#social distensing
Text
diary126
1/18-19/2024
thursday - friday
should sleep soon.
the interview went very well i think. the guy seemed to like me and not care about anything. it seems like at this pizza place that is basically a pseudo chuck-e-cheese (i'm such a winner in life) i'll be working in the arcade area. i'm so freddy , i'm so fazbear.
i've gotta do a drug test and stuff. i'll ace that cuz i'm #straightedge. it's really easy for me to not do drugs, generally, or i guess i never have, so i don't really have the urge. i don't think i'm missing out on a lot, i don't even drink, some people find that very weird though.
i also spent all of today out with my gf and her mom, which was fun, we went to this cafe that's closing forever soon, it's really sweet, the place had a thing where you could write yourself a postcard and mail it to yourself, months in the future, a kind of time capsule-ish thing. the woman there told us that her dog just had puppies, and that she saw on her home camera, and had to close up shop to go help her dog, and then come back, and this was still happening, one puppy left inside the womb, still coming. she was very sad it seemed like, she said no one wanted to buy the business to someone on the phone, so they were just selling everything, all the stock, so my gf and i got some postcards, and some stickers, and other stuff. i'll post the postcards i got tomorrow but i just really like the box.
my gf got some sanrio ones, i should maybe get pix of those too.
today before the interview, while i was alone at home, i was just reading wiseblood by flannery o'conner, she's such a great writer, makes me want to write something fast/messy in that way again, i think that will filter down to music some way though. her approach to these overripe and grotesque distensions of reality, where everyone is haunted in excess, where we all know that as real and the exaggeration on lays bare what we use reason/social norms to displace. there is a part early on where you are watching a character stare through a window at a knee, fat and white, disembodied almost, just that one image through the window, this peeping tom preacher-but-not-a-preacher. there is a lot to say about it, flannery herself said she never gave up catholicism because she was forever haunted by it, the protagonist is similar, the guilt in him is infinite and inescapable, he is wrestling not with disbelief in god, but the impossibility of not believing in god. it is too base an assumption in his world, that jesus died for him, he's always trying to refute it, but it turns around on him always.
anyway, re: the job, the next thing is on monday at 3 pm.
re: music, i messed w/ the problem song, but tomorrow i'm just not gonna, i'm gonna try and get other stuff mixed better, and then when it's finally time to do another full listen i'll take my notes again and see, honest this time. i was listening to the locust and it just made me feel like i grasped something, idk, i don't know if i did really but that band always gives me ideas about how i should sound, they were so perfect, like an actual diamond in music, perfectly formed, geometric and strange, off in a cave unseen, crystalline growth out of waste, excess of time/life, gravestone clusters.
i am tired now thoo i hope i didn't fuck my sleep up or whatever. i have to be ready for monday
byebye!!!!!!!!!
1 note
·
View note
Photo

😩 Bloating and gas can make life's simplest moments uncomfortable. Whether you're at a party 🥂, a work meeting 💼, or just relaxing at home 🏡, persistent bloating and gas can disrupt your daily life and affect your well-being. We'll explain the common reasons behind bloating and gas, with a focus on those dealing with Irritable Bowel Syndrome (IBS) 🤯. We'll provide expert insights 📚 to help you understand the causes and discover effective solutions to ease your discomfort 🌈. Understanding the Impact of Bloating and Gas in IBS: Before we discuss the causes, let's grasp how bloating and gas affect individuals with IBS 🙌, and why living with these symptoms can be challenging. In the context of IBS, bloating goes beyond discomfort. It often means severe abdominal pain 🤢, an unrelenting feeling of fullness 🥴, and visible distension that can make daily tasks feel difficult 🏃♀️. For those with IBS, bloating is not an occasional bother; it's a constant companion, influencing daily decisions 🗓️. Excessive gas is also a significant issue for IBS sufferers. It's not just about occasional belching 😳 or flatulence 💨; it's a persistent struggle that adds stress and anxiety 😓 to daily life. The unpredictability of gas can lead to social isolation 🙈, significantly impacting one's quality of life 😔. The Unpredictability of IBS: Living with IBS means dealing with unpredictable discomfort. Symptoms can vary widely day-to-day 🌞, making planning activities challenging. Imagine canceling plans last minute due to sudden bloating or gas 🤦♂️. It's a daily battle often unnoticed by those who don't experience it firsthand. Navigating Triggers: One of the most frustrating aspects of IBS is identifying triggers for bloating and gas 🤯. It could be certain foods 🍔, stress 😫, hormonal changes 🌡️, or a combination. Recognizing and managing these triggers takes patience and persistence 💪. We can work towards a future where bloating and gas no longer dominate your daily life 🚀. Book a free discovery call on my website. #DigestiveHealth #IBSRelief #TheRealGutDoctor
0 notes
Text
Caquetá, village of Los Pozos, facilities of the Chinese oil company Emerald Energy, where 78 ESMAD uniformed men and six civilian workers were kidnapped. The Ombudsman's Office, the Ministries of the Interior, Justice, Mines, Environment, the High Commissioner for Peace and the Coordinator of the Colombian South East of Agrarian, Environmental and Social Processes (COSCOPASS), reached an unequal agreement: 19 agreements versus 2 peasant agreements. It is not possible to speak of a humanitarian siege because there were two deaths: a policeman with his throat cut, Deputy Ricardo Arley Monroy Prieto and a farmer who died from a shot. Who carried firearms at the time? The mob stirred up by the 27th front, Teófilo Forero column of the farc.
It must be remembered that, in June 2011, three Chinese contractor engineers from the same company, Hong, Jing, Fu and their translator, were kidnapped for a year. It is said out there that they were recovered after paying the ransom in Panama.
It was in front of Los Pozos, that President Andrés Pastrana was uselessly waiting for the presence of alias “Tirofijo”, in the Distension Zone from 1998 to 2002, a situation that gave rise to the popular La Silla Vacía website. In the village "Nueva Colombia", in the village of La Siberia, two days after the end of this concession to the farc, in the rural area, the politician Íngrid Betancourt was kidnapped.
Furthermore, the keys to battalion number 36 Cazadores de San Vicente de Caguan were handed over in good faith by the government in power, good faith that was abused by the narcoterrorists. There is an airstrip there with capacity for a C-130 Hercules and the Omega Joint Task Force currently operates.
If, since February of this year, they had warned of the social discontent that was cradling in that area, a transit route for drug trafficking, forecasts could well have been taken and more soldiers or police were sent to the site.
With all these backgrounds, no one escapes the importance of the staging on Saturday the 4th, with all its consequences. There is talk of a million dollars for blackmailing the Chinese communist government. Communists against communists.
Although, to tell the truth, faces we see hearts we do not know.
THE IMPROPER MONEY
The involvement of Petro's son, in the scandal of the financing of his father, is frankly noisy.
Even if his parent denies it, the embarrassing spectacle of the palace dolphin, it can be up to him, the president.
Well that he received them, well that he did not, of which there is no proof, although there would be according to a complaint filed before the Electoral Council about excesses of the money to finance his campaign.
And what about the pair of Spaniards, Vendrell and Grau?
1 note
·
View note
Text
Struggling With Severe Cancer Pain In The Middle Of Night?
Learn More About Breakthrough Pain In Cancer
Medical advancement has transitioned cancer from being a rapidly fatal disease to a chronic disease. Cancer pain, however, still remains a major problem affecting 30–40% at the time of diagnosis, and 75% of those with advanced cancer. Although it may not always be possible to relieve the cancer-related pain completely but fortunately it can be effectively managed in most individuals with appropriate therapy. Effective pain control has been shown to improve the quality of life in all stages of the disease. Breakthrough pain is one pain which troubles even those cancer patients whose pain is otherwise well controlled. Its management requires careful evaluation by specialists with attention to detail. In the subsequent section we discuss more about the breakthrough pain and commonly asked questions.
What is breakthrough pain?
Breakthrough cancer pain (BTcP) is a transient exacerbation of pain superimposed on the background of controlled persistent pain. In simple words it refers to the sudden, relatively short lasting severe pain episodes one experiences from time to time, often catching one unprepared, despite having background pain well controlled.
Here are a few characteristics of breakthrough pain
Pain is of moderate to severe intensity (between 4-10/10, average score 7/10)
Onset is rapid (between 3 to 5 minutes) or in some cases more gradual reaching peak intensity within a few minutes. In about two thirds of the patients time to maximum pain intensity is less than 10 minutes
Duration of an untreated episode can be between 1 min and 4 h (average 30 min)
Multiple, predictable (in one third of patients) or unpredictable episodes throughout the day
Effective pain management requires assessment of responsible factors and having a management plan rather than trying to reach out for emergency services during unsocial hours in a panic mode.
How common is breakthrough pain and what causes this pain?
BTcP is a common problem with studies reporting the incidence as approx. 50% to 75%. This is despite using strong painkillers to control the baseline pain. Patients with the severe persisting pain, advanced cancer disease, and aggressive anticancer treatments are more likely to experience breakthrough pain.
BTcP may result from the cancer itself (70–80% of cases) or the anticancer treatment (10–20% of cases) and is seen more commonly is association with certain cancers like head and neck cancer (70%), gastrointestinal (59%), lung (55%) and breast cancer (52%). Common examples of BTcP include mouth pain on swallowing due to inflammation of mouth lining (mucositis) or bone pain due to movement.
BTcP can originate from numerous sources (somatic, visceral, or neuropathic) and the cause may be different from the sources of persisting background pain. It may be associated with
Voluntary movements like sitting, standing
Involuntary movements like intestinal distension or
May occur spontaneously
This distinction is relevant as it may encourage more targeted treatment approaches. Up to half of the patients may experience two or more types of BTcP. Sometimes the term episodic pain is used synonymously with breakthrough pain although some researchers ascribe a different meaning to this term.
Another type of BTcP which one commonly encounters is the increased pain that can occur when the effect of painkillers is wearing off, just before the next dose is due. This is addressed as the “end of dose failure.” Some studies include this as a type of breakthrough pain whereas others do not.
Why do we need to treat breakthrough pain?
Breakthrough cancer pain is a common problem and can be associated with a variety of physical, psychological and social complications. Persisting pain often robs the sufferers of their independence and their ability to perform routine tasks, adversely affecting the quality of life. Besides causing suffering, the severity and unpredictability of breakthrough pain can adversely impact one’s confidence level, emotional health and social interactions. Moreover, it is associated with increased utilisation of healthcare and social care services with obvious financial implications.
How do we address this type of pain?
All cancer pain patients should be specifically assessed for the presence of BTcP. A standard pain management & palliative care practice is to prescribe medications for the constant background pain and a separate on-demand dose of pain relieving measures for breakthrough pain. In BTcP there is no one treatment which works universally and the treatment needs to be individualised.
Selecting the right option requires a fair amount of expertise and familiarity with all the available options. There are a number of factors which need to be taken in to account when deciding on the treatment and these include
Underlying cause of pain
Type of pain (nerve pain, nociceptive, mixed)
Pain characteristics (onset, duration, severity)
Predictable or unpredictable
Previous response to pain relieving medications including opioids (efficacy, tolerability)
Background analgesic medications (may need to be adjusted) and drug interactions
Patient-related factors including age, other organ function, stage of the cancer and individual preferences
Cost, availability and safety aspects
Opioids (morphine like drugs) are considered as the preferred medications for treating BTcP. The profile of the drug selected to treat the BTcP needs to mirror the pain profile one is experiencing. For example, in cases of sudden onset short-lasting pain episodes, drugs like oral morphine may prove to be ineffective as they take 30 to 45 minutes to work. In such a situation rapidly acting drugs are more likely to be useful. A mismatch between pain profile and drug selected is likely to produce poor relief and/or more side effects
The route of drug administration is important as it controls how quickly the pain relieving effects are apparent. Drugs given directly into the veins have a rapid effect although it requires an intravenous cannula to be present. Alternative routes such as through the nose or by intraoral route (sucking on tablets) of the rightly chosen drugs work within 5 -15 min. The dose of ‘rescue medication’ is determined by individual titration to ensure maximum relief with minimal side effects and may be subject to change over time.
A predictable episode of BTcP triggered by known factors for example, eating can be managed by a planned administration of medicine prior to the activity taking into account the time taken for the medication to work. Some patients choose to restrict activity to reduce the number of BTcP episodes.
Once the trial medication has been started, dose titration and regular reassessments are essential. All patients with new BTcP medications should be reevaluated within 48–72 h. Patient education regarding the correct and appropriate use of medications is essential as research evidence demonstrates incorrect usage, misuse / abuse and underuse in a significant proportion.
Other non-opioid drugs are also useful in the management of BTcP. Examples include anti-inflammatories, benzodiazepines, paracetamol etc. Preventing and treating BTcP is not just about medications as interventional techniques and non-pharmacological methods are other options which can be helpful.
TAG : Body pain treatment in Delhi , Best Back Pain Doctor in Delhi , Pain Specialist in Delhi, Best pain specialist in Delhi, Back pain treatment in Delhi, Cancer Pain treatment in Delhi
#Dr. Amod Manocha#Cancer Pain treatment in Gurgaon#Cancer Pain Treatment in Delhi#Pain Specialist in Gurgaon#pain#Pain Management in South Delhi
0 notes
Text
What Are The Signs When I Should Consult A Gastroenterologist?
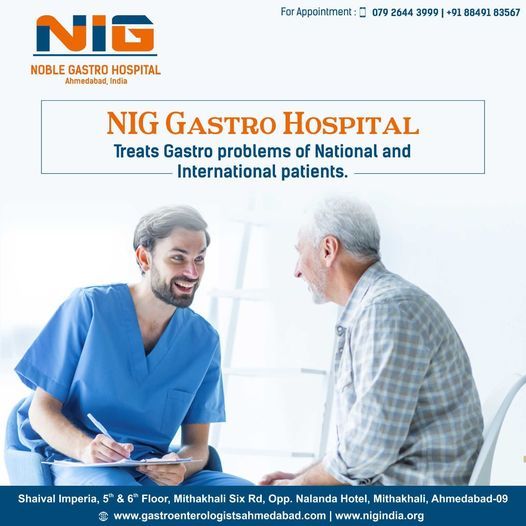
1. DIFFICULTY IN SWALLOWING When a patient feels that something is caught in the food pipe, it usually requires an upper GI endoscopy for diagnosis and further organization of the said problem. Endoscopy can diagnose difficulties like reflux esophagitis, tumour of the oesophagus, achalasia cardiac, and stricture (narrowing of the oesophagus). These problems can be managed by detailed medications, endoscopic procedures, or surgery. Hence, assembly a gastroenterologist, before you lose significant weight is extremely advisable.
2. STANDING ACIDITY AND INDIGESTION Patients by short-lasting symptoms of acidity, liquid reflux, or digestions can be managed by temporary over-the-counter tablet, while when these symptoms are chronic and long-standing, they must see a gastroenterologist for more direction. These patients often have H Pylori infections. In presence of weight loss, persistent vomiting, or bleeding serious problems like a gastric ulcer bleeding, tumour or dilated veins in the stomach region can be found during endoscopy.
3. BLOOD IN VOMITING The presence of blood in vomiting indicated a medical crisis. In such a situation, the patient may need emergency endoscopy apart from medical management, resuscitation, and blood transfusion. In these patients active bleeding is controlled by endoscopy, sometimes further bleeding is prevented by endoscopy.
4. CONSTIPATION Constipation is a very common problem seen international and is often overlooked. Constipation not only produces symptoms like feeling of incomplete evacuation, and abdominal pain but it also generates social and mental distress. Careful examination, laboratory investigation, and colonoscopy help to find out the cause of constipation, and treating them makes patients feel the same. Irritable bowel disease, functional constipation, colonic tumors, colonic polyps, inflammation of the rectum, and solitary rectal ulcer syndrome are the common treatable causes of constipation.
5. BLOOD IN STOOLS The appearance of blood in stool in small quantities can be achieved on outpatient bases, while a large amount of blood in stools can become a medical emergency. Ulcers in the internal lining of the small or large bowel, tumor, or polyp can be readily diagnosed and treated by endoscopy. Gastroenterology is a very vast subject, multiple reasons are seen in various patients with pain in the abdomen, vomiting, distension of the abdomen, or assembly of fluid in the abdomen. These all patients require to see a gastroenterologist for finding out the reason and the way to get relief from it. There could be multiple causes of shoulder pain in teenagers and adolescent kids. It is important to seek prompt medical attention and suitable orthopaedic treatment that relieves them from pain and inflammation while ensuring their ability to resume active sports.
Best Gastroenterologist Doctor In Ahmedabad
Constipation Doctor In Ahmedabad
Top Gastroenterologist In Ahmedabad
#Top Gastroenterologist In Ahmedabad#Best Gastroenterologist Doctor In Ahmedabad#Gastro Hospital In Ahmedabad#Gastroenterologist Near Me#Gastroenterologist In Ahmedabad
0 notes
Text
Cancer Pain Treatment in Gurgaon
Struggling With Severe Cancer Pain In The Middle Of Night?
Learn More About Breakthrough Pain In Cancer
Medical advancement has transitioned cancer from being a rapidly fatal disease to chronic disease. Cancer pain, however, still remains a major problem affecting 30–40% at the time of diagnosis, and 75% of those with advanced cancer. Although it may not always be possible to relieve cancer-related pain completely fortunately it can be effectively managed in most individuals with appropriate therapy. Effective pain control has been shown to improve the quality of life in all stages of the disease. Breakthrough pain is one pain that troubles even those cancer patients whose pain is otherwise well controlled. Its management requires careful evaluation by specialists with attention to detail. In the subsequent section we discuss more breakthrough pain and commonly asked questions.
What is breakthrough pain?
Breakthrough cancer pain (BTcP) is a transient exacerbation of pain superimposed on the background of controlled persistent pain. In simple words it refers to the sudden, relatively short-lasting severe pain episodes one experiences from time to time, often catching one unprepared, despite having background pain well controlled.
Here are a few characteristics of breakthrough pain
Pain is of moderate to severe intensity (between 4-10/10, average score 7/10)
Onset is rapid (between 3 to 5 minutes) or in some cases more gradual reaching peak intensity within a few minutes. In about two-thirds of the patients, the time to maximum pain intensity is less than 10 minutes
The duration of an untreated episode can be between 1 min and 4 h (average 30 min)
Multiple, predictable (in one-third of patients) or unpredictable episodes throughout the day
Effective pain management requires assessment of responsible factors and having a management plan rather than trying to reach out for emergency services during unsocial hours in a panic mode.
How common is breakthrough pain and what causes this pain?
BTcP is a common problem with studies reporting the incidence as approx. 50% to 75%. This is despite using strong painkillers to control the baseline pain. Patients with severe persisting pain, advanced cancer disease, and aggressive anticancer treatments are more likely to experience breakthrough pain.
BTcP may result from cancer itself (70–80% of cases) or the anticancer treatment (10–20% of cases) and is seen more commonly associated with certain cancers like head and neck cancer (70%), gastrointestinal (59%), lung (55%) and breast cancer (52%). Common examples of BTcP include mouth pain on swallowing due to inflammation of mouth lining (mucositis) or bone pain due to movement.
BTcP can originate from numerous sources (somatic, visceral, or neuropathic) and the cause may be different from the sources of persisting background pain. It may be associated with
Voluntary movements like sitting, standing
Involuntary movements like intestinal distension or
May occur spontaneously
This distinction is relevant as it may encourage more targeted treatment approaches. Up to half of the patients may experience two or more types of BTcP. Sometimes the term episodic pain is used synonymously with breakthrough pain although some researchers ascribe a different meaning to this term.
Another type of BTcP that one commonly encounters is the increased pain that can occur when the effect of painkillers is wearing off, just before the next dose is due. This is addressed as the “end of dose failure.” Some studies include this as a type of breakthrough pain whereas others do not.
Why do we need to treat breakthrough pain?
Breakthrough cancer pain is a common problem and can be associated with a variety of physical, psychological and social complications. Persisting pain often robs the sufferers of their independence and their ability to perform routine tasks, adversely affecting the quality of life. Besides causing suffering, the severity and unpredictability of breakthrough pain can adversely impact one’s confidence level, emotional health, and social interactions. Moreover, it is associated with increased utilization of healthcare and social care services with obvious financial implications.
How do we address this type of pain?
All cancer pain patients should be specifically assessed for the presence of BTcP. Standard pain management & palliative care practice is to prescribe medications for the constant background pain and a separate on-demand dose of pain-relieving measures for breakthrough pain. In BTcP there is no one treatment that works universally and the treatment needs to be individualized.
Selecting the right option requires a fair amount of expertise and familiarity with all the available options. There are a number of factors that need to be taken into account when deciding on the treatment and these include
The underlying cause of pain
Type of pain (nerve pain, nociceptive, mixed)
Pain characteristics (onset, duration, severity)
Predictable or unpredictable
Previous response to pain-relieving medications including opioids (efficacy, tolerability)
Background analgesic medications (may need to be adjusted) and drug interactions
Patient-related factors include age, other organ function, stage of cancer and individual preferences
Cost, availability, and safety aspects
Opioids (morphine-like drugs) are considered the preferred medications for treating BTcP. The profile of the drug selected to treat the BTcP needs to mirror the pain profile one is experiencing. For example, in cases of sudden onset short-lasting pain episodes, drugs like oral morphine may prove to be ineffective as they take 30 to 45 minutes to work. In such a situation rapidly acting drugs are more likely to be useful. A mismatch between pain profile and drug selected is likely to produce poor relief and/or more side effects
The route of drug administration is important as it controls how quickly the pain-relieving effects are apparent. Drugs given directly into the veins have a rapid effect although it requires an intravenous cannula to be present. Alternative routes such as through the nose or by intraoral route (sucking on tablets) of the rightly chosen drugs work within 5 -15 min. The dose of ‘rescue medication’ is determined by individual titration to ensure maximum relief with minimal side effects and may be subject to change over time.
A predictable episode of BTcP triggered by known factors, for example, eating can be managed by a planned administration of medicine prior to the activity taking into account the time taken for the medication to work. Some patients choose to restrict activity to reduce the number of BTcP episodes.
Once the trial medication has been started, dose titration and regular reassessments are essential. All patients with new BTcP medications should be reevaluated within 48–72 h. Patient education regarding the correct and appropriate use of medications is essential as research evidence demonstrates incorrect usage, misuse/abuse, and underuse in a significant proportion.
Other non-opioid drugs are also useful in the management of BTcP. Examples include anti-inflammatories, benzodiazepines, paracetamol, etc. Preventing and treating BTcP is not just about medications as interventional techniques and non-pharmacological methods are other options that can be helpful.
Tags = Cancer Pain Treatment in Delhi, Pain Management in Delhi, Pain specialist in Gurgaon
Struggling With Severe Cancer Pain In
The Middle Of Night?
Learn More About Breakthrough Pain In Cancer
Medical advancement has transitioned cancer from being a rapidly fatal disease to chronic disease. Cancer pain, however, still remains a major problem affecting 30–40% at the time of diagnosis, and 75% of those with advanced cancer. Although it may not always be possible to relieve cancer-related pain completely fortunately it can be effectively managed in most individuals with appropriate therapy. Effective pain control has been shown to improve the quality of life in all stages of the disease. Breakthrough pain is one pain that troubles even those cancer patients whose pain is otherwise well controlled. Its management requires careful evaluation by specialists with attention to detail. In the subsequent section we discuss more breakthrough pain and commonly asked questions.
What is breakthrough pain?
Breakthrough cancer pain (BTcP) is a transient exacerbation of pain superimposed on the background of controlled persistent pain. In simple words it refers to the sudden, relatively short-lasting severe pain episodes one experiences from time to time, often catching one unprepared, despite having background pain well controlled.
Here are a few characteristics of breakthrough pain
Pain is of moderate to severe intensity (between 4-10/10, average score 7/10)
Onset is rapid (between 3 to 5 minutes) or in some cases more gradual reaching peak intensity within a few minutes. In about two-thirds of the patients, the time to maximum pain intensity is less than 10 minutes
The duration of an untreated episode can be between 1 min and 4 h (average 30 min)
Multiple, predictable (in one-third of patients) or unpredictable episodes throughout the day
Effective pain management requires assessment of responsible factors and having a management plan rather than trying to reach out for emergency services during unsocial hours in a panic mode.
How common is breakthrough pain and what causes this pain?
BTcP is a common problem with studies reporting the incidence as approx. 50% to 75%. This is despite using strong painkillers to control the baseline pain. Patients with severe persisting pain, advanced cancer disease, and aggressive anticancer treatments are more likely to experience breakthrough pain.
BTcP may result from cancer itself (70–80% of cases) or the anticancer treatment (10–20% of cases) and is seen more commonly associated with certain cancers like head and neck cancer (70%), gastrointestinal (59%), lung (55%) and breast cancer (52%). Common examples of BTcP include mouth pain on swallowing due to inflammation of mouth lining (mucositis) or bone pain due to movement.
BTcP can originate from numerous sources (somatic, visceral, or neuropathic) and the cause may be different from the sources of persisting background pain. It may be associated with
Voluntary movements like sitting, standing
Involuntary movements like intestinal distension or
May occur spontaneously
This distinction is relevant as it may encourage more targeted treatment approaches. Up to half of the patients may experience two or more types of BTcP. Sometimes the term episodic pain is used synonymously with breakthrough pain although some researchers ascribe a different meaning to this term.
Another type of BTcP that one commonly encounters is the increased pain that can occur when the effect of painkillers is wearing off, just before the next dose is due. This is addressed as the “end of dose failure.” Some studies include this as a type of breakthrough pain whereas others do not.
Why do we need to treat breakthrough pain?
Breakthrough cancer pain is a common problem and can be associated with a variety of physical, psychological and social complications. Persisting pain often robs the sufferers of their independence and their ability to perform routine tasks, adversely affecting the quality of life. Besides causing suffering, the severity and unpredictability of breakthrough pain can adversely impact one’s confidence level, emotional health, and social interactions. Moreover, it is associated with increased utilization of healthcare and social care services with obvious financial implications.
How do we address this type of pain?
All cancer pain patients should be specifically assessed for the presence of BTcP. Standard pain management & palliative care practice is to prescribe medications for the constant background pain and a separate on-demand dose of pain-relieving measures for breakthrough pain. In BTcP there is no one treatment that works universally and the treatment needs to be individualized.
Selecting the right option requires a fair amount of expertise and familiarity with all the available options. There are a number of factors that need to be taken into account when deciding on the treatment and these include
The underlying cause of pain
Type of pain (nerve pain, nociceptive, mixed)
Pain characteristics (onset, duration, severity)
Predictable or unpredictable
Previous response to pain-relieving medications including opioids (efficacy, tolerability)
Background analgesic medications (may need to be adjusted) and drug interactions
Patient-related factors include age, other organ function, stage of cancer and individual preferences
Cost, availability, and safety aspects
Opioids (morphine-like drugs) are considered the preferred medications for treating BTcP. The profile of the drug selected to treat the BTcP needs to mirror the pain profile one is experiencing. For example, in cases of sudden onset short-lasting pain episodes, drugs like oral morphine may prove to be ineffective as they take 30 to 45 minutes to work. In such a situation rapidly acting drugs are more likely to be useful. A mismatch between pain profile and drug selected is likely to produce poor relief and/or more side effects
The route of drug administration is important as it controls how quickly the pain-relieving effects are apparent. Drugs given directly into the veins have a rapid effect although it requires an intravenous cannula to be present. Alternative routes such as through the nose or by intraoral route (sucking on tablets) of the rightly chosen drugs work within 5 -15 min. The dose of ‘rescue medication’ is determined by individual titration to ensure maximum relief with minimal side effects and may be subject to change over time.
A predictable episode of BTcP triggered by known factors, for example, eating can be managed by a planned administration of medicine prior to the activity taking into account the time taken for the medication to work. Some patients choose to restrict activity to reduce the number of BTcP episodes.
Once the trial medication has been started, dose titration and regular reassessments are essential. All patients with new BTcP medications should be reevaluated within 48–72 h. Patient education regarding the correct and appropriate use of medications is essential as research evidence demonstrates incorrect usage, misuse/abuse, and underuse in a significant proportion.
Other non-opioid drugs are also useful in the management of BTcP. Examples include anti-inflammatories, benzodiazepines, paracetamol, etc. Preventing and treating BTcP is not just about medications as interventional techniques and non-pharmacological methods are other options that can be helpful.
Tags = Cancer Pain Treatment in Delhi, Pain Management in Delhi, Pain specialist in Gurgaon
0 notes
Text
How to Deal With a Traumatized Animal

You might question exactly how to handle a shocked animal. This post will explore the sources of injury as well as exactly how to deal with trauma in pets. Injury can originate from a selection of resources, including misuse, forget, or workplace. Regardless of the source, a pet misbehaving ought to be treated in the same way as humans. Besides, they will never ever be the same as well as will be prone to issue scenarios for the rest of their lives. Research has actually revealed that a high portion of adult female giraffes living in the Serengeti bear the marks of lion attacks. Harbor cetaceans living in the southerly North Sea have claw marks left by gray seals. In a similar way, one hundred percent of manta rays staying in some African waters have several shark bite injuries. PTSD as well as the linked signs can have a profound impact on a species' survival. The initial assessment of a shocked animal needs to be repeated usually.
A physician needs to keep in mind the pet's psychological state, dimension of its pupils, and any kind of other irregularities. A vet ought to additionally look for any type of signs of abdominal discomfort, wounding, or distension, which might be indicative of fluid or gas in the abdomen. Stomach X-rays are additionally valuable in recognizing bladder integrity and also establishing if the animal is struggling with interior bleeding or an intestinal system tear. An elephant's action to a hazard or harmful circumstance is commonly an indication of trauma, which might result in serious consequences for the pet. In one research study, Karen McComb tape-recorded the reactions of elephant herds to unfamiliar sounds and also calls. She likewise videotaped how wild elephants reacted to the sound of an elephant. Protected herds showed increased PTSD-like symptoms. Jumbo as well as various other elephants in the wild likewise suffered unplanned killing. Elephants experience cumulative trauma as well as mourning. Click on this link for more information on how to deal with a traumatized animal.
This psychological reaction can affect the pet's social behavior as well as team organization. It can also affect its interactions with other teams. One example is the tusk killing, which is a serious traumatic experience for an elephant. This occasion has actually epigenetically impacted the psychology of these pets. On top of that, elephants are specifically at risk to the effects of trauma if their moms have been eliminated. As an example, if a research study reveals that a drug is causing PTSD in an animal, it is not likely to be efficient in humans. Animal models are likewise subject to inequalities in between their behavioral patterns and also the differing symptoms of human PTSD. An inadequately translated research can result in an imprecise diagnosis and inadequate treatments. As well as animal models are an important tool for research and development. If you're questioning just how to handle injury in pets, consider this.
Keep reading on https://en.wikipedia.org/wiki/Psychological_trauma and most importantly, convert your knowledge into action, otherwise it remains a source of untapped energy as well as wasted potential.
1 note
·
View note
Text
Alcoholic Liver Disease in Delhi - Gastrodelhi
The liver is the site of alcohol metabolism. Excess to alcohol can overwhelm this capacity and lead to the development of what is called Alcoholic Liver Disease. The damage caused to the liver by alcohol can take the form of fatty liver, alcoholic hepatitis, or cirrhosis (permanent damage with scarring).
According to an estimate of around 1.4 lakh, people died of cirrhosis related to excessive alcohol consumption in the year 2016. Almost all of the heavy drinkers will have a fatty liver. Higher the amount of alcohol consumption and longer it is consumed bears a direct relation to the development of cirrhosis. Men are likely to have cirrhosis than women due to a higher amount of alcohol consumed. Women have twice the higher risk of developing cirrhosis than men.
Stages of Alcoholic Liver Disease
The spectrum includes a simple fatty liver, acute alcoholic hepatitis, and alcoholic cirrhosis. It is the natural history of the disease but the overlap can occur.
Hepatic Steatosis or Fatty Liver: There is an accumulation of fat in the liver. This stage is reversible with alcohol abstinence i.e. quitting alcohol and modifying the sedentary lifestyle to a more active one.
Acute Alcoholic Hepatitis: It is the stage in which alcohol causes inflammation of the liver substance. The reversibility of the process depends upon the damage already done. Long term survival in alcoholic hepatitis patients who stop consuming alcohol is significantly greater than the patients who continue taking alcohol.
Alcoholic Cirrhosis: This is the end-stage liver disease which is considered to be irreversible. It is characterized by the scarring of the liver. It is the result of prolonged and severe liver damage.
Symptoms
The patients with fatty liver are usually asymptomatic.
Alcoholic hepatitis varies in severity and similarly the symptoms. Symptoms can be mild such as anorexia, weight loss, abdominal distension, nausea, or vomiting. In severe cases, it can present with encephalopathy and liver failure.
Alcoholic cirrhosis presents with signs and symptoms of liver failure such as jaundice, itching, loss of body hails, bleeding tendencies, hematemesis, ascites (collection of fluid in the abdomen), and encephalopathy (sleeplessness, drowsiness, confusion and if severe unconsciousness).
Diagnosis
With the suspicion of the disease the treating doctor will be getting –
Blood tests such as complete blood count, liver function test, coagulation profile, and others.
Ultrasound of the abdomen or CT scan of the abdomen will also be done as the case may be.
A liver biopsy may sometimes be needed.
Fibroscan is also helpful in assessing the severity and progression of the disease.
Treatment
The mainstay of the treatment of alcoholic liver disease is quitting alcohol. Quitting alcohol may not be easy for many and therefore requires proper counseling and rehabilitation program. Patients with severe symptoms may require hospitalization for workup and management. Alcoholic hepatitis patients usually have some nutritional deficiencies. They require vitamin supplementations and a good protein and caloric intake.
Liver transplantation is required for advanced cirrhosis with decompensation (ascites, encephalopathy, jaundice, variceal bleed). The earlier the option is taken the better the prognosis.
Conclusion
The spectrum of alcoholic liver disease is varied from the reversibility of fatty liver to the irreversibility of cirrhosis. Alcohol silently kills the drinker every passing day. It destroys the social, personal, and professional life of the patient.
Tag = GI Surgeon in Delhi
0 notes
Text



331 notes
·
View notes
Text
My parents have a patio so people can visit them and social distance. (Technically we made the flat walkway so my dad could get in and out easily after being in the hospital)
Anyway I was sitting out there and my dad goes “Just letting you know the missionaries are coming for a home visit on the patio and I don’t know when”
Me:

#former mormon#lds#exmo#exmormon#mormon#apostake#apostate#ex mormon#church#ex lds#ex cult#cult#church of jesus christ of latter day saints#religion#social distensing
22 notes
·
View notes
Text
How normal people social distance:


How the gays do it:


#Dazai Osamu#Nakahara Chuuya#Soukoku#dazai x chuuya#dachuu#bsd chuuya#bsd dazai#memes#bsd memes#yeet#corona#bungou stray dogs#bungou gay dogs#i am extra like chuuya#social distensing#gays
68 notes
·
View notes
Photo


“Time is the longest distance between two places.”
― Tennessee Williams, from The Glass Menagerie
#books#tennessee williams#the glass menagerie#plays#playwright#author quotes#book quotes#corona virus#social distensing#extinction#dinosaurs#parade
176 notes
·
View notes
Text


#hazbin#hazbin hotel#hazbin demon#social distensing#wear a mask#mask#stay safe#vaggie#hazbin vaggie#charlie#charlie hazbin hotel#hazbin charlie
50 notes
·
View notes
Text

Aubrey buys this for Barclay
#taz#the adventure zone#taz amnesty#the adventure zone amensty#aubrey little#taz aubrey#barclay#taz barclay#bigfoot#covid 19#social distensing
113 notes
·
View notes
Text
394 notes
·
View notes
Last Seen Blogs

neo-layouts
welcome to neo layouts !!

inclusive-picrews
PICREWS

headspace-hotel
I did it. I touched grass

shimadont
ryu ga waga teki wa shut the hell up

paulbro94
The Untitled Adventures of Captain Paulbro94