#the world is at accurately diagnosing and understanding neurodivergent conditions
Note
lil bit of a question based on one of ur replies to that ask, you don't have to answer! - do you think hypothetically speaking a person on the spectrum would be allowed to become an idol? to be clear I'm not saying that's what she is specifically, I could never tell if she or really anyone show clear signs of that, but just in general. I feel like they wouldn't? Or maybe it'd depend on the severity?
For starters, I think there are already idols with undiagnosed/unpublicised autism in the industry. Also I don't believe in autism severity - it alienates those classed with severe from the rest of autistic society, and puts those who would be classed as mild in a class above the rest, as well as minimizing their struggles by calling it mild.
But this kind of poses a really interesting question on the nature of autism, which I think will become more and more relevant as the Covid Kids grow up - Will a lack of healthy social development during childhood be incorrectly conflated with autism? What impact might this have on society, and how will it shape conversations and attitudes towards autism? There are many studies which suggests this causes development issues, but impairments aren't the same as neurodivergencies. Having worked with a lot of kids with special educational needs, I learnt the difference between overdiagnosis of boys with autism (who really were boys with CPTSD/boundary issues), and underdiagnosis of girls (who are notoriously brushed off as quirky and not disordered and only get their struggles acknowledged in adlthood after masking for years), and this is reflected in adulthood too with how many autistic women are incorrectly diagnosed with BPD and not autism, and not enough men are correctly diagnosed with BPD. This alone shows how misunderstood autism is by the people who are supposed to diagnose it. I guess by saying this, I also mean the idol trainee system can inadvertently create symptoms in trainees which mimick autism - and it might genuinely be impossible to differentiate between the impact of this... unique *twitches* upbringing of a trainee, and an autistic trainee.
As many people allege, neurodivergency is often considered a spectrum and even if someone has symptoms, it might not necessarily warrant a diagnosis, or even if it did, they might not want to ID with it for whatever reason. This, combined with a culture that massively underdiagnoses autism for both boys and girls due to how stigmatized it is. Despite a study which claims 1 in 38 children in SK have traits that would qualify for an Autism diagnosis (compare with 1 in 100 in USA which is probably inaccurate but w/e), only 1/3 of the kids that were flagged were actually diagnosed. Many families with a diagnosis keep it secret, even from the kid, many families who suspect autism in their child won't bring it up due to the shame associated with a diagnosis, and many don't even know what it is or what to look for, and it won't even cross their minds. Of course, these attitudes aren't unique to Korea, these ableist attitudes are global, it's just that it seems the prevalent attitude in Korea is pretending it doesn't exist. (though attitudes are changing postively!) Taking this into account, I really doubt a company would even know if one of their trainees had an autism diagnosis. If any of the staff suspected autism, I don't think they'd push for a diagnosis, and if they did actually know, I don't think they'd make it public. With a global and local lack of understanding of autism, I think it makes it extraordinarily difficult for someone to "come out" as autistic in the industry.
I'm not sure if you the asker are neurodivergent/on the spectrum yourself, but I don't think autism would necessarily be too limiting to prevent a successful career. Not every autistic person has social anxiety despite whatever social difficulties they have, and a talent motivated by special interest such as singing or dancing might actually help them be more skilled than their peers. Of course there's sensory issues, but we've seen idols have meltdowns over sensory issues before and come out the other side mostly okay, and we also know that in groups with healthy friendships that the members are happy to accomodate other members' quirks or struggles. Autism or no autism, people who care about other people naturally accomodate for other people's needs and difficulties. Implying that autistic people couldn't succeed in the idol industry rubs me the wrong way a little - anyone with autism is going to struggle in any career they do, some people more than others, some careers more than others, but having autism shouldn't universally rule out any career of any kind.
While I was joking about Sunmi, I don't see why it wouldn't be possible.
#for transparency so nobody takes this the wromg way i have neurodivergent diagnoses plural#if it wasnt already obvious from my... everything...#i dont wanna link anything like sources cuz i dont have the bandwidth to check whether theyre like secretly evil etc#also yeah sunmi has a bpd diagnosis but i srsly dont mean anything by it i just mean moreso how broadly inept#the world is at accurately diagnosing and understanding neurodivergent conditions#long post
19 notes
·
View notes
Text
Im laying my bets now. the entire idea that autism (and adhd) is more common in men and boys is pure myth created by poor science, backwards statistics and faulty parameters of the condition itself. in another 50 years we will understand it was never a gendered condition. just a highly gendered and biased measurement system. i'm absurdly confident on that
the rates of autism in girls is "rising" exponentially. it is rising even more exponentially in girls than in boys. not because girls are becoming more autistic. but because the "science" is just getting better at measuring and accurately acknowledging autism in girls.
autism often does present differently in girls, due to how girls are raised or personality differences. the literature and criteria was based on boy sample groups. the entire research data was done on white men as if that is a standard default person and control group.
not only that, doctors and teachers and parents literally were not looking for it in girls under the false widely propagated belief it was rare in women in girls. it is a self fulfilling prophecy. that's not science.
we will soon have to reckon with the lost generations of autistic girls and women and children assigned female at birth* who never got diagnosis and early intervention. we should be forcing the world to reckon with it right now. a great deal of autistic millennial women are brilliant minds who dropped out of STEM and the workforce due to their untreated and misidentified disability overtaking their life. the impact of never Knowing you or your child is autistic or adhd is difficult to comprehend for autistic and adhd people who did get diagnosed as children. even when the awareness and interventions were unhelpful or harmful. the harm of not knowing means the child trying even harder to become neurotypical and a level of autistic burnout few others on the spectrum can comprehend, often taking place after the woman is a legal adult, and there are no legal protections in place for this disabled person.
the unmitigated stress of being developmentally delayed and never knowing it, simply hating and blaming yourself and fighting day in and out past your limits to become neurotypical, limits your don't know you should have because you have never been so much as briefed on what adhd or autism can feel like. you don't know the distres and tiredness you're feeling is "dysregulation". this is why we see women in nervous breakdowns. psychiatric wards. treatment resistant depression. electric shock therapy. hard drug addiction. cutting. homelessness. personality disorders. dissociation. psychosis. early death by accident or suicide. (obviously people who are not autistic or adhd have these illnesses but my point is untold and disproportionate numbers of them are undiagnosed neurodivergent with unprocessed trauma. i'm telling you. more than you think).
it's why we see young people on tiktok not faking DID per say, but describing a dissociated experiences and fractured sense of self and escapist alternate personalities, a mental illness that has much less in common with traditional DID, but has much in common with struggling and under-treated autistic people. DID is a very rare condition. autism is very common. autism can create out of body experiences and self protective blurring of reality and fantasy so extreme, no person can be expected to understand it is autism if they never been advised about their own disability and the knowledge that should he available to them. it's no wonder we have people with mislabeled rare disorders like DID who are clearly very sick but instead of showing real DID signs, are sick with all the signs of severe unassisted autism they have been completely barred from understanding or coping with in any other way. for those lucky enough, we see unemployed young women with severe chronic pain in their 20s and 30s who look and feel like they're elderly and gave up their dreams when they hit 21 or 25 and their brains stopped working and their bodies shut down. now they mostly scroll tumblr and tiktok and try to remember to open the blinds. they have a roof but people scorn them for entitled laziness and worst of all derided for "self diagnosing".
again i'm asking why CFS chronic fatigue syndrome is so responsive to adderall. i'm asking why professionals are reluctant to test women for adhd if she does well in school because she is very bookish and why experts in the field are openly amused and doubtful to test a woman for autism if she has a long term boyfriend. why is ability to mask or function a disqualification. why is inability to function in women, who later turn out to be autistic or adhd, so aggressively mischaracterized as BPD, bipolar, depression, OCD, schizophrenia. why is autism and adhd clinically diagnosed and defined by distress and dysfunction and not by intrinsic traits and qualities that present while still functional for preventative care. why are all people, men and women forced to wait until their lives and minds are deteriorating and they have experienced some irreversible disasters and pain before they can be diagnosed. why must girls and boys wait until their daily life as children have become unbearable hell for them before their disability can be treated and acknowledged. and if these policies are changing now, why are doctors and psychiatrists not eagerly and urgently reaching out to find the vulnerable adults they missed during more archaic screening methods. we aren't rising in adhd diagnosis because of tiktok you assholes. adult onset adhd and autism don't exist. those people were always adhd. adult onset skill regression and increase in severity due to stress DOES happen in adulthood. modern day stresses like loss of structure during the pandemic and social media is advancing to become more attention span draining. everyone is feeling the effects but these are causing adhd and autistic people to cope less and mask less effectively so they are running into significant problems, their loved ones are noticing, they are getting referrals and suddenly forced to google their rapidly worsening mental issues for the first time and seeing they line up with a known neurological condition . this is obvious. doctors blaming it on some sort of trend are being willfully clueless
*because autism especially is screened identified diagnosed and first intervened ages 2-5, before a child has an internal concept of self or gender and above all before they can express their gender, diagnostic practices and criteria are based on how adults perceive a child via birth assignments. and the studies are overwhelmingly beholden to data only on children assigned male at birth, rarely accounting for their actual future gender either. as part of the warped science insisting that autism is as if somehow linked to the y chromosome and not a universally likely human quality, you see amab kids laser focused on as candidates and afab kids fucked over most of all. all children assigned female have the worst chances of their developmental disability being identified and acknowledged in a timely manner and disproportionately experience late diagnosis in later adolescence or adulthood. tho i wouldn't be surprised if trans womens rates of accurate diagnosis is lower than cis men. as trans girls may present autism differently and characteristic of girls autism, even while still in the closet or before she knows she is trans. regardless adults are very vigilant for signs of autism, even atypical ones, in any child they perceive as a boy. so any millennial or gen z child identified female at birth had significantly worse chance at receiving autistic support compared to peers
in particular women assigned male at birth might have a better chance at being identified for types of autism that are often labeled "high functioning", involves high masking, and often receives few services. these more invisible types of autism often need to be diagnosed before age 5 in order to qualify under the criteria at all. and so in the days where autism was believed to be 20x more common in the genetics of xy children, any chance of being considered and diagnosed would come down to almost purely birth assignment dependent. with the less outwardly visible types of autism, a person who misses this window will remain autistic all their life but once they learn a certain level of skills and masking, no matter how late they learn these, the person will no longer qualify for diagnosis, either not until they have a nervous breakdown or possibly not ever qualify. it's this type of more hidden autism we see struggling across the board as undiagnosed adults including both trans and cis women especially, tho we are seeing it disproportionately even more so in undiagnosed afabs of any gender. who are dropping out of schooling and work and succumbing to severe mental illnesses during what should be the prime of their lives. overall tho birth assignment is not everything this is an issue that disproportionately impacts cis women. trans women. trans men. non-binary people. likely doubling for those that are afab. and then tripling and quadrupling for children who are not white.
bit of an understatement in that last part there. gender likely isn't even the biggest barrier to proper diagnosis and treatment. probably race is even more so. but since gender is such a big disparity in itself across race and one i relate to and can speak on from experience ive focused on it here. a more in-depth look is needed on the neglect of adhd and autistic children of color especially black native and latino kids. but for now do keep in mind the points i'm making increase exponentially for kids who aren't white across all genders including cis boys
#this is dramatic and long but it's a dramatic situation that is completely slept on in the public eye#it's not just about me this is about people who had it so much worse. tho my insider experience obviously brought it to my attention#i'm pretty sure i'm not autistic im adhd but the reality of adhd is a lot more like autism than we are acknowledging#a topic for another day#autism in women#adhd in women#atypical autism#adhd inattentive#undiagnosed autistic#undiagnosed neurodivergent#undiagnosed autism#undiagnosed adhd
30 notes
·
View notes
Note
Hey, Nyarla. I've been following you for a while and although this is a safe space and you seem extremely open minded and kind, I don't feel brave enough to say this off-anon due to past experiences.
You're one of the first authors who, without writing for it directly, has made me comfortable reading your headcanon sets and your fics and blurs, because they way you represent characters is comforting.
I am autistic, and it is extremely hard to have people not treat you like you're either mentally impaired (due to misinformation) or plain creepy (due to ableism), and it is disheartening to just exist sometimes. Often times, this kind of treatment gets applied from authors into their work. I don't think everyone has to know everything about every single condition in the world, but it seems there's a tendency to, most of the time, infantilize or demonize, or apply the aforementioned treatment, to neurodivergent people.
But to my very pleasant surprise, you had this set of headcanons for Mihawk, titled "Mood Swings", where you wrote the reader with some bipolar tendencies, and I couldn't help but bawl. I genuinely cried for a good while, in both relief and happiness. You didn't demonize bipolar tendencies, nor make him annoyed, nor anything of the sort. You were SO respectful about it, and so fucking mature in your writing, and it felt like a warm hug and a reassuring pat on the back.
You haven't even written anything for an autistic reader themselves, and you still helped me immensely with one single fic. Thank you so much for the way you write, and for the way you interact with your followers. You're wonderful, and I am eternally grateful to you for just one single set of headcanons like that. You reaffirmed the comfort within my comfort character. I hope you yourself find joy in the fact you, unknowingly, made a person so irremediably happy.
I can't thank you enough ❤️
I understand completely the desire to remain anonymous, but please know I still have the utmost respect for you for sending me this, and I really just wanna give you the biggest hug in the world, and I legitimately have tears in my eyes right now.
I'm going to come out and say right now, I'm schizophrenic. My official diagnoses is schizoaffective disorder depressive type, which essentially means that I experience symptoms of psychosis associated with schizophrenia (mostly auditory hallucinations in my case, occasionally visual, tends to worsen with lack of sleep) in tandem with symptoms characteristic of depression. I don't tend to tell people about it, because I know how schizophrenia is depicted in fiction and media in general. Typically as psychos that do bad things "because the voices said to."
I'm saying this because I want you to know that I understand how people tend to attach stigma to mental health conditions and neurodivergence, and I know how much it sucks and how much it hurts; and also that I respect you so, so much for talking about it. It's kind of skewed whether schizophrenia is considered neurodivergeant or not, but I tend toward identifying as neurodivergent. Experiencing the world differently, processing information differently, thinking differently is the general definition of ND, and I definitely identify with that.
I haven't specifically written autistic characters/readers largely because I don't feel like I would be able to accurately represent it, and I do not want to write it in a way that would make anyone uncomfortable or upset. I helped raise two of my nephews that were autistic, and they were both so different, in personality and quirks and "symptoms." They're also amazing and vibrant and intellient in ways that I can't even begin to describe.
Two of my favorite fictional characters that are generally accepted as being autistic are L and Near from Death Note. It's never explicitly stated in the manga or anime that they're autistic, but they're both written and depicted in a way that shows how they think and experience things differently without demeaning them for it; that other characters are a little nervous or intimidated around them at first, but grow to understand and form bonds with them over the course of the story; and they're also shown to be distinctly different from each other in personality, rather than carbon copies of each other. As such, if you haven't read/watched Death Note, I highly recommend it. Manga more than anime for personal reasons (there were some differences made in the ending of the anime that I don't agree with but I'm not going to get into that here)
ANYWAY
I'm also really beyond happy that you enjoyed Mood Swings. I wrote it with exactly the intention of representing Bi-Polar symptoms realistically and without any stigma. Knowing that you found it comforting makes me so, so happy. That was exactly what I wanted. I've seen "bi-polar" used synonymously with "psycho" so often, usually in tandem with a particular word rhyming with "witch," and I hate it so much.
Mental health isn't a joke. Some people are born with their brains wired differently. Some people are forced to live through trauma that rewires their brain. It makes day-to-day life exhausting beyond measure, particularly if it involves interacting with other people, and it's even more exhausting when others poke fun at it and don't take it seriously.
I know I'm repeating myself, but I really, sincerely want this blog to be a safe place for everyone. So it makes me so, so happy to recieve Asks like yours. So thank you again, and I hope you (and anyone else who needs it) continue to find this to be a safe place.
7 notes
·
View notes
Text
Content warning for discussion about depression, suicidality, mental illness, disability, therapy, treatment, hospitals, and the American healthcare system.
I don’t know a lot about John Fetterman; he seems like a decent guy though and I hope his treatment goes well. When I first saw the headline that he was checking himself into the hospital for depression, I thought, “well, good, I hope this starts many conversations about hospitalization for mental health treatment.”
I have already been thinking about hospitalization a lot lately. I turn 40 soon, which means it’s also the 10 year anniversary of my most recent mental hospitalization, following what had been my fourth or fifth suicide attempt. That stay got me on medication I still rely on today, and the follow-up outpatient care eventually led to the ADHD diagnosis which explained why my depression had been so resistant to treatment for such a long time. (Like I said, before age 30, I had four or five suicide attempts, over fifteen years in and out of therapy with at least half a dozen practitioners by that point, including a previous hospitalization, and tried more SSRIs and supplemental medications than I can remember.) Turns out all the serotonin in the world can’t make a difference if you don’t have dopamine.
One of the things my therapists would often ‘congratulate’ me on was my very clear and precise self-awareness regarding my mental illness. But that level of introspection meant over the years I grew increasingly frustrated and isolated by others’ inability to understand or empathize with my struggles. Even when I had complete lucidity over my mental state and could communicate it in a descriptive and accurate manner, there was no way the other person could actually *know* what it really *felt* like. Excepting, of course, some of the other patients who were in my unit at the hospital. In the year or two following my second hospitalization, I came to realize that the major barrier to neurotypical people understanding people with mental illness disorders and other neurodivergent diagnoses is that, unlike physical ailments, there really is no temporary mental illness. Of course some people experience trauma, grief, or deep sadness that require a short period of medical intervention, but the type of conditions that lead to multiple crises and hospitalizations are always lifelong. I do not pretend that passing physical maladies are truly comparable to permanent physical disabilities, but the fact that almost all people will have an injury or illness at some point that will at least partially debilitate them before recovery gives them at least a starting point to imagine what a permanent disability would be like. I do think this is part of the reason why society has been much better about creating standards for accessibility and accommodation regarding physical status as compared to mental status (although of course they are still woefully lacking in both areas).
After this realization, I had an idea for a comic I wanted to do about my experience with mental illness, and more specifically treatment for mental illness, especially in regards to how it works in the United States. I think I even talked about the general outline of it with one of my therapists, but of course, it never came to any kind of fruition because of ADHD and extreme executive dysfunction. (I mean, that’s why I gave up comics and any kind of art as a career all together, after all.) So here is the script I have carried around in my head for some nine or ten years, a bit of solace for whenever someone (including myself) asks me why I can’t just do a certain thing, or why I take so long to do something, or just in general why I am how I am.
Imagine you are walking along one day, and suddenly both of your legs break. Now, this isn’t the first time you’ve broken a leg, in fact, it seems to happen with some frequency, but rarely simultaneously, and this time they are really bad; all kinds of messed up angles that shouldn’t be there.
“Hey! Help!” You cry out, “I really need someone to help me!”
A few people pass by not noticing or pretending to not notice, but eventually someone stops and says, “oh wow, that looks really bad!”
“Yeah, I know” you reply, “can you help?”
“Oh sure, there’s a hospital just a block that way. If you get up and walk over there I’m sure they can fix you right up!”
“Uhh, what. Are you joking?”
“No, it’s just right there, see? It’s a really short walk!”
“Both my legs are extremely broken. I’m quite sure I cannot walk at all.”
“Have you even tried though? Look, I walk all the time, it’s quite easy, just put one foot in front of the other. Watch how I do it and I’m sure you can too!” And you watch them easily walk away as you are lying on the ground.
You start dragging yourself in the direction of the hospital using your hands and arms, continuing to ask for help from those walking past you. One person suggests that if your leg doesn’t work, you could just hop on the other leg. You explain, no, both of your legs are broken, you don’t have another leg to use. They look at you with a puzzled expression and say, “well that just doesn’t make any sense” while shaking their head and then going on about their business.
The last person you ask for help says, “oh, of course, let me carry you the rest of the way” and you let out a huge sigh of relief.
They continue, “just stand up so I can pick you up and piggyback you over there.”
“Umm, is it not clear that is entirely impossible for me?”
“Ugh, just standing?” They scoff, “how can I be expected to help you when you aren’t willing to help yourself even a little bit?”
“I mean, I already dragged myself over fifty yards of pavement, I think that’s pretty good.”
“That’s ridiculous, everyone can stand, even toddlers can stand for a little bit. All I’m asking you to do is stand for a few seconds so it’s easier for me to pick you up.”
You look down at your legs, each curved in a different spiraling shape, now fairly bloody from being dragged down the street. “And I am telling you I definitely cannot do that” you respond as they walk away.
Eventually you do manage to drag yourself through the hospital doors, your arms bruised and scraped, looking almost as bad as your legs. Fortunately the medical staff gets to you and takes you in for surgery right away. Well, not quite right away, as you’re hard to see on the floor, and perhaps one or two of the orderlies accidentally trampled you or ran a gurney over you, but none of that matters because now you’re in the hands of professionals and they are going to fix you!
The first thing they do, of course, is take you in for x-rays after asking you a few questions. They wheel you in to meet the doctor, and you think, “ah great, we’ll have the surgery to set the bones and then in a few weeks or months I’ll be good as new!” The doctor then explains that no, that is not going to be what’s happening, as you can clearly see in your x-rays, you don’t actually have any bones in your legs, just a bunch of toothpicks held together with scotch tape.
On your floor of the hospital, you meet other patients with toothpicks and scotch tape in their legs, some with twigs held together with twine, some that have plastic forks and hot glue, and even a few that were somehow getting by with crazy straws and silly string. Most of them are like you and never had bones in their legs to begin with, but there are a few that had their bones stolen by someone, or lost them in a horrible accident. You also see a few patients that do have real bones in their legs, but they also grew spring-loaded hammers attached to their toes that whack them in the shins every time they try to take a step.
Well, the toothpicks and scotch tape definitely explain why your legs seem to break so easily and frequently, but is there any way you can get real bones for your legs?
“Oh no,” the doctor explains, “your body can’t grow bones in your legs, and it would reject any bones we transplant into your legs, plus you would have no idea how to walk with them.”
“Well, I would argue I can barely walk as it is,” you respond, “but I guess I see your point.”
So you and the doctor discuss options and plans for treatment. Perhaps you can start by upgrading to bamboo skewers and duct tape, there’s a lot of new and exciting research coming out about the use of wooden dowels, and maybe once you’ve been in outpatient treatment for a while you can find a carpenter who can carve you custom support with hinges that are actually screwed in.
(And since this all happened before the Affordable Care Act was passed into law, and since even after it was passed it didn’t provide anywhere near the help that is needed.) “This all sounds good, but I just don’t know how I’ll be able to afford it. I’ve had a hard time staying employed, since my legs break every few months and jobs almost always require some amount of standing and walking.”
The hospital staff reassures you, “don’t worry, there’s a program for people without leg bones to help pay for their treatments, just go to this building when you check out.”
And so after about a week you do check out of the hospital, legs in full casts up to your hips to protect your new, but fragile, sticks inside. You’re able to hobble around surprisingly well using crutches, so you make your way to the address you were given.
When you get there, you find a building surrounded by a 10-foot tall stone wall and a 5-foot wide moat. You circle the whole building, but there are definitely no doors, bridges, or even windows within reach. You do find someone who seems to look official and in charge though.
“Excuse me,” you ask, “is this the place for people without bones in their legs? How am I supposed to enter?”
“Yes, this is it. You’ll just need to pole-vault over the moat and wall.”
“Umm, I think there’s been some mistake. I’m just recovering from both my legs breaking, as are most of the other people seeking your services, I believe. Are you able to provide any kind of assistance for me?”
“Oh, there’s no mistake. You grab onto the pole with your hands, so it’s totally fine for your to do. And we can loan you a pole if you need, you’ll just need to do 10 jumping jacks and a short hopscotch run.”
You roll your eyes thinking, how on earth does anyone ever get through this? As you look around, you see more people with fresh casts on their legs, or old bandages, or some with a leg still broken. You see a lot of them run a few steps with the pole only to have a leg give out from under them and they fall again. Many of them do just give up and crawl away at that point. Some people look like they have family members that are trying to push them over, or do the pole-vaulting themselves while carrying the injured person. A few have even hired a catapult to fling them over, but that seems to cost more than any financial assistance you could get. Eventually you decide to tunnel your way under. It’s slow and laborious, but it seems the least risky, and you really don’t want to break a leg again.
When you finally get through, you do start getting regular checks on how your legs are doing. You learn how to spot splinters so you can plus some glue on them before they turn into full fractures. And importantly you start working with a trainer to build up the strength of your leg muscles, and learn how to walk more delicately so that the sticks in your legs don’t get so much damage from impact. It’s a slow walk, but you’re staying upright, and it feels like something you can maintain for while.
As you start getting back out in the world more, you do notice that everyone walks much faster than you. Most of the time it doesn’t bother you that much, but sometimes you’re walking somewhere with family, friends, or coworkers, and they’re just getting really impatient with how slow you are. Some times you take the time to explain about how you don’t have bones in your legs, and if you walk any faster you risk one or both of your legs breaking again. And they will make a sad face and say that they will wait for you to catch up, but no one ever slows down to match your pace for more than a few strides. So more often you just say you’re tired, and the other person responds, “oh, that’s too bad. I would wait for you, but I have to go run this 10K to support #NoLegBonesAwareness - you really should join next time, bye!”
The worst thing that happens, though, is when someone asks you, “have you thought about what would help you walk better?” And you want to scream at them, “Bitch, of course I have! I think about it all the fucking time! Having actual fucking bones in my goddamn legs would help!” But of course you can’t do that because at least they’re trying to understand that you have a problem that they don’t know how to fix, whereas everyone else is suggesting calcium and vitamin D supplements to help your non-existent bones grow. Or when they find out walking is difficult for you, they suggest jogging might be easier instead. Or perhaps flying? Have you tried flying?
And so you just keep walking along, mostly slowly, sometimes a little quicker, and sometimes really, really slow. And meanwhile your peers are getting married, buying houses, starting families, all the regular things society likes to celebrate. And one day you realize you’ve been walking for a really long time, years maybe, without breaking a leg, and it’s the first time in your life you’ve gone that long without a broken leg. And you know that’s a much harder and more difficult achievement than any degree anyone’s earned or promotion they got, and took so much more work. But there’s only about a half dozen people in the entire world that actually understand that, and you’re not close with any of them.
And while you’re thinking about that, you hear a sickening, yet familiar crunch.
That’s what it’s like to live with mental illness.
#depression#tw sucidal ideation#mental illness#mental health#adhd#disability#hospitalization#adhd problems#tw depressing thoughts#healthcare#john fetterman#no bones day#cw depression#cw mental health#cw mental illness#tw injury
4 notes
·
View notes
Text
Hello world!
Hi! I'm Zero! they/she pronouns please!


This was meant to be a quick about-me, but I ended up doing something a lot more comprehensive! So yeah, here's that!
I write/work in disability advocacy, social justice, and education.
I focus on autism, ADHD, PTSD, cPTSD, and LGBTQIA+.
I am disabled, autistic, dyspraxic, and an ADHDer; I have PTSD—both the acute and cPTSD colors—and prolonged grief disorder; I am nonbinary.
I diagnosed myself with all of these as I grew up and received formal diagnoses for most of them in my 30s. My career in math education mostly ended in 2020 shortly after my love died in the first year of the covid pandemic. Both autistic and career burnout caught up with me; all of these things made continuing being in a classroom untenable.
Although I no longer teach in front of a class, I still write and study on the topics of education, mathematics, and math education.
I have "traits consistent with" being bipolar and having borderline personality disorder (BPD), although I have not been formally diagnosed with those ones. I am probably subclinical for bipolar—"subclinical", as in, a diagnosis would not be appropriate—and I believe that my BPD is better explained through the lens of neurodivergence, PTSD, and cPTSD.
I'm interested in connecting with other advocates, educators, and social-justice-oriented content creators!
More on Diagnoses and Accommodations!
I define "Diagnosis" to mean, "Associating a named condition with the person." There are "good", "neutral", and "bad" diagnoses. I believe the purpose of a diagnosis is to provide perspectives, frames of reference, and actionable accommodations.
Basically, does knowing the diagnosis help the person make sense of their state of being? For external conditions like PTSD or even something like a broken bone, the diagnosis is frequently the first step to recovery. For conditions that are inherent like being autistic or being nonbinary, the diagnosis provides a frame of reference to better understand and interact with the world.
Note that most people want a so-called "accurate" diagnosis, but they define accuracy based on some arbitrary listing of what the condition is and how it affects people. To the point that, eventually, anti-autism groups like Autism Speaks will release what they'll claim is a genetic test for "true" autism.
When that happens, they'll arbitrarily define people as autistic based on if they have those genetic markers or not and say anyone who was self-diagnosed or diagnosed by any other method other than their genetic test are not "actually autistic". Their plan has many objectives, but none of those objectives are about helping autistic people live and thrive with their lives.
It would be like if someone wanted to make all their dishes better by washing and cleaning them and your first step was to throw out any dishes you disliked. Sure, maybe that world seems "cleaner" to you—the person doing the cleaning—but those dishes are not benefited through stripping their status as "deserving to exist" and throwing them in the trash.
A good friend recently introduced me to a wonderful quote that encapsulates a lot of what I believe with respect to accommodations and diagnoses. It comes from Marcus Parks, one of the hosts of the podcast, "The Last Podcast on the Left". He has said, "Your mental health is not your fault, but it is your responsibility."
Too frequently, mental health ends up stigmatized due to the fact that society only really makes a big deal about it or even notices it when it causes friction. We've gotten a little bit better over the years as disabled communities have grown online and we started comparing notes, but for far too long, we only got "diagnosed" as a way to other us.
If you're undiagnosed, good luck! I hope that you will luck into everything you need. But once you get a "good" diagnosis, then you really do start to understand more and more about yourself and what you need in order to not just continue living, but in order to thrive as best you can.
I usually use the analogy of glasses/contacts. I have something like 20/400 or 20/600 vision, which is legally blind, but so long as I have glasses or contacts, I can pretty much get by with only minor inconveniences. It's not my fault that I cannot see, but it is my responsibility to accommodate my vision, and, when my vision is unaccommodated, to not do something like get in the driver's seat of a vehicle.
Because, for the most part, my vision is well-accommodated and only minorly stigmatized by society, I did not list "impaired vision" up front when I was discussing my identities. That being said, it still impacts my life and how I interact with the world. I need to do things like have back-up glasses when I go out wearing contacts or else risk being stranded. I have to think about wearing contacts during any scenario where my glasses are in physical danger.
(I once knocked my glasses off my face swatting at an insect for them to tumble down in front of me... the me sitting on a riding lawn mower at the time. Goodbye glasses. So, now I don't wear glasses to mow the grass).
Especially since 2020, the financial cost of accommodating this condition has been staggering for me, but even then, having impaired vision is something that is well accommodated for me, so although sometimes annoying, it doesn't make me feel like my life is completely different from someone who does not need glasses.
And that's really my current goal for most things I am working on in this advocacy space:
To help people accommodate themselves in ways that are going to give them the best chance for success, and,
To change societal views away from these boogieman-like representations of our people and the conditions we live with.
Thanks for reading!
#actually autistic#actually adhd#complex ptsd#actually disabled#disability#human rights#personal#autoethnography#mental health
4 notes
·
View notes
Text
On being uncertain if you’re neurodivergent
(I’m kinda responding to this post over here because while i doubt the last addition was derailment, putting this there would definitely be a complete hijack because this is a larger thing I’ve been meaning to write about and that post was more a prompt than a thing I’m directly replying to)
@intpdreamer said:
I have to ask. How strongly do you need to relate for this to be a valid thing to ask yourself? I relate much more strongly to how autistic people describe their experience of and interactions with the world than how most nt people do, but I'm scared to presume too much from that for fear of being That Person. But surely some people who relate to a lot of nd traits really do do so because of an undiagnosed neurodivergency? I completely get why the "we're all a bit" conclusion is bad and why being scared of being neurodivergent would be offensive, but how is someone supposed to know if they're "nt downplaying what a trait really means and concluding they have it" vs "actually neurodivergent but undiagnosed relating to the trait because they do have it"?
General prelude: this is apparently a controversial opinion and probably not representative of the broader ND community. I have only limited expertise, but I do have some. My tl;dr answer to the “how do you know” question at the end is mostly “you likely don’t” with some “i guess that’s what diagnosis is meant for?” and some “make sure you really understand what the trait is about, how pervasive and significant it is, and whether you also have other ones”
How to tell?
I don’t believe neurodivergent vs neurotypical to be a discrete thing. By which I mean, it’s not like there’s some idk structure in some person’s brain and not in another that you can be like, “you’re neurodivergent. you’re not.” Brains are incredibly fkin messy. So, there’s a whole miscellany of differences in like, size of structures or sensitivity or connectivity, each of which is probably continuous...but the combination of them is definitely continuous.
Which is not to say there’s some clear definable “spectrum” from “Maximally Neurotypical” to “Maximally Neurodivergent” (I mean, I guess you could add shit up or something but it’s not really very meaningful). Here’s a representation made by an autistic person:
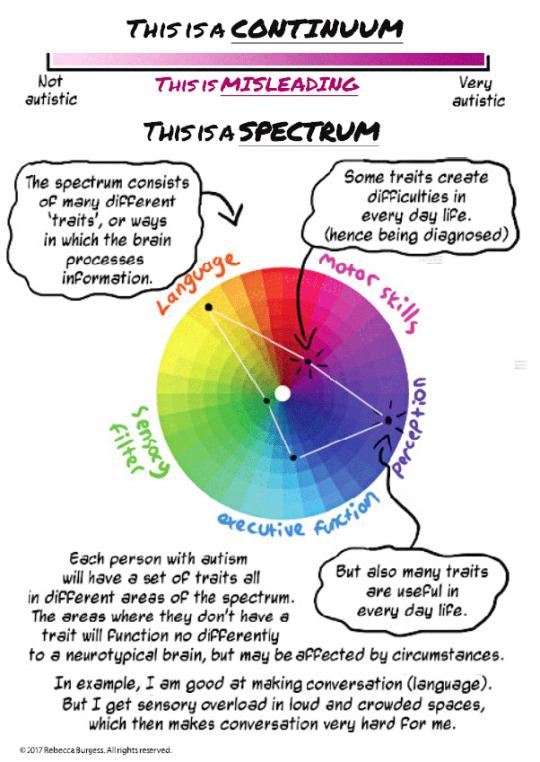
(full comic)
So, at some point, we pick some sort of threshold to define what is significant aberration for any given trait, and how many traits you gotta have to Have The Condition. How do we decide it? Well, clinically, it goes like “does this thing fuck with your life?” (for how many, we test it out on lots of people and kinda sorta figure whether we think having x amount over- or underdecides people with significant effects; there’s a lot of judgement involved and it’s broadly agreed that there isn’t nearly enough of this done for it to be very accurate -- your clinician is meant to use their judgement on each particular case).
There’s a misconception that this is particular to psychiatric diagnoses, but it’s like, most shit. A person in that thread mentioned diabetes...that’s continuous, too. We picked out a threshold for that, too. The only difference is that there’s things you can quantitavely measure and find out at exactly what point it is that shit starts fucking with your life. (“everybody’s a little X” is still pretty silly and meaningless for both)
What this means is that there’s a lot of people who are in fact clear-cut neurotypical or neurodivergent...but there’s also a bunch of people hovering around the threshold point where it’s just like...??? up to judgement. And if you’ve never been diagnosed, it’s absolutely likely that you may be in any of those 3 groups and it’d be a complex call to make.
There’s a whole raaange of shit recommended for assessment, some of which you can self-administer (I think many of the listed instruments can be found here) if you really want to.
But I think...if you make an effort to understand autism/other neurodivergence and the specific traits you’re thinking of, it’s generally unlikely that you’re "nt downplaying what a trait really means and concluding they have it". That usually comes from people who’ve made no such effort. IF you know an ND person who’s happy to discuss (like, pls don’t expect them to do that), they could probably help confirm/deny whether you’re correctly understanding the trait.
And of course, if you vaguely relate to like, ONE or two traits, it’s probably disingenuous to presume. But if you consistently relate to many/most traits, have made effort to understand what they mean beyond face value, and they’re significant enough to affect your life beyond quirks, you’re probably good. But...
Does it really matter?
The chief purpose of formal diagnosis is treatment, research and resources (e.g. disability benefits). I’d venture that the purposes of informal identification with a diagnosis (or label in general) include understanding, community, communication and resources (e.g. information). I’m not sure which of these (or others) you’re seeking, but understanding and resources are free. I back using whatever frameworks are available to you to help understand yourself better. Asking yourself is 100% your right at all times.
The difficulty only really comes in with the community and communication aspects. So, let’s imagine you go wrong -- you’re actually NT but you read a couple things and decide you’re autistic. You start participating as a member in conversations about autism and telling people you’re autistic. What does that mean?
So, chances are that if you’re extrapolating from your personal experiences but are actually NT, you’re wrong about a bunch of shit. You’re now creating or reinforcing a bunch of misconceptions about autism to NTs. You’re also trivialising autistic people’s experiences by behaving as though your quirks are a whole thing. This is bad.
If you made and are continuing to make efforts to listen and understand, you’re probably not doing this too much. And upon considering it, you could probably reduce it further. But maybe it’s better if you don’t do it at all?
It’s my experience that people of the form “I think I might be X” are welcomed in many communities of X if approached sincerely (it’s also been my experience that they’re quite enthusiastic to help you understand because a lot of them also didn’t realise for a very long time and it improved their lives substantially when they did). Also, if you say “I think I might be X” to some random person in your life and proceed to do dumb shit that would’ve spread misconceptions, it’s a lot less likely that this person will go on to say, “this is what X people are like”.
So that’s probably a sensible middle ground where you don’t have to be 100% sure but you can still get (and add!) value from the descriptor.
Bit of a personal comment
So, with me...my psychiatrist suspects I’m autistic, and so did my mother (although she’s clueless and doesn’t count). The hospital diagnosed me with a personality disorder, and strongly suggested bipolar in the terms used in their comments. My psychiatrist has not diagnosed me with bipolar, but is nevertheless treating me with mood stabilisers. She also wanted me to test for epilepsy. I strongly suspect ADHD. Suffice to say, I have no fucking clue what’s actually going on with my brain and it seems neither does anyone else. The only thing we all agree on is there’s definitely something.
So, in the end, I read and apply shit from all sources, and I ID as generic “neurodivergent”.
Diagnoses and labels are very useful tools, but at the end of the day, they’re just that -- tools. And sometimes they can be very stupid and limited. Think things through properly and understand them well; be considerate and don’t impose; and then do what you think is best for you.
#(none of this is specifically targeted)#(except i guess 'if you're asking this question and making this effort you're probably good')#neurodivergence#autism#adhd#thoughts#diagnosis#self-dx is beneficial#if you take care to avoid the known possible harms
6 notes
·
View notes
Note
I have an idea for a fic and I think you could do it better justice than I could, so here goes: Fitz realizes he's autistic after his child is diagnosed autistic. Partly inspired by your post thinking up an autistic fitz childhood fic and my own fitz as a dad feels after writing my little ficlet. Of course, if you don't want to write it, that's perfectly fine.
Processing Systems
sorry this took a while to write! femslash feb happened so you know how that is. but here it is! in all its very educational glory! (with some fluff, it’s not all boring)
3210 words
read on AO3
“Dr. and Dr. Fitz-Simmons, thank you for joining us,” the diagnostician,Dr. Booth, says, a professional smile on her face. Fitz and Jemma take a seatacross from her at her desk, while Caroline, as calm as the four-year-old canmanage, bounds into the diagnostician’s window seat and presses her faceagainst the glass, watching the cars go by outside, her hands twisting togetherin her lap.
“Thank you for seeing us on such short notice,” Jemma says.“Our schedules can be a bit … hectic, as you know, but you’ve been very accommodatingwith your time.”
“Of course.” Dr. Booth readjusts her glasses, peering at apile of papers on her desk. “Now, you said you were advised to come here byyour daughter’s school, correct? This wasn’t an unprompted decision.”
“She’s our first,” Fitz explains, glancing over to Caroline,who hasn’t moved, is just staring wide-eyed out the window. “And neither of ushave a lot of experience with kids. We didn’t think there was anything …different, about her.” He scratches at his face, then looks down at his lap,adding somewhat defensively, “We didn’t think there was anything to beconcerned about.”
“No one said anything about concern,” says Dr. Booth. “Youdon’t have to see this in a negative light. But if there is something to know,it’s good to know when your child is still young. There are steps you can taketo make sure your child is accommodated for, both at home and at school.”
“So there is something to know,” Jemma says, half aquestion.
“Before we get into the results, I just want the both of youto know the kind of strides that the field of psychology has taken in the lastdecade or so. We’re understanding different conditions more and more each year,diagnosis is becoming more accurate, treatment plans and accommodations aremore highly developed. There’s more to help families now than there ever hasbeen.”
“What are the results?” Fitz asks gruffly.
“Well,” Dr. Booth looks at her paper, a light smile on herface. “According to the tests we had Caroline do, as well as observation, and interviewswith the both of you, I’ve determined that Caroline does qualify for adiagnosis of Autism Spectrum Disorder.”
Jemma lets out a breath, looks towards Caroline, who doesn’tseem to be paying attention, and then towards Fitz, who’s eyebrows are drawntogether.
“There’s nothing wrong with my kid,” he bites out.
“I never said there was,” Dr. Booth assures him.
“You just said she has a disorder,” Fitz argues, facepinched in upset.
“Well, yes, that’s the official title. But not everyone seesit that way. Autism is classified as a disorder, but according to some schoolsof thought, it’s just one of the many kinds of neurodivergencies.”
“I guess—” Jemma starts, grabbing Fitz’s hand to rub herthumb along the side of his thumb, “we just don’t know much about it, is all. Imean, you hear things, but we aren’t really educated in the area. It’s inneither of our areas of expertise.”
“I can answer any questions you have, but let me explain alittle of the basics. Autism, or ASD, is classified as a developmentaldisability. It means that those with it—autistic people—hit developmentalcheckpoints at a different rate and sometimes in a different order than thegeneral population. It impacts aspects of communication such as spoken languageand body language, social skills, and will impact how autistic people processtheir environment and the world around them.”
“So it’s like …” Jemma risks a glance at Fitz, who’s notlooking at either of them. “It’s like having a different processing system inher brain.”
“Exactly,” Dr. Booth says. “Some autistic people compare itto being an Android phone in a world of iPhones. There’s nothing inherentlylesser about either system, they’re just different. They have different coding,run different apps, have different strengths and weaknesses. There are inherentchallenges in living in a world that wasn’t built for you, which is why it’s adisability, but every autistic person will have different ways of coping with andadapting to that. Some people can adapt in such a way that you wouldn’t be ableto tell the difference, and some people don’t.”
“So … you’re saying when she grows up, she might be—” Jemmawinces, thinking. “’Normal’, for lack of a better word.”
“No,” Dr. Booth says. “She’ll always be autistic, it’s notsomething you grow out of. Some people are just better at blending in. Forexample, most people wouldn’t guess I was autistic just from talking to me, butI am. And to be honest with you, I think it makes me even better at this jobthan most people are.”
“Because you can relate?” Jemma asks.
“That’s one reason. Autistic people are also highly attunedto the details of things, which is necessary when you’re a diagnostician. We’revery good at picking out patterns. There are certain advantages to having anautistic brain. Different strengths and weaknesses, like I said.”
Jemma squeezes Fitz’s hand, watching the side of his face.She can see he’s still obviously upset about something. “Doesn’t sound soscary,” Jemma says, trying to comfort them both.
“You know—” Fitz cuts himself off, glancing at the ceiling,then to Dr. Booth, then back up. “You know, where- where are you even gettingthis? She just- She seems like a normal kid. You- You say she’s different, butwhere are you getting that? How come you say my kid is so different? That she-she’s got different processing, or something.”
Dr. Booth watches him steadily, and finally he looks at her,then looks away. “You know, no one is saying this is a bad thing, Dr.Fitz-Simmons. There’s no need to be defensive about it. Having terms like thisto describe your child’s experiences can be a very helpful thing, in the longrun.”
“I think we would just be more comfortable if we understoodexactly where the diagnosis came from,” Jemma says, squeezing Fitz’s handagain.
“Of course,” Dr. Booth says, “I can explain how I came tothis conclusion. Well, I mentioned that autistic people process the worlddifferently. These differences in perception can affect our senses—manifestingin what we call sensory defensiveness and sensory seeking behaviors, of whichCaroline shows both.”
“Can you explain what that means?” Jemma asks, when Fitzdoesn’t say anything.
“We’ll start with sensory defensiveness. It means avoidanceof unpleasant sensory experiences, showing a level of sensitivity outside ofthe normal range. Caroline, for example, didn’t like when I turned the mainlight on in the testing room because it hurt her eyes, so we turned on a dimmerlamp instead. You both said that she startles easily and will cover her ears atloud noises, refuses to eat foods if she doesn’t like the texture, and is onlycomfortable in mild weather.”
“All that she gets from her dad, really,” Jemma says,smiling at him. “He’s always been sensitive to that kind of stuff.”
“Hey.”
“What? You have. You hate the cold, the heat, loud noises,certain foods—”
“Everyone has preferences,” Fitz defends. “Don’t seeanything wrong with that.”
“Let’s move on to the sensory seeking behaviors. Shedisplays what we call ‘stimming’—it’s short for self-stimulation. Autisticpeople do it to help themselves process their environment, both external andinternal. Stimming behaviors that Caroline displayed included hand flapping,hand twirling, bouncing, chewing on her lips and fingers—”
“Well, she gets that from me, too,” Fitz cuts her off. “I’vealways felt better when I’m in motion. She’s just twitchy, like me.”
“Okay,” Dr. Booth says, leveling him with a careful smile.“Her language skills are also a point of interest. She shows the capacity for avery advanced vocabulary, but rarely spoke when prompted. When she did, it wasjust to tell me about her favorite fish.”
“Oh yes,” Jemma says, beaming. “She does love fish. Allaquatic life, actually. She knows so much about it. It’s all she talks about,really.”
“And she showed an understanding of words far beyond her agelevel when she did, but for the most part she was silent. She obviouslyunderstood all my instructions, but didn’t respond to them.”
“I mean, she’s already above where I was,” Fitz says. “Ididn’t even speak ‘till I was six. But when I did, it was all about monkeys.She loves animals, just like me. She’s just focused.”
“We would call something like that a ‘special interest’,”Dr. Booth informs them. “It’s common for autistic people to want to focus on theirinterests when they’re by themselves, as well as a way of interacting withothers.”
“Was that all?” Jemma asks.
“Well, she also displayed what we refer to as ‘asymmetricalmotor skills’. Her fine motor skills, small movements, like her handwriting, werereally quite good. At or above the normal range. But gross motor skills, thingslike walking, controlling broad movement of her limbs when we played games,were much poorer.”
“Clumsiness runs in the family,” Fitz says. “I’m kind of aklutz. Good with my hands, though.”
“You know,” Dr. Booth starts cautiously, lacing her fingerson the table, turning to Fitz. “You seem to relate to an awful lot of thetraits your daughter displays, Dr. Fitz-Simmons.”
“W-Well—” Fitz scratches the back of his head, glancing atJemma. “I mean, she’s my kid. There’s going to be similarities.”
“Have you ever considered getting evaluated?”
Fitz just stares, Jemma glancing between them.
“What would that entail?” she asks.
“A similar process to what your daughter went through. A fewtests, an interview, some paperwork. It takes a few hours, when all is said anddone, over a day or two.”
“Sh-Should I?” Fitz asks, aimed at Jemma, mouth bobbing intoan open gape.
Jemma watches him carefully, then turns back to Dr. Booth.“What are the benefits?”
“Well, for adults especially, having an official word foryour experiences can be very relieving. It helps you to make sense of somethings that may have been in the dark in your life before. It can also help youfeel connected to other people like yourself—the autistic community is growingand thriving nowadays, and you can always reach out to other people who havesimilar experiences. And it opens avenues for accommodations in the workplaceas well, should you need them.”
She turns back to Fitz, giving a little shrug. “Is thatsomething you’re interested in?”
He looks away. “Maybe.”
“Well, I only evaluate children, but I can refer you to somevery good diagnosticians who evaluate adults as well. You don’t have to take meup on it if you don’t want to, but from my personal experience, I think it’ssomething worth looking in to.”
Fitz picks at the fabric of his pants. “Yeah, alright.I-I’ll think about it.”
“Our time is about up here, but before you go let me giveyou this—” She hands over a stapled stack of papers. “It’s Caroline’s officialdiagnosis results. You’ll find a full explanation of the results of each test,as well as her scores on the IQ portion of the test. That’s another thing tonote—her test scores vary highly over the different tests. Most people havemore concentrated scores, whereas Caroline scored within a range of 30thpercentile to the 99th. Also included in there is the next steps youcan follow: places to do more research, as well as the possible benefits ofthings like occupational therapy.”
“If we have any questions—” Jemma starts.
“Feel free to email me, and I’ll get back to you as soon asI can.”
Fitz takes the papers as he stands, bending and curling themwithin his grasp.
Jemma shakes Dr. Booth’s hand. “Thank you for your time, Dr.Booth, this has been very helpful.”
“I’m happy to do it. And can I just say, even though she wasa little scared when we started out, it’s obvious that Caroline is a very happykid. I think the two of you have done an excellent job of raising her so far,even without these resources.”
“Thank you,” Jemma says, “that means a lot.” She turns toCaroline, who’s still pressed against the window, looking like she hasn’t beenpaying attention at all. “Caroline, darling, we’re going now.”
Caroline jumps down from the seat, bounding up to Jemma inbouncing steps. She reaches up, and Jemma picks her up with a grunt and settlesher on her hip.
“Can fish be autistic?” Caroline asks, eyes wide, lookingaround the room.
“Oh, I didn’t realize you were listening.” She glances atDr. Booth, smiling. “No, I don’t think they can be. I think it’s special tohumans.”
“Humans are fish,” Caroline says. “Everything’s fish.”
“Well, I don’t think that fish that live in the ocean can beautistic. Just people-fish.”
“What about dolphins? They’re mammals.”
“No,” Jemma laughs. “But they might have their own version.”
Caroline gives a noncommittalhum, then starts playing with Jemma’s hair.
Dr. Booth smiles at them. “Sosmart, that one. I think she takes after her parents.”
“Thank you again,” Jemma says,and then the three of them make their way out of the room.
As they’re walking out to thecar, Jemma watches Fitz, who hasn’t said anything.
“You’ll think about it?” sheasks.
“Yeah,” he replies. “I’ll thinkabout it.”
-
A month later, Jemma is sittingin their living room looking over some files, as Caroline lays on the floorlooking at a marine biology textbook. She doesn’t know how to read most of thewords (though she recognizes the shape of most of the species names), but shelikes looking at the pictures and diagrams.
The front door opens and closes,and Jemma looks up nervously.
“Fitz?” she calls.
“Just me,” is the response.
Her body relaxes, and she goes backto looking at the file as he takes off his shoes and hangs up his coat, thoughshe’s not really reading it. After a minute he joins them in the living room,plopping heavily onto the couch. There’s a set of papers clutched in one of hishands.
He’s quiet, and Jemma tries towait for him to speak, but after only a few seconds she can’t help herself.
“Well?” she asks. “What’d theysay?”
He uncurls the papers, and handsthem over. Jemma takes them, reading quickly.
Diagnosis: Autism SpectrumDisorder
She reads it again, then scanslower down on the page. There’s a lot about test results, results of theinterview, a lot of numbers that Jemma hasn’t started to unpack yet. But, thereit is. Plain as day.
“So,” she says.
“Yeah.”
“How are you feeling about it?”
He scoots down on the couch,tilting his head to rest against the back. He blows out a breath, fingerstwisting together on his stomach. “Relieved, I think.”
“Well … that’s good, isn’t it?This is a good thing.”
“It- It explains a lot of things.Things I’ve been confused about. Things that I didn’t necessarily have wordsfor, before. I just … I wish I’d known sooner.”
“Do you think it would’vehelped?”
“Yeah,” he admits softly. “I-SHIELD knew. I called Coulson and asked, it’s been on my file since theAcademy.”
Jemma’s brows furrow. “They knewand never told you?”
He shakes his head, eyes on theceiling. “Wasn’t in the policy to tell, I guess. And Coulson just assumed Iknew already.”
“Well, in any case,” Jemma says, “youknow now, and that’s what’s important. And, can I just say, I’m really proud ofyou for doing this. I know it was scary, but you went through with it anyway,and I think that was really brave. And I think this is going to be a goodthing, getting to learn more about yourself.”
“Yeah.” Fitz finally turns tolook at her. “Yeah, I think this is going to be a good thing, too.”
“And,” Jemma adds, “it’s justanother way that you can relate to our daughter.”
“That’s true,” Fitz says,smiling, and then scoots off the couch to settle on the floor in front ofCaroline. “Did you hear, monkey? Daddy’s autistic, too. We have the same kindof brain.”
“Shovelhead sharks clonethemselves,” Caroline replies, still looking at her book. “So they’d have thesame kind of brain, too.”
“That’s true.” Fitz nods. “Theywould. I didn’t clone myself, though. You can tell because you’re much cuterthan me.”
“She does have the curls,” Jemma points out.
“That she does.” He grins. “Oneof the many wonderful things she gets from me.”
“She gets some things from me,” Jemma quips, as he moves to sit back on thecouch next to her, grabbing up her hand. “Like her love of biology.”
“Ah- Love of animals,” Fitz shootsback, a teasing grin on his face. “Still from me.”
“I like animals.”
“You like dissecting them, Jem,that’s different.”
“Fine. What about her love oftidiness? That definitely comes from me.”
“Well … I do keep my lab verytidy. But she also keeps her room clean, which I do not, so sure, I’ll give youthat one.”
Jemma beams. “Hah. I knew therewas something.”
Fitz smiles, but eventually itdrops. “Do you … Do you think this is gonna change anything?”
Jemma tilts her head, peering athim. “Like what?”
“Dunno,” Fitz mumbles.
“I don’t think it’ll changeanything unless you want them to change.”
“If I do … d’you think that’sbad?”
“No,” Jemma assures him. “How youthink of yourself is going through a change, I don’t think it’s bad if you wantother things to change along with it. If anything, it might change how open youare with certain things about yourself. And how you think those things deserveto be treated.”
“Caroline … She’ll have names forall these things. She’ll understand it. Understand herself, better than I did.”
“Yes, she will.”
“And- And I’m glad we know, now.So we can give her the best life she can have.”
Jemma raises their conjoinedhands to press a kiss to the back of his. “You’re already a great dad, Fitz. You’realready giving her an amazing life. But yes, this will make things easier, nowthat we know.”
Fitz ducks his head, smiling, andthen turns to Caroline. “Hey, monkey, do you want to watch Finding Nemo? Youcan tell us all the species names when they come on screen.”
Caroline immediately jumps up,her hands flapping at her sides. “Yes, yes, yes!”
Fitz gets up to put in the DVD,and on his way back scoops Caroline off the floor and plops her onto his lap ashe settles back onto the couch. She presses back against him, picking up hishand so she can play with his fingers as she watches. Jemma leans against hisside, resting one hand on his leg.
“Amphiprion ocellaris,”Caroline says as the movie starts.
Fitz presses a kiss againsther hair. “Good job, monkey. Good job.”
#aosficnet#buskidsnet#lmao this is .... educational like i said#i hope it's not too boring#just wanted to really be able to explain some key things so that fitz has a base to go off of#also!! the kid is named after caroline herschel btw#because you know they would#and her special interest is ocean life because i'm mean and like irony :) :)#anyway enjoy!#leo fitz#jemma simmons#aos#fitzsimmons#unlessimwrongwhichyouknowimnot
45 notes
·
View notes
Last Seen Blogs

weki8meki
ma

the-queen-in-yell0w
☀Midnight Sun☀

mickmathersartblog
MickMathersARTblog

calissarowan
Calissa Rowan

reactnative7
Untitled