#compare health insurance policies
Text
A Comprehensive Guide to Comparing Insurance Policies
Compare Insurance Policies: Insurance is a critical component of financial planning, providing protection and peace of mind against unforeseen events.
However, with numerous insurance providers and policy options available, choosing the right coverage can be overwhelming.
How To Compare Insurance Policies
In this guide, we’ll explore how to compare insurance policies effectively, step by step,…

View On WordPress
#auto insurance#best auto insurance#best life insurance policies in india#best term insurance#car insurance#cash value life insurance#cheap car insurance#compare business insurance policies#compare commercial auto insurance policies#compare commercial insurance policies#compare general liability insurance policies#compare health insurance policies#compare insurance policies#compare small business insurance policies#health insurance#health insurance 101#health insurance explained#home insurance#insurance#insurance advice#insurance policies#insurance policy#insurance quote#life insurance#life insurance 101#life insurance agent#life insurance policies#term insurance#term life insurance#think insurance
0 notes
Text
my stepmother’s emotional state never stops amazing me
#why are you like that...... how are you like that and still alive#finally aged out of my dads health insurance and i guess they got the notification of this in their mail#because my dad is the policy holder therefore they sent it to His address#but it since it had my name on it my stepmother stuffed the whole thing into one of those big orange envelopes#and payed money to send it to me with a note that said ''change your mailing address.''#bonnie.... i changed my mailing address to my boyfriends parents house when i was like 17 lmao....#i have not received mail to your house in nearly a decade...........#she hates me soo so much even a reminder that i exist is enough to send her into a passive aggressive rage#im sorry???? you made a decision as a full grown middle aged woman???#to marry a man who traumatized himself abusing his first wife so hard she offed herself to get away from him??????#and that this trauma manifests as a very weird emotional projection of his guilt and grief onto his dead wife's daughter#sorry you're aware of the fact that you are an emotional band aid for an irredeemably fucked up man and mean nothing to him comparatively???#you got married in the same church they held my mother's funeral in not even 9 months after she died....#i really don't know what you thought you were getting lmao#mau
4 notes
·
View notes
Text
#travel#insurance#international#abroad#plan#boarding#costs#refundable#coverage#credit#cards#policies#expenses#medical#baggage#trip#cancellation#rewards#luggage#travelers#compare#deductible#health#claims#comprehensive#buy#weather
0 notes
Text
Know how to compare health insurance plans.
There are different terms which are important to know before you compare health insurance policy and choose a plan for your near and dear ones. We cover all of it here.
0 notes
Text
In this world of uncertainties, while losses can be hard, insurance can compensate you monetarily. You can insure your life, automobiles, buildings, furniture and much more. Insurance is a subject matter of financial protection based on insurable interest. Deciding the insurance cover and type of insurance plan can be a task. This is where you might feel the need to consult experts like RURASH.
#Buy Health#Term#Life#and General Insurance Plans Online#best health insurance plan#health insurance plans#online health insurance#compare & buy best health insurance plans online in India#best health insurance plans in India#buy medical insurance policy online#health insurance plans for family#buy insurance policy online in India#Buy Insurance Services Online#insurance plans and services online mumbai#Best Buy Insurance Plans online#How to buy health insurance#Buy insurance services online in India
0 notes
Text
How To Compare Affordable Health Insurance Plans Online In India?
With the rapid advancements in technology, finding the right health insurance plan online is no longer difficult. It has become elementary and convenient. With so many options available on the internet, you can compare insurance plans online to choose the one that suits your requirements perfectly.
Now, let us take a look at some of how you can compare health insurance plans online:Once you have a list of all the health insurance plans available, it is time to pick one. This can be an overwhelming process. But if you take some time to understand what each plan offers and compare insurance policy prices before making your decision, it will be much easier to choose the best option for yourself.
0 notes
Text
Cigna’s nopeinator

I'm touring my new, nationally bestselling novel The Bezzle! Catch me THURSDAY (May 2) in WINNIPEG, then Calgary (May 3), Vancouver (May 4), Tartu, Estonia, and beyond!

Cigna – like all private health insurers – has two contradictory imperatives:
To keep its customers healthy; and
To make as much money for its shareholders as is possible.
Now, there's a hypothetical way to resolve these contradictions, a story much beloved by advocates of America's wasteful, cruel, inefficient private health industry: "If health is a "market," then a health insurer that fails to keep its customers healthy will lose those customers and thus make less for its shareholders." In this thought-experiment, Cigna will "find an equilibrium" between spending money to keep its customers healthy, thus retaining their business, and also "seeking efficiencies" to create a standard of care that's cost-effective.
But health care isn't a market. Most of us get our health-care through our employers, who offer small handful of options that nevertheless manage to be so complex in their particulars that they're impossible to directly compare, and somehow all end up not covering the things we need them for. Oh, and you can only change insurers once or twice per year, and doing so incurs savage switching costs, like losing access to your family doctor and specialists providers.
Cigna – like other health insurers – is "too big to care." It doesn't have to worry about losing your business, so it grows progressively less interested in even pretending to keep you healthy.
The most important way for an insurer to protect its profits at the expense of your health is to deny care that your doctor believes you need. Cigna has transformed itself into a care-denying assembly line.
Dr Debby Day is a Cigna whistleblower. Dr Day was a Cigna medical director, charged with reviewing denied cases, a job she held for 20 years. In 2022, she was forced out by Cigna. Writing for Propublica and The Capitol Forum, Patrick Rucker and David Armstrong tell her story, revealing the true "equilibrium" that Cigna has found:
https://www.propublica.org/article/cigna-medical-director-doctor-patient-preapproval-denials-insurance
Dr Day took her job seriously. Early in her career, she discovered a pattern of claims from doctors for an expensive therapy called intravenous immunoglobulin in cases where this made no medical sense. Dr Day reviewed the scientific literature on IVIG and developed a Cigna-wide policy for its use that saved the company millions of dollars.
This is how it's supposed to work: insurers (whether private or public) should permit all the medically necessary interventions and deny interventions that aren't supported by evidence, and they should determine the difference through internal reviewers who are treated as independent experts.
But as the competitive landscape for US healthcare dwindled – and as Cigna bought out more parts of its supply chain and merged with more of its major rivals – the company became uniquely focused on denying claims, irrespective of their medical merit.
In Dr Day's story, the turning point came when Cinga outsourced pre-approvals to registered nurses in the Philippines. Legally, a nurse can approve a claim, but only an MD can deny a claim. So Dr Day and her colleagues would have to sign off when a nurse deemed a procedure, therapy or drug to be medically unnecessary.
This is a complex determination to make, even under ideal circumstances, but Cigna's Filipino outsource partners were far from ideal. Dr Day found that nurses were "sloppy" – they'd confuse a mother with her newborn baby and deny care on that grounds, or confuse an injured hip with an injured neck and deny permission for an ultrasound. Dr Day reviewed a claim for a test that was denied because STI tests weren't "medically necessary" – but the patient's doctor had applied for a test to diagnose a toenail fungus, not an STI.
Even if the nurses' evaluations had been careful, Dr Day wanted to conduct her own, thorough investigation before overriding another doctor's judgment about the care that doctor's patient warranted. When a nurse recommended denying care "for a cancer patient or a sick baby," Dr Day would research medical guidelines, read studies and review the patient's record before signing off on the recommendation.
This was how the claims denial process is said to work, but it's not how it was supposed to work. Dr Day was markedly slower than her peers, who would "click and close" claims by pasting the nurses' own rationale for denying the claim into the relevant form, acting as a rubber-stamp rather than a skilled reviewer.
Dr Day knew she was slower than her peers. Cigna made sure of that, producing a "productivity dashboard" that scored doctors based on "handle time," which Cigna describes as the average time its doctors spend on different kinds of claims. But Dr Day and other Cigna sources say that this was a maximum, not an average – a way of disciplining doctors.
These were not long times. If a doctor asked Cigna not to discharge their patient from hospital care and a nurse denied that claim, the doctor reviewing that claim was supposed to spend not more than 4.5 minutes on their review. Other timelines were even more aggressive: many denials of prescription drugs were meant to be resolved in fewer than two minutes.
Cigna told Propublica and The Capitol Forum that its productivity scores weren't based on a simple calculation about whether its MD reviewers were hitting these brutal processing time targets, describing the scores as a proprietary mix of factors that reflected a nuanced view of care. But when Propublica and The Capitol Forum created a crude algorithm to generate scores by comparing a doctor's performance relative to the company's targets, they found the results fit very neatly into the actual scores that Cigna assigned to its docs:
The newsrooms’ formula accurately reproduced the scores of 87% of the Cigna doctors listed; the scores of all but one of the rest fell within 1 to 2 percentage points of the number generated by this formula. When asked about this formula, Cigna said it may be inaccurate but didn’t elaborate.
As Dr Day slipped lower on the productivity chart, her bosses pressured her bring her score up (Day recorded her phone calls and saved her emails, and the reporters verified them). Among other things, Dr Day's boss made it clear that her annual bonus and stock options were contingent on her making quota.
Cigna denies all of this. They smeared Dr Day as a "disgruntled former employee" (as though that has any bearing on the truthfulness of her account), and declined to explain the discrepancies between Dr Day's accusations and Cigna's bland denials.
This isn't new for Cigna. Last year, Propublica and Capitol Forum revealed the existence of an algorithmic claims denial system that allowed its doctors to bulk-deny claims in as little as 1.2 seconds:
https://www.propublica.org/article/cigna-pxdx-medical-health-insurance-rejection-claims
Cigna insisted that this was a mischaracterization, saying the system existed to speed up the approval of claims, despite the first-hand accounts of Cigna's own doctors and the doctors whose care recommendations were blocked by the system. One Cigna doctor used this system to "review" and deny 60,000 claims in one month.
Beyond serving as an indictment of the US for-profit health industry, and of Cigna's business practices, this is also a cautionary tale about the idea that critical AI applications can be resolved with "humans in the loop."
AI pitchmen claim that even unreliable AI can be fixed by adding a "human in the loop" that reviews the AI's judgments:
https://pluralistic.net/2024/04/23/maximal-plausibility/#reverse-centaurs
In this world, the AI is an assistant to the human. For example, a radiologist might have an AI double-check their assessments of chest X-rays, and revisit those X-rays where the AI's assessment didn't match their own. This robot-assisted-human configuration is called a "centaur."
In reality, "human in the loop" is almost always a reverse-centaur. If the hospital buys an AI, fires half its radiologists and orders the remainder to review the AI's superhuman assessments of chest X-rays, that's not an AI assisted radiologist, that's a radiologist-assisted AI. Accuracy goes down, but so do costs. That's the bet that AI investors are making.
Many AI applications turn out not to even be "AI" – they're just low-waged workers in an overseas call-center pretending to be an algorithm (some Indian techies joke that AI stands for "absent Indians"). That was the case with Amazon's Grab and Go stores where, supposedly, AI-enabled cameras counted up all the things you put in your shopping basket and automatically billed you for them. In reality, the cameras were connected to Indian call-centers where low-waged workers made those assessments:
https://pluralistic.net/2024/01/29/pay-no-attention/#to-the-little-man-behind-the-curtain
This Potemkin AI represents an intermediate step between outsourcing and AI. Over the past three decades, the growth of cheap telecommunications and logistics systems let corporations outsource customer service to low-waged offshore workers. The corporations used the excuse that these subcontractors were far from the firm and its customers to deny them any agency, giving them rigid scripts and procedures to follow.
This was a very usefully dysfunctional system. As a customer with a complaint, you would call the customer service line, wait for a long time on hold, spend an interminable time working through a proscribed claims-handling process with a rep who was prohibited from diverging from that process. That process nearly always ended with you being told that nothing could be done.
At that point, a large number of customers would have given up on getting a refund, exchange or credit. The money paid out to the few customers who were stubborn or angry enough to karen their way to a supervisor and get something out of the company amounted to pennies, relative to the sums the company reaped by ripping off the rest.
The Amazon Grab and Go workers were humans in robot suits, but these customer service reps were robots in human suits. The software told them what to say, and they said it, and all they were allowed to say was what appeared on their screens. They were reverse centaurs, serving as the human faces of the intransigent robots programmed by monopolists that were too big to care.
AI is the final stage of this progression: robots without the human suits. The AI turns its "human in the loop" into a "moral crumple zone," which Madeleine Clare Elish describes as "a component that bears the brunt of the moral and legal responsibilities when the overall system malfunctions":
https://estsjournal.org/index.php/ests/article/view/260
The Filipino nurses in the Cigna system are an avoidable expense. As Cigna's own dabbling in algorithmic claim-denial shows, they can be jettisoned in favor of a system that uses productivity dashboards and other bossware to push doctors to robosign hundreds or thousands of denials per day, on the pretense that these denials were "reviewed" by a licensed physician.

If you'd like an essay-formatted version of this post to read or share, here's a link to it on pluralistic.net, my surveillance-free, ad-free, tracker-free blog:
https://pluralistic.net/2024/04/29/what-part-of-no/#dont-you-understand
#pluralistic#cigna#computer says no#bossware#moral crumple zones#medicare for all#m4a#whistleblowers#dr debby day#Madeleine Clare Elish#automation#ai#outsourcing#human in the loop#humans in the loop
235 notes
·
View notes
Text
The casual cruelty with which Columbia administrators rushed to do the bidding of their reactionary masters in Congress provides a quick lesson in who actually is the elite, and who is not. The students at the fancy college, it turns out, do not in fact run the fancy college. The university doesn’t treat them as bosses, and barely even as stakeholders. Instead, it treats them as subjects to be disciplined—and in disciplining them, it has a wide range of tools. Students are a kind of indentured employee; they are dependent on the university for housing, for health insurance, for the next steps in their career and life plans. If the university decides they are not sufficiently docile, it is trivially easy for the university to destroy their lives.
Everyone pretty much knows that young people have few resources and few levers of influence. We’re all aware that even supposedly rich kids don’t actually have control of their parent’s bank accounts and can be cut loose with nothing on a whim. We all know that young people have few connections and little influence compared to Congresspeople, administrators, and angry donors. And it is because people know that college students have little power that they become enraged when college students attempt to organize or demand some say in institutional or (god forbid) national policies.
Young people are “elites” not because they actually have power, but because the spectacle of them asserting autonomy in any way is at odds with the way things are supposed to be. They are pretentious for the same reason that women or LGBT people or Black people are considered pretentious elites when they contradict their supposed betters. When the right people have power; that’s natural; when the wrong people, marginalized people, have power—that’s an unbearable imposition.
It's easy to make light of college student activism, and to insinuate that people attending a swanky university can’t really have anything to protest about. But young people engage in activism for the same reason other marginalized people engage in activism; they have firsthand experience of inequality and injustice, and because they are treated unequally, they don’t have a lot of other ways to demand accountability or change. The vitriol directed at young people is not because young people are powerful; it’s because they aren’t, and so their assertions of autonomy are seen as a threat to established hierarchies.
99 notes
·
View notes
Text
FOR ANYONE IN FLORIDA:
Governor Ronald McDonald McDipshit is trying to require public colleges to hand over info on transgender (or, I assume, otherwise gender-nonconforming) students.
Under both FERPA (Family Educational Rights and Privacy Act) and HIPAA (Health Insurance Portability and Accountability Act), this is illegal.
FERPA protects your college records if that college receives federal funding. Under FERPA, even your parents cannot request your grades, your classes, or your medical records in the hands of the college (among other things). Circumstances under which records can be shared without your authorization are limited:
"FERPA generally prohibits disclosure without consent, either internally or externally, of personally identifiable information from education records. But it permits (although it does not require) such disclosure without consent in certain situations. These include:
1. to other school officials, including teachers, within the institution who the college determines have legitimate educational interests;
2. to the parents of a student under age 21 concerning the student's violation of any federal, state, or local law or school policy or rule governing alcohol or drug use or possession; and
3. in connection with a health or safety emergency."
(https://www.cga.ct.gov/2005/rpt/2005-R-0195.htm)
HIPAA applies to all medical records, whether held by a college, a hospital, or a private doctor's office. Again, there are guidelines for exactly when your information can be shared without express, written permission from you:
"The Privacy Rule sets rules and limits on who can look at and receive your health information
To make sure that your health information is protected in a way that does not interfere with your health care, your information can be used and shared:
For your treatment and care coordination
To pay doctors and hospitals for your health care and to help run their businesses
With your family, relatives, friends, or others you identify who are involved with your health care or your health care bills, unless you object
To make sure doctors give good care and nursing homes are clean and safe
To protect the public's health, such as by reporting when the flu is in your area
To make required reports to the police, such as reporting gunshot wounds"
In other words, DeSantis cannot legally access your medical (or other college) records, either through the college itself, a hospital, or an individual.
Both FERPA and HIPAA are federal programs, so they apply no matter where you are in the US and how much DeSantis stomps his little feet and yells. FERPA protects your educational records; HIPAA protects your medical records (specifically, PHI, or Protected Health Information). DeSantis could ask to know how many people at the Mickey Mouse Medical Hospital have received prescriptions for hormones, had top or bottom surgery, etc., but he cannot demand access to your name, SSN, birthdate, specific treatment records, etc., unless you provide written authorization for him to do so. Along the same lines, he could demand the College of Rats in the Kitchen and Gators on the Stage tell him how many students total identify as transgender, nonbinary, genderfluid, gender non-conforming, etc. He could even ask for the average GPA of trans students compared to cis students (as a whole). But he cannot - again - ask for your personal records, or any of the information therein, without your express permission.
Don't panic, okay? I know the federal government isn't always trustworthy, but I've spent enough time dealing with both FERPA and HIPAA to know that they take this stuff very seriously. If you need to contact someone about a violation of either -
FERPA (college records) is under the US Department of Education, and you can find more info on reporting a potential violation here:
HIPAA (which covers all your medical info) is under the US Health and Human Services' Office of Civil Rights, and you can find more info on reporting a violation here:
At the moment, DeSantis is requesting only information not covered by either HIPAA or FERPA: "Republican Florida Gov. Ron DeSantis is asking state universities for the number and ages of their students who sought gender dysphoria treatment, including sex reassignment surgery and hormone prescriptions, according to a survey released Wednesday."
Source:
If you are concerned that your records either as a student or a patient may have been shared without your permission, either because of this or in any other circumstance, you have rights.
Hang in there.

705 notes
·
View notes
Text
Some Gen Zers have grown critical of capitalism in recent years.
Rather than dismiss the whole system, many are embracing an idea one researcher calls "safety capitalism."
Gen Zers are less likely to take certain risks, which could be one reason they want more of a social safety net.
When someone loses their job or can't work for health reasons, how much government support should they receive? If you ask many Gen Zers that question, they'll say the current social safety net is insufficient.
Christina Elson, executive director of the Center for the Study of Capitalism at Wake Forest University, told Business Insider that many young people have embraced an idea she calls "safety capitalism."
The theory behind safety capitalism is that a successful capitalist system can and should provide sufficient protection — or safety — for those who need support following circumstances like a job loss or illness. One of the key questions facing any economic system is, "What should failure look like," Elson asked.
While many Americans receive support from a variety of social programs such as unemployment, food stamps, or disability, some of these have been scaled back since the height of the pandemic. As things stand, many Gen Zers think the US's social safety net is inadequate.
Sixty-five percent of Gen Zers think the government should provide a job to anyone who wants one, according to a Wake Forest survey of 2,000 Gen Zers and millennials conducted with YouGov in 2022. Forty-five percent said they had a positive impression of universal basic income policies. In a 2023 survey conducted by the same group, 65% percent of Gen Zers said unemployment payments should match one's salary.
Most Gen Zers still support capitalist ideas like private home ownership and entrepreneurship, Elson said. But many are frustrated with how the high costs of things like healthcare, housing, and education have taken a financial toll on Americans — and think these systems could benefit from more government intervention.
"You hear about 'billionaires should be outlawed' — that really isn't the issue," Elson previously told BI regarding Gen Zer's concerns. "The issue is the bottom. What is the appropriate bottom living standard for an American citizen, and what role should the government have in ensuring that people don't fall below that?"
Some are even turning away from capitalism altogether. In a Business Insider survey conducted last July of over 1,800 Americans, 28% of Gen Z respondents said they somewhat or strongly preferred the economic system of socialism over capitalism, the most of any generation. Twenty-nine percent of Gen Zers preferred capitalism — the rest didn't have a preference or weren't sure.
Why Gen Z wants an expanded safety net
Compared to past generations, young people today are less likely to drive, drink, have sex, and more likely to live at home, per some surveys. Elson said these examples point to a level of risk aversion that may be unique to Gen Zers.
"Gen Z are 'younger for longer,' — they go out into the world slower," she said, adding, "What is it that this generation needs in order to feel that they're able to go out there and take risks?"
Elson said many Gen Zers seek a "redesign of social safety" to enhance what some feel is an outdated system. For example, unemployment insurance and Social Security were introduced nearly 90 years ago during the Great Depression.
The financial challenges currently facing the Social Security system — due in part to the US's aging population — are arguably further evidence of a system that's in need of reform.
"All of this network has been designed for another time and place," Elson said.
Exactly what, if any, changes the US should make to its social safety net is up for debate. Some young people may look to Europe, where countries generally have a larger social safety net than the US.
In Germany, eligible unemployed individuals receive between 60% and 67% of their previous salary for up to a year. Policies like universal health insurance and guaranteed sick leave are also more common in Europe. Before temporary changes were enacted during the pandemic, most US states offered six months of unemployment benefits, with Americans collecting an average of $372 a week, per PBS.
Regardless, Elson said it's important that the US's entrepreneurial culture — which can reward risk-taking and drive economic progress — remains intact.
Most businesses fail, but as prominent investor Charlie Munger once said — and Elson referenced in a recent post — a level of failure may be necessary to have a thriving economy.
"Capitalism without failure is like religion without hell," Munger said.
19 notes
·
View notes
Text
The Weather
While not in the US, an article from CBC News in Canada offers a look into the upcoming respiratory illness season. Data from Internal Alberta Health Services shows that patients hospitalized with COVID passed 900 and “roughly doubled” in a month. Accurate data are hard to find, however, as the provincial government changed how COVID statistics are reported. Cameron Westhead, second vice-president with United Nurses of Alberta, commented, “This government likes to talk about personal responsibility and making decisions that are best for yourself and your family. But we don’t have the data to make those kinds of decisions.”
In addition, an outbreak in the community has the potential to overwhelm hospital systems again. Isolation requirements, PPE needs, and healthcare worker burnout are all major concerns with COVID patients. Rather than stripping healthcare of the precautions we need to control the ongoing pandemic, we must advocate for more support for healthcare workers, masks in healthcare, and acknowledgment of the severity of COVID infections.
Wastewater
We continue to wait for Verily, the organization taking over the National Wastewater Surveillance System (NWSS) contract from Biobot, to provide a readable Nationwide representation of the current wastewater levels.
According to WastewaterSCAN, COVID wastewater concentration is medium nationally, apart from high levels in the Northeast. As of October 16, 2023, the national average of wastewater levels is 216.9 PMMoV Normalized. Regionally, the Midwest is 317.0 PMMoV Normalized, the Northeast is 589.82 PMMoV Normalized, the South is 152.3 PMMoV Normalized, and the West is 164.7 PMMoV Normalized. We emphasize that Wastewater SCAN has fewer wastewater sites represented as compared to Biobot. Combined with some other caveats, including the difficulty of interpreting their plots, we remain skeptical of Wastewater SCAN’s data.
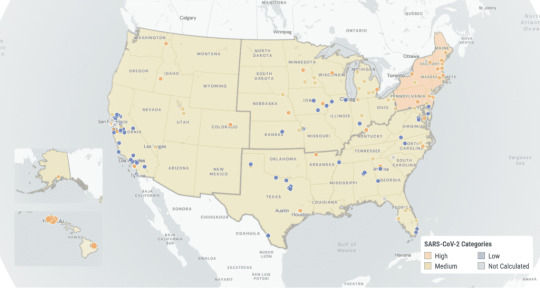

The above graphic shows the overall trend for the United States. The y-axis is a scale for the quantity of nucleic acids, PMMoV Normalized (x1 million). While concentrations have been trending downward–with a possible recent uptick–we urge the importance of layers of protection. As the Northern Hemisphere enters winter and many folks celebrate holidays, please protect yourself and others with masking, distancing, clean air, vaccines, and other layers of protection. For more on layers of protection, refer to this writeup on PeoplesCDC.org.
Vaccines
NPR reports that parents are finding it difficult to find pediatric doses of the new COVID vaccines for their children. The CDC reports that pediatric doses are available, but several factors are limiting their spread. Faulty websites or outdated information from public and private organizations, shipping delays or errors in the number of doses shipped, and issues with public and private insurance all contribute to a lackadaisical approach to public health. Parents are frustrated at the situation and scared for their kids, especially as we enter flu season.
We hope that if you haven’t been able to receive an updated 2023-2024 COVID vaccine, you are able to access a dose soon. If you have questions about insurance coverage, visit the KFF information page here. For children covered under state insurance, see information about the Vaccines for Children program. Uninsured adults may receive assistance through the Bridge Access Program. Please note not every pharmacy or clinic participates in this important program.
Long COVID
An article from the University of Minnesota’s Center for Infectious Disease Research and Policy (CIDRAP) argues that Long COVID studies in children are lacking. Estimates of prevalence of Long COVID in children range from 1% to 70%. Children may have different experiences with Long COVID from adults, as well as having limited vocabulary to describe their symptoms. Poor study design also contributes to artificially low numbers. Hannah Davis, co-founder of the Patient-Led Research Collaborative, suggests that further studies could use a prepandemic cohort or electronic health record data to serve as controls rather than a cohort defined by negative PCR tests, which could contain false negatives. Additionally, more longitudinal studies are needed. The article highlights a huge range of uncertainty reflecting a lack of research. Children with Long COVID deserve recognition, care, and support.
Take Action
Reminder to either submit a written comment or register to give an oral comment to the CDC’s HICPAC meeting on November 2-3, 2023. National Nurses United provided some guidance on talking points one can use during the oral comments. You can submit written comments to [email protected] starting November 1, 2023, with the deadline at 11:59 pm on November 6, 2023. To request time for an oral comment during the webcast, submit your request to the oral comment submission form no later than 11:59 p.m., EST, October 23, 2023.
As the CDC is poised to weaken protections for patients and healthcare workers, please sign on with National Nurses United and demand the CDC be transparent. At the link, you can fill out a form to send an email to CDC/HICPAC leaders that emphasizes the need to post the updated guidelines in full for public review, make meetings and comments open to the public, and use a science-based approach to aerosol transmission.
Notes: 1) The numbers in this report were current as of 10/20/2023. 2) Changes in testing access as well as data reporting have led many federal data sources to become less reliable. 3) Wastewater data are being sourced from WastewaterSCAN and no longer from BioBot due to the end of the contract with the CDC. 3) Check out the links throughout & see our website for more!
#op#covid#covid 19#covid isn't over#covid19#coronavirus#pandemic#pcdc#people's cdc#long covid#public health#covid vaccine#covid-19#medical#img#described in alt text
22 notes
·
View notes
Text

happy Dussehra
#happydussehra#dussehra#navratri2023#compare policy#health insurance#health insurance benefits#life insurance plans#health insurance plan#festival#term insurance#healthcare#health#term insurance plan#festiveseason#festivevibes
0 notes
Text
#Buy Health#Term#Life#and General Insurance Plans Online#best health insurance plan#health insurance plans#online health insurance#compare & buy best health insurance plans online in India#best health insurance plans in India#buy medical insurance policy online#health insurance plans for family#buy insurance policy online in India#Buy Insurance Services Online#insurance plans and services online mumbai#Best Buy Insurance Plans online#How to buy health insurance#Buy insurance services online in India
0 notes
Text
Best for industrial law and labour law for HR

HR labor law is the area where employment-related legal requirements and HR management practices converge. This area is crucial for making sure businesses manage their workforces efficiently and adhere to all relevant rules and regulations. The following are some salient features of HR labor law.
Hiring and Recruitment: HR practitioners must be aware of the laws pertaining to hiring and recruitment procedures, such as those pertaining to equal employment opportunity (EEO) and anti-discrimination, as well as those regulating the hiring of foreign nationals and minors.
Employment Agreements and Contracts: HR specialists are frequently in charge of creating and managing employment agreements, which may contain provisions pertaining to pay, benefits, working hours, and layoff policies. They are responsible for making sure that these contracts abide by all applicable labor laws and rules.
Wages and Hours: HR departments are in charge of making sure that rules pertaining to minimum wage, overtime compensation, and other requirements pertaining to remuneration are followed. This entails abiding with rules like the Fair Labor Standards Act (FLSA) in the US or comparable laws in other nations.
Workplace Safety and Health: By putting policies and processes in place that go by occupational safety and health standards, HR professionals help to promote workplace safety and health. They might also assist in organizing safety procedure training and managing workers' compensation claims.
HR departments are frequently tasked with handling matters related to employee relations, including as grievances, disciplinary actions, and conflicts. They have to make sure that employee rights are upheld and that disciplinary actions adhere to labor regulations.
Employee Benefits and Leave: Human resources specialists oversee benefit schemes like health insurance, paid time off, and retirement plans. Laws pertaining to the administration of benefits, such as those governing leave entitlements like the Family and Medical Leave Act (FMLA), must be understood by them.
Termination and Layoffs: HR specialists are in charge of managing employee terminations, including any necessary layoffs or downsizing projects. They have to make sure that all termination procedures adhere to labor rules, including giving notice and paying severance when necessary.
Employee Privacy and Data Protection: When handling sensitive employee data, HR departments are in charge of protecting employee privacy and making sure that data protection rules are followed.
Union Relations: HR specialists may be involved in collective bargaining discussions, contract administration, and handling in companies where workers are members of a union.
To know "How many labour laws are there ?" click here
6 notes
·
View notes
Text

At least 59.4 percent of illegal immigrant-led homes use one or more welfare programs, compared with 39 percent of households headed by people born in the United States, according to the Dec. 19 report.
High rates of welfare use among illegal immigrants “primarily reflect their generally lower education levels and their resulting low-incomes, coupled with the large share who have U.S.-born children who are eligible for all welfare programs from birth,” the report reads.
“More than half of all illegal immigrant households have one or more U.S.-born children.”
Children born to illegal immigrants in the United States, also known as “anchor babies,‘ are considered to have automatic birthright citizenship even though the U.S. Supreme Court hasn’t explicitly ruled on the matter. Illegal immigrants can’t access most welfare programs, a restriction that eases for their children who are born in the country.
“The American welfare system is designed in large part to help low-income families with children, which describes a large share of immigrants,” CIS states in the report.
A dozen states offer Medicaid to all low-income children regardless of immigration status. Such children also have access to various government food and meal programs.
Programs such as Temporary Assistance for Needy Families, the Women, Infants, and Children nutrition program, free or subsidized lunch and breakfast for students, and Medicaid for children (Children’s Health Insurance Program) were “explicitly created for minors,” the report states.
The CIS report is based on data from the U.S. Census Bureau’s 2022 Survey of Income and Program Participation (SIPP).
“The reality is that illegal immigrants are included in the SIPP, a large share of them are poor, and they or their U.S.-born children have welfare eligibility; and many take advantage of this eligibility,” CIS stated.
“A very large share of immigrants come to America, have children, struggle to provide for them, and so turn to taxpayers for support. This can be seen as especially problematic given that there is already a large number of Americans who are also struggling to provide for their children.”
According to data from the Federation for American Immigration Reform (FAIR), the total number of U.S.-born children of illegal aliens in the United States as of June stood at 5.78 million, a population more than two times that of Chicago.
FAIR estimates that “illegal aliens and their U.S.-born children impose a net annual cost of $150.6 billion on American taxpayers as of the beginning of 2023.” Over the past five years, the annual cost has risen by almost $35 billion.
“This burden will only continue to grow as a result of the Biden administration’s open-borders policies,” the organization warns.
Ending Birthright Citizenship
Multiple GOP members have taken a strong stance against birthright citizenship. In 2018, former President Donald Trump said he would remove birthright citizenship via executive order, which didn’t happen.
In his 2024 campaign, President Trump has reiterated his position on the matter. In a May video, President Trump promised to sign an executive order on day one of his second term to solve the issue.
Such an order would end the “unfair practice known as birth tourism, where hundreds of thousands of people from all over the planet squat in hotels for their last few weeks of pregnancy to illegitimately and illegally obtain U.S. citizenship for the child, often to later exploit chain migration to jump the line and get green cards for themselves and their family members.”
“At least one parent will have to be a citizen or a legal resident in order to qualify,” President Trump stated.
Republican presidential candidate Vivek Ramaswamy called for an end to birthright citizenship for children of illegal immigrants during the second GOP debate, in September.
“Now, the left will howl about the Constitution and the 14th Amendment. The difference between me and them is I’ve actually read the 14th Amendment. And what it says is that all persons born or naturalized in the United States and subject to the laws and jurisdiction thereof are citizens,” Mr. Ramaswamy said.
“So nobody believes that the kid of a Mexican diplomat in this country enjoys birthright citizenship—not a judge or legal scholar in this country will disagree with me on that. Well, if the kid of a Mexican diplomat doesn’t enjoy birthright citizenship, then neither does the kid of an illegal migrant who broke the law to come here.”
In July, Rep. Matt Gaetz (R-Fla.) introduced a proposal called “End Birthright Citizenship Fraud Act of 2023,” which aims to abolish automatic birthright citizenship for U.S.-born children of illegal immigrants.
Under the legislation, at least one parent of the child must be a U.S. national or a refugee, have lawful permanent citizenship, or be an active member of the military.
“My legislation recognizes that American citizenship is a privilege—not an automatic right to be co-opted by illegal aliens,” Mr. Gaetz said in a statement.
“This is an important step in preserving the sanctity of American citizenship and ensures that citizenship is not treated as a loophole to be exploited but rather a privilege to be earned when legally migrating to our country.”
4 notes
·
View notes
Text
Its studies pre-suppose that Israeli policies are fatally hurting Palestinian health and work. And when biased people look for evidence of their thesis, they can invariably find it - as long as they ignore any counter-evidence.
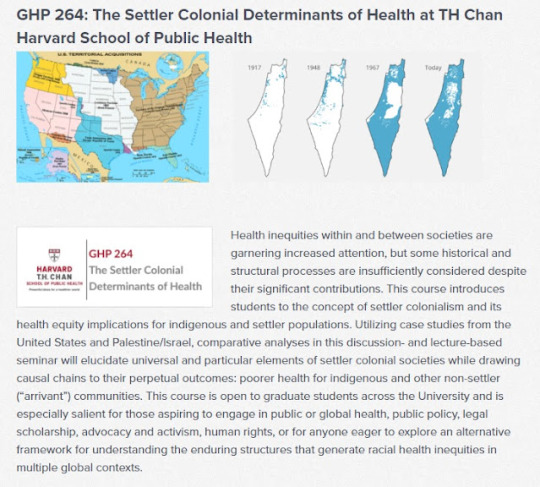
Similarly, Harvard's School of Public Health offers a course that looks at Palestinian health through the lens of Israeli "settler colonialism" making the initial assumption that health services are drastically impacted by Israeli policies.
Yes, a Harvard University course actually highlights "The Map that Lies" that has been thoroughly debunked and retracted by numerous organizations.
Yet in real life, Palestinian healthcare - and indeed, Palestinians' general quality of life - is better than that of neighboring Jordan which does not suffer from "settler colonialism" or "Israeli apartheid:"
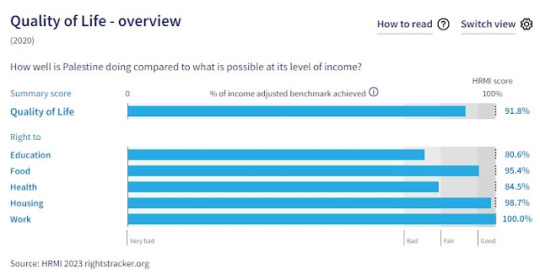
In fact, it is difficult to find studies that look at and evaluate Palestinian healthcare on its own merits, or that compares it with the rest of the Arab Middle East - something that is basic in studying the healthcare of every nation on the planet. One rare example that does is this obscure paper, "Experiences of Palestinian patients with hospital services: a mixed-methods study" which employs a standardized survey used throughout the world to evaluate patient experiences in Palestinian hospitals. They aren't great, they aren't terrible, and the study makes recommendations on how to improve them.
Palestinians themselves blame their governments, not Israel, for healthcare shortfalls. A recent survey says that one third of Palestinians say they do not have enough hospitals, 24% complained of scarcity of supplies, 20% said the lack of skilled medical professionals was the biggest problem, and 10% said it
was the high costs of care or the lack of medical insurance.
18 notes
·
View notes
Last Seen Blogs

apprentice-s
it's golden hour somewhere

yyspodujh62276
해외선물대여계좌

hiwarnheli
Hiwar Nheli

c0rgibuttsdrivemenuts
I Like Corg Butts and I Cannot Lie!

shoppingguidelk-blog
Shopping Guide