#antidepression regimen
Text

thank you to @punkpresentmic for having an aizawa + cats tag all neat and curated that comfort my achy brain
#aizawa shouta#my hero academia#bnha#my art#fanart#antidepression regimen#is what I am calling the scheduling of creative bullshit each day
69 notes
·
View notes
Text
So I'm in the process of weaning off one of my antidepressants. Partly because I don't think it's as necessary anymore because of a change in my living situation, partly because this one has unpleasant withdrawal symptoms that kick in fast and I don't like that.
The thing is? Following my doctor's regimen means that I still get those withdrawal symptoms on the days I don't take it, but it's more manageable.
And that's probably got a lot to do with the whole experienced medical professional thing. But also, I think there might be another aspect of it.
When I miss a dose because I didn't get a refill, there's a lot of dread and anxiety involved. What if my insurance arbitrarily decides not to cover my refill? What if they do decide to cover it, but only after waffling about it for three weeks? What if they decide that yeah, they'll cover it, but only if I have l see my doctor first so I'll have to call out of work on short notice to get to that appointment? What if the zaps are so bad that I just can't get up to the pharmacy at all for even longer?
(Every single one of these has happened to me, by the way. Most of them within the past year. In the USA, these are not irrational fears.)
When I skip a dose at my doctor's instructions, that fear isn't involved. The zaps are there, but they're bearable because I know they're temporary, and because they're not underscored by those very real fears.
Similarly, I've got a second job right now that I kind of hate. But it's bearable, because I know I can survive without it (albeit with more financial anxiety, but I'd still be okay). And if I make it to a certain date, I get a sign-on bonus. I can hold out that long and walk out the door the next day. That's something I can handle, the way I wasn't able to handle it when my last job turned toxic-- because that other job had been my only source of income and insurance, and I had no way of knowing if or when I would ever find something stable enough to leave.
What I'm saying is that humans can bear a lot, but I don't think we're meant to bear it forever. We need an escape route. We need a safety net.
(And one of the often unspoken cruelties of poverty is the total absence of those essential safety nets and escape routes. It creates an another layer of intense stress on top of everything else.)
15 notes
·
View notes
Note
PLEASE hit me with bipolar kirby . please. i wanna hear everything
BP2 with rapid cycling that took forever to get properly diagnosed because medical misogyny
It didn't help that her first hypomanic episode was triggered while she was going through drug withdrawal (ironically her disease made her more susceptible to addiction in the first place)
The second time it happened, she couldn't blame it on any external factors. She just assumed she was getting out of her period of acute grief/trauma and this was what being normal was like -- it had been so long since she felt that way
Diagnosed with unipolar depression first because that's what was getting in the way of her functioning. The SSRIs trigger another manic episode, which reaffirms that "oh yeah, this is just what feeling normal is"
One day she was telling her therapist about how she was going through these cycles of feeling great for a little while followed by long periods of bad depression, but they didn't seem to correlate with anything in her life? What's that about?
Was absolutely terrible with taking her mood stabilizers at first. She liked being manic. It made her feel productive for once. She knew, realistically, that the better the highs, the worse the lows, but the lows couldn't be that bad, right?
Oh. Yes they could.
Kept getting into the habit of taking on too much when she was manic and having her world collapse when she was depressed. The pressure of this is what got her back on a regular medication regimen
Was terrified of the diagnosis gutting her chances at becoming an agent. This is the part during the polygraph exam where she started crying. "Is it treated?" the person administering the test asked, and she nodded. "Okay, we'll make a note of that." Turns out it wasn't half as big a deal as she expected.
Still has trouble noticing when she switches from one mode to another. A few days in, she'll stop and go, "Oh. I slept 3 hours and feel fine. Seems bad." Or "Oh, I want to sleep 14 hours. Seems bad."
Getting Nina was the main thing that kept her life from totally imploding, because no matter how bad she got, she had to get up and take care of the cat
Cannot sit still when manic. Paces around the room instead
Fidget fidget fidget. "Oh wait what was that I didn't hear it". This is the one thing that never changes regardless of what part of a cycle she's in
"Whoa, you're talking really fast, can you slow down?" "That would be torture actually"
Keeps paper plates around because washing dishes is the first thing to go when the depression gets bad
Mainly takes lithium but her brain doesn't react well to SSRIs, so she supplements it with Seroquel instead of a typical antidepressant. Looks like she and Sam have something in common
15 notes
·
View notes
Note
Hey, Doc. What advice would you give to incel, blackpilled, etc. men trying to improve their mental health and worldview?
That's a tough one. If I understand it correctly, the 'black pill' ideology basically entails a fatalism wherein the individual believes their lives are bad because they are not conventionally attractive, their lives will always be bad, and nothing can ever change this.
at its core, this type of fatalism is not all that dissimilar to that seen in many cases of depression as well as a host of other psychological difficulties. There is a negative core belief that colors and skews the way the individual seems interprets and interacts with the world around them. And the only way to circumnavigate the matter is to constantly question, test and analyze the negative assumptions until one’s perspective becomes more objective and less skewed by self-prejudice.
Easier said than done, of course. But this is the basic principle of cognitive behavioral therapy wherein there are scores of different exercises meant to help the individual to regularly question and reanalyze their negative assumptions and look at life experiences through a clearer, more rational and less prejudiced lens.
In my experience, people who might fit into the concept of an incel are generally quite obsessed with issues of status and seeing the self and others as existing on a continuum based on value. Here those who are attractive, talented, famous, wealthy or in some fashion charismatic have high vale; whereas those who are unattractive, who are shy, uncertain or socially awkward are viewed as of low value.
That whole dichotomy needs to be thrown out the window.
The idea that one’s personal value is based on physical appearance and how successful they are at dating is exactly the kind of negative and irrational assumption that requires constant questioning and reanalysis.
A successful regimen of cognitive behavioral therapy (which can often be expedited through concurrent use of antidepressant medication) will likely lead to a stark decrease in self-hatred.
I don’t believe there has ever been a chauvinist whose sexism is not based in self-hatred and insecurity. Indeed improving one’s self-esteem and reducing self-hatred almost always entails a decrease in hatred toward others; reductions in bigotry, sexism, racism, heterosexism, the whole ball of yarn.
Successfully treating self-loathing is not an easy ordeal. It takes a lot of work and the individual needs to want to change. But it is very much possible.
4 notes
·
View notes
Text
How to become proactive in the medication profession? - Yisa Bray
Inquire with your pharmacist about any potential drug-food interactions in your current regimen. For instance, studies indicate that the vitamin K found in green leafy vegetables may reduce the efficacy of blood thinners such as Warfarin and Coumadin. Alcohol can intensify the effects of diabetes medications like insulin. Additionally, grapefruit can result in abnormally high levels of a medicines used to treat high blood pressure -Yisa Bray

Your medicines can be filled at one drugstore. Your medication records are kept in one location if you only use one pharmacy. Your pharmacist can assist you in keeping track of all of your medications, assess any risks, including possible harmful medicine interactions, and, if necessary, communicate with your doctor. You're also more likely to get refills on time and take your medication as prescribed if you only visit one pharmacy.
Use a chart for visual cues. This strategy aids in the formation of a successful habit and enhances your memory of everyday steps. In this situation, increasing your medicine adherence also improves safety. Use pieces of paper with images on them that are vividly coloured. Place them in a line on the refrigerator or the bathroom mirror to indicate which pills to take in the morning, which in the evening, and which to take with food or while brushing your teeth.
With your doctor or pharmacist, go over your medications. This will enable your doctor or pharmacist to determine whether you are taking any medicines or medicines combinations that increase your risk of falling. These medications include antidepressants, sedatives, and high blood pressure medications. - Yisa Bray
Put several prescriptions on the same refill cycle. To align the schedules for all of your medicine refills, ask your pharmacist for assistance. Some pharmacies coordinate your refill dates so you can pick them up at the same time with the help of your insurance provider and doctor. You'll go to the pharmacy less frequently and adhere better to your medicine routine.
As a reminder, use a pill dispenser. If you take medicines more than once a day, use a pill dispenser with slots for morning, noon, and night in addition to each day of the week. You can easily check if you have taken your medication using this.
12 notes
·
View notes
Text
Psychopharmacology Basics
Another day, another class with pharmacology. This is just a little review on drug principles. Most of these notes came from Videbeck's Psychiatric-Mental Health Nursing textbook and the lecture powerpoint deck. Some information is excluded if it was not covered by the professor, so this is not a complete source of information for nursing psychopharmacology.
This section will cover pharmacology basics, treatment principles and neurotransmitters.
Pharmacology Basics
Efficacy: the maximum therapeutic effect that a drug can achieve. Aka, the drug's ability to work within the human body.
Potency: the amount needed to achieve efficacy. Aka, the drug's concentration that allows it to work.
Half-life: the time it takes for a drug to be reduced by half within the body. The shorter the half-life, the more of the drug is required to maintain a therapeutic level within the body. The longer the half-life, the less is required to maintain the same level because it stays in the body longer.
Off-label use: uses for a drug other than what it was approved to treat
Black box warning: if a drug has a life-threatening side effect then there must be a warning in a literal black box on the label so it stands out
Pharmacologic Treatment Principles
Selecting the Drug. The chosen medication is selected based on how well it treats or reduces the patient's symptoms
Starting the Drug. Most psychotropic drugs take several weeks to be effective, so adequate doses must be given over a sufficient amount of time before the effects are realized
Amount of the Drug. The lowest effective dosage is used and titrated up or down as needed
Taking the Drug. The medication regimen should be as simple as possible to promote compliance
Differences for Older Adults. Older adults require lower dosages because it takes longer for their bodies to metabolize drugs
Stopping the Drug. Gradually taper off a drug rather than abruptly stopping it or the patient may suffer from temporary rebound, recurrence or withdrawal effects
Adjusting the Drug. Continuous follow up is necessary to ensure the patient is receiving the adequate dosage required
Neurotransmitters
There are four neurotransmitters that are of particular interest to mental health.
Dopamine
MOA: Excitatory
Effects: controls complex movements, motivation, cognition and regulates emotional responses
Increases schizophrenia, mania
Decreases Parkinson's Disease
Antipsychotics block dopamine receptors and reduce dopamine activity
Derived from the amino acid tyrosine
Norepinephrine (NE)
MOA: Excitatory
Effects: changes in attention, learning, memory, sleep, wakefulness and mood regulation
Increases mania, anxiety, schizophrenia
Decreases depression
Antidepressants block NE reuptake or inhibit MAO from metabolizing it
Serotonin
MOA: Inhibitory
Effects: controls food intake, sleep, wakefulness, temp regulation, pain control, sexual behavior and emotions regulation
Decreases depression
Antidepressants block serotonin reuptake so there is additional volume available in the synapse
Derived from the amino acid tryptophan
γ-aminobutyric acid (GABA)
MOA: Inhibitory
Effects: moderates the other neurotransmitters through inhibitory action rather than promoting direct stimulation
Increases apathy (lack of anxiety)
Decreases anxiety disorders, schizophrenia, mania
Benzodiazepines increase GABA to help treat anxiety and induce sleep
#nursing school#pharmacology#mental health pharmacology#pharmacology basics#neurotransmitters#nclexrn prep
16 notes
·
View notes
Text
Psychopathology, Ch. 9 notes
{Note: I have no personal experience with disordered eating and I don’t know how accurate this chapter of the textbook is. If you struggle with an eating disorder or previously have, and you notice incorrect information in this post, please feel welcome to drop corrections in the comments.}
Eating disorders: psychological disorders characterized by disturbed patterns of eating and maladaptive ways of controlling body weight.
Describe the key features of anorexia nervosa.
Anorexia nervosa: an eating disorder characterized by maintenance of an abnormally low body weight, a distorted body image, and intense fears of gaining weight.
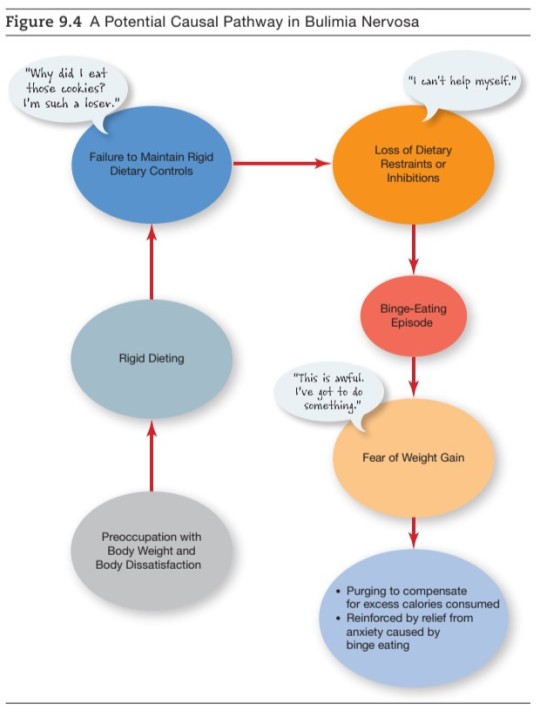
Describe the key features of bulimia nervosa.
Bulimia nervosa: an eating disorder characterized by recurrent binge eating followed by self-induced purging, accompanied by overconcern with body weight and shape.
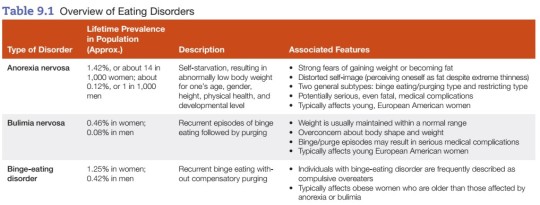
Describe causal factors involved in anorexia & bulimia.
- Eating disorders typically begin in adolescence and affect more females than males.
- Anorexia and bulimia are linked to preoccupations with weight control and maladaptive methods of trying to keep weight low.
- Many other factors are implicated in their development, including social pressures on young women to adhere to unrealistic standards of thinness, issues of control, underlying psychological problems, and conflict within the family, especially over issues of autonomy.
Body mass index (BMI): a standard measure that takes both body weight and height into account.

Evaluate methods used to treat anorexia & bulimia.
Severe cases of anorexia are often treated in an inpatient setting in which a re-feeding regimen can be closely monitored. Behavior modification and other psychological interventions, including psychotherapy and family therapy, may also be helpful. Most cases of bulimia are treated on an outpatient basis, with evidence supporting the therapeutic benefits of cognitive behavioral therapy (CBT), interpersonal psychotherapy, and antidepressant medication.
Describe the key feature of binge-eating disorder and identify effective treatments for the disorder.
Binge-eating disorder (BED): an eating disorder characterized by recurrent eating binges without subsequent purging.
- People with BED tend to be older than those with anorexia or bulimia and are more likely to be obese.
- CBT and antidepressant medication have been shown to be effective in treating BED.

Sleep-wake disorders: persistent or recurrent sleep-related problems that cause distress or impaired functioning.
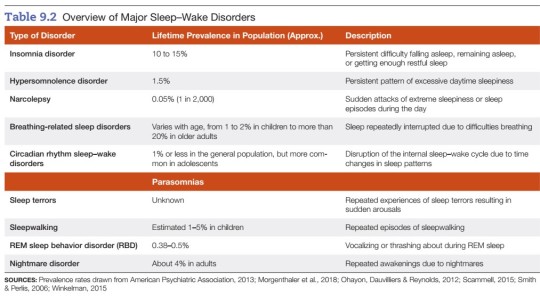
Describe the key features of insomnia disorder.
Insomnia: difficulties falling asleep, remaining asleep, or achieving restorative sleep.
- frequently associated with worrying and anxiety, especially performance anxiety associated with overconcern about not getting enough sleep
Insomnia disorder: a sleep-wake disorder characterized by chronic or persistent insomnia not caused by another psychological or physical disorder or by the effects of drugs or medications.
Describe the key features of hypersomnolence disorder.
Hypersomnolence disorder: persistent pattern of excessive sleepiness during the day.
- Despite adequate amounts of sleep, these patients feel unrefreshed upon awakening and aren’t alert during the day.
Describe the key features of narcolepsy.
Narcolepsy: a sleep disorder characterized by sudden, irresistible episodes of sleep.
- may involve genetic factors and loss of brain cells in the hypothalamus that produce a wakefulness-regulating chemical
Cataplexy: a physical condition triggered by a strong emotional reaction that involves loss of muscle tone and voluntary muscle control, which may result in a person slumping or collapsing to the floor.
Sleep paralysis: a temporary state of muscle paralysis upon awakening.
Hypnagogic hallucinations: hallucinations occurring at the threshold between wakefulness and sleep onset or shortly upon awakening.
Describe the key features of breathing-related sleep disorders.
Breathing-related sleep disorders: sleep disorders involving recurrent episodes of momentary cessation of breathing during sleep; often associated with daytime sleepiness.
Obstructive sleep apnea hypopnea syndrome: a subtype of breathing-related sleep disorders more commonly called obstructive sleep apnea. It typically involves repeated episodes during sleep of snorting or gasping for breath, pauses of breath, or abnormally shallow breathing.
Describe the key features of circadian rhythm sleep-wake disorders.
Circadian rhythm sleep-wake disorders: sleep-wake disorders characterized by a mismatch between the body’s normal sleep-wake cycle and the demands of the environment.
- more likely to occur as a result of frequent shifts in work schedule or frequent travel between time zones
Identify the major types of parasomnias and describe their key features.
Parasomnias: sleep-wake disorders involving abnormal behavior patterns associated with partial or incomplete arousals.
Sleep terrors: a sleep-wake disorder characterized by recurrent episodes of terror-induced arousals during sleep.
Sleepwalking: a sleep-wake disorder involving repeated episodes of sleepwalking.
REM sleep behavior disorder (RBD): a sleep-wake disorder characterized by vocalizing parts of a dream or thrashing about during a dream.
Nightmare disorder: a sleep-wake disorder characterized by recurrent awakenings due to frightening nightmares.
Evaluate methods used to treat sleep-wake disorders and apply your knowledge to identify more adaptive sleep habits.
A. Biological approaches
- anti-anxiety drugs are most commonly used; however, this is not always a good long term solution because of the potential for psychological and/or physical dependence on sleep aids.
B. Psychological approaches
- cognitive behavioral interventions have emerged as treatment of choice for patients with chronic insomnia
C. Healthy sleep habits
1. Establish a regular sleep-wake cycle.
2. Limit activities in bed to sleeping (as much as possible).
3. Get out of bed after 10-20 minutes if you are unable to fall asleep; take action to restore a restful state of mind.
4. Avoid daytime naps and avoid ruminating in bed.
5. Establish a regular daytime exercise schedule.
6. Avoid use of caffeinated beverages in the late afternoon & evening.
7. Replace self-defeating thoughts with helpful alternatives.
#eating disorders#disordered eating#psychology#psychopathology#abnormal psychology#my notes#study blog#sleep disorders
3 notes
·
View notes
Text
Trigger warning: discussion of a teen’s suicide. This is one of the differences between the Trans cult and gender critical feminism, feminists want kids to get access to the right mental health services before starting medical procedures which would also catch cases depression while the trans cult just uses every suicide to convince themselves and others that they should just bypass that into medical transitioning
Disturbing commentary made at the American Academy of Pediatrics Conference has emerged after a Professor of Pediatrics appeared to “glorify” a minor’s tragic suicide while discussing “gender affirming care.”
The American Academy of Pediatrics (AAP) held its annual conference in Anaheim this week, featuring four days of panels intended to be focused on the state of child-focused healthcare in the United States. But what should have been a gathering of professionals intent on improving the state of pediatrics has prompted outrage after one Doctor was seen giving a speech which appeared to lionize a teenager’s death.

On October 11, Dr. Julia Mason uploaded a phone camera recording to Twitter of Dr. Morissa Ladinsky giving a panel talk at the conference. Ladinsky’s presentation, titled “Standing Up for Gender-Affirming Care,” was focused on discussing “current public policy landscape on gender-affirming care as well as the impact on children and families.”
But Ladinsky’s presentation drew particular concern from Mason, who is a US-based pediatrician and a clinical advisor at the Society for Evidence Based Gender Medicine.
On Twitter, Mason, who was in attendance at the conference, took footage of Ladinsky discussing the 2014 suicide of Ohio teen Leelah Alcorn. Alcorn, who was born male but identified as transgender, ended his life by stepping in front of an oncoming semitrailer on a highway near his home. The suicide came after a prolonged depression and drastically increased Prozac regimen, both of which were related to his self-perception.
The FDA states that antidepressants, including Prozac, may increase the risk of suicide in children and adolescents. In a Reddit post made before his death, Alcorn wrote he was taking 60mg per day — which is far higher than the standard recommended pediatric dose.
Mason recorded Ladinsky seeming to lionize Alcorn’s suicide, repeatedly calling it “bold.”

Referring to Alcorn using feminine pronouns, Ladinsky can be heard saying: “And in the final days of 2014… a local 16-year-old lady, Leelah Alcorn, of trans experience, stepped boldly in front of a tractor-trailer, ending her life. Her suicide note, written to post on social media about an hour after her death, went viral around the world. Now, Leelah was not my patient. But I took care of hundreds of her classmates at Kings Mills High School. But each day, on the way to work, I passed that spot — where this teen boldly ended her life…”
Taken in the context of the subject of Ladinsky’s panel, Alcorn’s death appears to have been used to push the narrative that teenagers will commit suicide unless sufficiently “affirmed” by practitioners and parents.
Ladinsky’s comments prompted outrage from Twitter users who watched Mason’s footage, many of whom pointed out the dangerous nature of glorifying suicide in minors.
Medical experts uniformly agree that suicide contagion is a risk amongst adolescents, and the U.S. Department of Health and Homeland Services has set forward guidelines to limit the risk of suicide contagion. Among those recommendations include that “reports should not glorify the victim and should not imply that suicide was effective in achieving a personal goal,” such as gaining attention.
“This is so grossly exploitative,” Physician Mike Ziffra wrote in response to Mason’s post, to which Mason replied that the positive reaction from the audience towards Ladinsky’s comments left her “feeling crazy.”
Other users who watched the video noted that Ladinsky’s tone, which some described as “gleeful,” disturbed them, and that her use of the teenager’s tragic death to push a political mandate was disturbing.

The comments at the conference were not the first time Ladinsky has used the threat of suicides in teenagers to promote “gender affirming care” for minors.
In May, Ladinsky wrote an op-ed in Alabama’s largest news outlet in protest of a state law that would make it illegal to facilitate the medical transitioning of minors.
“I am a pediatrician. But Alabama may soon take my white coat and stethoscope, charging me with a felony for doing my job,” Ladinsky wrote.
In the article, she details a young patient in her care who attempted suicide three times, and continues that only “affirming” care will prevent the potential deaths of gender-distressed children.
“… internalized guilt, confusion, shame and sense of defeat lead almost half of transgender youth to embark on suicide during their journeys. Our clinic patients have made large right turns away from that darkness, serving as daily reminders of the healing power released by affirmation and hope.”
Earlier this year, Ladinsky was featured on a podcast during which she claimed that children as young as four years old can understand the concept of their “gender identity.”
“Between four, five, even six years old, a sense of gender identity fills in. Remember the dress-up box? Did you put on the princess outfit? If you were assigned male at birth, what did your teacher say? Or how did they look? Those are the beginnings of aligning someone’s internal sense of gender with what is available to them to express it.”
The podcast Ladinsky spoke on was through Pride365 Plus — an LGBT resource site which appears to exist solely to promote products distributed by pharmacy benefit manager and health care provider Optum.
#American Academy of Pediatrics Conference#Dr Morissa Ladinsky#Doctors glorifying teen suicide#Prozac and teen use#Suicide contagion
7 notes
·
View notes
Text
Quick Quiz: Could PAXLOVID Be Right for You?
Are you looking for a new treatment option to manage your anxiety or depression? Then you might want to consider paxlovid online. But is this medication right for you? Take our quick quiz to find out if PAXLOVID could be the answer to your mental health needs. In this blog post, we'll discuss what PAXLOVID is, its potential benefits, and how it could help you. Read on to find out if PAXLOVID could be the right choice for you.
What is PAXLOVID?
buy paxzen online is a new type of prescription medication that has been recently approved by the FDA for the treatment of severe depression. The drug works by blocking the reuptake of serotonin, a neurotransmitter in the brain responsible for regulating mood. By blocking the reuptake of serotonin, PAXLOVID helps to restore an individual's serotonin levels, and improve their overall mood. Additionally, research suggests that PAXLOVID may be helpful for those who suffer from anxiety as well. It is important to note that PAXLOVID should only be used under the supervision of a healthcare provider.
How does PAXLOVID work?
paxlovid from india works by blocking the action of certain chemicals in the brain that are linked to feelings of anxiety, depression, and other mood disorders. It is believed to reduce symptoms of anxiety and depression by interfering with the chemical reactions in the brain that cause them.
PAXLOVID affects a neurotransmitter called serotonin, which is responsible for regulating mood and behavior. By blocking certain receptors in the brain, PAXLOVID increases the amount of serotonin available in the brain. This in turn helps to balance moods and emotions, leading to fewer episodes of anxiety and depression.
Additionally, PAXLOVID may also have a positive effect on sleep quality and reduce symptoms of insomnia. It works by inhibiting the reuptake of serotonin, which increases its availability in the brain, resulting in better sleep quality.
PAXLOVID is typically taken as an oral tablet or capsule once daily or as directed by your healthcare provider. It is important to take PAXLOVID exactly as prescribed and not to increase or decrease your dose without first consulting your doctor.
Who is a good candidate for PAXLOVID?
PAXLOVID is an FDA-approved medication that is used to treat adults and adolescents ages 12 and older with Attention Deficit Hyperactivity Disorder (ADHD). The medication is a stimulant that works to improve concentration, focus, and attention.
The most important factor in determining if you are a good candidate for PAXLOVID is whether or not your symptoms are severe enough to warrant the use of medication. If lifestyle changes, such as increased exercise, improved sleep, and time management techniques have not been successful in managing your symptoms, then PAXLOVID may be an appropriate treatment option for you.
Your doctor may also consider whether you are able to understand the risks and benefits of the medication before prescribing it. People with underlying heart conditions, mental health issues, or a family history of addiction may not be good candidates for this type of medication.
In addition, people who are taking certain types of medications, such as blood thinners, seizure medications, or antidepressant drugs, should speak with their doctor before starting PAXLOVID. Your doctor may be able to adjust your current medication regimen to reduce potential interactions.
PAXLOVID can be an effective treatment option for many people with ADHD who have not seen improvement from lifestyle modifications alone. If you think that you might be a good candidate for this medication, talk to your doctor about the potential benefits and risks.
What are the side effects of PAXLOVID?
The most common side effects of PAXLOVID are mild, such as nausea, dizziness, drowsiness, and headache. In some cases, more serious side effects may occur, such as: severe allergic reactions (rash, hives, difficulty breathing, swelling of the face, lips, tongue, or throat), agitation, confusion, hallucinations, or aggression. Other potential side effects include changes in heart rhythm, fainting, seizures, and suicidal thoughts or actions.
If you experience any of these side effects while taking PAXLOVID, contact your healthcare provider immediately. Do not stop taking your medication unless advised to do so by your healthcare provider. Be sure to tell your healthcare provider about all medications you take and any other medical conditions you have, as these may affect how PAXLOVID is metabolized and the side effects you experience.
Is PAXLOVID right for me?
If you’re considering whether or not PAXLOVID is the right treatment for you, it’s important to first understand how it works and what kind of patient it is intended to help. PAXLOVID is a medication that works by inhibiting certain enzymes in the body that are involved in tumor growth. This means that it can be used as a treatment for some types of cancer, such as non-small cell lung cancer and metastatic melanoma. It may also be useful in treating some other medical conditions, such as multiple sclerosis, Crohn’s disease, and ulcerative colitis.
The best way to find out if you are a good candidate for PAXLOVID is to discuss it with your doctor. Your doctor will evaluate your condition and determine if the drug is right for you. Your doctor will also be able to tell you about any potential side effects that may occur with the use of the drug. It is important to note that all medications come with potential risks and side effects, so it is important to weigh the benefits against the potential risks before making a decision.
To help you decide if PAXLOVID is right for you, take this quick quiz:
1. Are you 18 years of age or older?
2. Do you suffer from non-small cell lung cancer, metastatic melanoma, multiple sclerosis, Crohn’s disease, or ulcerative colitis?
3. Are you willing to discuss any potential side effects with your doctor before starting the medication?
4. Are you willing to comply with all instructions given by your doctor regarding the use of PAXLOVID?
If you answered “yes” to all of these questions, then you may be a good candidate for PAXLOVID. However, it is important to keep in mind that this medication may not be right for everyone. Be sure to discuss it with your doctor and make an informed decision based on your individual health situation.
you can buy from : buy paxzen online
https://buypaxlovid.net/
2 notes
·
View notes
Text
i think its the love/hate relationship i have with therapy that makes online discussions about it difficult to digest, or at least in the sense of uhh the therapy speak topic. never feels like theres enough discussion about the limitations of therapy especially as it concerns people who are, in some way, alienated by society either through marginalization, class struggle, disability, etc.
trying to cope with an environment where you're repeatedly in stress just turns into a constant up-and-down compiled with shame for me anyway, like, 'im doing what im supposed to be doing so why is it not working'
not even to mention how common it is for these people, especially, to have therapy weaponized against them. i was lucky enough to have a therapist affirmative enough to gladly help me access hormones, but that was after a very troubling instance when i was 16 where my therapist outed myself to my mom and i just refused to see her anymore afterwards. trying to find 'the right one' is a crapshoot, and the bad experiences just compound the self-doubt and cynicism towards the institution of psychology as a whole
the distance that a therapist creates between a client, which is the healthiest way of going about it for both parties as a power-imbalanced, personal relationship is very Not Good (and god knows it can lead to vulnerable people being easily taken advantage of), can leave some with a misunderstanding or numbness towards the aspects of a real, fulfilling relationship with an equal party. this is where the tools we're taught for introspection can lead us to further alienation even from our peers.
even now as i'm trying to find another one thanks to how shit school is on my idiot brain, i already have to theorized about 'how im going to handle it'. having a difficult time forming attachments to people is a benefit in this situation (with therapy being both distant and temporary), but a detriment in every other aspect of my life, and knowing that makes it hard to believe that there will be a fulfilling way for me to change that part of me. perhaps thats why im more warmed up to the idea of psychoactive therapies outside of the typical 'heres an antidepressant' regimen?
I think knowing my roommates ex-partner for a while when they were still somewhat together, who is a therapist, has made me do a lot of thinking on it too. I don't think I have a place to confront it (difficulty with attachment == too much distance for me to have much to say), but I could tell when she utilized her therapeutic trainings as a way to hurt my roommate. and now that she (who is in her mid to upper 30s I'm pretty sure) is engaged to someone who was also in our friends circle (who is my age, and suffered from a lot of bad shit) makes me feel a lot more concerned about it. she resisted introspection on her willing and knowingly participating in adultery with a married man, and does not at all have any introspection on her alcohol consumption, and its like. yeah. these people are fallible, and that inevitably carries over into their work with some of the most vulnerable people.
social support systems have always been much more helpful for me, but again. attachment problem. i'm just constantly on the outside looking in when it comes to group situations. so idk, life sux smoke weed or whatever
tangential article(s) semi-related: https://internetprincess.substack.com/p/no-good-alone
https://persinette.substack.com/p/less-tiktok-more-screaming
1 note
·
View note
Text

meant to draw izuku picking up his classmates. however. sometimes that cookie crumble.
14 notes
·
View notes
Text
Links Between Stress Shift Work And Serotonin Levels

The 21st Century is best characterized by the advent of ultra-modern technology, global commercial and business, and the unstoppable desire to get and stay ahead. Because of these factors, business corporations compete in a world where the economy is active 24 hours a day, seven days a week. This phenomenon created a demand for employees that would work even during the night upto the wee hours of the morning. This work schedule reversed employee lifestyle, making the day their time to for sleeping. Shifts may disrupt the normal body functions, hamper sleep cycles, and reduce the body’s serotonin levels. Serotonin is a neurotransmitter that is found in the central nervous system and impacts multiple functions like mood, sleep, sexuality, and appetite. This neurotransmitter may also promote cell regeneration.
Studies show that non-day shift workers tend to have lower levels of “feel-good” hormones called serotonin. Researchers at the University of Buenos Aires led by Dr. Carlos J, Pirola studied 683 men and compared 437 day workers to 246 shift workers. The results, the shift workers’ serotonin levels, measured through blood tests were significantly lower than those on regular day schedules. In addition to reduced serotonin levels, shift workers were also found to have higher cholesterol, hip-to-waist ratios, increased blood pressure, and higher triglyceride levels.
Because serotonin levels administer sleep patterns and other body functions, the University of Buenos Aires study suggested that shift work may also lead to a so-called Shift Work Sleep Disorder. People with this disorder tend to remain awake when they should be sleeping. These individuals can be very tired during waking hours. This disorder takes place because of a work schedule that takes place during the normal sleep period. Because of this, people who have difficulty getting sleep because their bodies are still programmed to be awake. The time of being asleep and being awake is different from what the body’s internal clock expects.
Other studies also found out that non-standard and night shift work may affect the cardiovascular and metabolic systems. These studies suggest that there is a possibility that shift work is directly responsible for high blood pressure and increased body fat, according the researchers of the Buenos Aires study. In addition to the disruption of sleep patterns, reduced levels of serotonin are also linked to other conditions like stress, anxiety, and depression.
Lifestyle changes can lead to improved serotonin levels. To make serotonin levels consistent, sleep patterns should be consistent and food regimens should include necessary vitamins and minerals to control the serotonin levels. Certain drugs and substances like caffeine, nicotine, alcohol, and antidepressants should be avoided because they may deplete serotonin production.
Individuals who want to improve their serotonin levels can use medication to aid them in their goal. The amino acid 5-HTP can be taken as a supplement and improve the body’s ability to manufacture serotonin. Another amino acid called L-tryptophan is used by the body to produce serotonin. However, before taking these supplements, patients are advised to seek the approval of doctors and other health professionals. Individuals who choose to work in the night should maintain adequate rest to lessen ill-effects that may develop. Healthy lifestyles and nutritious food regimens may improve serotonin levels and improve one’s quality of life.
if you free tips Get The Ultimate Keto Meal Plan⚡️ Make
#Links Between Stress Shift Work And Serotonin Levels#health#fitness#wellness#happy#support#success#gym#lifestyle#workout
5 notes
·
View notes
Note
BRAIN ZAPS ARENT NORMAL?!?;?
Nope!! Usually, they're only when you're withdrawing from an antidepressant, changing the dosage, or inconsistently taking your medication. It's not really supposed to happen if nothing is changing in your medicine regimen and something worth talking to your doctor about!
(Disclaimer I am not a medical professional, I just have a special interest in clinical psychology and this is what my doctor told me)
4 notes
·
View notes
Text
seroquel is a real drug
I started taking an antidepressant a few weeks ago and I feel fine in almost exactly the same way I felt a couple years ago, when I was taking fluvoxamine, plus some other symptoms that seemed to arise from a fluvoxamine/seroquel combination. When I told my doctor this, he said there was no reason to doubt it, because it's a pretty good model of how many people's symptoms improve from combining two different drugs -- fluvoxamine + another antidepressant like sertraline.
I'm not a doctor or anything and a lot of this will just sound like science fiction to you if you don't know anything about the underlying drugs. But it would have been really surprising to me if my doctor hadn't had access to this drug combination research; I'm pretty sure it'd have been impossible to find in my own area without asking someone I trust who has been prescribing it regularly for over 10 years (the last 5 or so as a primary treatment for depression), and that's a very unusual kind of doctor.
The most common and obvious way that combination meds have been studied is in people with some kind of substance abuse disorder, and this is a pretty natural place to look for them, because people who use two drugs tend to be much less tolerant than people using only one. That's one of the reasons that fluvoxamine is usually added to Prozac, for instance, and sometimes it's even a reason not to prescribe Prozac at all, even though Prozac is much more effective than fluvoxamine/sertraline. But it turns out it's just as easy to find them in nondrug-using people, too: fluvoxamine/sertraline are frequently prescribed for people who have trouble adhering to their medical regimens or are otherwise high-maintenance, and the results with this population are the same (and much better!) as the results with the substance abuse population.
There are a few different reasons why this is possible. One is that both fluvoxamine and sertraline themselves have addictive potentials, but it turns out that when you add them, you get a milder one. ("Milder" means less of a "potent drug" than either fluvoxamine or sertraline on their own, although it's still "potent enough" to require a therapeutic dose and is thus often unpleasant to take.) This is actually very well-known, and the fluvoxamine/sertraline combination has been prescribed to patients who refuse to take fluvoxamine ("I know I said I was going to take it but I just don't want it") and vice versa.
Another reason is that some people just have a low tolerance for many medicines and are able to stay on them only by combining them with another medicine that helps to balance out their own deficiencies. The way this works is not fully understood but involves interactions with the cytochrome system which is responsible for the metabolism of a wide variety of drugs, including some antidepressants. One of the drugs that seems to fit this role is the anticonvulsant carbamazepine. So some people take fluvoxamine only when necessary, but others may need both fluvoxamine and carbamazepine for most of the time, without the need to take them at the same time.
6 notes
·
View notes
Note
🐑, 🐔, 🐄, 🕯, 🍅, 🐝
These are for the cottagecore asks. Hope it makes you smile today.
Thank you so much for the ask! It made me smile indeed. c:
🐑 Sheep: What is a comfort item you own?
Oh gosh, I have so many... My favorite might be the black-velvet cloak with a satin purple lining. I deeply mourn that it's not Socially Acceptable to wear a cloak to an office job, because when it's cool enough outside, I would LOVE to! (When I worked at Chipotle, Pizza Hut, and PetSmart, I would wear my cloak to work! The people at Chipotle freaking LOVED it.)
Alas, I work in a building with government security and I work on a contract with a rather strict Dress Code. And also I don't trust the people downtown enough to walk around in a cloak...
🐔 Chicken: What is a comfort movie/show for you?
I'm hyperfixated and predictable. My comfort movie is Justice League vs. Teen Titans, and my comfort show is the 2003 Teen Titans series!
🐄 Cow: What is one other tumblr blog you really appreciate?
Oh gosh, just one? It's hard to choose just one... Any blog that belongs to my friends has HEAPS of appreciation! "Appreciate" in particular applies to my fellow RPers who patiently wait until I have the time, energy, and muse to Actually Write something-- even when it takes months! I'm so immensely grateful for their grace.
🕯️ Candle: What is something you can’t go to bed without?
Well, my antidepressant, for one thing... :P (It has Major Sleepiness side effects for the first couple hours after taking it, so it's best to take it before bedtime, and it's a Very Important part of my mental health regimen!)
But on a more fun note, I have this one specific blanket that my dad gave me when I was like... 13, 14 years old? (Gods, I'm realizing I've had this thing for half my life!) It's nothing special, a little brown thing from Walmart that only covers me shoulders-to-toes if I have it on a diagonal angle, with kind of a silky underside and a very thin top layer. But the fact that it's so thin and silky makes it easy for me to sleep under! I get overheated very easily, so a thin blanket that still has enough weight to be Comforting is great (and very hard to find!), and I'm Extremely Sensitive to Touch and Tactile Sensation, but it's a very nice smooth gentle Tactile Sensation, so it's really the ideal blanket for me.
It brings me so much comfort that I put a blanket inspired by it in my stories! (It's handmade by Srentha for Dove when she's Struggling^tm and needs lots of comfort, so she can wrap it around herself for comfort if he can't be there.)
🍅 Tomato: Have you ever gardened, and if so, what is your favorite thing to grow?
I have! I've always loved plants like small silent friends, helping my Nana in her garden as a kid, and when I moved in with my co-worker from the pet store she helped me garden things like cilantro and zebra flowers, and when I lived in the Metroparks I had SO many houseplants and potted herbs! Schefflera, snake plant, peace lily, lemon balm that my chinchillas absolutely demolished when I wasn't looking. (They ate the whole plant! It's safe for them, don't worry.) My very first houseplant was a Norfolk island pine. Unfortunately my houseplants and herbs got wiped out by aerial blight after I moved from the apartment, and it scared me away from plants for a little while because I blamed myself. I only Very Recently got enough forgiveness and courage to try again, and for now all I have is a small but rapidly-growing pothos.
My favorite thing to grow is DEFINITELY the lemon balm! It's in the mint family, so it's super hardy and a vigorous grower, it always has such a gentle and friendly energy, and it's good for absolutely Everything I use plants for, herbal healing and mysticism alike! It helps headaches, stomach upsets, it soothes mild pain, it helps soothe stress, it helps you fall asleep, and mystically it's great for protection, energizing, cleaning, and insight. Plus, it's one of the only Fresh Plants my chinchillas will actually eat. This is a big deal for Dusty, because he's EXTREMELY picky about fresh foods!
🐝 Bee: What is a video game that you find comforting?
Pokemon Pearl. ~<3 That was the game that initially inspired me to start writing Pokemon fanfics! I also have a lot of strong Happy Comfort Nostalgia for Pokemon Battle Revolution too, because I played it with all but one of my siblings!
3 notes
·
View notes
Text
Finding Hope Again: Treatment-Resistant Depression Breakthroughs
For those struggling with depression, the journey to finding relief can feel overwhelming. You may have tried different medications, therapy sessions, and lifestyle changes, yet the darkness persists. If traditional treatments haven’t brought lasting improvement, you’re not alone. This is where exciting advancements in treatment-resistant depression (TRD) offer a beacon of hope: transcranial magnetic stimulation (TMS) and esketamine (Spravato®) therapy. We at Ohio Psychiatric Services have an experienced team of qualified professionals to offer you these services at our Lancaster and Hilliard centers in Ohio.
Understanding Treatment-Resistant Depression?
TRD is diagnosed when depression symptoms persist despite trying at least two different medication regimens at appropriate doses for a sufficient length of time. It’s a frustrating experience, but the good news is, there are new options.
TMS: A Non-Invasive Approach
For those struggling with depression, the journey to finding relief can feel overwhelming. You may have tried different medications, therapy sessions, and lifestyle changes, yet the darkness persists. If traditional treatments haven’t brought lasting improvement, you’re not alone. This is where exciting advancements in treatment-resistant depression (TRD) offer a beacon of hope: transcranial magnetic stimulation (TMS) and esketamine (Spravato®) therapy. We at Ohio Psychiatric Services have an experienced team of qualified professionals to offer you these services at our Lancaster and Hilliard centers in Ohio.
Esketamine (Spravato®): A Rapid-Acting Relief
Spravato® is a nasal spray medication containing esketamine, which works differently than traditional antidepressants. It can offer relatively quick relief, often within hours or days, for patients with TRD. Spravato® is administered under medical supervision in a safe and controlled setting.
TMS: A Non-Invasive Approach
For those struggling with depression, the journey to finding relief can feel overwhelming. You may have tried different medications, therapy sessions, and lifestyle changes, yet the darkness persists. If traditional treatments haven’t brought lasting improvement, you’re not alone. This is where exciting advancements in treatment-resistant depression (TRD) offer a beacon of hope: transcranial magnetic stimulation (TMS) and esketamine (Spravato®) therapy. We at Ohio Psychiatric Services have an experienced team of qualified professionals to offer you these services at our Lancaster and Hilliard centers in Ohio.
Why Consider TMS or Esketamine (Spravato®)?
Effective for TRD: Both TMS and Spravato® are FDA-approved for treatment-resistant depression, offering hope where other options haven’t worked.
Relatively Fast-Acting: Unlike traditional antidepressants that can take weeks to show improvement, Spravato® can provide relief within days. TMS may take longer, but some patients experience improvement within the treatment course.
Non-Invasive and Safe: TMS is a non-invasive procedure with minimal side effects. Spravato® requires medical supervision but is generally well-tolerated.
A Personalized Path to Recovery
Don’t let treatment-resistant depression hold you back from living a fulfilling life. We at Ohio Psychiatric Services and TMS Center, understand the unique challenges of TRD and we can help. Our team of experienced professionals will work with you to develop a personalized treatment plan tailored to your specific needs. We offer both TMS and Spravato® therapy, and may combine these innovative treatments with supportive therapy to optimize your recovery journey.
Your Journey to Hope Begins Today
If you’re struggling with TRD, there is hope. Reach out to us today for a free consultation. We’ll discuss your situation and explore if TMS or Esketamine (Spravato®) therapy could be the key to unlocking a brighter future. You deserve to feel hope again, and we’re here to support you on your path to recovery.
Contact us today to learn more by calling (740) 201-6021 or visit us at https://ohiopsychiatricservices.com/ to book an appointment.
0 notes
Last Seen Blogs

slvrstarlight
secrect gardens in my mind

queer-artsy-lil-shit
I'm here I'm queer and I'm a depressed artist

hellofaboss
Helluva Boss

choandsfora-blog
Sem título

multiverse-sparkles
warm sunshine