#psychiatry critical
Text
So, Peer Respites are a not-very-well-known alternative to psychiatric hospitalization. They are 100% voluntary and staffed by peers, AKA individuals with lived experience of mental illness/emotional distress/what-have-you. Generally, they are a homelike environment where you can come and go as you please, and there is lots of voluntary programming like groups, art, yoga, etc. You can bring your own food or cook meals together with staff and other residents. Stays are usually anywhere from five days to two weeks, depending on the respite house and also your own wants and needs. There are no restraints, strip searches, or seclusion.
They're also on the rise!! I know this because I've spent all day today compiling data on peer respites in the US so I could create this fun graph for ya'll.

In the past ten years, at least 38 new peer respites have opened in the US. The data for 2023 is incomplete, but at least one has already opened, and another is scheduled for a soft opening later this year.
Some things about the data:
I did not include peer respites which were permanently closed (2) or could not find an opening date for (1)
I used the National Empowerment Center's Directory of Peer Respites, along with some internet sleuthing to find a few more (and to find the opening dates for each one). Because of this, I may have missed a few.
There were a handful of peer respites for which I could not pin down a for-certain, exact date for. I did include these in the dataset as I was able to find rough estimates.
I have also not done a deep dive for all peer respites that were unsuccessful, which may skew the data a little bit.
I included Soteria Vermont as well, as it technically fits the definition despite being specifically for people with psychosis
If you would like to help get a peer respite off the ground, I would recommend donating to Peer Support Space Inc.'s Orlando FL Peer Respite. Their soft launch is November 2023, and they are scheduled to open to the public in January 2024. This is really important, because Florida's only peer respite has recently permanently closed.
If you're interested in starting your own peer respite, the National Empowerment Center has a list of resources here.
If you are interested in seeking help from a peer respite, there is a directory of most of them here. You can also look at the Google Doc I created to compile my data, which has a few more/is slightly more updated - though it's not nearly as nicely put together as the other one!
If anyone would like to add any information, non-US peer respites, etc, feel free to!
#peer respites#peer respite#psych ward#psych hospital#psychiatric hospitalization#psych critical#psychiatry critical#anti psychiatry#antipsych#antipsychiatry#mental illness#neurodivergency#disability#hospital diversion#psychiatry#disability pride month#psychiatric survivors#putting in all the tags I can think of so ppl see this lol
2K notes
·
View notes
Text







Men have no. Business. In. The. Psychiatric. Therapy. Of. Girls. And. Women.
Not only because men are much more likely to be biased and more likely to mindlessly accept misogynistic theory in psychiatry, but also because especially young, vulnerable girls and women cannot differentiate an adult male in authority being understanding and offering a space to be vulnerable "without consequences" from a romantic or sexual interest. There were so many more comments of girls admitting they're in love with their male therapist. This is fucking scary.
#radblr#radfem do touch#radfem#radical feminism#radical feminist#radfems do interact#gender critical#radfems please interact#radfems do touch#psychiatry critical
2K notes
·
View notes
Text
Sometimes, when talking about the current psychiatric system, we get lost in anger and don’t look towards alternatives and what a better tomorrow might look like. Here’s some cool mental health/psychiatry reform things that I think are neat (Somewhat US centric bc that’s where I live). Lots of them focus on psychosis, because I think psychosis is a sorely ignored subject in mental health activism.
US Peer Respite Directory - A list of voluntary, community-based, non-clinical crisis support group-home like environments that are staffed by people with lived experience of mental illness and/or lived experiences in the psychiatric system.
Students With Psychosis - A nonprofit that empowers students with psychosis through virtual programming, support groups, etc. They’re run by the amazing Cecilia McGough, an advocate with schizophrenia.
Hearing Voices Network - A network of support groups for people who hear voices, see visions, and have other extreme experiences. Focused on supporting individuals without judgement and giving them a place to explore their experiences and grow from them.
Open Dialogue - An psychosocial approach to psychiatric services that focuses on treating clients with respect, shared decision-making, dialogue between client, providers, and family (if the client wants family involved), and more minimal use of medication.
CommonGround software - A software developed by Dr. Pat Deegan that allows clients to communicate their needs to their providers more efficiently to support shared-decision making. Dr. Deegan has a lived experience of being diagnosed with schizophrenia and believes in personal medicine and med empowerment.
Project LETS - A radical approach to peer support and healing that has a disability justice centered approach, giving people with lived experience a voice and focusing on mutual aid. They provide peer mental health advocates, self-harm prevention, and more.
Integrative Psychiatry - A holistic form of psychiatry that focuses on nutrition, exercise, therapy, and psychosocial factors, where medication is just an aspect of treatment. US database of integrative psychiatrists here.
Soteria Houses - Community homes with peer support that provide residents with personal power, responsibilities, and “being with” residents, that focus on a humane and person-centered approach.
Relating to Voices Using Compassion Focused Therapy - A self-help book by Drs. Eleanor Longden and Charlie Heriot Maitland about managing distressing voices and building a respectful, cooperative relationship with them. Views voices as potential allies in emotional problem-solving rather than enemies.
Clubhouse International - A non-profit organization that gives people with mental illness opportunities for friendship, employment, housing, educational, and medical services all in one place. It was founded by a group of friends who survived a psychiatric hospital together.
Psychosis Research Unit - A group of psychology researchers who are doing research on and developing psychotherapeutic techniques for coping with and managing psychosis, such as CBT for psychosis and Talking with Voices therapy.
#mental health#psychiatry critical#psychiatry reform#anti psychiatry#psych critical#psychosis#psych reform#mental illness#uhhhhhh idk what else to tag this with so people see it#social justice#neurodiversity#idk
1K notes
·
View notes
Text
a lot of people, when faced with antipsych rhetoric, will accuse us of trying to take their meds away.
the stock response is that no, we’re not trying to take anyone’s meds away, we’re trying to remove the gatekeeping and prescriptive framework that meds are currently accessed in to begin with, making it so that no-one is forced to take meds they don’t want to take and that anyone can access any meds they want to take without needing to go through an institutional authority.
and like, that’s true, but i think it’s missing the inherent anxiety being expressed: that less people will be on meds, if the psychiatric institution is abolished and we are able to disseminate accurate information about the long-term effects of some of the most commonly prescribed psych meds (SSRIs and antipsychotics in particular). i don’t think these people would ever articulate it this way themselves, but i think a lot of pathologized peoples who have bought into the psychiatric institution’s narrative have an idea of medicated=good, and unmedicated=bad, and therefore have an automatic anxiety response to the idea of a large number of people going off their meds, even if that doesn’t include them, personally.
there’s an anxiety deeply embedded in MI and neurodivergent spaces that buy into the pathology framework about unmedicated MI people being dangerous, or just unpredictable in a way that is framed as harmful to themselves and others. there’s also a strong attitude of like... not trusting individual MI people to ascertain accurately if their meds work for them or not. there’s a reason MI spaces love to lean heavily on the “i was doing great, so i decided i didn’t need my meds, and when i went off them i was suddenly suicidal and miserable, because my meds were the only thing making me do great” anecdote--while it’s an accurate anecdote for many people, it’s also incredibly useful for pushing the narrative that MI people cannot accurately assess our relationships with medication, and that it’s necessary to leave that assessment to a doctor or other outside professional.
the idea of less people being on medication of their own free will is genuinely incredibly anxiety-provoking to a lot of pathologized peoples. the idea that MI people might not need the meds they’re currently, right now, taking, is incredibly destabilizing to their worldview. the idea that they themselves might have the option to go off their meds is anxiety-provoking! from an internal view, it feels like they’re being threatened. no matter how many times you explain that nobody’s trying to personally take their meds away, they still have the feeling of being under threat. i think that’s where the disconnect in a lot of these discussions happens.
318 notes
·
View notes
Text
Content warning: Talk of pressuring systems to integrate and/or fuse.
Long anti-psych rant incoming
Screenshotting this because its a 5 year old post and we don't wanna bring discourse or anything to OP.
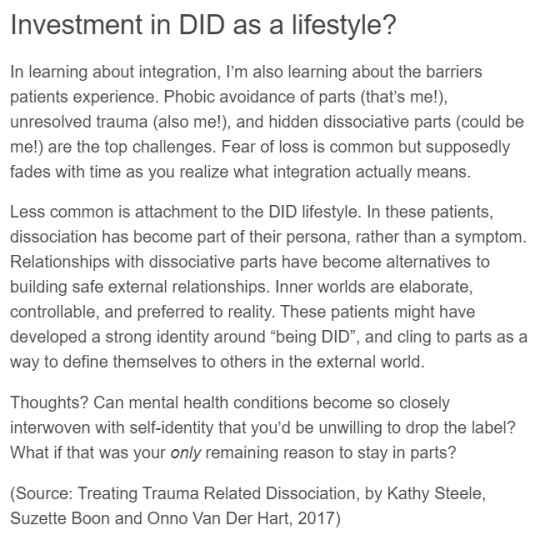
Ok so this quote is like a microcosm of the ways in which mainstream psychiatry refuses to allow patients any autonomy in our recovery.
Like, this hypothetical example of "DID as a lifestyle" is a perfect example of a system that would (likely) be benefitted from pursuing healthy multiplicity rather than full fusion. But instead of recognizing that, and working with the patient to find a way to function happily as a system, they label it as a "barrier to integration".
Its made clear in this example that being a system is deeply important to this patient. But the authors do not recognize the humanity of the individual system members. They seem to imply that in-system relationships function solely as an avoidant behavior, and its clear that they see them as inherently lesser than external relationships. They view the internal world, lives, and identities of system members as being obstacles to normalcy.
Because that's really what matters to them at the end of the day. The patient's desires are secondary, if they're even taken into account all. Any positive experience with their neurodivergency is viewed as an obstacle in the way of the predetermined goal. And its been decided for the patient long before they walk in the door. The goal is enforcing hegemonic ideals of normalcy, complacency, and obedience.
Because you know what? Even if this hypothetical patient's experiences are exclusively pathological, even if their in-system relationships are for the purpose of avoidance, even if they are "clinging" onto parts as a coping mechanism. So fucking what? Sure, call it "anti-recovery" if you want to, but we value that autonomy of individuals to decide how they want to live their lives, and that includes continuing to live with their disorder as they see fit.
Because its laid out clearly here. The patient's ability to decide for themselves what they want is seen as a problem to be solved. Their experience and self-expression is a pathology to be cured. And under no circumstances will we stand for that.
59 notes
·
View notes
Text
The topic of medication for psychosis can be a truly loaded one, and I understand how people on either side of the debate feel strongly on the question, to the point where it can be a difficult thing to have a conversation about. Especially online in a public space, where nuance and delivery often gets lost.
My quick and dirty take is that autonomy is extremely important, both from an ethical point of view, and a psychological one.
People should get to make their own damn choices about medication, and no one gets to shame us for it, whether we choose to take antipsychotics or not. Everyone's situation is individual, and there are no one size fits all "right" answers.
There is information and there is even misinformation. And I'm passionate about people having access to all the facts, so they are able to make an informed choice.
Too often I find that trained psychiatrists themselves don't have access to all the facts, and I don't really believe that "the doctor always knows best".
I think that forcing medication on people in willful ignorance of the patient's discomfort, is violence. And I think the harm of this violent act outweighs any benefits the medication could have otherwise carried.
A lot of us have complicated emotions around drugs. Maybe it was forced on us, maybe it ruined something, or maybe it saved something. Maybe it was helpful but at a point it became a heavy weight we didn't know how to put down. I struggled for 7 years, every single day (except when i lost the battle) to make myself swallow my meds. No one forced me. It still felt like an act of violence against myself. I also still believe that it was the right thing for myself at the time. For the past half a year i have not been on any antipsychotic. I have complicated emotions on it, but right now that is right for me. I am prioritizing other parts of my life experience over parts of my mental stability. Personally, I only get to do this because at 31 years of age, my life is now so stable, and my support network so strong, that I get to make that choice for myself and still be the happiest I can be.
In any case, I want to make it clear that this blog is a safe space for psychotic people regardless of whether we choose medication or not. You don't owe anyone an explanation. And no one owes you an explanation. We can and should freely share information and experiences, but we should aim to do so without judgement and without claiming "wrong and right" individual conclusions.
#pseriouslyschizophrenic#actuallypsychotic#schizo spec#antipsychotics#medication#psychiatry critical
54 notes
·
View notes
Text
an unstoppable force (my moral objection to working in a psychiatric setting because i know the abuse that so often takes place there and i can’t stand the idea of ever participating in or benefiting from something that treats people that way) meets an immovable object (i made the mistake of being a psych major years ago so now those are the most common jobs in my area that i’m actually qualified for and i need money so bad if i want to get out of the hell house i live in anytime soon)
#i have an interview today and i feel so guilty for even applying#but FUCK i need money#i just need to move out of my shitty transphobic neglectful parents’ house#and then i’ll be closer to jobs that i don’t despise the idea of doing#im going to keep applying and looking for better shit but i hate that i might have to do that for any amount of time#but honestly i don’t know if there’s really even anything else for me to find atm#i WILL quit on the spot if they ask me directly to do some fucked up shit tho#like i’ll suck up being in that setting temporarily so i can get out but i will not actively participate#god i hate it here#going back in time to tell my past self that being a psych major is such a bad idea and i’ll just come to hate the field#poss.speaks#vent#personal#anti psychiatry#psychiatry critical#not avpd
31 notes
·
View notes
Text
0. The really simple story of psychiatry
No psychiatric treatments have ever been based on any scientific discovery of the cause of anything psychiatry calls “mental illness” and no causes have ever been found.
Treatments are entirely based on hiding symptoms, with the underlying conditions never addressed.
#psychiatry#anti psychiatry#anti psych#mental illness#mental health#psych critical#psychiatry critical
9 notes
·
View notes
Text

Disorder (and the DSM) is a subjective term rooted in neuronormativity and by default; colonialism, captialism and white supremacy.
If disorder is the lens of the pathology paradigm, neurodivergent is the lens of the neurodiversity paradigm.
This is why disorder and neurodivergent are not interchangeable and why, if we are aiming to be neurodiversity affirming and unpack neuronormativity, we need to move away from disorder; a term that reinforces neuronormativity and pathologises anyone who diverges from it.
You cannot be neurodiversity affirming until you stop viewing people as having a disorder. If you can do it for Autism or ADHD, you can do it for every other neurodivergence.
Disorder isn’t neutral. Never has been.
@livedexperienceeducator
#neurodivergence is not disorder#neurodiversity paradigm#neurodiversity#neurodivergence#autism#adhd#ptsd#cptsd#complex trauma#mental health#psychology#diagnostic model#dsm#mad pride#psychiatry critical#language#resources
17 notes
·
View notes
Text
SSRIs are so statistically ineffective when compared to a placebo that it's baffling that they're handed out like candy
3 notes
·
View notes
Text
Good news! There are plenty! Most of which have been in practice for years and have been shown to work! And these are just some of the alternatives!
#my art#mental health#mental health reform#psych reform#psychiatry critical#healthcare#healthcare reform#anti psychiatry#psychiatry#psychology#mental illness#psych critical
438 notes
·
View notes
Note
I think sensory processing issues aren't seen as specific to asd is because
1) sensory processing issues are either an incredibly common symptom found in a lot of neurodivergencies or their own separate disorder that is commonly comorbid with asd (I personally like to think of them as their own separate thing as many people in my family have sensory processing issues but otherwise would be considered neurotypical)
2) it's only in the most recent edition of the dsm that sensory processing issues are mentioned in connection to asd, specifically in the "determining severity level" section (I personally dislike this change since I don't get why you'd use a sensory disorder to determine the severity of a social skills/communication/executive functioning disorder)
But basically it boils down to sensory processing issues being acknowledged as a common symptom in multiple disorders before this current wave of asd activism, combined with sensory processing issues only recently being officially connected with asd in the dsm.
Also I just want to say I really appreciate your posts about symptoms not being tied to one diagnosis and about relating and stuff. Sensory processing issues run in my family, and I had ongoing trauma my entire childhood that started before I can remember, so it's literally impossible to say in my case whether I'm autistic, have sensory processing issues and trauma, or some combination of those things. I've also got some type of dissociative plurality thing going on but it doesn't really match the experiences I've seen other people describe and like. It's just really nice seeing the acknowledgement from someone else that not everyone is going to fit neatly in the boxes created by the dsm or online disability communities
Hey!! Yeah I think you are correct on account of the sensory processing - it's a trait commonly seen in a variety of difficulties (and even on its own entirely), and not as heavily associated with ASD specifically. And I feel like if hard pressed, most people would eventually agree that no ONE symptom or trait cannot exist in the same form in someone who's not austistic. And in that way I find myself questioning the protectiveness over certain terms that are used to describe some of those experiences. Esp when it's directed at other disabled and marginalized people who are looking for community and language to describe their experiences.. (not arguing anything, just thinking out loud :p)
I'm happy my post resonated with you!! I relate to what you describe to a degree, as well as I relate it to the experience of a number of my loved ones. And it's really one of the reasons I'm so against this "disorder superiority", where symptoms occurring outside a confirmed specific 'correct disorder' are considered misconstrued at best, fake at worst.
Which leads to everything from people telling me I "must be austistic" because I'm so awkward and weird, to people insisting my friend must have terrible "repressed childhood trauma" she has forgotten bc she has experiences of identity compartmentalization, to people hating on me for being "endo" until they talk to me for ten minutes and then insist I have osdd, to me anxiously trying to avoid using terms like stimming because it's not "mine" and I'm a bad ally if I don't say "fidgeting" bc only autistic people stim (but I also fidget and it's not the same thing), claiming my heavily traumatized partner can't have the symptoms of DID because most of the major trauma happened after he was 10, etc etc.
And it's shit bc for someone like you, it's not like you don't relate to autistic experiences a lot (orherwise you wouldn't be wondering), but unless you are willing to publically agree that you're austistic, there's going to be people who will be armchair diagnosing you if you talk about you experiences, or who will find it distasteful for you to discuss your experiences.
Similarly to how people on occasion have been SO MAD about my odd little plural identity stuff, until they conclude that I'm osdd but has been misled by the evil antipsychiatric agenda or whatever.. and it's like.
If the ONLY thing I would need to do differently for those people to stop being unhappy about my public behaviour is to diagnose myself with osdd (a disorder not present in any diagnostic manual where I live, and based on a set of symptoms that has been repeatedly (i believe wrongly) counted among my psychotic symptoms by all psychiatrists I've ever spoken to), then that's fucked up.
I DO NOT NEED TO CONSENT TO BEING CATEGORISED USING ANY WHICH SPECIFIC DIAGNOSTIC MANUAL FOR MY EXPERIENCES TO BE VALID.
[Do these people think that these sets of symptoms didn't exist before they got described in the Big Book? What ahistorical arrogance! To assume that yes, now, at this Peak of Psychiatric Science, we have finally successfully described all things ever correctly, and there could be no more left to discover or describe - yet clearly 30 years ago (or in most of the world) they were (are) missing a lot, according to these very same people?! Baffling.]
Ultimately it really doesn't matter whether any of us could or could not technically be diagnosed with this or that thing. And frankly, as an educated psychologist this may sound petty or even hypocritical.. But fucking hell, I am tired of the amount of deference to our psychiatric overlords and the DSM-bible..
And the amount of toxicity and exclusion and abuse and gatekeeping that is hiding behind "but science says...!".
It does not. It literally does not. I'm not gonna go into it heavily, but the classification of mental disorders is not a particularly data driven project.
Sorry for going off on a whole ass rant... oops... i think I'm in a Mood lol
2 notes
·
View notes
Text
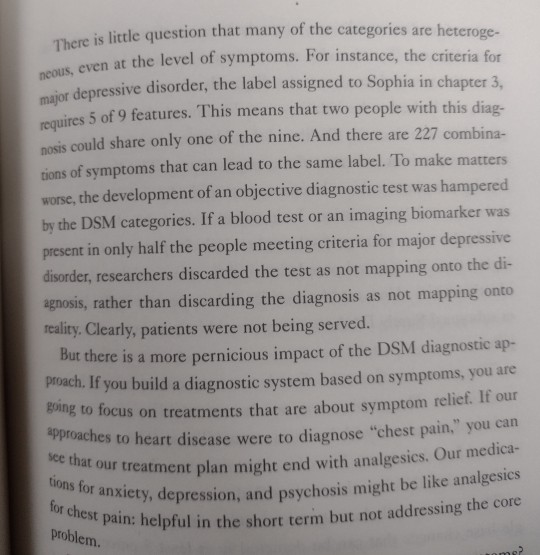
This puts so many of my issues with the DSM into words.
It fucks with research, it fucks with patient care, it's based on symptoms and not causes or treatment response. This means we could be lumping together groups of unrelated disorders simply because they have similar symptoms.
And that's not even getting into the patholigization of certain natural human differences, such as autism.
#Healing by Thomas Insel#Psych critical#Psychiatry critical#This book... Has some issues but I love his critique of the DSM
13 notes
·
View notes
Text
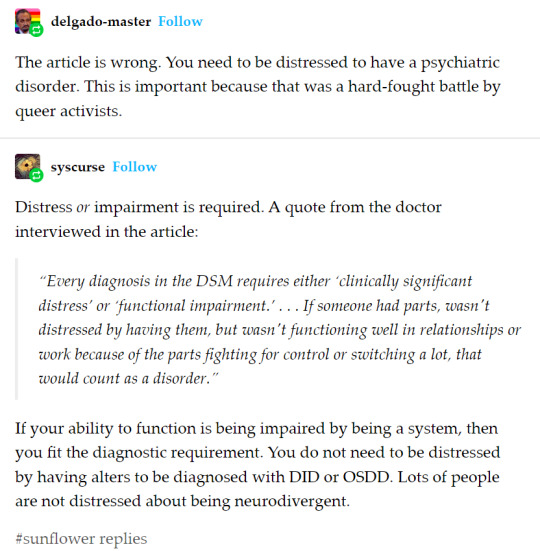

Sysmeds seem to be completely unable to be critical of the DSM or anything else they read if it’s “official,” lol.
The fight to exclude non-distressed impairment from definitions of disorder is a hard-fought ongoing battle by disability activists.
Currently, what is considered “functioning wrong” is determined entirely by (white Western) standards of what is “bad functioning”: when something goes against a set notion of what the body should be like/do. Once again sysmeds (like certain other bigoted/exclusionist/identity-invalidating/-disbelieving groups) essentialize the “default” human body (or what they consider the default) at the expense of individual needs and desires and experiences. If the body/mind is working “wrongly,” but the individual is okay with it and not distressed by it, where’s the issue? Why is it an illness, why does it need to be “fixed”?
Consider that not everyone aligns with the expected default regarding what they want and feel in comparison to what their body/mind is doing. And that is okay.
Major strawman/edge case there: anti-sysmedicalists have never said that the distress we discuss is “distress from knowing you have DID (they’re probably thinking of people feeling despair/internalized stigma).” We acknowledge that you can be in distress from experiencing DID while unaware/in denial of it. Not what this is about. If you “have parts” but are not in distress, it is not DID.
If someone “experiences issues” with relationships/work, that means they are distressed by it. But distress has to be evaluated in isolation: is their distress caused by having alters itself, or the alters fighting/switching a lot but not having alters itself (as in, if the fighting & frequent switching were addressed there would no longer be any distress), or is it because they are forced to do relationships/work because of society/capitalism forcing them into distressing situations they would not experience if they had choice in a liberated world?
Unless they aren’t distressed, but still do relationships/work in a way normative society considers “wrong”/rulebreaking/inefficient/whatever, and go through that totally aware and fine with it, and although they are incapable of forcing themselves to conform they are totally fine with not conforming. In which, once again, the problem would be with external society alone, not the way their brain works itself.
Perhaps think for a damn second before you start saying “disorder is when you can’t be a good little capitalist stooge on the assembly line being as productive as your peers even if you don’t have a problem with that as long as your bosses do.” Perhaps consider where that rhetoric likely came from, and who would benefit from it.
(Note: I’m not saying situations 1 or 2 would not qualify as DID/disordered. But clarifications.)
Seems like sysmeds on average/mostly consider autism inherently a disorder. But why would my autism be a disorder, if in an accommodating and non-stigmatizing world I would not experience any distress from the fact that I have it, and all the distress I experience right now is allowed to be because of/caused by external factors? (Obviously every autistic person has different experiences. But also, obviously, nuance exists.)
I do have actual disorders and the experience is quite different, they’re mostly hell with a few occasional reprieves (though I’m kind of recovering and have been doing better these past few months) but yeah, I’m extremely pissed off at medicalists trying to equate the two experiences. I (personally) would greatly appreciate if I had the option to make them/their symptoms go away entirely, as they’re quite unpleasant. I think it's quite ridiculous that certain people would claim experiencing that is equivalent to merely experiencing abnormality/non-normativity/divergence/difference.
Going to (shamelessly) self-promote my essay here, I scribbled it down at 2am two months ago and have been too low on spoons to edit out any potentially undesirable bits but I’m too tired of explaining the same things over and over and it’s reasonably comprehensive.
This post is not about origins, it is about currently experienced effects. Do not complain about this post being pro-/anti-endo, I’m pro-endo but that’s not really relevant to this.
#OP#syscourse#disability justice#disability liberation#neurodiversity#neurodivergent liberation#antipsych#anti psych#psych critical#psychiatry critical#autimedicalism#neuromedicalism#anti sysmedicalism#pro nondisordered systems#disabled#actually neurodivergent
28 notes
·
View notes
Photo
[Image Description: A series of tweets written by twitter user the_corvidae. The tweets read:
If you work within the psych system/as a mental health professional, know that your voice and opinion is not being centered on this account. You’re not disallowed from speaking but when I ask about experiences with mental health services, I am wholeheartedly not asking you.
Even if you are anti-psych. Even if you agree with what I’m saying. Even if you also have lived experiences as a patient. You’re working for the systemically oppressive system that is causing all of these issues. You’re going to be taken with a grain of salt, sorry not sorry.
Your voice is always the first voice people listen to on mental health. You are the one who is always believed, who is always respected and acknowledged in these discussions. I’m giving someone else a turn to actually be heard. People like me don’t often get that chance.
I distrust you because I distrust the oppressive institution that pays your bills. It’s as simple as that.
End image description.]
66 notes
·
View notes
Text
I don’t really like it when stoners criticize psych meds because of how they effect your mind as if weed induced psychosis is any better.
3 notes
·
View notes
Last Seen Blogs

duhasterreicht-wasduwolltest
BEST MOMENTS HAPPEN WHEN THEY ARE UNPLANNED

raccconteur
oh, baby

womensarts-blog
#WOMENSART

feydfuckery
long live #feydfuckernation

outboundmalangnolimit-blog
Outbound Malang