#or all the non-death non-long covid health side effects that can result from a covid infection even in asymptomatic and mild cases
Text
Covid is still killing more Americans than all opioids combined, each week (2024).
We are supposed to "go back to normal" and "don't worry about Covid", despite it having a higher death toll on average.
Unlike opioid drugs, Covid can effect literally anyone.
Even the vaccinated are still at some risk of infection, though the new updated shots are much better at preventing breakthrough infections.
Why so many in government and the media are willing to ignore the reality of Covid when it's still worse than the opioid crisis is beyond me.
#covid isn't over#tw: drugs#tw: opioids#and this isn't even touching the reality of Long Covid#or all the non-death non-long covid health side effects that can result from a covid infection even in asymptomatic and mild cases#back to normal#covid denial
166 notes
·
View notes
Text
1. Vaccine data on preventing disease
I will start this post by summarizing (hopefully as simply as I can) a handful of studies pertaining to how well the vaccines work at preventing disease. I will start by looking at some of the early vaccine studies for the mRNA vaccines (as these are the ones I have researched most heavily). These are older studies done back before vaccine distribution really got big. In fact, I remember doing a journal club meeting on one of these articles sometime late last fall.
The first is one of the Pfizer studies. This one excluded people with compromised immunity which I understand, but angered me greatly when it came out (as a person with compromised immunity). Note that it was designed and funded by Pfizer, though when you look at the protocol and stats it appears well-designed. Like other studies discussed here, infection with COVID-19 used the FDA definition which is a positive test with at least one symptom (which can be basically anything). However, in summary, they found that a 2-dose regimen offered 95% protection against COVID-19 infection per the above definition. (SOURCE)
The second study (on Moderna) was funded by the Biomedical Advanced Research and Development Authority and the National Institute of Allergy and Infectious Diseases, and the study protocol was designed by Moderna with their assistance. This study also used the FDA definition of COVID-19 as a positive test with a symptom and excluded the immune compromised. However, it found that a vaccination was 94.1% efficacious in preventing COVID-19 infection. (SOURCE)
Now that that part is out of the way I wanted to go over some more real-world data; that is, how are these vaccines actually functioning out there? Are they working on a population level like these studies suggest they ought to? Well...
The Morbidity and Mortality Weekly Report from April through July of 2021 shows that vaccination reduces chances of catching COVID 5 fold. This report was important in examining how the vaccines are responding since the delta variant of COVID-19 has started to surge. (SOURCE)
A study out of California found in July of 2021 that COVID-19 infection rates in unvaccinated people are ~5X higher than in vaccinated people. (SOURCE) They do raise the concerns that more studies are needed on how long immunity lasts and whether it will wane.
Another study examined COVID-19 vaccination effectiveness among health care workers, a group that is heavily exposed to COVID-19. They looked at whether the vaccines would prevent disease (in their study, defined as a positive test with at least one symptom). They specifically looked at the mRNA vaccines (Pfizer, Moderna). The study found "a single dose...to be 82% effective against symptomatic COVID-19 and 2 doses to be 94% effective." (SOURCE)
And before you say "but those were only symptomatic cases!" here is another study also looking at health care workers. This study spanning December 2020-March 2021 basically tested all of their enrollees for 13 weeks and found that those who received 1 vaccine dose had 80% lower chances of getting COVID, while those with 2 doses had a 90% lower chance of getting COVID. This testing was done regardless of symptom burden. (SOURCE)
There is ongoing data collection on how long immunity lasts with some new reports (warning - following study is not yet peer reviewed) suggests that vaccine efficacy may drop to ~85% after 6 months in preventing disease, but efficacy in preventing severe disease remains very high, at 97%. Still, though, 85% is pretty good. (SOURCE)
So here are just a TEENY TINY number of the many studies coming out regarding the vaccines. I could sit here and list so many more, but then this post would be way too bloated and repetitive because they all say the same thing: the vaccine works. This conclusion is both consistent and reproducible, which when talking about scientific studies, means there is some good research backing it up. And before anyone says anything--YES, you can still catch COVID after getting a vaccine. Nothing works 100% of the time. Just because my car has an air bag and I use seat belts doesn't mean I won't get injured if I crash my car. But based on the available data, it works well in preventing infection in a lot of people, and furthermore, there is one other MAJOR benefit to the vaccine which I will discuss below.
2. Vaccine data on preventing severe disease:
Probably the most important realization that has come out of the past few months is our understanding of how robustly these vaccines effect disease course and severity. I am from eastern KY so one of the big hospital systems in my area is Appalachian Regional Health, which spans 13 facilities. According to their latest stats, they have 213 patients hospitalized with COVID-19. Of those, 16 are vaccinated. That means a little over 92% of the COVID patients there sick enough to need hospitalized are unvaccinated. For further reference, another major hospital in the region, Pikeville Medical, today reported that 70 of their 88 hospitalized COVID patients (~80%) are unvaccinated, and 20 their 24 (83%) ICU COVID-19 patients are unvaccinated. Another regional hospital, Kings Daughters, had recently reported that 86.5% of those hospitalized with COVID are unvaccinated and 100% of COVID patients in their ICU are unvaccinated. So before I even get to national statistics, you can look at these numbers as already see a trend, and I would hope you can see that these numbers are way too high and too consistent to be coincidence. For sources on these numbers you can visit the ARH, PMC, & KDMC websites or facebook pages where they post their stats (HERE, HERE, and HERE)
Now to post a few studies backing this up:
A recent CDC Morbidity and Mortality Weekly Report (we talked about this one earlier) shows that vaccination reduces chances of hospitalization due to COVID-19 by ten fold. (SOURCE) The same report shows that vaccination reduces the risk of death due to COVID-19 by ten fold, as well!
Another recent study that incorporated delta variant data into their research has found that "unvaccinated adults aged ≥18 years are 17 times more likely to be hospitalized compared with vaccinated adults." (SOURCE).
Another study coming out of California, also post-delta surge, showed similar results, with hospitalization rates ~29X higher in unvaccinated people. (SOURCE)
Another study looked at how the vaccine protects adults over age 65, which is going to be a more vulnerable group. It found that adults >65 who received 1 dose of a COVID vaccine saw a 64% reduction in hospitalization if they contracted disease, and those with 2 doses saw a 94% reduction in hospitalization with disease. (SOURCE)
To me, studies like these are really important. What we are seeing over and over again right now is that our health care system is being absolutely flooded by unvaccinated COVID patients who need to be hospitalized. This is stressing the health system in ways it was not built to endure. We do not have enough equipment or staff to manage the volume of patients we are seeing.
Sadly, this does not just affect COVID patients. When a bunch of unvaccinated people get sick and take up ICU beds, that means anyone who gets sick with non-COVID problems, like strokes and heart attacks, also suffer when there aren't beds left for them. For example, your grandmother who developed a bad bacterial pneumonia and is in respiratory distress may die because an unvaccinated COVID-19 patient got there first and took the last vent in the hospital, and there aren’t any ICU beds to transfer her to nearby because the wait lists are all so long because all the ICUs are also filled with unvaccinated COVID patients. I'd argue this is the biggest problem we are facing right now regarding the pandemic even if this problem is invisible to people who don't work in healthcare. Please believe me when I say this: we are drowning, and we are drowning because of unvaccinated COVID patients who are getting severely ill. This is completely unnecessary and avoidable when we are seeing over and over again that vaccination does wonders to prevent you from getting sick enough to need the hospital at all.
Don’t believe me still? I want each of you reading this to visit the webpage for some of your local hospitals. Most of them are posting daily or weekly COVID admission and death statistics. Just take a look at them. Take a look at who is getting admitted and who is dying.
3. Vaccine safety:
Any vaccine, medication, herbal supplement, or what have you that goes into your body carries the risk of an adverse side effect. As a result each of us has to ask ourselves, do the potential benefits outweigh the potential risks? To answer that we need to better understand the risks associated with COVID-19 vaccination, and that means turning back to the data we have available.
According to NYT Vaccine Tracker, there have been 5.73 billion vaccine doses administered worldwide since its release. This generates an abundance of data for us to work with--more than we have for most medications you take every day--in regards to understanding safety profiles of these immunizations. Given that impressive number, we are by no means seeing widespread death or disability popping up due to the vaccine, but let's get more specific. We have seen a couple common possible adverse effects:
Flu-like symptoms: Most common by far is going to be flu-like symptoms or redness/pain at the injection site. This is actually a good side effect because it means that the vaccine is doing what it is meant to do. I won't talk much more about this one because I doubt flu-like symptoms are the reason people are scared of the vaccine. But for most of you, if you have any side effects at all, this will be as bad as it gets. You are more likely to have these symptoms after dose #2.
Anaphylaxis: Anaphylaxis can occur in anyone when you encounter a substance you have a try allergy to. This is going to be a rare side effect (2 to 5 people per million, or 0.00025%), but is also why you are asked to wait 15-30 minutes to be monitored after receiving your vaccine. That way if you show any signs of distress you can be given immediate treatment. Any time you get a vaccine or start a new medicine a severe allergy is a possible reaction, but if you already KNOW that you are highly allergic to something in the vaccine, you should not receive it.
TTP: This is a disorder that causes abnormal clotting or bleeding. It seems to be associated exclusively with the J&J or AstraZeneca adenoviral-vector vaccines based on current data trends. While rare, this is going to be the most serious adverse effect from the immunization. Data suggest the highest risk is for women under 50, but it is still remarkably rare with only 45 confirmed cases of TTP after over 14 million vaccine doses given. This is an incredibly, incredibly low incidence. Of note, however, patients with the actual COVID-19 virus have a SIGNIFICANTLY increased risk of clotting, especially in severe disease. This increased risk may be due to the production of auto-antibodies in response to COVID-19 infection. Summary: your risk of a blood clot is much higher with the actual virus than the vaccine.
Myocarditis/Pericarditis: These are conditions involving inflammation around the heart tissues or heart muscle. There does appear to be an increased rate of myo/pericarditis after vaccination. This is more common in teenaged males who received an mRNA vaccine (such as Moderna or Pfizer). This is also very rare. According to VAERS, 1404 cases of possible myo/pericarditis were reported after vaccination through September of 2021, though only 817 were able to be confirmed. A CDC report from June 2021 estimated about 60 cases of myo/pericarditis may develop per 1 million vaccine series completed (if you are male aged 12-17; otherwise the rate is lower). However, that same report also estimated the prevention of 71 ICU admissions, 2 death, and 215 hospitalizations among that same group per million vaccines given. Again it is a risk-benefit discussion, but here the numbers definitely point to a benefit overall. Vaccine-induced myocarditis and/or pericarditis are generally one-time events with an excellent prognosis, so rarely represent a threat to life. As the authors of the study linked above stated, "The absolute incidence was extremely low, cases were mild, and all patients recovered. Fear of myocarditis or pericarditis should not influence COVID-19 vaccine decisions."
Guillain-Barré Syndrome: This is a disorder of the nervous system that can cause temporary weakness and paralysis. It is commonly seen after immunizations or infections with various pathogens. It has been associated with adenovirus-vector vaccines (J&J, AstraZeneca) at a very low rate (about 0.0008%) with J&J reporting ~100 cases per 12.2 million doses per VAERS data, and 227 cases out of 51.4 million doses given per EU/EEA to the EMA again through June 2021. People with a history of Guillan-barre are more likely to get it again, so your risk is probably slightly higher if you have had issues with this before, so people with this history may want to opt for an mRNA vaccine which has not been associated with this.
4. Addressing Common Concerns
If the vaccine works, why do you feel unsafe if I don't get it? A vaccinated person is more protected from you than if they were not vaccinated, but no vaccine (or medical treatment in general) works 100% of the time, so there is always a risk of spreading disease no matter what. This is true for every single vaccine in history so COVID shots aren't special in this way. The data supports indisputibly that the vaccine reduces the RISK of getting COVID, but does not protect against it perfectly, so people should still use common sense. Also, vaccine works much, much better when everyone gets them, which is why vaccinated people enourage others to get the shot too. Think about it. Most of the studies I linked said the vaccines were in the range of 90-95% effective at preventing disease. If everyone in the room is vaccinated, the chances any of them (with their 90-95% protection) are infected and spreading COVID is going to be lower than a room of unvaccinated people, who have no protection against disease. Think now of yourself as a vaccinated bystander inside each of those rooms. In room 1, there is a low rate of COVID-19 being spread around, so your vaccine-induced immunity is now bolstered by the fact that there is also low spread in the community, making your overall chances of getting sick extremely low. In room 2 there is likely moderate to high spread of COVID-19 virus, meaning that even if you are vaccinated, because your vaccine can never be 100% effective, you sadly still have a chance of getting sick (even if it is lower than it would be if you were not vaccinated). Does that make sense?
If vaccines work, why do I have to wear a mask? Same reason as above. We can get into masks later, but point is, both offer protection against the spread of COVID-19, but neither is 100% surefire perfect immunity. Human bodies just don't work that way, sadly. By using both, you increase your chances of preventing catching or spreading disease more than if you did either one in isolation. Bringing back the car example, a seat belt is good, an air bag is also good, but I'd definitely prefer to get a car that has both a seat belt AND an air bag.
Why is the vaccine not approved for kids? Lacking data on safety and efficacy, as young children were excluded from many of the trials that looked at these vaccines.
We don't have long term safety data. It is unprecedented for an immunization to cause new side effects years later. These shots work by activating your immune system. Any problems they are going to cause will occur surrounding that period of immune activation (meaning, at most a few weeks after you get it). That is why this vaccines typically have any side effects show up within days to weeks of administration. The idea that novel side effects will pop up YEARS later is unlikely. Now, a vaccination may have cause side effect that has long-lasting health implications, such as developing TTP and having a stroke from it, but my point is that will start within weeks of vaccination, not randomly 5 years later after the vaccine has long since left your system. As a result, any side effects from the vaccine are things we will already be seeing right now. The virus, though... I can tell you that scar tissue in lungs doesn't magically vanish, and brain damage from hypoxia doesn't vanish. I can tell you that those who develop a generalized COVID inflammatory response are dealing with symptoms months post-infection. I can tell you that the virus itself is causing irreversible health problems and disability, and we KNOW that right now without waiting another 5 years. And we know that being unvaccinated increases your risk of getting sick enough to have these permanent disabilities. We also don't have time to wait 5-10 years on more data to deal with this problem. Action has to be taken now, or a lot of people won't be alive in 5 years to talk about the long term effects. I wish none of this had ever happened, but it did, and we have to do something or it won't get any better. This is a global pandemic; we have to cooperate with each other to eradicate it.
Vaccines should not be mandated by the state or companies. I don't really disagree. I do not think authority figures should be able to tell any person that they have to put any substance into their body against their will or else face starvation or homelessness, which is a real threat if people get fired over their vaccine status. HOWEVER neither your nor my beliefs on this topic change the fact that the vaccine works and is VITAL to keeping our health system from collapsing, and you really should be choosing to get it on your own based on the available data regardless of what your boss is saying. Please don't refuse to get the vaccine just to "send a message" or take a stand against your boss or whoever, because I promise you they will fire you without a second thought, and the only person you are sending a message to is that little grandma we talked about earlier who needs intubated but can't find a free vent or ICU bed, so dies in the emergency room while unvaccinated people take up all the space in the hospital.
5. In Summary
There are risks associated with COVID-19 vaccination, as with any vaccine or medicine, but they are remarkably, remarkably low. The potential benefits of vaccination are significant, with a decreased risk of infection, hospitalization, and severe disease among those who are vaccinated. This benefit extends to the community as well, in that it means you are less likely to catch (and therefore spread) COVID-19, increase the rate of herd immunity in your area which protects everyone (especially the medically vulnerable), and reduces preventable, unnecessary COVID-19 admissions that are weighing down the health system and clogging up hospital beds. If you look at this purely from a risk-benefit standpoint there is no mathematical reason not to favor getting the vaccine, and I strongly urge everyone who can safely do so to schedule it.
I suppose my take-away statement is this: I am a physician. If you are willing to trust my advice when you show up to the hospital in respiratory distress, trust my advice now in trying to prevent you from getting to that point.
Please.
#covid-19#pandemic#covid vaccine#covid-19 vaccination#medblr#medical#population health#preventative medicine
218 notes
·
View notes
Note
Do you believe the SPN writers owed us the "right" ending? (This is a serious question!) And if so, what was it? Would you require a "happily ever after" for all the characters involved? Is the mental health of the audience a priority when creating a story? I know, a lot of thoughts, but I'm v curious!
Well, I think any writers of any show owe their audience the “right” ending. That being said, I still firmly believe that what we got as an ending (that englobes 19 and 20, btw) resulted from corporate fuckery rather than from the writers shooting themselves in the head with their own gun. If you’ve been attentive enough for the past few seasons, you’d have noticed the theme and the clear meta storylines being laid out by the writing team, and the way season 15 all up to episode 18 was absolutely, utterly, completely following that path. The way both episodes 19 and 20 can be separated from the rest of the season is a clear hint at what happened, and that’s also why it can be this easily disregarded.
Now, back to your question. To me, the right ending involved several things.
Dean getting to speak his truth: not only did that involved the situation with Cas needing to be addressed in any way, but that also involved getting Dean to let go. To me, Dean was always going to die at the end. What I didn’t picture was his death being this meaningless, on an insignificant hunt, only with Sam by his side, delivering a 5 minutes speech that could’ve been avoided in favor of calling a goddamn ambulance to save his life. I expected something along the lines of Sam and Dean raiding Heaven in their final battle against Chuck, and at the end of it Dean choosing to stay behind, choosing the Afterlife and having something with Cas while Sam went back to Earth to live his life as the Leader he was always supposed to be. Which brings me to my second point.
Sam rising up to the leadership position he was always supposed to get: I think I made a post sorely for this at some point, but long story short Sam’s storyline has been carefully crafted since season 1 to end at a point where Sam was supposed to become the leader of this big old hunter family in America. Yet, he ends up closing up the bunker (effectively turning down everything he’s worked for for the past 3 decades of his life, everything Dean, Cas and their entire extended family fought for), and runs off to live a meaningless life with a blurry wife and a proxy kid he names after his brother. This is nowhere close to anything they’ve ever laid out for Sam’s path, and I don’t even understand how Sam stans can be okay with where he ended up. He spends the last 4 decades of his life mourning his brother and turning his back on everything the show made a point of crafting for him. He never becomes the leader he was supposed to. He never gets back to Eileen. He apparently forgets everything about the past two decades of his life. Again, the show makes a point of telling us “you thought what we showed you for 15 seasons was real? Well, here’s our #1 character turning his back on everything we made a point of carefully tell, because non of it mattered”
Cas’ place in the finale: Parts of what makes no sense is the fact that Cas disappears in the Empty after ep. 18 and nothing about it gets addressed later on. I’m not even talking about Misha being in the episodes, because if Covid really was the excuse here (hint, it’s not, but bear with me regardless) there were SO MANY easy ways to explains this storyline without needing Misha to be on screen. You’re telling me there was no way to grab an extra to wear one of the trenchcoats and sit next to Jensen in the Impala? You’re telling me there was no way of adding ADR at the end of 20 to add a simple “Hello Dean” to the scene, before Sam appears in Heaven? You’re telling me there was no way of having a Winbros conversation about what happened? Castiel’s absence makes no sense, if not for the fact that he’s been a core character of the show for 12 years, and not having him at the end felt like a punch to the guts. Castiel was also deeply linked to Dean’s character arc, and his absence leaves Dean’s storyline entirely incomplete (which, I may have to add, is completely hysterical judging by the fact that he’s literally the second main character of the show). I’m not gonna go on and on, but basically I pictured Castiel being there when Dean came along, and being part of the reason Dean makes a choice of staying instead of going back.
There are a lot more things to say. The complete disappearance of Eileen in favor or Sam getting a blurry wife. The complete erasure of the Found Family angle they made a point of cultivating for so long. Basically, 19 and 20 felt like the whole series being ripped away to pieces and the show telling us that it was all a lie. The “right” ending, to me, involved Sam and Dean finally being at peace. It involved Sam finding Eileen again and working up to the leadership position he was always supposed to get. It involved Dean finally making a choice for himself instead of thinking as a 2-unit with Sam. It involved Dean speaking his truth to Cas. It involved the co-dependence finally being bid goodbye.
Would you require a "happily ever after" for all the characters involved?
No, because at the end of the day this is Supernatural, this is not necessarily the picture-perfect show for a “happily ever after”. That being said, you can have a satisfying ending without it being happily ever after. Dean choosing to stay in Heaven is essentially Dean choosing to metaphorically die. Sam and Dean finally going their own way in different realms is fulfilling and satisfying, but doesn’t really qualify as a happily ever after either.
Is the mental health of the audience a priority when creating a story?
Good fucking lord, YES. It SHOULD BE a priority. I assume this is in relation to something I wrote a while back, where I basically said that the ending they wrote was dangerous. And I stand by it. This ending sent so many wrong messages to the audience of a beloved 15-year-old show. “We made you think that family didn’t end in blood? Well, we lied, and that’s why the ending of Supernatural will consist of sorely Sam and Dean, with the meaningful appearance of OG Bobby at the end of it”; “Speak your truth and you will be silenced”; “you’ll never be free from trauma so it’s better to just choose to bleed to death and die”. I think I could go on for hours, but you get the idea. This ending was dangerous, and I wish they’d considered the trauma that would unleash on their own fandom because it’s making me insane. I’m glad I’m at a point in my life where I can take care of myself, but a couple of years back that would have been enough to set me back on my own destructive path. And it’s making me sick to think that it probably did put many fans down to the point where it fucked with their sanity.
Yes, it should be a priority. Obviously, it wasn’t a priority when crafting an ending for Supernatural.
Sorry, that got excruciatingly long. I hope that answered part of your questions, but feel free to reach out for more!
#at this point i feel like this ending is going to drive me insane for years#corporate fuckery#spn finale#finale fuckery#is this meta?#idk#jus.meta#spn 15x19#spn 15x20
73 notes
·
View notes
Text
A Guide to Outpatient COVID Treatment: Step-By-Step Doctors’ Plan That Could Save Your Life
Recently, Dr. Peter McCullough, MD, of Baylor University Medical Center in Dallas testified to Texas Senate HHS Committee about how mass media and even some government agencies are silencing clinical outpatient evidence for effective treatment of COVID19 and instead push vaccines only (video shown below).
Treatments like those mentioned by Dr. McCullough can be found in sites like https://c19early.com/ but specifically, McCullough refers to the following Appendix to a document published by Association of American Physicians and Surgeons (AAPSonline.org) as an educational resource. It is based on a paper published in American Journal of Medicine (link), by Dr. Peter McCullough and 22 other clinicians (MDs) and researchers (PhDs).
“Seek early treatment and be your own advocate. All of the physicians contributing to this booklet are on the frontlines treating outpatients at the first signs of COVID illness. Studies in the US and many other countries clearly show that patients who are treated within the first 5 days of symptoms have better outcomes using the combination of medications in the algorithm below.”

COVID-19 hospitalizations and death can be reduced with outpatient treatment.
Principles of COVID-19 outpatient care include: 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, 4) antiplatelet/antithrombotic therapy 5) administration of oxygen, monitoring, and telemedicine.
“For the ambulatory patient with recognized early signs and symptoms of COVID-19, often with nasal real-time reverse transcription or oral antigen testing pending, the following 4 principles could be deployed in a layered and escalating manner depending on clinical manifestations of COVID-19-like illness and confirmed infection: 1) reduction of reinoculation, 2) combination antiviral therapy, 3) immunomodulation, and 4) antiplatelet/antithrombotic therapy. Because the results of testing could take up to a week to return, treatment can be started before the results are known. For patients with cardinal features of the syndrome (ie, fever, body aches, nasal congestion, loss of taste and smell, etc.) and suspected false-negative testing, treatment can be the same as those with confirmed COVID-19. Future randomized trials are expected to confirm, reject, refine, and expand these principles. In this article, they are set forth in emergency response to the growing pandemic as shown in Figure 1 .
Treatment algorithm for COVID-19-like and confirmed COVID-19 illness in ambulatory patients at home in self-quarantine. BMI = body mass index; CKD = chronic kidney disease; CVD = cardiovascular disease; DM = diabetes mellitus; Dz = disease; HCQ = hydroxychloroquine; Mgt = management; O2 = oxygen; Ox = oximetry; Yr = year.
The basic groups of prescription medicines and other therapies used in COVID-19:
▪ Combination anti-viral medicines started as soon as symptoms occur ▪ Medicines to decrease inflammation, such as corticosteroids (called immunomodulators)
▪ Anticoagulant therapy to prevent blood-clots that can cause strokes, heart attacks, kidney shut-down, and death.
▪ Non-prescription supportive treatments with zinc, vitamin D, vitamin C, electrolyte drinks such as Pedialyte, and others.
▪ Home-based oxygen support, such as with an oxygen concentrator. These machines are available by physician prescription from home health medical supply businesses and are covered on most medical insurance plans.
I. Antiviral Agents:
These must be started quickly at STAGE I (Days 1-5):
Symptoms include sore throat, nasal stuffiness, fatigue, headaches, body aches, loss of taste and/or smell, loss of appetite, nausea, diarrhea, fever.
These medicines stop the virus from (1) entering the cells and (2) from multiplying once inside the cells, and they reduce bacterial invasion in the sinuses and lung:
▪ *Hydroxychloroquine (HCQ) with azithromycin (AZM) or doxycycline
OR
▪ Ivermectin with azithromycin (AZM) or doxycycline
Either combination above must also include zinc sulfate or gluconate, plus supplemental vitamin D, and vitamin C. Some doctors also recommend adding a B complex vitamin.
Zinc is critical. It helps block the virus from multiplying.
Hydroxychloroquine is the carrier taking zinc INTO the cells to do its job.
An educational resource from The Association of American Physicians and Surgeons (AAPSonline.org) 16
II. Anti-inflammatory Agents - Corticosteroids (“steroids”): Oral and Nebulized.
These are started at STAGE II (Days 3-14) to reduce inflammation, the cause of added damage to the lungs and critical organs. Symptoms include worsening cough, difficulty breathing, chest heaviness/tightness or chest pain.
As inflammation damages the airways interfering with normal oxygen-carbon dioxide exchange, blood oxygen levels drop and people experience loss of focus, drowsiness, confusion, difficulty concentrating, low energy and severe fatigue.
The exaggerated Inflammation response in COVID further increases the risk of blood clots.
Prescription medicines and other support added now to Stage I medicines are: ▪ nebulized budesonide to help penetrate the lungs and reduce inflammation ▪ oral prednisone, methylprednisolone, dexamethasone
▪ colchicine – may also be added to reduce inflammation
▪ full strength adult aspirin 325 mg to reduce inflammation and risk of blood clots ▪ home oxygen concentrator may be needed to improve oxygen levels (requires physician prescription)
III. Prescription Anticoagulants (“blood thinners”):
STAGE III (Day 7 and beyond): Symptoms seen in Stage II intensify. Difficulty breathing becomes extreme, oxygen levels drop sharply, risk of heart attack or stroke increases. At this point, people are critically ill.
The medicines to be added to Stage I and II medicines now include:
▪ Aspirin 325 mg unless told not to take by your doctors
▪ And/or low molecular weight heparin injections (e.g. enoxaparin [Lovenox]) OR
▪ apixaban (Eliquis), or rivaroxaban (Xarelto), or dabigatran (Pradaxa) or
edoxaban (Savaysa) in standard doses for 5 to 30 days
If these added steps do not lead to improvement, or the patient becomes unstable, a 911 call is warranted for ER evaluation and hospital admission so that more aggressive IV medications (such as remdesivir, Regeneron, and others) may be considered, and more intensive ventilation regimens are possible in ICU settings.
IV. Vitamins, Supplements, and Oxygen.
▪ Zinc sulfate, gluconate or citrate. These forms are available in pharmacies, health food stores, and sold online. Zinc sulfate 220 mg provides 50 mg elemental zinc, the recommended anti-viral dose. Zinc in the form of zinc picolinate form is not recommended following reports of liver damage and tumors from studies about 20 years ago. Following these reports, the German Commission E that regulates supplements used in medical practice in Germany banned this form of zinc.
An educational resource from The Association of American Physicians and Surgeons (AAPSonline.org) 17
▪ Vitamin D3, preferable in oil in capsules for better absorption. Recommended doses for anti-viral benefit vary from 5000 IU or more for 5-30 days
▪ Vitamin C with bioflavonoids for antioxidant, anti-inflammatory effects. Dose
recommendations from our contributors vary from 1000 mg (1 gram) once or twice a day up to 4 or more times a day.
▪ A word about quercetin. Some physicians are recommending this supplement to reduce viral illnesses because quercetin acts as a zinc ionophore to improve zinc
uptake into cells. It is much less potent than HCQ as a zinc transporter, and it does
not reach high concentrations in lung cells that HCQ does. Quercetin may help
reduce risk of viral illness if you are basically healthy. But it is not potent enough to replace HCQ for treatment of COVID once you have symptoms, and it does not
adequately get into lung tissue unless you take massive doses (3-5 grams a day),
which cause significant GI side effects such as diarrhea.
Control of Contagion
A major goal of self-quarantine is the control of contagion. Many sources of information suggest the main place of viral transmission occurs in the home. Facial covering for all contacts within the home as well as frequent use of hand sanitizer and hand washing is mandatory. Sterilizing surfaces such as countertops, door handles, phones, and other devices is advised. When possible, other close contacts can move out of the domicile and temporarily stay with others not ill with SARS-CoV-2. Findings from multiple studies indicate that policies concerning control of the spread of SARS-CoV-2 are effective and extension into the home as the most frequent site of viral transfer is paramount.
Reduction of Self-Reinoculation
It is well-recognized that COVID-19 exists outside the human body in a bioaerosol of airborne particles and droplets. Because exhaled air in an infected person is considered to be “loaded” with inoculum, each exhalation and inhalation is effectively reinoculation. In patients who are hospitalized, negative pressure is applied to the room air largely to reduce spread outside of the room. We propose that fresh air could reduce reinoculation and potentially reduce the severity of illness and possibly reduce household spread during quarantine. This calls for open windows, fans for aeration, or spending long periods of time outdoors away from others with no face covering to disperse and not reinhale the viral bioaerosol.
Combination Antiviral Therapy
Rapid and amplified viral replication is the hallmark of most acute viral infections. By reducing the rate, quantity, or duration of viral replication, the degree of direct viral injury to the respiratory epithelium, vasculature, and organs may be lessened. Additionally, secondary processes that depend on viral stimulation, including the activation of inflammatory cells, cytokines, and coagulation, could potentially be lessened if viral replication is attenuated. Because no form of readily available medication has been designed specifically to inhibit SARS-CoV-2 replication, 2 or more of the nonspecific agents listed here can be entertained. None of the approaches listed have specific regulatory approved advertising labels for their manufacturers; thus all would be appropriately considered acceptable “off-label” use.
Zinc Lozenges and Zinc Sulfate
Zinc is a known inhibitor of coronavirus replication. Clinical trials of zinc lozenges in the common cold have demonstrated modest reductions in the duration and or severity of symptoms. By extension, this readily available nontoxic therapy could be deployed at the first signs of COVID-19. Zinc lozenges can be administered 5 times a day for up to 5 days and extended if needed if symptoms persist. The amount of elemental zinc lozenges is <25% of that in a single 220-mg zinc sulfate daily tablet. This dose of zinc sulfate has been effectively used in combination with antimalarials in early treatment of high-risk outpatients with COVID-19.
Antimalarials
Hydroxychloroquine (HCQ) is an antimalarial/anti-inflammatory drug that impairs endosomal transfer of virions within human cells. HCQ is also a zinc ionophore that conveys zinc intracellularly to block the SARS-CoV-2 RNA-dependent RNA polymerase, which is the core enzyme of the virus replication. The currently completed retrospective studies and randomized trials have generally shown these findings: 1) when started late in the hospital course and for short durations of time, antimalarials appear to be ineffective, 2) when started earlier in the hospital course, for progressively longer durations and in outpatients, antimalarials may reduce the progression of disease, prevent hospitalization, and are associated with reduced mortality. In a retrospective inpatient study of 2541 patients hospitalized with COVID-19, therapy associated with an adjusted reduction in mortality was HCQ alone (hazard ratio [HR] = 0.34, 95% confidence interval [CI] 0.25-0.46, P <0.001) and HCQ with azithromycin (HR = 0.29, 95% CI 0.22-0.40, P <0.001). HCQ was approved by the US Food and Drug Administration in 1955, has been used by hundreds of millions of people worldwide since then, is sold over the counter in many countries, and has a well-characterized safety profile that should not raise undue alarm. Although asymptomatic QT prolongation is a well-recognized and infrequent (<1%) complication of HCQ, it is possible that in the setting of acute illness symptomatic arrhythmias could develop. Data safety and monitoring boards have not declared safety concerns in any clinical trial published to date. Rare patients with a personal or family history of prolonged QT syndrome and those on additional QT prolonging, contraindicated drugs (eg, dofetilide, sotalol) should be treated with caution and a plan to monitor the QTc in the ambulatory setting. A typical HCQ regimen is 200 mg bid for 5 days and extended to 30 days for continued symptoms. A minimal sufficient dose of HCQ should be used, because in excessive doses the drug can interfere with early immune response to the virus.
Azithromycin
Azithromycin is a commonly used macrolide antibiotic that has antiviral properties mainly attributed to reduced endosomal transfer of virions as well as established anti-inflammatory effects. It has been commonly used in COVID-19 studies initially based on French reports demonstrating markedly reduced durations of viral shedding, fewer hospitalizations, and reduced mortality combination with HCQ as compared to those untreated. In the large inpatient study (n = 2451) discussed previously, those who received azithromycin alone had an adjusted HR for mortality of 1.05, 95% CI 0.68-1.62, and P = 0.83.23 The combination of HCQ and azithromycin has been used as standard of care in other contexts as a standard of care in more than 300,000 older adults with multiple comorbidities. This agent is well-tolerated and like HCQ can prolong the QTc in <1% of patients. The same safety precautions for HCQ listed previously could be extended to azithromycin with or without HCQ. Azithromycin provides additional coverage of bacterial upper respiratory pathogens that could potentially play a role in concurrent or secondary infection. Thus, this agent can serve as a safety net for patients with COVID-19 against clinical failure of the bacterial component of community-acquired pneumonia. The same safety precautions for HCQ could be extended to azithromycin with or without HCQ. Because both HCQ and azithromycin have small but potentially additive risks of QTc prolongation, patients with known or suspected arrhythmias or taking contraindicated medications or should have more thorough workup (eg, review of baseline electrocardiogram, imaging studies, etc.) before receiving these 2 together. One of many dosing schemes is 250 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection.
Doxycycline
Doxycycline is another common antibiotic with multiple intracellular effects that may reduce viral replication, cellular damage, and expression of inflammatory factors. This drug has no effect on cardiac conduction and has the main caveat of gastrointestinal upset and esophagitis. As with azithromycin, doxycycline has the advantage of offering antibacterial coverage for superimposed bacterial infection in the upper respiratory tract. Doxycycline has a high degree of activity against many common respiratory pathogens including Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, anaerobes such as Bacteroides and anaerobic/microaerophilic streptococci and atypical agents like Legionella, Mycoplasma pneumoniae, and Chlamydia pneumoniae. One of many dosing schemes is 200 mg po followed by 100 mg po bid for 5 days and may extend to 30 days for persistent symptoms or evidence of bacterial superinfection. Doxycycline may be useful with HCQ for patients in whom the HCQ-azithromycin combination is not desired.
Favipiravir
Favipiravir, an oral selective inhibitor of RNA-dependent RNA polymerase, is approved for ambulatory use in COVID-19 in Russia, India, and other countries outside of the United States.35 It has been previously used for treatment of some life-threatening infections such as Ebola virus, Lassa virus, and rabies. Its therapeutic efficacy has been proven in these diseases. Like, the antimalarials and antibiotics, favipiravir has no large-scale randomized trials completed at this time, given the short time frame of the pandemic. A dose administration could be 1600 mg po bid on day 1, following by 600 mg po bid for 14 days.
Immunomodulators
The manifestations of COVID-19 that prompt hospitalization and that may well lead to multiorgan system failure are attributed to a cytokine storm. The characteristic profile of a patient acutely ill with COVID-19 includes leukocytosis with a relative neutropenia. These patients have higher serum level of cytokines (ie, TNF-α, IFN-γ, IL-1β, IL-2, IL-4, IL-6, and IL-10) and C-reactive protein than control individuals. Among patients with COVID-19, serum IL-6 and IL-10 levels appear even more elevated in the critically ill. As with any acute inflammatory state, early treatment with immunomodulators is expected to impart greater benefit. In COVID-19, some of the first respiratory findings are nasal congestion, cough, and wheezing. These features are due to excess inflammation and cytokine activation. Early use of corticosteroids is a rational intervention for patients with COVID-19 with these features as they would be in acute asthma or reactive airways disease. The RECOVERY trial randomized 6425 hospitalized patients with COVID-19 in a 2:1 ratio to dexamethasone 6 mg po/IV daily for up to 10 days and found dexamethasone reduced mortality (HR = 0.65, 95% CI 0.51-0.82, P <0.001). One potential dosing scheme for outpatients starting on day 5 or the onset of respiratory symptoms is prednisone 1 mg/kg given daily for 5 days with or without a subsequent taper.
Colchicine
Colchicine is a nonsteroidal antimitotic drug that blocks metaphase by binding to the ends of microtubules to prevent the elongation of the microtubule polymer. This agent has proven useful in gout and idiopathic recurrent pericarditis. The GRECCO-19 randomized open-label trial in 105 hospitalized patients with COVID-19 found that colchicine was associated with a reduction in D-dimer levels and improved clinical outcomes. The clinical primary end point (2-point change in World Health Organization ordinal scale) occurred in 14.0% in the control group (7 of 50 patients) and 1.8% in the colchicine group (1 of 55 patients) (odds ratio, 0.11; 95% CI, 0.01-0.96; P = 0.02). Because the short-term safety profile is well understood, it is reasonable to consider this agent along with corticosteroids in an attempt to reduce the effects of cytokine storm. A dosing scheme of 1.2 mg po, followed by 0.6 mg po bid for 3 weeks can be considered.
Antiplatelet Agents and Antithrombotics
Multiple studies have described increased rates of pathological macro- and micro-thrombosis. Patients with COVID-19 have described chest heaviness associated with desaturation that suggests the possibility of pulmonary thrombosis. Multiple reports have described elevated D-dimer levels in acutely ill patients with COVID-19, which has been consistently associated with increased risk of deep venous thrombosis and pulmonary embolism. Necropsy studies have described pulmonary microthrombosis in COVID-19. These observations support the notion that endothelial injury and thrombosis play a role oxygen desaturation, a cardinal reason for hospitalization and supportive care. Based on this pathophysiologic rationale, aspirin 81 mg daily can be administered as an initial antiplatelet and anti-inflammatory agent. Ambulatory patients can be additionally treated with subcutaneous low-molecular-weight heparin or with short-acting novel anticoagulant drugs in dosing schemes similar to those use in outpatient thromboprophylaxis. In a retrospective study of 2773 inpatients with COVID-19, 28% received anticoagulant therapy within 2 days of admission, and despite being used in more severe cases, anticoagulant administration was associated with a reduction in mortality (HR = 0.86 per day of therapy, 95% CI: 0.82-0.89; P <0.001). Additional supportive data on the use anticoagulants reducing mortality has been reported in hospitalized patients with elevated D-dimer levels and higher comorbidity scores.53 Many acutely ill outpatients also have general indications for venous thromboembolism prophylaxis applicable to COVID-19.
Delivery of Oxygen and Monitoring
Because ambulatory centers and clinics have been reticent to have face-to-face visits with patients with COVID-19, telemedicine is a reasonable platform for monitoring. Clinical impressions can be gained with audio and video interviews by the physician with the patient. Supplemental information, including vital signs and symptoms, will be important to guide the physician. A significant component of safe outpatient management is maintenance of arterial oxygen saturation on room air or prescribed home oxygen under direct supervision by daily telemedicine with escalation to hospitalization for assisted ventilation if needed. Self-proning could be entertained for confident patients with good at-home monitoring.
Many of the measures discussed in this article could be extended to seniors in COVID-19 treatment units in nursing homes and other nonhospital settings. This would leave the purposes of hospitalization to the administration of intravenous fluid and parenteral medication, assisted pressure or mechanical ventilation, and advanced mechanical circulatory support.”
youtube
This is the group’s statement on vaccines:
“Vaccines in Development:
Several vaccine models are being investigated for SARS-CoV-2 (COVID-19) including DNA and RNA vaccines. These vaccines take genetic information from other sources that is introduced into the cells. This information includes instructions to produce a SARS2-like viral antigen itself, and the immune system then reacts to it to develop immunity to the virus.
The most important consideration before approving a vaccine for human use is to make sure that the vaccine is safe and effective. Developing safe and controlled infection models for humans normally takes many years of phased testing in the lab and then in humans. Many physicians and scientists have been concerned that vaccine manufacturers, with government support, are speeding up this process in ways that are not allowing adequate time for the usual phased testing leading up to human clinical trials. Two vaccine manufacturers already have voluntarily paused their clinical trials in people due to serious adverse events.
Currently, there are no RNA-based vaccines approved for human use so it would seem prudent to take the time needed to ensure safety. Vaccines for RNA viruses are notoriously challenging and difficult to develop. We still, after all these years since AIDS emerged in the 1980s, do not have a vaccine for the AIDS virus, or the SARS-1 coronavirus that emerged in 2002-2003, and both are RNA viruses.
Several attempts have been made to create vaccines for coronavirus and other respiratory viruses but none of the vaccines have survived the testing phases. The vaccine trials for SARS-1 from 2003, for example, was shut down because it produced autoimmune hypersensitivity reactions when exposed to the natural virus after immunization in animal studies.
Another problem is that the SARS-2 virus has already shown many mutations. Viruses adapt to the environment to survive. Like the flu virus, it is difficult to predict what mutations will occur and circulate around the world each season. A new vaccine must be reformulated to adjust to the changing genetic makeup of the SARS-2 virus.
Even the best vaccines for flu are only about 30-60% effective. Compare that with an effectiveness for improvement ranging from 64% to more than 90% in more than 100 new studies showing early, outpatient treatment with our existing medications described in chapters.
As research on the vaccine continues, safety and effectiveness are of primary concern. The good news is there are very safe and effective early treatments already available as we described in Chapter 3. Clearly, early, home-based treatment has now been so successful and offers so much hope, there is less urgency to have a vaccine.”
You can sign up to receive the full protocol here: https://aapsonline.org/covidpatientguide/ or find the research paper here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7410805/
5 notes
·
View notes
Text
Pfizer Bullies Nations to Put Up Collateral for Lawsuits

As reported by New Delhi-based World Is One News (WION),1Pfizer is demanding countries put up sovereign assets as collateral for expected vaccine injury lawsuits resulting from its COVID-19 inoculation. In other words, it wants governments to guarantee the company will be compensated for any expenses resulting from injury lawsuits against it.
WION reports that Argentina and Brazil have rejected Pfizer’s demands. Initially, the company demanded indemnification legislation to be enacted, such as that which it enjoys in the U.S. Argentina proposed legislation that would restrict Pfizer’s financial responsibility for injuries to those resulting from negligence or malice.
Pfizer rejected the proposal. It also rejected a rewritten proposal that included a clearer definition of negligence. Pfizer then demanded the Argentinian government put up sovereign assets — including its bank reserves, military bases and embassy buildings — as collateral. Argentina refused. A similar situation occurred in Brazil. Pfizer demanded Brazil:
“Waive sovereignty of its assets abroad in favor of Pfizer”
Not apply its domestic laws to the company
Not penalize Pfizer for vaccine delivery delays
Exempt Pfizer from all civil liability for side effects
Brazil rejected Pfizer’s demands, calling them “abusive.” As noted by WION, Pfizer developed its vaccine with the help of government funding, and now it — a private company — is demanding governments hand over sovereign assets to ensure the company won’t lose a dime if its product injures people, even if those injuries are the result of negligent company practices, fraud or malice.
youtube
Don’t Expect Compensation if Injured by COVID-19 Vaccine
In the U.S., vaccine makers already enjoy full indemnity against injuries occurring from this or any other pandemic vaccine under the PREP Act. If you’re injured, you’d have to file a compensation claim with the Countermeasures Injury Compensation Program (CICP),6 which is funded by U.S. taxpayers via Congressional appropriation to the Department of Health and Human Services (DHHS).
While similar to the National Vaccine Injury Compensation Program (NVICP), which applies to nonpandemic vaccines, the CICP is even less generous when it comes to compensation. For example, while the NVICP pays some of the costs associated with any given claim, the CICP does not. This means you’ll also be responsible for attorney fees and expert witness fees.
A significant problem with the CICP is that it’s administered within the DHHS, which is also sponsoring the COVID-19 vaccination program. This conflict of interest makes the CICP less than likely to find fault with the vaccine.
Your only route of appeal is within the DHHS, where your case would simply be reviewed by another employee. The DHHS is also responsible for making the payment, so the DHHS effectively acts as judge, jury and defendant. As reported by Dr. Meryl Nass,7 the maximum payout you can receive — even in cases of permanent disability or death — is $250,000 per person; however, you’d have to exhaust your private insurance policy before the CICP gives you a dime.
CICP will only pay the difference between what your insurance covers and the total payout amount established for your case. For permanent disability, even $250,000 won’t go far. The CICP also has a one year statute of limitations, so you have to act quickly.
This too is a significant problem, as no one really knows what injuries might arise from the COVID-19 vaccine, or when, and this makes tying the injury to the vaccination a difficult prospect. Employers that mandate the COVID-19 vaccine will also be indemnified from liability for side effects. Instead, claims will be routed through worker’s compensation programs.
If the COVID-19 vaccines are as safe as the manufacturers claim, why do they insist on so much indemnification? Do they suspect or know something they’re refusing to admit publicly?
Side Effects Are Inevitable
Of course, those of us who have been looking at the science behind the mRNA technology used to create these novel “vaccines” have long since realized there are tremendous risks involved. For starters, mRNA vaccines are most accurately referred to as gene therapies, as this is what they are.
They effectively turn your cells into bioreactors that churn out viral proteins to incite an immune response, and there’s no off-switch.8 Based on historical and preliminary evidence, significant short- and long-term side effects are, quite frankly, inevitable.
For starters, your body sees the synthetic mRNA as “non-self,” which can cause autoantibodies to attack your own tissues. Judy Mikovits, Ph.D., explained this in her interview, featured in “How COVID-19 ‘Vaccines’ May Destroy the Lives of Millions.”
Free mRNA also drive inflammatory diseases, which is why making synthetic mRNA thermostable — i.e., slowing the breakdown of the RNA by encasing it in lipid nanoparticles — is likely to be problematic. The nanoparticles themselves also pose a risk. COVID-19 vaccines use PEGylated lipid nanoparticles, which is known to cause allergic reactions and anaphylaxis.9,10
What’s more, previous attempts to develop an mRNA-based drug using lipid nanoparticles failed and had to be abandoned because when the dose was too low, the drug had no effect, and when dosed too high, the drug became too toxic.11 An obvious question is: What has changed that now makes this technology safe enough for mass use?
As detailed in my interview with Mikovits, the synthetic RNA influences the gene syncytin, which can result in:
Brain inflammation
Dysregulated communication between the microglia in your brain, which are critical for clearing toxins and pathogens
Dysregulated immune system
Dysregulated endocannabinoid system (which calms inflammation)
1 note
·
View note
Photo

Over the past couple of weeks I’ve made a concerted effort to distance myself from just about every news feed and platform that has nothing better to do than report the latest covid statistics. The reason for this is quite honestly, like many people I have had enough. Despite my best efforts, the media bombardment is so pervasive that an update got through, and instead of deleting it, I did the math.
In South Africa at the time of receiving that update there were supposedly 1 039 161 positive cases counted, with 20 033 deaths. I am no maths genius but it wasn’t a stretch to figure out that this was around 2%. I then looked for the data for the United States which is also around 2% and the UK which is around 3%. On average this virus has a mortality rate of 2.5% with the majority of those deaths affecting the elderly and those with pre-existing conditions, otherwise known as co-morbidities. Except that the data reflected is questionable.
When you sift through the conspiracy theories and start talking to credible professionals in the medical industry you begin to see a pattern emerging. Looking at the data of years gone by, pneumonia and flu viruses year on year have also resulted in between a 1% and 2% death rate. So why the hysteria?
According to the WHO: A pandemic is defined as “an epidemic occurring worldwide, or over a very wide area, crossing international boundaries and usually affecting a large number of people”. The classical definition includes nothing about population immunity, virology or disease severity. By this definition, pandemics can be said to occur annually in each of the temperate southern and northern hemispheres, given that seasonal epidemics cross international boundaries and affect a large number of people. This happens every year but the world doesn’t come to a grinding halt because of it.
According to the British Medical Journal the PCR test is inaccurate, picking up dead and ineffective virus particles that may be found on most people, most of the time. It states that the PCR test, never designed for this kind of testing has an error margin of 97%. That’s insanity no matter how you want to spin it. If the widely accepted method for determining whether or not a person is infected is fundamentally flawed, the resulting data is completely inaccurate.
Added to which, the death statistics are also questionable. They do not define who died because of the virus or with the virus. For example, a colleague’s mother passed away from pancreatic cancer in July, yet the death certificate states covid19 as cause of death. This is not an isolated incident.
The World Health Organisation guidelines state that “COVID-19 should be recorded on the medical certificate of cause of death for ALL decedents where the disease, or is assumed to have caused, or contributed to death, i.e. COVID-19 is the underlying cause of death”. This means no one really knows how many have died directly from a covid infection.
The Centre for Evidence-Based Medicine has shown that one in thirteen (7.8%) deaths with COVID-19 on the death certificate did not have the disease as the underlying cause of death, further distorting the data.
The decisions directly related to our lives and livelihoods are based on inaccurate or distorted data and no one is doing anything about it.
Enough about the deliberate distortion of the facts. The question is why is this happening?
There is a frenetic urgency to get the world vaccinated. Bill Gates began pushing the vaccination agenda way back in 2013 if not earlier. And naturally people, at least people who can still think for themselves are extremely wary of this vaccine. At the time of writing this, the vaccine has only been available for a couple of weeks, and in this short window the significant adverse effects in those already having received the vaccination is 3% based on recent published information. Higher than the death rate of the virus. If you were to go by statistics alone, the vaccine will kill more people than the virus.
The pharmaceutical companies and their stakeholders are naturally elated that the powers that be are enforcing and coercing people into having to accept this vaccine, creating the illusion that their freedom lies on the other side of a needle. And further perpetuating the myth that drugs are going to save you. Bearing in mind that the manufacturers of this technology are free of any kind of liability arising from death or damage caused by a substance that is being trialed simultaneously on millions of people. In simple terms, if the vaccine harms you or renders you infertile you have no recourse.
Recently a second strain of the virus has emerged, This is nothing new - viruses mutate. This is why there is a different flu strain each season. It has been a year since the first strain emerged and as viruses seem to be excellent timekeepers, its right on schedule for an upgrade. This is further going to throw a spanner into the vaccine works. Will the current vaccine work with the new strain or create other complications? If people have indeed contracted the original virus, will taking the vaccine have immune suppressing effects rendering them more vulnerable to other strains? Pregnant women and women of “child bearing age” have been warned by the NHS not to take the vaccine because it may render them sterile or have deleterious effects on the foetus. But its ok to give this unknown quantity to the elderly or your child? I think not.
What happened to freedom of choice? What happened to autonomy? What happened to informed consent? What happened to common sense?
For me personally, the most disturbing part of this experience is how people I thought of as free thinking, intelligent individuals are simply kowtowing, going with the flow because they don’t want to be seen as outliers. It baffles me how so many people are afraid of voicing an opinion. It wasn’t so long ago that the Nazis used this kind of brainwashing and propaganda to commit genocide. And we are going down this path again with our eyes wide open.
Back in early 2020 governments the world over were advised by the WHO to impose widespread lockdown measures in order to curb the spread of the virus. The media were so distracted with whether or not the virus came from a bat or a pangolin that no one thought to ask if these counter measures at controlling people was the best option for the economies of the world in the first place. No one gave any thought to the destruction that would ensue. How many people would lose their jobs, livelihoods and minds in the process. Because we trusted the people we vote for to do what is in our best interest.
The second-largest funder of the WHO is the Bill and Melinda Gates Foundation, which provides 9.8% of the WHO’s funds, effectively calling the shots! After Trump pulled funding, The World Health Organisation is now effectively owned by Microsoft and China. Bloody terrifying thought that is!
It is now too late to put the genie back in the bottle. For governments to admit that they acted without a full understanding of the facts or unable to foresee the chaos and destruction that would ensue, going back and admitting they were wrong will result in chaos, crippling class actions and people in power being forced to step down. There will be anarchy. Confidence in governments the world over has been severely compromised not to mention the unstable public option of giant pharmaceutical companies.
The puppet masters at the WHO (Gates) is also a major shareholder in Pfizer. Incidentally the Gates foundation funded the development of the Pfizer owned sterilisation contraceptive Sayana, targeting specifically third world countries.
At the risk of joining the ranks of the conspiracy theorists, it seems that the company who gave birth to computer viruses has also given birth to a means of enforced sterilisation.
Getting rid of the elderly and ill, controlling those who are young and able though fear and ensuring that those who can have children are stopped in their tracks. The facts really do speak for themselves, but you can connect the dots?
Perhaps people do nothing and say nothing because they feel that their opinions don’t count? They they won’t be heard amongst the noise created by the media and the hysteria? People don’t speak up because they are afraid of what there peers may think of them. And this is why the greatest tragedies throughout human history happen.
People who do nothing. People who say nothing. In the face of glaring evidence that the emperor is wearing no clothes, the average person waits for someone else to take action. We are in a mess and in the hands of people who do not have anyones best interest at heart except for themselves and their own agendas.
So what good can possibly come from this situation? Thankfully some have realised that their health is in their own hands and no one can save them except for themselves. If you take the steps to stay healthy - eat real food, get decent sleep, surround yourself with positive people and exercise - preferably in the sunlight, chances are you won’t even know if you catch a virus because your body is innately geared towards protecting you from getting seriously ill.
It has hopefully brought to light the logical realisation that if you aren’t feeling well, stay at home. Wash your hands and don’t sneeze on people.
With luck, more of us will wake up and realise that no vaccine or drug can save you from bad decisions. Giant corporations are not creating vaccines because they care about you, they care about their profits. If they engineered medicine for altruistic purposes they would be non-profits not multibillion dollar organisations. And perhaps more people will realise that governments and government institutions are controlled by the private sector who are the giants they are, because we, the public created them.
We buy their products, whether the product is software, insurance, junk food or drugs. We created these organisations who are controlling the governments who are controlling us - with fear. With hope more people we will start to see the self perpetuating, destructive cycle that we have come to think of as normal, or maybe not.
My greatest wish for you in 2021 who ever you are, wherever you are, is to wake up and take responsibility for you own health, your own choices and your own autonomy. Speak up when something doesn’t add up and stop feeding the fear.
https://www.bmj.com/content/371/bmj.m4916
https://www.icd10monitor.com/false-positives-in-pcr-tests-for-covid-19
https://www.chiropractic.org/informed-consent-and-freedom-of-choice-on-vaccination-issues/
https://www.cebm.net/covid-19/death-certificate-data-covid-19-as-the-underlying-cause-of-death/
https://sif.gatesfoundation.org/investments/pfizer/
https://www.devex.com/news/big-concerns-over-gates-foundation-s-potential-to-become-largest-who-donor-97377
2 notes
·
View notes
Text
Understanding Obesity (Part 1): Why worry about obesity?
In Brunei, 1 in 2 children are living with either overweight or obesity. This makes us top in ASEAN for child obesity. We have always strived to be top of the list, recognised in the region and all, but this is not really what we meant... It doesn’t stop there - the prevalence just keeps increasing over the years. If nothing is done soon enough, it won’t be long until we’re seeing a generation with more people living with obesity than those with normal weight. Adults don’t fare better as 63% of adults are living with excess weight (BMI>25), making us second in the region.
Why is this such an issue? Why can’t we just accept that people have different lifestyles, different body sizes, different composition of body fats, varying lifespan and so on? Why can’t we just embrace individuality? Why is obesity worth our undue attention?

Impact on Physical Health
Firstly, living with obesity poses threat to physical health by increasing their risk of developing a range of diseases, such as high blood pressure, type 2 diabetes, cardiovascular diseases, certain types of cancer, osteoarthritis (joint pain), sleep apnoea, chronic kidney disease - the list just goes on.
In children, their chances of developing asthma and musculoskeletal problems are doubled, T2 diabetes and hypertension quadrupled, and non-alcoholic fatty liver disease increased by 26 times. If not addressed effectively, they are likely to carry over the health conditions into adulthood. In fact, children with obesity are around 5 times more likely to live with obesity and its related comorbidities as adults. More recently, people living with obesity has also been shown to be twice more likely to be hospitalised with COVID-19 compared to those with lower BMI.
So it is rarely the case that obesity kills you. But rather, obesity skyrockets the chances of us developing these deadly complications. In fact, excess weight is one of the risk factors that ALL top three leading causes of deaths in Brunei share in common, i.e. 1) cancer, 2) cardiovascular diseases, and 3) diabetes.
I often personally hear people disregarding obesity intervention efforts with “I’m here for a good time, not a long time”. It’s used as song titles, printed on shirts, mugs, tweeted multiple times a day and glorified like an Aristotle principle. This implies that some people are fine with dying early, as long as they are happy. However, we have to be mindful of how these complications resulting from obesity does not just reduce our life expectancy, but mainly our healthy life expectancy (years of life spent in good health). Living with sakit lutut, four hours of dialysis thrice per week, insulin jabs, medications, fatigue - these all gives rise to a significantly poorer quality of life regardless of how long you live. One might then have to rethink that ideology.
Impact on Mental Health
Secondly, obesity also contributes to psychosocial challenges that a child or adult may face, such as:
stigma: overweight respondents were 12 times more likely, obese respondents were 37 times more likely, and severely obese respondents were 100 times more likely to report discrimination in the workplace
depression: being overweight in childhood was associated with increased risk of lifetime major depressive disorder
generally poor mental health due to binge-eating disorder, anxiety, low self-esteem and poor body image. Around 1 in 2 of bariatric surgery candidates report a history of mental health treatment.
Stigma and discrimination are pervasive among individuals with obesity who are frequently blamed for their excess weight. This argument is rendered justified by many as apparently ‘it may motivate individuals to adopt healthier behaviours’ (basically through a passive-aggressive approach). However, various research has shown that such theory is deeply flawed; direct and indirect stigmatisation towards individuals with obesity only further threatens mental and physical health, likely to adversely drive weight gain and only acts as a barrier for effective obesity interventions (here, here, here, here, and many more!!!). The rise in childhood obesity and poor mental health among children has thus been recognised as a syndemic -- two epidemics interacting synergistically and contributing to excess burden of disease within the population.
Impact on Economy
Lastly, the impacts of obesity extends beyond individual health and into the wider economy. It results in direct economic costs through substantial spending of healthcare services (UK example):
the NHS expenditure is almost double on each individual with obesity compared to those with normal BMI
estimated £5 billion per year spent on treating obesity and diabetes -- more than that spent on the police, fire service and judiciary system combined
Obesity also results in indirect economic costs extending beyond the healthcare sector, through productivity losses such as:
absenteeism: an individual with obesity takes an extra four days off per year. A total of 16 million days of absence due to obesity was reported in 2014
presenteeism: working while experiencing mental or physical health problems among individuals with obesity were reported to result in producing work of poorer quality and lower productivity in the workplace
Bottom Line
The consequences of living with obesity are not just limited to the individual’s physical health, but also their mental health and extends to the wider socioeconomic environment. Obesity has been formally classified by the World Obesity Federation (WOF) and World Health Organisation (WHO) as not just a disease, but also one of pandemic nature due to its widespread global burden. Unlike pandemics of infectious diseases where the impacts are sudden and stark - attributable to a single cause, the hidden pandemic of obesity is progressive and far more complex. It does not solely affect the respective individuals, but the whole population. It is what is known as a public health crisis.
This post might have sounded a little condescending, with me telling the world the dark side of living with obesity. Hold your horses -- please continue to read Part 2 as I talk about the causes of obesity, as only then can I convey what I am really trying to say.
* Some figures indicate relative and not absolute risk, so please interpret with caution.
** Main References:
Time to Solve Childhood Obesity An Independent Report by the Chief Medical Officer, 2019 (Professor Dame Sally Davies) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/837907/cmo-special-report-childhood-obesity-october-2019.pdf
Gene Eating by Giles Yeo
Photo: World Obesity Federation
#brunei#obesity#childhood obesity#child obesity#asia#brunei darussalam#ncd#non-communicable diseases#brunei health#malaysia#indonesia#singapore#south-east asia#overweight#obesity cause#causes of obesity#nutrition#food#dietetics#health#healthy
3 notes
·
View notes
Link
via Politics – FiveThirtyEight
cwick (Chadwick Matlin, deputy editor): Clare, Kaleigh and Maggie, thanks for joining me to talk about the president’s medicine cabinet. Yesterday, President Trump revealed that he’s taking hydroxychloroquine, an anti-malarial medication, to help prevent him from contracting COVID-19. Trump’s comments were the culmination of his interest in the drug, which he has hyped for months as a way to help fight the pandemic. Let’s talk about what the science says about hydroxychloroquine, what Trump has said about it, and what it says about Trump that he’s taking it.
So, let’s start with the science, which is about the only thing that can ground us in this frenzied moment. Can hydroxychloroquine prevent someone from getting COVID-19?
clare.malone (Clare Malone, senior political writer): (Readers can, on their own time, imagine what else is in the president’s gold-plated medicine cabinet.)
maggie (Maggie Koerth, senior science writer): What we’re basically looking at here is a massive lack of evidence for anything, Chad.
kaleigh (Kaleigh Rogers, science and politics reporter): The results from the few studies that have been done are mixed, at best. Some have found hydroxychloroquine reduced the duration of COVID-19, others have found no difference between using the drug and not, and at least one found there was actually a worse outcome for patients who were on hydroxychloroquine versus those who were not.
maggie: There are ongoing studies of better quality happening — I’m particularly interested in one that’s looking at COVID-19 incidence and outcomes in lupus patients who were already taking hydroxychloroquine for their chronic illness — but we just don’t have evidence to say it does anything.
kaleigh: We do know from past trials of hydroxychloroquine that it can cause abnormal heart rhythms, so the president’s claim that there’s no harm in trying it is not based on evidence. This isn’t like taking vitamin C.
cwick: And are these all studies that test for whether hydroxychloroquine prevents COVID-19? Or are they testing whether it improves treatment of the disease?
kaleigh: Most trials I’ve seen are to treat COVID-19, not to prevent it. (Though there is at least one trial currently testing it out for preventive use.)
cwick: So Trump’s decision to take it preventively complicates things further. We’re in the dearth-iest corner of the dearth of evidence.
maggie: You have the science side of things, which is mostly proceeding as it ought to, and you have the political side, which is full of hype and boom-or-bust demand.
cwick: With that said, Clare, why is Trump doing this? Or maybe the better question: Why is Trump telling us he’s doing it?
clare.malone: On a personal level, Trump is likely taking it because of the recent infections of White House staff and because, well, as we all know, he’s a germaphobe!
But I think it’s a piece of his public response to the outbreak. He attempted, in a quite pitched way at first, to convince the public that things were not as bad as they were made out to be. He promised a non-entity of a disease at first and compared it to the flu. The idea of taking this drug plays into all that, in a more tamped-down way, because he’s offering the public a sort of “cure” or hope. I don’t think it’s a slip of the tongue, but it is a key part of his own thinking about the virus and a key part of how he wants to talk about it in public.
cwick: That’s interesting, Clare. One of the defining characteristics of this disease has been its uncertainty. That’s in part because we haven’t known how to treat those who are sick (let alone make the rest of us immune). Trump seems to be saying: If a medication is good enough to make the president feel safer, it’s good enough to make you feel safer.
maggie: I’m interested, Clare, in whether we’ve seen presidents get so specific in their hope-peddling before. It seems normal for a president to say, “Oh there’s all this research being done and we will have options, let’s fund them.” But it feels to me like Trump has uniquely used the bully pulpit to tout specific products — hydroxychloroquine, that Abbott Laboratories test — when there was more than one option out there. And it’s come back to bite him multiple times. Because when science is moving fast, most of the “good ideas” are going to fail at first. Pinning hope on specific brands and products seems like a real risk he’s taken on.
clare.malone: Right, Chad. The president has gotten A TON of flak for his refusal to wear a mask, but that’s also part of his messaging! It’s certainly odd that he’s taking this drug and not wearing a mask, but he’s a big believer in the sort of traditional displays of “masculine” strength that American politicians have thought the public likes to see. His no-mask thing is the pandemic equivalent of presidential candidates not wearing winter coats while campaigning in Iowa in January.
cwick: This isn’t about promoting promising research, or the latest trial results. He is, in effect, becoming part of the trial himself.
kaleigh: Except it’s not controlled, randomized or blind, so his “trial” is scientifically meaningless. I drink coffee every day and haven’t gotten COVID-19 yet — maybe that’s a prophylactic, too! This is the logic of anecdotal evidence.
maggie: So this reminds me of the study I saw about how men were significantly less likely than women to take non-pharmaceutical preventive measures in a health crisis, like wearing masks, but were more likely than women to take pharmaceutical measures.
kaleigh: His announcement that he’s taking it certainly felt defiant, like he’s doubling down in spite of the evidence. He also spent some time yesterday criticizing a Veterans Affairs study, which found that patients on hydroxychloroquine actually had a higher risk of death.
cwick: Kaleigh, your point about the VA study is super interesting. We’ve seen how the president can dismiss news and findings that run counter to the narrative he wants to promote, and part of his political struggle during this crisis has been knowing when to embrace the science and when to reject it out of hand. By putting his chips in on one drug, the drug itself becomes a cause to rally behind, and news that disputes its power becomes easier for Trump to critique. Essentially, hydroxychloroquine has become part of the White House policy agenda.
clare.malone: Also, if you’ve eschewed a lot of the science in your initial stages of your response, you might as well bet big on a miracle cure, right? Maybe you’ll be right and people will credit with you being early to the party. Americans do love pharmaceutical solutions to their problems.
Shoutout here to former Sen. Bob Dole, the OG American politician-pharmaceuticals spokesman.
kaleigh: It is strange that he got so fixated on this one possible treatment, though. The antiviral drug Remdesivir, by contrast, actually has some promising early results. Why is Trump so interested in hydroxychloroquine? He has scoffed at questions about whether he, say, owns stock in a company that produces the drug, but he also hasn’t provided a lot of explanation about why he’s so fascinated with it.
cwick: Some would have you believe that it might be an issue of cronyism. Here’s the New York Times from April: “Some associates of Mr. Trump’s have financial interests in the issue. Sanofi’s largest shareholders include Fisher Asset Management, the investment company run by Ken Fisher, a major donor to Republicans, including Mr. Trump. A spokesman for Mr. Fisher declined to comment.”
clare.malone: It’s a good question. I’m a bit skeptical of the stock interests answer, since what Trump seems to own is quite negligible. But to Chad’s point, Trump’s personal phone line is always known to be open to friends outside the White House! In the initial stages of the crisis, there’s a sense that he was hesitant to trigger portions of the Defense Production Act because of feedback from the Chamber of Commerce and private industry.
maggie: And meanwhile, his political advocacy has pushed for millions to be spent on it … supplies acquired by the VA and the Strategic National Stockpile.
kaleigh: One thing is clear: When Trump touts a treatment, interest goes up. Not only do Google searches soar, but at least one online prescription service reported a nearly six-fold increase in demand for hydroxychloroquine prescriptions after Trump first mentioned the drug.
maggie: We know there were people from the anti-vaccine movement promoting the so-called ”miracle mineral solution” to him — a pseudoscience “treatment” that basically amounts to industrial bleach — before he spent that one press conference talking about treating yourself with disinfectant.
clare.malone: And we know Trump is susceptible to anti-vaxxers from earlier in his time in public life.
maggie: I can see why the open phone line thing would work in real estate — hot backdoor tips from buddies. But that doesn’t really work in science.
clare.malone: But isn’t it more politics masquerading as science? Which might be the whole problem.
cwick: Right, it seems like we’re all arriving at the same terminus: The president has long demonstrated a contrarian approach to science, so his taking hydroxychloroquine despite iffy science is as much about the political as it is about the personal.
kaleigh: What is the political motivation to fixate on one drug and also continue to tout it against all current evidence?
clare.malone: Momentum. You’ve already been saying it: Why stop saying it?! You’ll just look more fallible.
cwick: Politicians don’t like to be wrong.
maggie: This politician in particular really doesn’t like to be wrong — maybe even more so than others.
clare.malone: It’s the spin zone, y’all! Hop on in. It’s dark, but that’s what it is.
kaleigh: Right, changing your mind based on new and better information is bad in politics, for some reason.
clare.malone: Flip flopping.
cwick: It’s considered bad in broader society, too!
clare.malone: Is it?? That’s actually an interesting question.
cwick: I’d say that I’m reconsidering, but then you’d think I was weak…
3 notes
·
View notes
Text
Time to hold China accountable.

As the internet brought the world closer together, international logistics connected the dots between supply and markets to create an intricate network of global business transactions. A new world order of commerce has taken shape whether we like it or not.
The abundance of lower cost-of-labor goods and materials, and the freedom to operate in less regulated countries has driven major manufacturing from the west to offshore operations in Asia and other parts of the world.
China has been the single largest benefactor of this evolution and has done so by implementing aggressive tactics that at first, appear favorable to foreign companies to operate in the country. The caveat to this favorable business environment is the Chinese policy requiring mandatory local ownership, leveraging the company’s proprietary technologies while pushing other countries to open their markets for tax free Chinese goods. The American public has remained blissfully unaware of the potential vulnerabilities of this new world order as they continue to fill their carts with cheap merchandise from their local major box stores, pharmacies and supermarkets.
The outbreak and spread of Corona virus (Covid-19) and its impact on the world’s economies has exposed the weaknesses of this new world order. In trying to control the spread of this disease, America now finds itself facing a shortage of pharmaceutical and medical products that are urgently needed during this current heath crisis.
The United States remains the global leader in drug research and development. However, about 60 percent of factories manufacturing drug ingredients and finished medicines for U.S. patients are located overseas, with China and India accounting for 40 percent. Chinese pharmaceutical companies now supply more than 90 percent of U.S. antibiotics, vitamin C, ibuprofen, hydrocortisone, and other medicines as well as 70 percent of acetaminophen.
For the past two decades, China has well taken advantage of these new opportunities for commerce to become the second largest economy in world. However, with this success, the Chinese government has ignored or refused to engage in human rights, implement or maintain consumer safety policies or environmental stewardship. China has often exported tainted food and pharmaceutical products with little to no accountability.
The China One policy advocated by its President Xi Jinping to bring all of China under a single leader is about world dominance thru consolidation of power and economic dependencies. The Chinese have used their amassed wealth from trade to push an agenda of territorial expansion and geopolitical influence in developing nations. They are leveraging massive loans to many small, developing nations to secure territorial assets and increase their military footprint. These countries, when they can’t afford to repay these loans become captive to Chinese policies.
The current Chinese Authoritarian Government, President Xi Jinping can dictate how they spend their national wealth and implement programs with great speed to achieve their objectives. They are in control of 1.2 billion people’s minds with their message. China is experiencing viral health crisis, but authorities are more focused on managing political damage and controlling the perception of their masses, in order to divert attention away from any potential uprising within the country. Their most recent propaganda informs the Chinese people that the U.S Military developed and spread the virus in China. The Chinese Government is nervous and acutely aware that the recent unrest in Hong Kong will resurface once the pandemic begins to wane.
As of this writing, the Chinese government has refused to allow the CDC into the country and has ignored offers of assistance from the WHO to conduct onsite investigations. In an article published last week in Xinhua, the state-run media agency, was the claim that China could impose pharmaceutical export controls on America at its discretion. This threat highlights the actual control China has on the world’s supply chain and what they may be willing to do. This is the new norm when it comes to China’s economic and military strategies. To suffocate nations with economic and/or geopolitical leverage where their native populations become rebellious to their own governments. China is a master of this craft after many years of well-oiled communist ideology.
To date, there are over 132,000 confirmed cases and over 5000 deaths worldwide from the Covid-19 virus that originated in Wuhan, China. As these numbers continue to grow for the foreseeable future, the world’s governments have not yet come out to address liability for this pandemic. The official name of this specific virus is SARS-CoV-2 and the disease it causes is the Coronavirus disease 2019 or COVID-19. Coronaviruses are a family of viruses that are common within humans and various different species of animals, including camels, cattle, cats, dogs and bats.
Trillions of dollars and thousands of lives are now being lost in this new world order and China should be held accountable. This pandemic originated in the local Wuhan street markets where vendors sell raw meat, much of it tainted, from a variety of animals in unsanitary conditions. The practice of selling live animals such as dogs, cats and rats at these markets is prevalent throughout the country. The poor or non-existent sanitary conditions are perfect for incubating many diseases. The world has witnessed several pandemics originating from China, including, the Hong Kong Flu, Russian Flu and more recently the SARs virus. China has done very little to address the health and well-being of their own people with no consideration to the worldwide effects that result from their lack of action.
The Chinese authorities’ focus is on economic growth over consumer safety, comes at a steep cost to the rest of the world. In America and many other countries, businesses must comply with compulsory safety standards and are held accountable for their actions. There is a substantial cost to business to maintain compliance and abide by rules and regulations, knowing what the consequences might be if they fail to do so. China has side-stepped many of these requirements without penalty or serious consequences. The Chinese one-party authoritarian government is notorious for maintaining total control over their industries and people. But why have they neglected basic food safety standards?
The Chinese are masters at copying and counterfeiting manufactured products from the United States in an effort compete with America on the world market. They avoid regulations and compliance over dominance and profits. To this end, they do not accept the responsibility to safeguard the food, medicine or product safety for their own people. This negligence and its resulting effects on the population has now traveled outside of China and the whole world is at risk of economic and social collapse from this outbreak.
The United States and others must now hold accountable the government of China and the people responsible for this crisis. The world’s response to China should be an economic “shot-across-the-bow” to reconsider its current policies. A warning that you can’t reap the benefits economic development at the cost of humanity. To do so, invites economic or criminal retribution to those responsible. Governments that fail to manage their economic development and social responsibilities should be restricted from participating in the world’s markets as responsible countries do. There needs to be serious penalties in place to reign in and force retribution to those countries and individuals that do not comply with established health, safety and environmental practices and regulations
This should also be a clarion call for consumers who have increasingly relied on cheap “Made in China” goods for the past twenty plus years, at the risk of losing our local industries, skills and know-how. We are now relying not only on trinkets from China but many of our life-saving medicines.
The World should react to this pandemic as a crime against humanity. The message sent to China should be that they owe the world compensation for losses incurred from their violations and neglect of basic human rights and principles. In the interim, the depletion of our national reserves and additional expense resulting from the Corona virus will need to be compensated and this compensation should come from a “Corona tax” levied against all Chinese imported products. While this action will certainly meet with some resistance from consumers for increased prices, it will also force the Chinese to reconsider their current actions in ignoring basic principles in the health and welfare of their own and the world’s citizens. The immediate and long-term security for the United States can only be assured by rebuilding the country’s manufacturing infrastructure and reducing our dependence of foreign imports.
About the author: Ron Atapattu is the founder and President of the ShipOCI group of companies that include, Overseas Cargo, Inc, a third party logistics service provider specializing in the handling, storage, importation and export of perishable food products, Star Warehouse, one of the largest dry and temperature controlled warehouse facilities in the Southeastern United States and A Star Suppliers, makers and distributors of the elephantea™ line of organic tea products. Ron has over thirty years of experience in international supply chain logistics and has witnessed first-hand the practices of Chinese industries’ and Government that have led to the imbalance in trade and product safety failures that the world is experiencing today.
1 note
·
View note
Text
Why You Should Add Naloxone to Your Prescription Medication Bag

Opioids are compounds found in pain relief medicines because they have sedative and analgesic effects. Some of these compounds are codeine, morphine, methadone, tramadol, heroin, etc. Most of these compounds also have euphoric effects, which is why many use opioids even for non-medical reasons.
The rate of prescription drug abuse has increased over the years – especially since many have this drug in their prescription medication bag – and a general term for it is opioid overdose. This overdose occurs when someone intentionally or accidentally takes too much of a drug containing opioids. While this is usually the most common situation, opioid overdose can also occur when an opioid-containing drug comes in contact with other medication or an underlying health condition.
Opioid overdose can lead to many issues. For one, it can lead to opioid dependence, which is characterized by a strong desire to use opioids all the time without considering the negative consequences involved. This dependence can further lead to physiological issues like increased tolerance of the negative of opioids and withdrawal symptoms due to reduced intake of the medicine.
This can go on for a long time, and that’s just the beginning of the side effects. Opioid overdose affects the part of the brain which controls breathing. When this happens, the victim will begin to experience symptoms like unconsciousness, difficulty breathing, and pinpoint pupils. If nothing is done, the victim will end up dead.
According to World Health Organization (WHO), between 2000 and 2018, the death rate from opioid overdose has increased by 120%. This rate increased more during the COVID-19 pandemic. These statistics show a state of emergency.
The increased fatality rate has made it necessary for the U.S. Food and Drug Administration to develop a medicine that will counter the effects of opioids – naloxone. Naloxone reverses the results of an opioid in the system, such as restoring normal breathing in anyone who’s having breathing difficulty.

Naloxone should be prescribed to:
Anyone who’s been prescribed opioid pain relievers;
Patients at risk of opioid overdose or who has a history of opioid use disorder (OUD);
Patients with household members who are at risk of accidentally ingesting opioids.
So, as you purchase opioids, you should also buy naloxone. You might need it for unforeseen situations around you.
While it’s important to have naloxone alongside opioids, getting a medication bag for opioids is also important. The battle against opioid overdose has many negative consequences and a bag with a lock is your first line of defense. It is important that opioids do not reach people who would abuse the drug, intentionally or accidentally.
It’s important that an opioid bag also comes with a lock. Drug addicts would do anything to get their next fix, including stealing your medication bag. This makes it all the more important to get an opioid bag with a lock.
Cardinal Bag Supplies’ prescriptions medication bags with lock are secure and would discourage any drug addict or thief from getting into the bag and stealing opioids.
Also, these bags have been designed to show signs of tampering. This way, the rightful medicine owner will know if someone has had access to the medication bag and act promptly. To show your support of the move to reduce the prevailing opioid crisis in the country, you can customize your opioid bag and include a tag that says that you’re all for opioid overdose prevention.
Medication bag for opioids is more affordable than a medication lock box – and even more effective – so you don’t have to spend so much money to do what’s right.
Conclusion
As the opioid crisis rages on, preventive measures should also increase. This makes it more important to have the necessary items around for you to combat the situation.
Whatever you do, always have naloxone around you. You might need it at some point. Even if you don’t use it on yourself, you might need it to save someone else’s life.
0 notes
Text
Siginficant Impact of COVID-19 on Coffee in Food & Beverage Industry
Coffee Market,

COVID-19 Impact on Coffee in Food and Beverage Industry
The outbreak of the COVID-19 has affected the international trade majorly. One of the sectors which are facing the impact due to COVID-19 is coffee industry. It has highly affected the demand of the coffee market as demand and supply of various coffee stringent government rules such as lockdown has been implemented for maintaining social distancing in hotels, bars and restaurants.
According to CBI, this crisis has caused decrease in the sales volumes of coffee by 50.0% in Europe region and approximately by 25.0% in the United States. Due to decrease in sale volume, the roaster is ordering less coffee to providers as they have already warehouses full.
PRE COVID-19 IMPACT
Drinking coffee fuels an individual to start a day for working in offices, home and many others. Due to its fueling activity, it is one of the most consumable products in the market.
For instance,
· In America, especially in the U.S., around 66 billion cups of coffee per year is taken by consumers.
Similarly, there are many other countries which consume coffee highly and they are Finland, Sweden, Switzerland, Germany, France, Italy and others.
The consumption of coffee is increasing every year and this leads to high growth in the market value.
For instance,
· According to The International Coffee Organization (ICO), the world coffee consumption was increasing before COVID-19 which is represented in below graph.
FIGURE 1. COFFEE CONSUMPTION (2016-2019)

to high consumption pattern, the demand for the coffee was increasing till last year. And sudden outbreak of the Coronavirus completely impacted whole coffee market.
SCENARIO DUE TO COVID-19 IN COFFEE INDUSTRY
Till last year, the consumption of coffee was increasing as consumers were highly inclined for consuming coffee. As the pandemic started in early 2020, the destruction in the market took place. The coffee industry faced the destruction as the consumer behavior changed and hence the consumption pattern for the coffee declined.
For instance,
FIGURE 2. COMPARISON BETWEEN TWO YEARS IN WORLD COFFEE CONSUMPTION (IN THOUSANDS 60-KG BAGS)
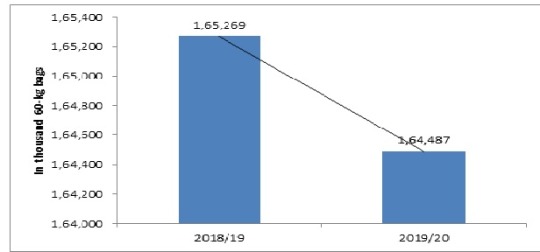
COVID-19 crisis impacts the demand of coffee on a wider range as due to lockdown in several countries, strict government rules regarding the closing of restaurants and bars and maintaining the distance is imposed which has impacted the restaurants severely and has affected the coffee demand on a wider range. Reduction in household incomes as various people lost their jobs and could translate into lower demand for coffee in volume terms.
According to strict Italian government rules, the closing of restaurants, shops and coffee bars by 6 PM, for maintain the social distance and reducing the COVID-19 impact, no gatherings and similar regulations to reduce the impact of virus are expected to restrain the consumption by 10-12% in the next quarter. Due to the delay in shipment the demand of coffee is widely affected and it is estimated to continue for a longer period if the situation is not controlled.
FACTORS AFFECTED THE COFFEE MARKET
The pandemic led into lockdown due to which the supply and demand chain broke and the market took a decline phase. Below chart represents number of factors declining the market growth amid COVID-19.
POST COVID-19 SCENARIO
Once the worst coronavirus crisis is over in future, the small coffee businesses or industries will recover as the lockdown will not be carried out. All the food service sectors will be open and number of customers will be visiting as of previous time. Yet, the sector believes most will survive. Again the production, consumption and international trading will be normal and the coffee sector will regain its position as of previous and may also grow with substantial growth rate in future.
COFFEE MANUFACTURERS: PERSPECTIVE AND INITIATIVES
The coffee demand among household consumption has been increased in the pandemic, whereas the demand of coffee in Europe and Americas were more in the food service sectors in cafes and bars. Due to the long term lockdown people are referring the coffee in their household usage. The household income has lowered the demand for coffee in terms of volume. The consumption of organic based products is gaining population including ready to drink coffee market.
The burst of pandemic panic complements a steady rise in coffee consumption and their sales that investors have largely overlooked amid the financial debacles of better-known organic coffees,
For instance,
“Considering the increasingly busy lifestyles of modern consumers, we are actively expanding our ready-to-drink portfolio to meet the demand for high-quality coffee with convenience, and to cultivate new growth areas in the increasingly competitive global coffee market, The epidemic has caused an impact on us, but with recovery under the guidance of COVID-19 the government and the support of the owners, we remain optimistic about the outlook.”
· Shakir Moin, Chief Operating Officer at Costa International
“Organic product sales outperformed the growth seen in the non-organic sector in the same time period, with significant increases in purchasing of grocery items such as tea and coffee and home-baking, alongside organic wine, beef and butters and fats.”
· Finn Cottle, Trade Consultant for Soil Association Certification
Due to the supply chain disruption of the raw material especially cocoa beans or cocoa powder used as major ingredient coffee manufacturing have rose concern to the coffee manufacturers. Companies like Olam have taken initiatives to create the crises in opportunity by helping farmers in the plantation of the cocoa plants in Africa region.
For instance,
“We have palm oil plantations in Gabon; we have coffee in several countries in East Africa and a bit in West Africa. We have cocoa – that’s another co major crop – as well as rice in Nigeria.”
· Julie Greene, WHO Heads Up Olam’s Corporate Responsibility and Sustainability
“Since the arrival of COVID-19 in Côte d’Ivoire on March 11, 2020, we have seen the interest of the chocolate and cocoa industry to support the government’s actions to stop the spread of the virus and in particular to ensure that it does not reach rural areas of our country. We are grateful to the chocolate and cocoa companies that have already made contributions and are carrying out activities against the pandemic. Today’s donation announced by WCF on behalf of its members and other associations in the sector reinforces the actions already taken individually. On behalf of the cocoa community of our country, I express to them our gratitude.”
· Yves Brahima Koné, Director-General of the Café-Cacao Council
CONCLUSION
The COVID-19 spread grew into a major public health epidemic worldwide. About 1.3 million people have tested positive for the virus to date, and more than 70,000 deaths have been confirmed. Furthermore, the COVID-19 pandemic affects people's daily lives and dramatically impacts economies around the world. The COVID-19 crisis poses a shock to demand and supply impacting foreign trade flows and production chains.
Although policymakers are adopting measures to save lives and reduce the economic harm, there is a global economic slowdown. Many international organizations and research institutes expect a sharp initial downturn in economic growth and increasing unemployment, accompanied by a rebound that will depend on the efficacy of measures taken in response to the COVID-19 crisis and how rapidly confidence returns. It is likely that the COVID-19 pandemic will have a profound effect on the global coffee industry, including production, consumption and trade.
Out-of-home use is declining dramatically in the short term as an increasing number of countries accept a complete or partial lockdown. Offices, coffee shops, and restaurants remain closed to reduce virus spread. At the other hand, data at the retail and supermarket rates show that panic purchasing and stockpiling in certain countries has contributed to increased customer demand.
That is impossible, however, to have a sustained impact on consumption. Following an initial increase in market, the demand in the coming weeks and months would be proportionally lower as customers draw down stocks kept at home. The outcome of a global recession caused by the direct and indirect effects of the COVID-19 pandemic can be expected to have a deeper impact on global coffee demand. In terms of volume, reduced household incomes could translate into lower coffee demand. However, price-sensitive consumers can replace higher-value coffee with lower-value blends or brands.
Nevertheless, the coffee demand’s revenue elasticity is likely to be weak, especially in high-income countries and traditional markets with high per capita consumption levels. The following quantitative analysis aims to define the relationship between GDP growth and coffee consumption, thereby providing an estimation of the demand-side shock resulting from the pandemic COVID-19.
0 notes
Text
IT GETS WORSE
‘Out for Blood’: Inside Tennessee’s Self-Imposed Vaccine Fiasco
Critics say Republicans turned what was just another vaccine-hesitant state into a creeping public-health disaster.
NASHVILLE—Less than a week before she was ousted as the top vaccine official in Tennessee, Dr. Michelle Fiscus received a package at her office. It had been sent via Amazon without any note or indication of who might be behind it, she told The Daily Beast.
Inside was a black leather muzzle with nylon straps that looked to be made to fit a dog.
Fiscus, who became head of the state’s immunization program in January of 2019 and practiced as a pediatrician in Middle Tennessee for 17 years, already knew she had a target on her back. At a June legislative hearing, she’d been singled out by name by Republican state lawmakers upset about the health department’s teen-focused vaccine outreach; at least one of them even threatened to dissolve the department over it.
In particular, GOP lawmakers seized on a memo Fiscus had sent to medical providers who administer vaccines in which she outlined the state’s Mature Minor Doctrine. It stems from a 1987 state Supreme Court decision that allows doctors to vaccinate minors above the age of 14 without parental consent.
The contentious hearing made headlines in Tennessee before the issue largely receded from the news. But within the Republican-dominated state government, pressure continued to mount. Two weeks ago, according to Fiscus’ husband, she was warned by supervisors that she might be fired. Then, on Monday, with COVID-19 cases rising again in the state and the share of Tennesseans fully vaccinated stuck below 40 percent—one of the worst rates in the country—she was terminated.
“Morale is terrible, and every day we were waiting for more restrictions on what we could do,” Dr. Fiscus told The Daily Beast.
Her ouster was the end-result of what interviews with lawmakers, health officials, and residents in the state suggest has been a titanic and bitterly partisan struggle over how to reach vaccine holdouts. Now, critics of the Republican majority in the state say Fiscus’ firing is poised to send the vaccine push even further off the rails—all to appease extremists.
“It is pretty clear what happened is that some ultra-conservatives in the state who bought into anti-vaccine and COVID-denialism were out for blood, and the governor’s administration offered up the head,” Senate Minority Leader Jeff Yarbo (D-Nashville) told The Daily Beast.
The Governor’s office did not respond to The Daily Beast’s request for comment. A spokesperson for the House Republican Caucus referred a request for comment to the Department of Health and the governor’s office, noting they “do not make personnel decisions regarding the executive branch.”
Bill Christian, a spokesperson for the Tennessee Department of Health, told The Daily Beast, “We cannot comment on HR or personnel matters. To be clear, our vaccination efforts have not been halted or shuttered.”
But Fiscus says her ouster is exactly what it looks like—a public-health official refusing to bow to anti-vaxxers or those catering to them in positions of power, and paying a price.
“Today, a 14-year-old in Tennessee can still go and get a vaccine without parental consent,” she told The Daily Beast. “According to the decree from the Tennessee Supreme Court ruling in 1987. I didn’t make the rule. I communicated to our providers that were getting COVID-19 vaccines what the rule was.”
That may be true, but it’s getting harder than ever for kids in Tennessee to access shots.
Fiscus’ firing was followed on Tuesday by a bombshell report from The Tennessean that the health department will cease all vaccine-related outreach to minors—not just for COVID-19, but for other diseases like the flu and HPV. The paper also reported that the health department will stop hosting COVID-19 vaccine events at schools and even stop sending postcards reminding teenagers who’ve been partially vaccinated to get their second dose.
Christian, the health spokesperson, explained it this way: “We are simply taking this time to focus on our messaging and ensure our outreach is focused on parents who are making these decisions for themselves and their families.”
But insiders say Tennessee has in a matter of weeks gone from being just another southern state with a vaccine-hesitancy problem to a showcase for Republicans who cower before hardcore anti-vaccine activists.
In May, days after the state began to administer vaccinations to children ages 12 and older, Fiscus sent a letter to more than 900 vaccine providers, clarifying that they could inoculate minors without a parent or guardian in the room.
The decision to inform providers about this option—stemming from what advocates describe as long-settled court precedent—touched a nerve among Republican lawmakers. In the heated June hearing, several state legislators spoke out against the health department promoting the fact that teenagers could get vaccinated on state social media accounts, calling it “reprehensible” and likening one ad providing life-saving information to “peer pressure.”
“The Department of Health is targeting our youth,” state Rep. Scott Cepicky (R-Culleoka) said during the hearing, while holding up a printout of the Facebook ad, according to The Tennessean. “When you have advertisements like this, with a young girl with a patch on her arm all smiling, we know how impressionable our young people are.”
“For a department of ours to make it seem like you need a vaccine ... to fit in is peer pressure applied by the state of Tennessee,” Cepicky added. “Personally, I think it's reprehensible that you would do that, that you would do that to our youth.”
State Sen. Kerry Roberts (R-Springfield) reiterated a colleague’s complaint against flyers and advertisements featuring children with the phrases “Tennesseans 12+ eligible for vaccines” and “Give COVID-19 vaccines a shot.”
“Market to parents, don’t market to children. Period,” he said during the hearing, according to the outlet.
Cepicky and Roberts did not respond to The Daily Beast’s request for comment.
The Tennessean also reported last month that Lisa Piercey, the health department commissioner whose name was on Fiscus’ resignation letter, tried to assuage the Republican outrage. Specifically, Piercey said in the hearing that private healthcare providers and doctors in the state could deny shots without parental permission.
Internal emails obtained by the New York Times and The Tennessean show the state has halted vaccine-education efforts aimed at people under 18 for a variety of ailments, including the flu. Among the emails included was a directive from Piercey to remove the department’s logo from all vaccine-related materials going forward, and a note from another official to stop “proactive outreach regarding routine vaccines.” (Some major metro areas in their state have their own health-department policies, and are poised to continue vaccine outreach.)
As in many states, right-wing activists banded together in Tennessee earlier in the pandemic to oppose social-distancing and other safety measures, including vaccines.
One local group powering pushback in the Volunteer State is called Tennessee Stands. On their website, the group says they “completely reject the myth that non-pharmaceutical interventions such as mask mandates, stay-at-home orders, school closures, and business closures had any effect whatsoever on the magnitude or the trajectory of the pandemic.” Tennessee Stands has filed lawsuits against state and local officials over various public-health mandates and regulations, and was behind legislation that would allow religious exemptions to future COVID vaccine mandates at schools.
Similar legislation was ultimately passed into law. A spokesperson for the group did not respond to a request for comment for this story.
Beyond rote right-wing activism, in Tennessee, anti-vaccine sentiment has previously exploded into violence. A 36-year-old woman was arrested in May after witnesses said she drove her SUV through a COVID vaccination tent while yelling “no vaccine.”
Lawmakers are worried the state is increasingly catering to conspiracy theorists. Meanwhile, COVID deaths are rising, and the state’s best hope for boosting its lagging rollout may be tough to replace.
“What person who is qualified to do her job would want that job now?” Sen. John Ray Clemmons (D-Nashville), asked in an interview with The Daily Beast. “Are they going to take that job because they are some ‘wink wink’ understanding they are not going to fulfill all the tasks of the job?”
Calling out his Republican colleagues, Clemmons said “using kids as a political tool” and Fiscus as a “political scapegoat” will only continue to harm the already fragile public health system in Tennessee.
“You have to wonder what their endgame is here,” he said. “Right now, it looks like a short-sided political move to score some points from a handful of extremists.”
Got a tip? Send it to The Daily Beast here.
0 notes
Text
Significant COVID-19 Impact on Medical Robotics in Healthcare Industry | Data Bridge Market Research

COVID-19 Impact on Medical Robotics in Healthcare Industry
The first case of COVID-19 was found in Wuhan, China. This pandemic has influenced the whole planet with its significant impacts on the economy and businesses worldwide. The COVID-19 spread worldwide in unprecedented ways due to its high infectious and contagious nature. As a result, the most outstanding medical challenge in the 21st century is yet to face worldwide. Though the emergence of the virus can be tracked back to Asia, many European countries and the U.S. have been struck massively by the pandemic. The virus has spread across all regions ranging from North America, Europe, Asia-Pacific, Middle East and Africa up to South America. The COVID- 19 has been declared a pandemic by World Health Organization (WHO) due to its increased spread globally. After the pandemic declaration, various countries announced the complete lockdown such as the Russia, Europe and Asian countries, to decrease its spread. Regardless of that, COVID-19 has increased the demand for robotics in supply chain and healthcare applications. According to the situation report of 12 April 2021 by WHO stated USD 135 million cases of the Coronavirus had been reported globally, and 2.9 million patients are dead due to the Coronavirus. South East Asia records cumulative cases of 16.17 million and death rates reached 0.2 million. In contrast, nearly 5 million doses of COVID-19 vaccines have been administered globally. The outbreak of COVID-19 has a massive impact on healthcare and at midyear; many innovative disinfection medical robots were announced every week trying to tackle the situation.
Price Impact
The COVID-19 had a devastating impact on the global economy. The several establishments have to remain shut while others scale down the operations or put on hold expansion plans as they tried to survive the unprecedented crisis. However, the demand for medical robotics in hospitals is increasing, considering the surgeries done in non-contact patient and healthcare workers environment, time efficiency, and more advantages. Robotics surgeries are known for various features such as better range of motion, better access to the operating area, reduced risk of pathogen spreads and infection. Despite many advancements and applications, there are only 4,000-5,000 robotic surgery centers worldwide because of high cost implementation requirements. The price of robotic surgery depends on surgery facilities and equipment in hospitals. Single medical robot cost around USD 2 million, whereas robotic surgery costs from USD 3,000 to USD 6,000. Considering the COVID-19 Pandemic and high requirement of medical and humanoid robots in hospitals the major market players are trying to manufacture products conveniently.
For instance,
· Californian Company ‘Intuitive Surgical’ is known for the best Medical Robot manufacture with their famous brand Da Vinci. The cost of the latest Da Vinci surgical robots costs around USD 2 Million price tags.
Impact on Demand
The COVID-19 pandemic has lifted the medical robotics market from its niche pedestal to the mainstream sector. Even before the pandemic, the latest advancement in AI and usage of robotics in the medical sector, including surgeries, were highly interested.
For instance,
· In 1983, the first surgical robot used was Arthrobot which performs as per voice commands assisted during orthopedic surgery in Canada
· In 1996, the first approved FDA-approved surgical robot ZEUS with tremor elimination and motion scaling was released by AESOP (Automated Endoscopic System for Optimal Positioning). This was the first medical robot to be used in long-distance laparoscopic cholecystectomy in New York for a French Patient
But the recent Coronavirus outbreak has further expanded the demand considering the major risk of doctors and frontline workers dealing with COVID-19 patients. Robotics has posed to be a successful shield in combatting the spread of the pathogen in hospitals and clinical centers. One of the major factors in the increasing demand for medical robots is the limitation of labor, thereby stating that the use of robots in the medical and surgical sectors can reduce contact between patients and healthcare providers/ doctors. The medical robots can also serve at maximum capacity during the required situations. As per the guidelines released by the government to reduce the pathogen spread, robotics are incorporated in various surgical sections where patients use during their hospital stay. Apart from surgeries, recently hospitals have taken initiatives in using medical robots for greeting patients, providing disinfectants and can provide food and medicines to patients thereby reducing patient and healthcare workers contact. The recent non-contact ultraviolet disinfection robots can widely reduce disinfection among hospital areas. Several companies operating in other domains are eager to enter and some have already entered the landscape of medical and surgical robotics to increase their revenue by meeting the emergent need of disinfection products for the virus infection.
The demand for medical robotics is rising to peek, enlightening the fact that these can mitigate pathogen spreading risk for healthcare workers, thereby decreases economic burden to a greater extend. Today’s surgeries are being performed even without having doctors physically in the operating room but with fewer staff members using robotic systems.
Impact on Supply Chain
The COVID-19 has created a significant impact on the supply chain of the medical robotics market. The sudden attack of COVID-19 and its subsequent implications for restrictions on trade and movement of goods has resulted in a shutdown of vast countries globally, resulting in disrupted supply chains due to limited materials and workforce, and slow down or stopping of manufacturing. Moreover, several manufacturing companies are retooling priority manufacturing to produce other essential medical supplies and equipment such as ventilators. But since medical robotics are in high demand by various healthcare sectors, the supply chain is again gaining speed; due to an increase in order from the consumers, the government allows the moments of transport vehicles to import and export the raw materials for the production of robots. Additionally, the manufacturers are also taking crucial steps to ensure the availability of raw materials by and also they have to look into the quality of products. Manufacturers need to take necessary steps about production processes, shifting to other facilities if required, changes in quality assurance, costs and procedures related to screening of workforce and offering of care if needed, changes in working hours, and others to maintain their supply chain.
The government has been firmly monitoring the supply chain to assume that the COVID-19 outbreak may adversely impact the supply chain of a medical product, including shortages of medical robots for various purposes in healthcare sectors in countries globally or potential disruptions in supply chains.
Many organizations are looking forward to improving and diversified the supply chain model to manage such a crucial situation. A diversified supply chain model including Robotic Process Automation is anticipated to improve the robotics supply to the highly required hospitals and surgical centers and increase end-to-end visibility.
The resulting COVID-19 pandemic has shown the various ways for supply chain management, which may be effective by robotics usage for numerous healthcare applications.
Conclusion
The impact of the novel COVID-19 virus is expected to leave a long-lasting effect on each healthcare sector. The outbreak prompted citizens to deal with confusion regarding the virus and its management. The virus poses a risk to human life and has caused economic distress and severe emotional strain. It produced a ripple effect that gave rise to a new collection of requirements and needs that were not needed earlier and the most essential one being the medical robotics which is highly needed in hospitals to minimize the contact between patient and healthcare workers to reduce the spread of pathogen.
COVID-19 pandemic outbreak has a positive impact on the growth of the medical robotics market due to non-contact patient surgeries and treatments. Moreover, many international governments, including U.S, China, Korea and Japan’s robotics organizations, focus exclusively on robotics in the medical and surgical arena and their manufacturing due to priority and essential requirements in this crucial period. Many government bodies and significant medical robotics market players are closely associated with patients and healthcare professionals for both side betterment considering contagious nature of virus and improvement of future economics.
#Medical Robotics Market#Medical Robotics Market Analysis#Medical Robotics Market Analysis in Developed Countries#Medical Robotics Market by Application#Medical Robotics Market by Type#Medical Robotics Market Forecast#Medical Robotics Future Innovation
0 notes
Link
via Politics – FiveThirtyEight
Dr. Royal S. Copeland, the field marshal in New York City’s battle against the 1918 influenza epidemic, knew his enemy was more than just a virus. As health commissioner, he oversaw a medical crisis that would eventually kill some 30,000 New Yorkers over three waves of the disease. In Copeland’s estimation, the problem was not only influenza but also the city’s crowded tenements and endemic poverty.
To modern eyes, the measures he took to stymie the spread might seem strange. In an extensive interview with The New York Times after the first wave of influenza had passed, Copeland touted the decision not to close New York’s public schools. It was, he reasoned, best to keep them open to give the city’s children respite from crowded apartments and, if need be, a point of access to the medical system. “We have practically 1,000,000 children in the public schools, about 750,000 of them from tenement homes. These homes are frequently unsanitary and crowded,” he said. “The children’s parents are occupied with the manifold duties involved in keeping the wolf from the door. No matter how loving they may be — and, of course, they are just as loving as any parents anywhere — they simply have not the time to give the necessary attention to the initial symptoms of disease.”
Even under normal circumstances, living in New York City requires a certain surrender of personal space: Subways are packed, apartments are small and bodegas get cramped with after-work shoppers. But not all New Yorkers have to live in a stressful crowd all the time, a fact the COVID-19 pandemic has laid all too bare. The city’s wealth inequality has always been apparent: financial safety nets, Whole Foods delivery and routine access to health care. But the pandemic has added a new layer to what affluence can afford some New Yorkers, including routine access to personal space and the flexibility that white-collar work allows. While over 100 years have gone by since the 1918 pandemic, some of Copeland’s worries about the difficult nature of city life — and the inequities of who lives the most comfortably — remain chillingly relevant.
We know already that the COVID-19 pandemic is affecting people of color more than white Americans. While the virus stalks the rich and poor — leading some to call it “the great equalizer” — those with lesser means have fewer places to hide from it. Dr. Andrew Goodman, a professor of public health at New York University who used to work for the city’s Health Promotion and Disease Prevention unit, pointed to the pandemic as “a more dramatic example of the health-inequity side of income inequality and racial inequality in the U.S.” Deaths from diseases that disproportionately affect minority communities, like diabetes and hypertension, “usually get spread out over time, and it doesn’t seem as dramatic,” Goodman said. “This is a more accelerated version.”
While there is a lot of uncertainty about the actual numbers of those infected — only a fraction of people who show symptoms are tested, so the rate of infection is almost certainly higher than what’s being reported — life in two New York City ZIP codes, one working class and one wealthy, gives us a glimpse into different ways of city living that might mean life or death in today’s New York.
Densely populated and working-class, East Elmhurst, Queens, has one of the highest rates of COVID-19 in New York City.
STEPHANIE KEITH / GETTY IMAGES
According to a running ProPublica tally of confirmed positive COVID-19 cases, the ZIP codes with the highest rate of infection are in a certain corner of Queens: East Elmhurst. One East Elmhurst ZIP code, 11370, is home to the notorious Rikers Island correctional facility, and has the highest recorded positive test rate in New York City — 127 percent worse than the city’s average. Jails like Rikers have become hotbeds for spreading the disease given their space constraints — well over 600 inmates and workers are infected with the virus at Rikers. East Elmhurst’s other, non-Rikers ZIP code, 11369, is a residential neighborhood and has the second worst positive test rate in the city, 121 percent greater than the average.
East Elmhurst has seen a high rate of individuals tested, and that might be in part because Elmhurst Hospital in neighboring Elmhurst, Queens — “the epicenter within the epicenter,” in the words of New York City Mayor Bill de Blasio — has set up a testing tent outside the hospital. According to 2018 data from the Census Bureau’s American Community Survey, 34,118 people live in the 1.1 square miles of East Elmhurst’s 11369 ZIP code. Sixty-four percent of its residents are Latino, and the median household income is $54,121, three-quarters of the median income in New York’s greater metro area. On the neighborhood’s northern border is LaGuardia Airport, and south of that are mosques and diners, a baseball field and blocks and blocks of houses cramped together. On those cramped blocks, the average household size is 3.2 people, 20 percent above the city average.
Nearly 11 percent of all households in ZIP code 11369 are also multigenerational, with three or more generations living under the same roof. It’s possible that the grouping of young and old together in one house could have something to do with higher infection rates. Researchers are still unclear about how many others a person infects when they have the virus, but early estimates were around 2 to 2.5 people. The elderly are more susceptible, and in Italy, doctors believe that the country’s culture of intergenerational living and familial closeness has had disastrous effects during the pandemic; Italy’s rate of death from COVID-19 is among the highest in the world.
Underlying conditions like asthma tend to be more prevalent in crowded environments, according to Dr. Y. Claire Wang, who specializes in public health and chronic disease prevention at the New York Academy of Medicine. The respiratory condition puts individuals at greater risk for COVID-19 complications, and households in city apartments with pests or mold, common problems in public housing units, often have higher rates of asthma, she said.
Things look different on the other side of the positive test rate list. ZIP code 11215 in Park Slope, Brooklyn, has among the city’s lowest rates of COVID-19, at 56 percent below average.1 Park Slope is a different New York from East Elmhurst in many ways. Two-thirds of its population is white, and at $123,583, the median household income is one and a half times greater than that of the average in New York’s greater metropolitan area. The neighborhood is named for its proximity to one of the city’s largest green spaces, Prospect Park, and it’s known for its gracious brownstones and tree-lined streets. The average household size in Park Slope is 2.4 people, and only 1.8 percent of households are multigenerational.
Residents of Park Slope, Brooklyn, tend to be affluent, with white-collar jobs easily adaptable to working from home.
ROY ROCHLIN / GETTY IMAGES
The racial and ethnic differences between Park Slope and East Elmhurst might prove particularly important as both neighborhoods weather the pandemic. Early statistical reports on the disease are already painting a picture of racial inequity. Earlier this week New York State released preliminary numbers that showed Latinos have the highest rate of COVID-19 fatality in New York City.
A Kaiser Family Foundation report on initial pandemic data reveals that minorities are bearing the brunt of infection and death from the virus in many places. Higher rates of chronic conditions in minorities put them at greater risk for serious complications from COVID-19. In Washington, D.C., where black residents make up 45 percent of the total population, they account for 29 percent of confirmed cases and 59 percent of deaths. In Michigan, black residents are 14 percent of the population, but represent 33 percent of confirmed cases and 41 percent of deaths.
“We say something as simple as ‘your ZIP code should not define your health’ — [but] in New York City, that’s often the story,” said Dr. Torian Easterling, the deputy commissioner of the Center for Health Equity and Community Wellness, a city agency that addresses racial and social inequities in health. He pointed to high rates of chronic diseases like diabetes and hypertension and a lack of access to healthy foods in minority communities as long-standing public health problems that have only been exacerbated by the onset of COVID-19.
During the 1918 pandemic, the white population had a higher rate of infection, according to a 2007 study of the outbreak by Thomas A. Garrett, then an economist at the St. Louis Federal Reserve. But that, Garrett surmised, had to do with the fact that the black population in the U.S. was still largely rural; the pandemic was a particular menace to cities. “[T]he nonwhite population in the United States has become much more urban. … A modern-day pandemic may result in greater nonwhite mortality rates because a greater percentage of the nonwhite population in the United States lives in urban areas,” he wrote. Census estimates from 2019 show that the majority of New York City residents are people of color.
Across New York, communities of color have long been more subject to chronic ailments like diabetes and hypertension. The COVID-19 pandemic has only exacerbated these trends.
JOHN NACION / NURPHOTO VIA GETTY IMAGES / ANGELA WEISS / AFP VIA GETTY IMAGES
Park Slope and the East Elmhurst ZIP code of 11369 are similarly dense, with roughly 32,000 and 31,000 people per square mile, respectively. But life in the neighborhoods is different in other ways that might contribute to their divergent rates of apparent COVID-19 infection. According to the latest Census Bureau count, the most prevalent jobs in East Elmhurst are clerical work, food service and construction. In Park Slope, management, entertainment, education and business are the most common professions. The typical East Elmhurst worker is required to leave home to perform their job, while the lines of work most common in Park Slope are adaptable to teleworking. And Latinos — East Elmhurst’s dominant ethnic group — are more likely than all other Americans to consider COVID-19 a threat to their financial stability, according to a recent Pew Research Center survey.
We’ve already seen how socioeconomic circumstances can correlate with Americans’ ability to stay at home. A recent New York Times analysis of anonymized cellphone data tracked the movements of Americans and found that those in the top 10 percent income bracket have limited their movements more than those in the bottom 10 percent. What Copeland said in 1918 could very likely still hold true: “I have no doubt that the most dangerous means of transmitting disease was the subway. … Many a man who was sick must have felt that he had to go to work.”
Copeland’s struggle against the currents of poverty and influenza would continue into 1920. Updating the public on the state of the epidemic, which had reemerged, Copeland told The New York Times that the health department was working to stop the eviction of tenants during the outbreak and described the struggle to attract nurses to the city’s hospitals, since wealthy individuals were offering them higher pay to work in private homes. He pleaded for better ventilation on subways and buses and criticized coffin-makers who were price-gouging the city’s residents. Even in death, New York was unrelenting.
And so it remains today. Early this week, the city announced that hospital morgues around New York were overflowing with the dead. An Associated Press report painted a grim picture of one Brooklyn hospital. Even with an infection rate much lower than those in Queens, “mounds of corpses” had become so difficult to navigate that hospital staff were stepping over them.
The great equalizer isn’t COVID-19 — it’s death. But in New York’s epidemic, death attends to the haves and have-nots differently: For the city’s poor, it hovers closely, and when it comes, it leaves them as crowded as ever.
2 notes
·
View notes
Last Seen Blogs

megaworldprojectsbyaldyneki-blog
Megaworld Projects

aramai-goshawk
aramai goshawk

lipstickthuggin-blog
Untitled

adafruit
adafruit

x-unnamedgraves-x
emo never dies