. Screening for Infectious Diseases:
• Rigorous Infectious Disease Tests: Patients undergo screening for infections such as HIV, hepatitis, and tuberculosis. Active infections are treated pre-transplant to reduce surgical complications.
4. Nutritional Assessment:
• Evaluation of Nutritional Status: A comprehensive assessment determines the patient's nutritional status, addressing malnutrition through dietary recommendations.
5. Assessment of Substance Use:
• Screening for Substance Abuse: Patients are evaluated for alcohol or drug abuse, which could interfere with post-transplant recovery and medication adherence.
6. Financial and Insurance Review:
• Financial Evaluation: Given the financial demands of a lung transplant procedure, patients must have a clear plan, including an assessment of insurance coverage and available resources to cover procedure and post-transplant care costs.
7. Education and Counseling:
• Patient Education: Patients and families receive thorough education about the lung transplant surgery, potential risks, and post-transplant care, enabling informed decisions.
• Counseling Support: Counseling services help patients address emotional challenges associated with transplantation, offering a safe space for fears and anxieties.
Some of the best hospitals in Delhi, such as Indraprastha Apollo Hospitals, offers pre-transplant testing followed by a successful lung transplant procedure, and post-transplant care to the patient. The cost of lung transplant in Delhi will include the cost of the diagnostic tests performed before the procedure.
#lung transplant#lung transplant procedure#lung transplant surgery#lung transplantation#lung diseases#lung failure#cost of lung transplant
0 notes
Text
reading about sergei brukhonenko and vladimir demikhov today and we are just 😭😭😭😭
#[ u know the heart-lung machine that’s used during heart bypass surgery to keep the heart alive and pumping outside the body?#these two russian surgeons were the forefathers of this technology that has saved countless lives over the years all around the world#they made many medical contributions to open heart procedures and organ transplants#but did u know how they discovered/tested out their invention?#they connected the lungs of one dog to the heart of another dog with their machine#...and then kept the decapitated head of the second dog alive for THREE hours#thus proving that the technology works#the dog head was neurologically patent and could respond to stimuli#blink its eyes and twitch and curl its lips like normal up until its heart finally gave out#😭😭😭😭#then demikhov went on to use this invention to perform transplants...such as attaching a puppy’s head to another dog#- making living functional cerberuses with multiple heads 😭😭😭😭#kinda have complicated feelings when I look at a heart-lung machine now ngl ]#[ brb need to go hug and coddle my doggo all night now ]#;;Oυт σƒ Jαzz#;;tbd
6 notes
·
View notes
Text
#Lung Transplant Surgery Cost in India#Lung Transplant in India#Lung Transplant Cost in India#Lung Transplant in India Procedure & Cost#How Much Does Lung Transplant Cost In India#Best lung transplant in India
0 notes
Text
So Large Bastard went into the hospital for transplant evaluation on February 13th 2021 and that was one of the major peaks of covid and basically we dropped him off at the hospital and that was it; nobody was allowed to visit him or see him and they pretty much immediately implanted a pump in his shoulder that made it painful and difficult for him to use the phone. At that point the message we were getting was "either he'll qualify for a transplant and you'll see him again when he is released after the transplant (and the waitlist, and the surgery, and the recovery) or we'll allow you to visit him when he's dying OR he won't qualify for transplant and we'll provide his end of life care and we'll allow you to visit him when he's dying" and on like February 16th, before we knew if he'd qualify for a transplant, I got a call from the hospital saying they were putting him on a heart/lung bypass machine because the pump they'd implanted in his shoulder and the pump they'd implanted in his heart weren't doing enough (both are designed to pump blood through about six feet of human, not through about seven feet of human, so they needed a much larger external pump). They asked me if I approved this procedure because he was kind of out of it, and held the phone up to him so I could ask him if he wanted this and say goodbye - I didn't know if that was goodbye until he got woken up by the doctors after stabilizing, or goodbye until he got approved for a transplant, or goodbye until he didn't get approved for a transplant and they'd take him off the machine to say goodbye for real if they couldn't keep him alive any longer.
And then they hung up the phone and I sat at my desk and stared at my computer and went back to work because literally what the hell else could I do? I couldn't drive to the hospital, I couldn't anxiously wait to see if the doctor would come out and tell me the machine had stabilized him. They said they'd call me in three hours with an update. So I took some orders and placed some calls and responded very politely to emails until I got off the clock at 5:30.
I had texted one of Large Bastard's friends who I'd been calling a lot and asked if we could meet up so I could explain what was going on so he could pass that info on to their radio nerd club. We were meeting up in the parking lot of an ihop because it was an easy outdoor location to describe to him when I wasn't actually capable of processing things like "addresses" or "street names" and I drove over to the ihop and at the red light for the left turn to go into the parking lot I fucking lost it. Like. I don't do the "hysterical crying" thing often but when I do, boy do I. I was in my truck with the windows rolled up and music on and I was sobbing so hard that it shook the truck and the crying was audible from outside the car.
I know it was audible from outside the car because a homeless man came up to my window and knocked and when I rolled the window down he told me "you're okay girl, you got this, it's gonna be alright" and I kind of nodded at him and sobbed at him and waved at him as he kept crossing the street and my light changed and I turned into the parking lot.
By the time my friend got there I had calmed down and stopped crying and through the entire rest of the process I never lost it in quite the same way; they took Large Bastard off the lung bypass part of the machine a day later and he was awake when they approved him for the transplant list, and a few days after that they started allowing a single, masked, socially distanced family member to start visiting patients in the transplant ICU for two hours a day, so I was able to come see him and he immediately said "look I have abs" and pulled his gown aside to show me that he'd lost so much weight as his body tried to eat itself to stay alive that he did, in fact, have an eight pack. And we laughed about it. It was uphill from there. It was never as hard for me as it was in the few hours after that phone call.
And in those few hours there was one dude who happened to be walking by who was kind enough to try to offer comfort to a complete stranger and I think about him all the time.
1K notes
·
View notes
Text
Jackson Avery x reader - together again

Can I request jackson avery x reader where they were childhood besties but went their separate ways when reader went to the military and they reunite during the merger? - Anon💜
Pulling on your scrubs, you rolled your shoulders and walked into the hallway and over to the surgery board.
“Looks like you’re pretty booked up.”
Looking over at Owen, you nodded your head.
“Yeah, think I could have one of your residents or interns for the day? Just an extra pair of hands to prep and such.”
“Not a problem, I’ll send someone to meet you at your first patients room.”
“Thanks.”
You walked to get some coffee before making your way over to the nurses station.
Sitting down, you looked through your patient files before you finally got up and made your way to the first patients room.
Inside was one of the interns and you handed him the file.
“Have you read up on the procedure?”
“Yeah, it’s a transplant, right?”
“I don’t know, is it?”
Turning to face the intern you crossed your arms across your chest and rose a brow at him.
He offered you a little smile.
“Sorry. Yes, it’s a lung transplant.”
“Yes, I’ll be having you help me today doctor?”
“Avery. Jackson Avery.”
You nodded your head and turned around to check your patient as you thought about that name.
You’d heard it somewhere, not the last name.
Of course everyone knew the name Avery. But his whole name? It rung a bell and you weren’t sure why.
“Doctor (L/N)?”
You looked towards the door at one of the other interns.
“We need your help.”
“Avery prep him.”
Jogging over the intern, you quickly helped them with their issue before you made your way to the operating room.
The whole day was tiring, and by the end you were nearly falling asleep in the hallway.
“Hey, maybe a coffee will help.”
You looked at Jackson and gave him a small smile and a nod thanks.
“Two sugars, just how you like it.” He smiled.
“How’d you know?”
“You don’t remember?”
You sat up a little and looked at him properly.
“Oh my god…”
He smiled and you laughed, reaching over to hug him lightly.
“Jackson im so sorry. It’s been so long!”
“It’s no problem, I know it has but I’m glad to know you’re safe.”
You pulled away as stood up, grabbing the coffee he handed you and gestured to the doors.
“How about some food and a catch up?”
“I’d like that.” He smiled.
It really had been years since you saw your best friend.
The moment you were old enough you left for the military while he decided to become a doctor.
Sometimes he wondered where he went in life, if he’d made it and where he decided to settle and work towards his goal.
Glancing at the man who was walking beside you, you couldn’t help but smile.
You missed him.
He was everything to you, all you’d ever known throughout your whole life. You grew up with him, now you were reunited with your best friend.
Sure, the pair of you had been apart for so long, but you were always inseparable
#greys anatomy x you#greys anatomy x reader#greys anatomy#greys anatomy imagine#Jackson Avery#Jackson Avery x reader#Jackson Avery x you#Jackson Avery imagine
557 notes
·
View notes
Text
I have absolutely nothing poetic to say and I am finally angry for the first time in 17 days that this is happening to me and I don’t know how to express how I feel like I am just fucking screaming inside to crawl out of my skin.
It’s so fucking unfair. I am fighting so hard to stay positive, to uplift other people, to comfort my loved ones about the very real fact that I am dying. And there’s nothing I can do, but take the pain everyday with a smile on my face and try to advocate for positivity to help your body heal and right now it just feels like fucking bullshit. I don’t want to be positive, I want to cry and punch walls and I don’t know how to keep saying to people that love me to please stop touching me and treating me like I’m a walking time bomb. The fact is, I am. I am shoving every feeling down except for this idiotic, “I’m smiling and laughing through the pain and all of this will be worth it when I am alive so there is no point being pissed off or talk about how god damn fucking unfair this is”.
I don’t god damn deserve having to be a “protected patient” while I am actively dying because my Mom decided to go off her fucking rocker and straight up abuse me. I should not be fighting to protect myself tooth and nail against her. I should be able to lean on my only parent and instead I have to safe guard myself to such extreme measures that I have to be a fucking Jane Doe so she stops sending people for me because I will not surrender control of my life to her. I would rather die. I have spent my entire life in the hands of self victimizing sociopaths and in the most vulnerable time, an absolutely inexpressible terrifying time, and I am forced to surrender my pride to let my family take care of me while I rail against letting anything else be taken away from me.
I am losing so much, it is so hard to even imagine life after this nor fathom what it will take to come back if I survive at all. I do not deserve to live disabled for what is left of my life. I do not know if I have it in me to go through procedure after procedure to be cut in half and have more pieces taken from me. I’m scared. I could die on the table and I very well might. My surgery is far more complex than a normal transplant. My recovery period is expected to be twice as long. I am scared. I will be on a ventilator and intubated for weeks. I will lose all autonomy and have to lean completely on my best friend and siblings. Leading up to my surgery, my medical team has to push me to the brink of death to move me up the transplant list. There is no guarantee I will even make it to the surgery once they have pushed my body far enough, I very well might have a heart attack and die before I can make it to the OR. If I live, I am disabled forever and on oxygen. I am no longer independent. I am so fucking afraid and it is so fucking unfair.
How the fuck do you talk to a 30 year old about their end of life directive? How am I supposed to just act like I am strong when I’ve had to take legal action against my only parent and I am making the scariest choices of my life knowing I am completely dependent on my best friend? How can people be so god damn selfish and destructive that they force a dying person who is drowning to fight a battle to prioritize their healing? I lay here in bed shaking because my blood pressure is so low, I am so anxious from trying to crack open my feelings about my fear of death and what is to come, and everything seems so fucking trivial.
No amount of sedatives is touching this. No amount of anxiety meds. No amount of writing, of coloring, of reading. I cannot stop shaking my feet and moving my legs or I think I will sink through the floor of the hospital or just take off running for the hills straight through the walls and run until my lungs give out and that way I can control how I die. Just as I’m writing this, I had phlebotomy come and order more vials of blood. I knew I didn’t feel well tonight. I knew my labs from the evening were going to be weird. I am scared because I was hoping I was wrong.
It just baffles me that at home there are people that call me family or claim they love me, but are home in their little worlds thinking about the little things that they want to believe about me to offer them solace. There is almost something amusing about it, not in a way that is meant to be dismissive of other feelings, but how small it is.
She’ll miss me one day and see that I was not broken the way I was, and that she missed out on loving someone because she only loved the image she wanted to preserve. She will see that the reason she has no one, is because others see the sadism and manipulation. How small I have always been. That there is a reason every person except one is rallying behind me telling her that she is helping kill me.
I don’t really care too much what the “he’s” think. I was not perfect by any means, but I was good and I loved hard and genuinely, despite my mistakes. I forgave, even when I was not forgiven for my mistakes and I was crucified for less. I rose above. Most of all, I loved and I know I gave and gave until I could not. I have no regrets, except for wishing I saw my worth before my life became something I could no longer recognize. These things seem so small now, it is hard to even place myself in their shoes anymore.
Those who only cared to weaponize my illness, who used my vulnerability to their own means to stroke their egos, the friends that did not show up. It is no real loss. The only loss again is that I wish I loved myself before I started losing my chance. I do not recognize the person in the mirror and if I live, I still will be a stranger. These people do not know me, and will not know me after this. I hope you do not come to my funeral.
I do not really know what is happening anymore.
I am the furthest thing from alone, and the loved ones that have stepped forward have moved me immeasurably about the purity of human nature. It is difficult to feel loss about the people I loved who left me or wounded me.
I hope I am missed. I hope people remember my laugh. I hope that those who have watched me dying the last two weeks in front of their eyes remember me walking in the wake of the shore in the sunshine. I hope no one forgets that I could lift a keg my size and that my biggest fears are grasshoppers and werewolves but I will walk straight into gunfire for someone I love. I hope someone loves my animals and don’t let them forget that I loved them more than anything. I hope people remember me for me, that I loved peaches and listening to soft piano, that I always made too big of pasta dishes and gave them all away. I hope they remember how fiercely I protected the people I love. I hope I see my Dad.
I’m not even going to edit this.
#personal#death tw#illness cw#terminally ill#liver transplant#spilled ink#words#spilled thoughts#prose
10 notes
·
View notes
Text
steddie ‘consumption as love’ blurb
tags: blood, guts, surgery, death, organ harvesting/transplant, graphic descriptions of violence, just generally grey’s anatomy type shit if they were really weird, very graphic
gang this one is real fucked up i BEG of you to proceed with caution. READ THE TAGS!!!
eddie would start out asking steve for a vial of his blood to wear around his neck. it’s certainly not the craziest thing he could ask, and by no means goes anywhere near the depths of his desires. these bone-deep, animalistic desires that threaten to overtake him every time he’s around him.
it’d start off with a vial of blood.
steve would reluctantly agree, if only because his boyfriend is weird as fuck and like, what’s the harm? they’ve all seen enough of each other’s insides, lord knows steve’s overdue for a blood test anyways. may as well, right?
it starts off that way.
in the end, steve’s decrepit body lay cold and pale in the bed they used to share.
he’s breathing, barely, his lungs rattling with the effort. messy stitches stretch across his abdomen like song lyrics scrawled in eddie’s journal. the handiwork is uneven, done by amateur fingers.
eddie’s tongue pokes out in concentration as he drags the knife across steve’s stomach. careful not to break the scars that have so tediously worked themselves into closure, his hand barely shakes this time around.
it takes a long time. harvesting organs is excruciatingly difficult, especially for someone with no formal training.
but he gets it.
after hours or days, steve’s raspy breathing only interrupted by weak moans, eddie’s hands wrap tenderly around one of the last viable organs in his body. he grips it carefully, fingers digging into the soft tissue.
eddie carries it over to a metal tin, laying on a bed of ice. he places it inside and makes his way back to his boyfriend.
he picks up the needle, a line of thread, and lovingly, painstakingly, stitches his lover back together.
the line is straighter this time, and he pats himself on the back. thinks steve will be quite proud of this one.
but steve’s long since stopped breathing. eddie doesn’t know when the rattling turned into gasping, when he started imagining it instead.
but he’s not worried about that right now.
right now, he’s laying down on the bed next to steve.
he’s bringing the tray over and placing it next to him.
he’s grabbing a scalpel, the same one he used on steve, and he’s gritting his teeth as he drags a red line across his own abdomen.
he’s looking past the dizziness, gasping against the pain, as he repeats the procedure on himself.
he’s careful not to drop his own organ as he takes it out and places it in the empty tin next to him, tinged red with steve’s blood.
he’s taking steve’s organ, he’s placing it into the cavity of his own abdomen.
he’s relishing in the feeling of his boyfriend’s blood beating beside his own. of the relentless ebb and flow of their shared vitality.
he doesn’t bother sewing himself back up. he simply holds steve’s hand, lets his, their blood bond their skin, and closes his eyes.
he joins steve in the afterlife with mismatched organs and hearts that beat in tandem.
#steddie#stranger things#eddie munson#steve harrington#steddie fanfic#steddie fic#steve x eddie#consumption as love#gore#its a LOT OF GORE#blood#guts#organ harvesting#organ transplant#this one is really fucked up please god proceed with caution#READ THE TAGS#eddie harvesting steves organs to put inside himself idk whAt to tell you
8 notes
·
View notes
Text
Still trying to process what my family is going through. Last Sunday my parents and I drove 2 hours away to visit my uncle, my moms brother, in the hospital because his lungs were failing. He was on oxygen but doing better than I thought. He had been in the hospital for 2-3 weeks already because he could no longer be supported by his oxygen at home. He had also been awaiting a lung transplant. Well Tuesday night we got the call that they had found lungs for him. Wednesday evening my mom and I drove 2 hours back to the hospital to be there for my uncle and support my aunt. He went into surgery around 2:30 in the afternoon and had been under for about 4 hours by the time we arrived. His surgery lasted about 9 hours, finishing around 11:30. His double lung transplant was a success. Doctors said he was in the best health possible for the procedure, and it couldn’t have come at a better time because his lungs were failing that very day. My mom and I slept a few hours in the car but got up around 5:30. We went to see my uncle in the ICU and he tried to communicate by writing on a notebook though still under sedation, he was only concerned his wife hadn’t been able to leave, and told her she should go home. My mom and I left first and my aunt left after updating us that my uncle stood up by himself. She returned to stay at the hospital the next day and then received news a residence was provided for her and family. His breathing tube was removed within a couple days and he was placed on oxygen again, now he’s just trying to learn how to use his new lungs. Still waiting to hear if he’s been moved to a regular hospital room, as he will be there for another month or so. We hope to go up to visit again soon, but first we must get through our work obligations before we can makes plans again. Of course if anything changes we will be on our way there in a snap.
June 2023
8 notes
·
View notes
Text
Medical student plays Digimon Survive: thoughts on Saki
I have an educated guess about Saki and...(spoilers below the cut!)
...her illness. The game never explicitly stated what it is, but with my medical background I can't help but think it over and take a stab at it.
My thesis statement? I think that Saki has cystic fibrosis.
Let's look at evidence from the game:

-she has an “awful cough"
Cystic fibrosis is a chronic disease involving abnormally large, constant buildup of mucus in the pulmonary and digestive systems. From what little the game shows us, her problems (visible problems, at least) seem primarily respiratory in nature. Floramon's comment on Saki's cough can be taken to mean a wet, productive cough, productive meaning "sputum production" in medical speak or in layman's terms, hacking up gunk from the lungs. The presence of a cough made me rule out leukemia. According to Saki's flashback, she is currently in a stable period so the doctor believes it's a good time for surgery. Leukemia is what came to my mind when I tried to think of diseases in distinct phases. I was thinking especially of acute lymphocytic leukemia, or childhood leukemia. Bone marrow transplant is an option for surgical treatment. It seemed to line up except there's the deal with Saki's bad cough. While shortness of breath is associated with leukemia, cough typically isn't. I have other reasons to rule out cancer, which I'll elaborate on later.
-she’s had it since she was little
Cystic fibrosis is a genetically inherited disorder (autosomal recessive, if you want the precise genetics terminology). Symptoms can manifest as soon as the moment of birth, sometimes it doesn't show up until adulthood. I think Saki has the early onset type.
-she gets fatigued easily
Yeah a ton of conditions entail this, but it doesn't detract from the case for cystic fibrosis. If your lungs are plugged up with gunk, you can't breathe right to meet your body's oxygen demands, and you'll tire out sooner than most people. Throughout the game, Saki has to pause and catch her breath, and has a hard time keeping up with everyone else. Far from precise evidence because again, you can say this for pretty much every kind of medical condition under the sun.
-she carries herself like someone on borrowed time
Saki knows that she doesn't have long, that she could be here today and gone tomorrow. She signed up for camp on a whim, trying to live her life to the fullest, however short it may likely be. Her disease was described by the doctor to be frightening. Saki herself says that it progresses quickly and the moment it worsens, it would eat her up someday. This leads me to think that whatever she has must be fatally progressive, with no hope for a cure. Something like cystic fibrosis. I ruled out asthma, which also involves respiratory issues but is not fatally progressive and incurable like cystic fibrosis. The lifespan of people with cystic fibrosis is a lot shorter than people without. Typical age range of life expectancy these days is 40s-50s, though a few have lived up to their 70s. In a nation like Japan where lifespan is above average, living to your 40s is basically only half your life. A scary thought for anyone, but especially for a 12 year-old girl.
-she needs surgical treatment
While cystic fibrosis isn't curable, symptoms can be managed with medications like antibiotics to ward off lung infections, bronchodilators to open up the lungs, and stool softeners for bowel issues, though problems can worsen to a point where surgery is necessary. Most common procedures involve treating inflamed sinuses and nasal polyps. Abdominal surgery is also an option for those having bowel issues. Lung transplant is like last resort for the most severe cases; of all the types of transplants, lung transplant is the most difficult to perform and with the lowest success rate. (Most people assume that heart transplant is the hardest to pull off, but actually it's the lungs because they're very prone to infection and rejection. I've helped manage anesthesia for both types of cases, and lung is a lot more involved. But I digress.) If Saki's at the point that the doctors are suggesting surgery for treatment, she's probably at the cusp of an advanced stage of the disease. Another reason I ruled out asthma is that asthma itself doesn't warrant surgery. I also ruled out cancer, because someone needing a tumor resection most likely wouldn't be allowed to postpone surgery and run off to camp. Someone getting chemotherapy for cancer will be immunocompromised, susceptible to serious illness from the slightest hint of potential for infection from radiation nuking their immune system. Saki is delicate, but not that delicate. The surgery is urgent, but apparently not that urgent if she can convince the doctor to postpone it a few times.
Getting into "that's a stretch" headcanon territory here:
Digimon Survive seems to be set in a world where people have realistic hair color. No one in the main cast has anime-colored hair, only black and shades of brown typical among Japanese people. The "wildest" we see is Kaito with his hair partly bleached. Saki stands out for being the only one among the kids with what looks like natural blonde hair (unlike Kaito). This reminds me of Yamato and Takeru having blonde hair, of how they have French descent from their grandfather, and that the blonde hair may be a nod to their background. So here's the thing: according to statistics, cystic fibrosis happens most commonly in people with northern European ancestry. Perhaps not a stretch to suggest that Saki might have some northern European blood, which lines up neatly with the idea that she has cystic fibrosis.

P.S on patient consent: I think it's interesting how it's implied that a 12 year-old girl like Saki is able to express her own consent for surgery. I train in and will someday practice pediatric anesthesia in the U.S, where minors under the age of 18 must have the consent of a parent or guardian for any procedure. (There are exceptions, like emancipated minors, which Saki is not because it's implied that she has parents who still have legal responsibility of her.) Maybe consent works differently in Japan. I dunno.
So there you have it. Do you agree, or do you think Saki's got some other medical condition? I'd like to hear your thoughts. Honestly, the game has kept it vague enough that there could be more than one right answer, or something made up entirely, for all we know. I just thought it'd be fun to offer my own interpretation of what it might be.
#digimon survive#digimon survive spoilers#saki kimishima#digimon theory#thanks for coming to my ted talk#it’s kind of my hobby to figure out what vaguely deliberately unnamed illnesses a fictional character is said to have
31 notes
·
View notes
Text
Starmania d'hier à aujourd'hui - Wodrascka

Just finished this book! I found it... not good! lol Basically mostly gossip about who liked/didn't like whom, a compilation of interviews and fan site pages, and suuuuuper dated language about LGBT themes even though the book was only written in 2018.
But a few interesting facts & tidbits that I didn't know/didn't remember:
Michel Berger's father was a pioneer of kidney transplants and dialysis and would see international stars like Rita Hayworth at his home office (before becoming partially amnesiac after a lung procedure he insisted on staying conscious for (??) and leaving his family behind as a result)
His mother was a concert pianist and the family's home had two grand pianos facing each other in the living room
Between his pop tunes and Starmania, Berger composed a conceptual piano/symphony/rock instrumental album called "Puzzle" (1971)
He lived in the USA for a bit and met/hung out with Ira Gerschwin (George's brother)
Everyone in the original Starmania troupe seems to have 1) admired France Gall's talent and 2) HATED HER lol
She says she was deathly afraid of singing "Monopolis" every night because the song wasn't written for her vocal range and she thought she wouldn't make it
Diane Dufresne told Balavoine that "French people can't sing" and he was devastated
She seems to have hated her role? Apparently she thought or had been told Stella would be the main character, but then they kept cutting the part (she says she "fished the Adieux d'un Sex Symbole" out of the trash can), maybe because Berger thought it was too outrageous. She refused to go on tour after the 79 Paris run, which might have killed it (when 30k tickets had been sold in France and Québec)
Tom O'Horgan wanted everyone to be naked during the "Procession du Gourou" bit which signified an orgy, but only 3 members of the troupe agreed and they ended up wearing little togas instead (except of course Diane Dufresne who was topless.)
[More under the cut]
The 1979 show's original stage was set at an incline, and opened up in the middle to reveal a 2-meter/6.5-foot deep pit which was the Underground Café -- and sometimes people fell into the pit.
It also made use of early laser technology, and the cast had to be careful not to be in the path of the beams because it would give you radiation.
Tom O'Horgan showed up in Paris with his full crew of stage techs and none of them spoke French. Berger & Gall had hired a very prim & proper translator who would very reluctantly translate the waves of insults he would shoot at the troupe, which he found unprofessional and bad.
If you believe Fabienne Thibault, she single-handedly cast all of Starmania and then saved it multiple times lol
President François Mittérand was a fan of the 88 version (which I knew) but comedian Coluche was too; he was petitioning Berger to have Johnny Hallyday record a version of "Stone." (Hallyday was going to be Johnny Rockfort in the original production but then Berger & Gall found Balavoine instead.)
Maurane famously left the 88 production in the lurch; she said she would only sign one-month contracts and renew them at the end of each month, but once she decided not to sign again she just stopped showing up instead of finishing her contract. Réjane Perry, who had never seen the show, was told she would have 3 weeks to learn the role and ended up having 2 days. She says she did her first show without rehearsing any of the duets or ensemble moments with the rest of the cast.
In 1988, Wenta as Sadia put out a cigarette into her hand during her jealousy fit over Johnny/Cristal; she had a thick band-aid in the palm of her hand to act as a protection but one night she missed it & burnt herself instead. She says she kept going and waited to be in her dressing room to scream "like a Tex Avery cartoon."
Fabienne Thibault says she hated the Lewis Furey version so much she was in tears by the end, and that it lacked vocal diversity: "On tombe dans l'uniformité canadienne, avec ces voix issues de la culture nord-américaine qui, à mon avis, distillent très peu d'émotion." "You end up with Canadian uniformity, with voices coming from that North-American tradition which, in my opinion, produce very little emotion." Tell us what you really think, Fabienne!
France Gall didn't authorize the Québecois lyrical versions of the show, which is why there's no official recording of them. Apparently she sicced her lawyers on Plamondon because of it.
The book ends with Plamondon talking about his new project, a 40-year anniversary revival which would be a "blockbuster" -- our 2022 production! :)
Onto my next book, which I think is Fabienne Thibault's own one and probably will tell me many more of her petty feelings towards France Gall lol
#starmania canon#starmania 1979#book#meta#in the press#comédie musicale#musical theatre#rock opera#france gall#diane dufresne#daniel balavoine#starmania 1988#starmania 1993#fabienne thibeault
14 notes
·
View notes
Text
#lung transplant surgery cost in india#Lung Transplant Surgery in india#Lung Transplant in India#Lung Transplant in India Procedure & Cost#How Much Does Lung Transplant Cost In India#Lung Transplant Cost in India
0 notes
Text
Patient is a [ ] yo male/female presenting to the clinic for a preoperative evaluation.
Procedure [ ]
Scheduled date of procedure [ ]
Surgeon performing procedure requesting consultation for preop is [ ] and can be contacted at [ ]
This patient is/is not medically optimized for the planned surgery, see below for details.
EKG collected in office, interpreted personally and under the direct supervision of attending physician as follows- sinus rate and rhythm, no evidence of ischemia or ST abnormalities, no blocks, normal QTc interval.
The following labs are to be completed prior to surgery, and will be evaluated upon completion. Procedure is to be performed as scheduled barring any extraordinary laboratory derangements of concern.
Current medication list has been thoroughly reviewed and should not interfere with surgery as written.
Patient has no prior history of adverse reactions to anesthesia, problems with airway management, difficult IV access, prolonged emergence, or postoperative nausea/vomiting.
Airway Mallampati score: This patient is a Grade based on the criteria listed below
-Grade I Tonsillar pillars, soft palate, entire uvula
-Grade II Tonsillar pillars, soft palate, part of uvula
-Grade III Soft palate, base of uvula
-Grade IV Hard palate only, no uvula visualized
Patient is a low/medium/high risk for this low/medium/high risk surgical procedure.
Will send documentation of this preoperative visit to surgeon [ ].
**** ADDITIONAL INFORMATION****
Patient Risk for Elective Surgical Procedure as Determined with the Criteria Below:
1- Very Low Risk
No known medical problems
2- Low Risk
Hypertension
Hyperlipidemia
Asthma
Other chronic, stable medical condition without significant functional impairment
3- Intermediate Risk
Age 70 or older
Non-insulin dependent diabetes
History of treated, stable CAD
Morbid obesity (BMI > 30)
Anemia (hemoglobin < 10)
Mild renal insufficiency
4- High Risk
-Chronic CHF
-Insulin-dependent diabetes mellitus
-Renal insufficiency: creatinine > 2
-Moderate COPD: FEV1 50% to 70%
-Obstructive sleep apnea
-History of stroke or TIA
-Known diagnosis of dementia
-Chronic pain syndrome
5- Very High Risk
-Unstable or severe cardiac disease
-Severe COPD: FEV1 < 50% predicted
-Use of home oxygen
-Pulmonary hypertension
-Severe liver disease
-Severe frailty; physical incapacitation
Surgical Risk Score Determined as Below:
1- Very Low Risk
Procedures that usually require only minimal or moderate sedation and have few physiologic effects
-Eye surgery
-GI endoscopy (without stents)
-Dental procedures
2- Low Risk
Procedures associated with minimal physiologic effect
-Hernia repair
-ENT procedures without planned flap or neck dissection
-Diagnostic cardiac catheterization
-Interventional radiology
-GI endoscopy with stent placement
-Cystoscopy
3- Intermediate Risk
Procedures associated with moderate changes in hemodynamics, risk of blood loss
-Intracranial and spine surgery
-Gynecologic and urologic surgery
-Intra-abdominal surgery without bowel resection
-Intra-thoracic surgery without lung resection
-Cardiac catheterization procedures including electrophysiology studies, ablations, AICD, pacemaker
4- High Risk
Procedures with possible significant effect on hemodynamics, blood loss
-Colorectal surgery with bowel resection
-Kidney transplant
-Major joint replacement (shoulder, knee, and hip)
-Open radical prostatectomy, cystectomy
-Major oncologic general surgery or gynecologic surgery
-Major oncologic head and neck surgery
5- Very High Risk
Procedures with major impact on hemodynamics, fluid shifts, possible major blood loss:
-Aortic surgery
-Cardiac surgery
-Intra-thoracic procedures with lung resection
-Major transplant surgery (heart, lung, liver)
High risk surgery: yes/no
Hx of ischemic heart disease: y/n
Hx of CHF: y/n
Hx of CVA/TIA: y/n
Pre-op tx with insulin: y/n
DM/how are blood sugars?
Pre-op Cr >2mg: y/n
OTHER EVALUATIONS BASED OFF PATIENT HISTORY SEE BELOW:
1. CARDIAC EVALUATION
A. Ischemic Cardiac Risk- Describe any history of cardiovascular disease and list the cardiologist/electrophysiologist. For CAD, report the results of the most recent stress test or cardiac cath, type of procedures or type of stents, date of MI, and recommendations for perioperative management. Include antiplatelet management. Continue baby aspirin for patients with cardiac stents - unless having neurosurgery, then coordinate with surgeon.
B. Ventricular function - include most recent echocardiogram evaluation ideally performed within the past 2 years
C. Valvular heart disease- include most recent echocardiogram, type of prosthetic valve
D. Arrhythmias - include any implanted devices and recent interrogation report, contact electrophysiology about device management during the surgery and include recommendations provided. For A-Fib, include CHA2DS2-VASc score
E. Beta blockade - All patients on chronic beta blockers should have these medications continue throughout the perioperative period unless there is a specifically documented contraindication.
F. Hypertension - Other than for cataract surgery, ACEI inhibitors and ARBs should be held for 24hours prior to surgery and diuretics should be held the morning of surgery
G. Vascular disease - include antiplatelet management and dates of strokes
2. PULMONARY EVALUATION
A. COPD/Asthma - include any recent exacerbations, intubations, chronic O2 use, amount of rescue inhaler use
B. OSA risk - STOPBANG score - address severity of sleep apnea and CPAP use
3. HEMATOLOGIC EVALUATION
A. Bleeding Risk - assess the bleeding risk and history for every patient
B. VTE Prophylaxis/Thrombotic risk - estimate risk and provide recommendations
C. Anticoagulation management - include pre-op and post-op medication instructions
D. Anemia - pre-op treatment plan
D. Oncology - history and treatments
4. ENDOCRINE EVALUATION
A. Diabetes mellitus - include type, medication use, recent A1c, pre-op and post-op management instructions
B. Adrenal insufficiency risk - assess for prolonged steroid use in the last year
5. RENAL EVALUATION
A. CKD - include stage, baseline labs
B. ESRD - include dialysis schedule, type, access, dry weight, location of dialysis. Generally, surgery should not be scheduled on a dialysis day.
C. Electrolyte abnormalities
6. GI EVALUATION
A. Liver disease - including MELD score and Child-Pugh classification
7. OTHER relevant comorbidities or anesthesia considerations
[substance abuse, chronic pain, delirium risk, PONV (post-operative nausea and vomiting) risk, psych disorders, neurologic disorders, infectious disease, etc.]
5 notes
·
View notes
Text
Lung Transplant In India- Procedure, Cost, Advancements All You Need To Know
Overview
Damaged lungs can make it difficult for the body to get the oxygen it needs to function. There are numerous diseases and conditions that either completely destroy the lungs or impair their ability to function properly. In such cases, a lung transplant can improve both longevity and quality of life. However, lung transplant surgery is a complex procedure that necessitates cutting-edge equipment and care. Here we will get to know about the procedure, expected result, lung transplant cost in India, and many more.
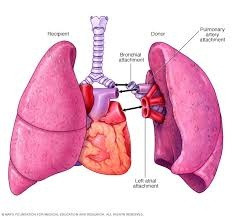
What is a lung transplant?
A lung transplant is a surgical procedure that replaces a patient's diseased lung with a healthy donor lung. When a patient has severe or advanced chronic lung disease, this improves their quality of life and extends their lifespan. A lung transplant can be done on either one or both lungs.
How can we help in the treatment?
If you have been suggested for a lung transplant, we act as your guide throughout your treatment journey and will be present physically with you even before your treatment is started. We will provide you with the following:
Expert physicians and surgeon’s opinions
Transparent communication
Coordinated care
Prior appointment with specialists
Assistance in hospital formalities
24*7 availability
Arrangement for medical travel
Assistance for accommodation and healthy recovery
Assistance in emergencies
We are committed to provide the best health care services to our patients. We have a team of trained and highly dedicated health experts who will be there by your side right from the beginning of your journey.
Conclusion-A lung transplant is a potentially life-saving procedure that can save the lives of patients suffering from fatal diseases. You can get world-class transplant services in India at a low cost without having to worry about safety precautions or the treatment quality.
4 notes
·
View notes
Text
Villain Profile: Iron Lung

The emergence of posthumans in 1951 brought with it a new revolution in biotechnology. Many prominent scientists, psychologists, biologists, physicians and others sought to use these to their fullest potential. One of them was Dr. Julius Leichtenberg.
Born in Hesse in 1937 and later immigrating to the UK, Leichtenberg was an aspiring neurosurgeon who attended the University of Oxford. His biggest influences were American neurosurgeon Robert White and Soviet organ donation pioneer Vladimir Demikhov.
Leichtenberg was fascinated by the idea of head and brain transplants, and believed it was possible to utilize this technology to save lives, whether it was preserving the brain or attaching it to a new body, either natural or artificial. The procedure had yet to be performed on a human and Liechtenberg and others were looking for willing subjects.
However, it was during this search that Leichtenberg, along with several other bystanders, were gravely injured in a fight between a posthuman criminal and police in the streets. The collateral damage left him so badly injured that being rendered quadriplegic was the best case scenario. It was more likely he would not survive.
Already a rather bitter man after facing criticism for his support of brain transplants, Liechtenberg's embitterment turned to spite and he decided to volunteer for his own work. With the help of thoroughly detailed notes and several assistants, he had his brain removed and preserved in solution and attached to a set of artificial sensory relays.
It would've been easy enough for Liechtenberg to simply find a donor body or have one grown for him and move on from there. But, after spending days, weeks and months fixating on his resentment- as well as possible unexpected psychological effects of being an isolated brain- he opted instead to pursue revenge.
The full details of what happened afterward is unclear, but Liechtenberg opted to have his brain preserved in a blast-proof canister and encased in an artificial body, which was then armed with various weapons and means for destruction. Early models were large, clunky and mechanical, which is where he earned his moniker in the press: "Iron Lung."
Iron Lung's primary M.O. is targeting posthumans, particularly those who try to use their abilities to make the world a better place, and either killing them or mutilating them to the point where they can no longer use them. He's shown no qualms about doing the same with other philanthropists, leaders, law enforcement or anyone else who gets in his way.
After numerous skirmishes, he's also gradually adapted his artificial bodies, upgrading them with new and better technology, weapons and equipment. He has now become a large, snake-like figure with a highly flexible body composed of synthetic muscle. He's also learned and employed a great deal of tactical skill, showing both proficiency in combat and the willingness to retreat when overwhelmed.
To date, no one has ever been able to capture him. The most that can be done is to cause him enough harm to force him to retreat and repair himself. With the only vital component of him being his brain, which is always hidden behind several layers of protection, the damage he can take is staggering. Efforts to stop him have gone so far have included RPGs, a Lockheed AH-56 Cheyenne and an FV4201 Chieftain tank.
He also possesses and artificial voice that retains his native accent, and while it sounds disturbingly even throughout (comparable to HAL 9000), the more damage he takes, the more this voice distorts until it devolves into a loud series of electronic whirs and blaring.
Because of the viciousness of his attacks and the nature of his existence, head and brain transplants remain a contentious subject, although a handful have been performed in the years between Iron Lung's emergence.
#the-helixverse#gene warriors#helix earth#oc#original character#my art#villain profile#Iron Lung#brain transplant#alternate history
4 notes
·
View notes
Text
Lung transplant patients can develop lung cancer. While the risk is relatively low compared to other complications, it is higher in lung transplant recipients than in the general population. Several factors contribute to this increased risk, including:
Immunosuppressive Medications: Transplant recipients must take medications to suppress their immune system to prevent organ rejection. These medications can reduce the body's ability to detect and fight cancer cells.
Chronic Inflammation: Lung transplant recipients often experience chronic inflammation in their transplanted lungs, which can contribute to the development of cancer over time.
Prior Lung Conditions: Many individuals who receive lung transplants have pre-existing lung conditions, which may already increase their risk of lung cancer.
Regular medical check-ups and cancer screenings are essential for lung transplant recipients to detect any potential cancer at an early, treatable stage. Monitoring for signs and symptoms of lung cancer and adhering to a doctor for cancer screening can help manage this risk.
What are the different types of lung infections?
There are various types of lung infections, which can affect different parts of the respiratory system. Some common lung infections include:
Pneumonia: This is an infection that inflames the air sacs in one or both lungs. It can be caused by bacteria, viruses, or fungi.
Bronchitis: Bronchitis is an inflammation of the bronchial tubes, often caused by viruses. Chronic bronchitis can be associated with smoking.
Tuberculosis (TB): TB is a bacterial infection caused by Mycobacterium tuberculosis that primarily affects the lungs but can also affect other parts of the body.
Influenza (Flu): Influenza is a viral respiratory infection that can cause fever, cough, and other respiratory symptoms.
Bronchiolitis: This is usually a viral infection that affects the small airways (bronchioles) in the lungs, often seen in infants and young children.
Lung Abscess: A lung abscess is a collection of pus within the lung tissue, usually caused by bacterial infection.
Pertussis (Whooping Cough): Pertussis is a highly contagious bacterial infection that can lead to severe coughing fits and affects the respiratory system.
Fungal Lung Infections: These can be caused by various types of fungi and can range from mild to severe, often affecting people with weakened immune systems.
Cystic Fibrosis Lung Infections: People with cystic fibrosis are prone to recurring lung infections due to thick and sticky mucus in the airways.
Aspergillosis: This is a fungal infection that can affect the lungs, particularly in individuals with weakened immune systems.
Consultation at the best hospitals like Indraprastha Apollo Hospitals, including oncologists and surgeons, is essential for personalised treatment recommendations. One must consult here to know more about lung cancer treatment, procedure of lung cancer treatment, cost of lung cancer treatment in Delhi.
#health#lung cancer treatment#lung cancer surgery#lung cancer#cancer surgery#surgery#cancer treatment#chemotherapy#radiation therapy
2 notes
·
View notes
Last Seen Blogs

juancorral
Chester's ONE

official-rawboss
Official Blog of Rawboss

lemni0scate
Domesticated abyss

nebula-remnants
NebulaRemnants

pokeretiwe
Untitled