#survival rates
Text
How Effective Is Breast Cancer Screening?
Mammograms are a type of screening where images of the breast tissue are taken. Mammograms detect breast cancer cells in mammary glands, as well as identify growths and tumors that might not be found at a physical exam. A mammogram is basically a high-quality picture that takes different views from all angles to show anything off from tissues to cysts or clots hidden within the breasts.
0 notes
Text
Lung Cancer: Early Signs, Symptoms, Stages
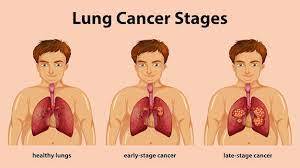
Cellular Deterioration in Pulmonary Tissues: The Dominant Precursor of Lethal Diseases
Cellular degradation within the pulmonary organs has emerged as the primary adversary confronting individuals afflicted by invasive neoplastic conditions, impacting not only spouses, acquaintances, and neighbors but also inflicting distress upon countless families. In the US, lung malignancies overwhelmed bosom carcinomas as the preeminent supporter of disease-related mortalities in ladies as soon as 1987. Cellular breakdown in the lungs losses comprise a fourth of all disease-related passings in America, outperforming the joined death paces of prostate, bosom, and colon malignancies. In 2017, almost 160,000 Americans capitulated to a cellular breakdown in the lungs.
Triggers of Pulmonary Carcinoma
The precise etiology of pulmonary carcinoma remains under meticulous scrutiny. Several risk elements have been identified as pivotal factors in the genesis of malignant cellular growths. Risk determinants encompass tobacco consumption, exposure to atmospheric contamination, and hereditary factors.
Does Tobacco Consumption Instigate Pulmonary Carcinoma?
The primary catalyst for pulmonary carcinoma in Homo sapiens is the utilization of tobacco products. In 1876, an apparatus was devised to mass-produce cylindrical tobacco sticks, rendering tobacco commodities economically accessible to virtually all segments of society. Prior to this innovation, pulmonary carcinoma was a relatively infrequent occurrence. Subsequent to the proliferation of mass-produced cigarettes, tobacco consumption witnessed a steep ascent, coinciding with a parallel surge in the incidence of pulmonary carcinoma. Presently, roughly 90% of all instances of pulmonary carcinoma are inextricably linked to tobacco usage. Radon gas, environmental pollutants, noxious agents, and various other factors contribute to the residual 10%.
Cigarettes and tobacco smoke encompass an excess of 70 carcinogenic compounds. Some of the carcinogenic constituents detected within tobacco smoke comprise:
Lead (an exceptionally toxic metallic element)
Arsenic (a potent insecticidal compound)
Cadmium (a constituent of batteries)
Isoprene (employed in the production of synthetic rubber)
Benzene (an adjunct in fuel formulations)
Cigar smoke abounds in tobacco-specific nitrosamines (TSNAs), recognized for their particularly malign properties.
Pulmonary Carcinoma and Cilia
Tobacco smoke impairs and, on occasion, eradicates ciliated projections on respiratory tract epithelial cells, designated as cilia. Cilia conventionally function to evacuate toxic substances, carcinogens, viral agents, and bacterial pathogens. In situations where smoke disrupts or eradicates cilia, these deleterious substances may amass within the pulmonary tissues, potentially precipitating infections and pulmonary carcinoma.
Indications of Pulmonary Carcinoma
Regrettably, pulmonary carcinomas frequently remain asymptomatic during their initial stages or present with obscure clinical manifestations that individuals are apt to disregard. Approximately 25% of individuals afflicted by pulmonary carcinomas devoid of clinical indications receive a diagnosis subsequent to undergoing a thoracic radiograph or computed tomography (CT) scan during a routine medical assessment or investigative procedures. Clinical indications of pulmonary carcinoma that might manifest comprise:
Persistent, recurrent paroxysms of coughing
Lethargy
Unexplained corporeal mass reduction
Breathlessness or paroxysms of wheezing
Expectoration of hemoptoic mucus
Thoracic discomfort
Three Conventional Approaches for Screening Pulmonary Carcinoma
Pulmonary carcinoma screening typically entails the deployment of three modalities.
Physiological Appraisal
A physiological appraisal is conducted to discern signs of paroxysms of wheezing, breathlessness, coughing, discomfort, and other conceivable indicators of pulmonary carcinoma. The extent to which the carcinoma has progressed determines additional early indicators, encompassing anhidrosis, engorged cervical veins, facial edema, conspicuously constricted pupils, and other diagnostic cues. The physiological appraisal also encompasses a detailed review of the patient's tobacco consumption history, in conjunction with a thoracic radiograph.
Sputum Cytology Assessment
A sputum cytology assessment entails the microscopic examination of the patient's expectorated mucus (sputum).
Spiral Computed Tomography (CT) Imaging
This CT imaging methodology assembles an intricate portrait of the internal anatomical components of the patient's physique. Within a spiral CT apparatus, intricate images are captured of the principal constituents of the patient's corporeal structure. These images are subsequently correlated with an X-ray device to craft three-dimensional representations of the patient's inner bodily organs. These illustrations may potentially unveil neoplastic growths.
A logical report set that people between the ages of 55 and 74, who have supported everyday utilization of something like one bunch of cigarettes for at least 30 years, may get benefits from a winding CT output of the pneumonic organs.
Finding of Pneumonic Carcinoma
Should the outcomes of the screening examinations intimate the presence of pulmonary carcinoma in an individual, conclusive diagnostic tests may be executed by a pathologist. The pathologist will scrutinize pulmonary cellular entities obtained from the patient's expectorated mucus, sputum, or extracted via a biopsy procedure, for the purposes of classifying and staging the pulmonary carcinoma.
Pulmonary Carcinoma Biopsy
As previously elucidated, the most efficacious approach for definitively diagnosing pulmonary carcinoma typically involves procuring a biological tissue specimen from the site of the suspected carcinoma. In most instances, pulmonary biopsies are obtained by means of a needle biopsy, bronchoscopic biopsy of the pulmonary organs, or via surgical excision of corporeal tissue. Various supplementary diagnostic assessments may be administered to accrue supplemental insights into the extent of the ailment's dissemination.
For further information concerning the categories of pulmonary carcinoma and the staging of pulmonary carcinoma, including stage IV pulmonary carcinoma, please refer to the subsequent segments.
Varieties of Pulmonary Carcinoma
Aspiratory carcinomas can be arranged into simply two essential groupings: little cell pneumonic carcinoma and non-little cell pneumonic carcinoma. Under 5% of pneumonic carcinomas will appear as a carcinoid neoplasm, while other abnormal malignancies include adenoid cystic carcinomas, lymphomas, and sarcomas. Significantly, occurrences of neoplastic arrangements beginning somewhere else inside the body and penetrating the pneumonic organs are not delegated aspiratory carcinomas.
Non-Small Cell Pulmonary Carcinoma
Non-small cell pulmonary carcinomas represent the most prevalent variant of pulmonary carcinoma. These malignancies account for roughly 90% of all pulmonary carcinomas and exhibit a relatively indolent course in comparison to small cell pulmonary carcinomas, signifying a more protracted progression to metastatic dissemination.
Small Cell Pulmonary Carcinoma
Small cell pulmonary carcinoma, colloquially known as oat cell pulmonary carcinoma, encompasses nearly 10% of all pulmonary carcinomas. This specific neoplastic form tends to disseminate with rapidity.
Stages of Pulmonary Carcinoma: 0-4
Subsequent to the determination of the specific subtype of pulmonary carcinoma, the condition is further stratified in terms of its pulmonary carcinoma staging. The staging system provides insights into the extent of neoplastic dissemination throughout the bodily structure, including its metastasis to lymph nodes or remote organ systems such as the cerebral cortex. Distinctions exist between the staging criteria for non-small cell pulmonary carcinomas and small cell pulmonary carcinomas. The ensuing stage classifications are extrapolated from the National Cancer Institute's documentation on pulmonary carcinoma staging; alternative staging methodologies may exhibit variations in categorization, such as the American Cancer Society's TNM classification scheme:
Small Cell Pulmonary Carcinoma Stages
Limited Stage: This stage designates small cell pulmonary carcinoma that remains confined to one hemisphere of the thoracic cavity, typically involving the pulmonary tissues and adjacent lymphatic structures. Approximately one-third of individuals diagnosed with small cell pulmonary carcinoma initially present with limited stage malignancies.
Extensive Stage: This pertains to small cell pulmonary carcinoma that has disseminated beyond the confines of a single pulmonary lobe, affecting either both pulmonary lobes, lymph nodes situated contralateral to the thoracic cavity, or extrapulmonary locations. Approximately two-thirds of individuals diagnosed with small cell pulmonary carcinoma initially present with extensive stage malignancies.
Non-Small Cell Pulmonary Carcinoma Stages
Occult (Hidden) Stage: In this phase, neoplastic cells are discernible in sputum cytology tests or alternative diagnostic procedures, albeit without an ascertained origin of the neoplastic process.
Stage 0 (Carcinoma in situ): This pulmonary carcinoma stage confines the presence of neoplastic cells to the superficial strata of the respiratory tract's mucosal lining, without penetration into deeper pulmonary tissues or extrapulmonary dissemination.
Stage I: Characterized by the detection of minute pulmonary neoplasms (measuring under 3 centimeters in diameter) that have not yet infiltrated adjacent pulmonary parenchyma, lymph nodes, or the principal bronchial segments of the pulmonary organs.
Stage II: Stage II pulmonary carcinoma can be diagnosed through various modalities. One plausible scenario is the infiltration of lymph nodes in proximity to the pulmonary organs.
Stage IIA: Neoplastic tumors measuring between 3 and 5 centimeters in diameter are categorized as Stage IIA, with additional criteria potentially contributing to this designation.
Stage IIB: Tumors within the range of 5 to 7 centimeters in diameter are classified as Stage IIB pulmonary carcinoma. Supplementary considerations may factor into this classification.
Stage III: Analogous to Stage II pulmonary carcinoma, Stage III comprises multiple interpretive frameworks. One elucidation denotes the coexistence of pulmonary neoplasia within the pulmonary organs and lymph nodes situated within the thoracic cavity. Stage III pulmonary carcinoma is further subdivided into two distinct subsets.
Stage IIIA: This category defines pulmonary carcinoma that has propagated to the ipsilateral thoracic cavity.
Stage IIIB: This classification characterizes pulmonary carcinoma whereby the affliction has extended to either the contralateral thoracic cavity or cranial to the clavicle.
Stage IV: This constitutes the terminal phase of pulmonary carcinoma. Neoplastic formations may exhibit varying dimensions, but two out of three of the ensuing criteria must be met:
Dissemination of the carcinoma to the contralateral pulmonary lobe of origin.
Identification of neoplastic cells within the serous fluid surrounding the pulmonary organs.
Neoplastic cellular presence within the serous fluid encapsulating the cardiac organ.
Deciphering Lung Cancer Survival Probabilities and Therapeutic Alternatives
Lung malignancy emerges as an imposing adversary, adept at concealing itself during its initial phases and presenting dismal prospects for those entrenched in its advanced stages. The metrics for survival exhibit fluctuations contingent upon the specific cancer subtype. According to statistics disseminated by the American Cancer Society, the five-year survival quotient for non-small cell lung carcinoma hovers around 24% across all phases. In stark contrast, small cell lung carcinoma regrettably plummets to an abysmal 6%. It is, however, noteworthy that these figures are susceptible to substantial augmentation when the ailment is identified and treated within the confines of its localized or regional confines, with distant-stage lung cancer manifesting as the most adverse scenario.
Surgical Interventions for Lung Cancer
In instances of rudimentary-stage (stage 0 or certain stage I) non-small cell lung carcinoma, surgical recourse proffers itself as a viable therapeutic modality. This procedural maneuver entails the excision of a segment or, in some instances, the entirety of the lung locus harboring the malignancy, occasionally culminating in a comprehensive remission. Nevertheless, it is imperative to acknowledge that a considerable cohort of patients still necessitates chemotherapy, radiation therapy, or a composite amalgamation thereof, aimed at eliminating any residual cancerous entities that may have eluded the surgical intervention. Regrettably, small cell lung carcinomas are rarely apprehended during their incipient phases, which invariably relegates both surgical procedures and ancillary treatment modalities to predominantly palliative roles, extending only a limited prospect of potential cure.
Cutting-edge Lung Cancer Remedial Approaches
The conventional armamentarium for addressing both small cell and non-small cell lung carcinomas frequently encompasses chemotherapy and, in select circumstances, radiation therapy and surgical interventions. Numerous patients grappling with the complexities of advanced-stage maladies receive a synergistic orchestration of these interventions, meticulously tailored to their specific clinical panorama and predicated upon the directives tendered by their oncological consultants.
Precision Therapeutics for Lung Cancer
Precision therapeutics are strategically poised to thwart or impede the proliferation of neoplastic cells by directing their focus towards the requisite vascularization imperative for their sustenance and proliferation. Simultaneously, alternate therapeutic modalities set their sights on sabotaging the molecular signaling cascades requisite for the multiplication and dissemination of malignant cells.
Empirical Investigations into Lung Cancer
In addition to precision therapeutics, a plethora of empirical studies and clinical assays present themselves as accessible avenues for eligible individuals. Some of these investigational forays may be feasibly accessible within a localized purview, affording afflicted individuals the invaluable opportunity to engage with pioneering therapeutic approaches and protocols in the sphere of lung cancer management.
Existence Beyond the Pronouncement of a Lung Cancer Diagnosis
The reception of a lung cancer diagnosis invariably evokes an inundation of emotions, chief among them being a palpable sense of being overwhelmed and despondency. Nonetheless, a ray of optimism emanates from the crucible of ongoing scientific research, kindling the flame of hope for survival and an elongated lifespan, contingent upon the judicious pursuit of apt therapeutic interventions. Accumulated scientific evidence underscores the superior prognosis accorded to individuals who elect to embrace a salubrious lifestyle and embark upon the path of smoking cessation, vis-à-vis their counterparts who eschew such transformative measures.
Lung Cancer and Passive Smoking
It is salient to underscore that tobacco smokers do not only imperil their individual health but also imperil the well-being of non-smokers inhabiting their immediate sphere, which includes spouses, offspring, and significant others. Exposure to secondhand smoke in the ambient environment confers a daunting 20% to 30% augmented susceptibility to the onset of lung cancer in these non-smoking individuals.
Occupational Exposure and Lung Cancer
While it remains an incontrovertible verity that smoking is the predominant etiological agent precipitating lung carcinoma, it is pertinent to acknowledge that a heterogeneous compendium of chemicals and compounds also transposes an elevated risk quotient. Agents such as asbestos, uranium, arsenic, benzene, and sundry others significantly amplify the proclivity for the development of lung cancer. Notably, exposure to asbestos, for instance, may instigate lung malignancy, manifesting as mesothelioma, numerous decades post-initial contact, thereby perpetuating the specter of lung infirmity over protracted time frames.
Radon Gas and Lung Cancer
Radon gas emerges as the second most formidable trigger of lung cancer. It subsists as an innate occurrence but is prone to permeating residential edifices, amassing within subterranean basements and crawl spaces. Although its qualities encompass odorlessness and chromatic neutrality, it remains susceptible to detection via simplistic and cost-effective examination kits. It is imperative to recognize that smokers who confront this insidious gas hazard an augmented proclivity for the incipience of lung cancer, contrasted with their non-smoking counterparts.
Atmospheric Contamination and Lung Cancer
Certain pundits in the scientific community postulate the connotation between atmospheric contamination and the genesis of lung carcinoma. Multiple investigations tender a repository of data proffering cogent substantiation for the inference that atmospheric pollutants, including diesel exhaust, may substantially contribute to the genesis of lung cancer in select individuals. Conservative estimates from researchers posit that approximately 5% of lung cancer incidents can be imputed to the pernicious influence of atmospheric pollution.
Supplementary Risk Factors for Lung Cancer
Despite the proliferation of insights into the intricacies of lung cancer, myriad complexities and scenarios remain enshrouded in the mists of obscurity. An exemplary conundrum resides in the enigmatic proclivity for certain families to manifest a lineage characterized by the scourge of lung cancer, notwithstanding the absence of apparent precipitating risk factors. Analogous mysteries persist in relation to specific patients who fall victim to lung cancer in the absence of readily discernible risk factors. There exists a tentative correlation between the consumption of water exhibiting elevated arsenic concentrations and the augmentation of lung cancer vulnerability, yet the precise mechanistic underpinnings of this phenomenon remain an enigma. Analogously, the rationale behind the preponderance of adenocarcinoma incidence among non-smokers, rather than their smoking counterparts, remains elusive.
Lung Cancer Aversion
For the lion's share of lung cancer instances, preemptive strategies are attainable through the embrace of abstention from smoking and the meticulous avoidance of secondhand smoke exposure. Those who choose to relinquish their tobacco habit bear witness to a precipitous decline in their susceptibility to lung cancer, with their risk profile mirroring that of individuals who have never indulged in the act of smoking. Concurrently, the adoption of prudence with regard to other risk factors, encompassing specific chemicals and compounds such as benzene and asbestos, alongside the conscientious curtailment of atmospheric contamination exposure, affords a panoply of avenues for the prevention of lung cancer in targeted subsets of the populace.
#Lung cancer#Early signs#Symptoms#Stages#Diagnosis#Treatment options#Risk factors#Prevention#awareness#Survival rates
0 notes
Link
#survival#malignant mesothelioma#PULMONARY MALIGNANT#PULMONARY MALIGNANT MESOTHELIOMA#survival rates
0 notes
Text

fhsf just for fun ,
this is how i imagine it would be if sebek got transported to yuu's world via her coffin
#twisted wonderland#twst#twst yuu#twst mc#sebek zigvolt#fanart#but then how can return home#he shouldn't be that careless#he would go crazy living in yuu's world bcs mal mal is nonexistent#and he wouldn't fit into any job of this world#there should be like a survival on real life chart rating for every nrc students
1K notes
·
View notes
Photo




1 note
·
View note
Text
I wonder when the Noldor looked around at their dwindling numbers and realized that they were dying faster than they could ever keep up with.
#tolkien#silmarillion#I actually have a lot of feelings about this#because the noldor that come over from Valinor are pretty much all you get for the first age’s long war#birth rates are also in the basement if they exist at all#elves don’t have children during war#even if the siege of Angband is peaceful enough to relax that custom#I still don’t think you would have many children#elves have known war before - we know they did before the great journey#but it’s also got to be sobering to realize that your casualty rates are literally unsustainable#(like so#the house of finwë probably isn’t a representative sample of casualty rates#but damn the big picture still can’t be good#we have one grandchild of finwë who survives to the second age out of fifteen and that’s a very very bad rate)#what does that DO to a people group#to go from immortal and undying#to accepting that your whole clan is getting whittled down chunk by chunk#when did they start realizing that even if they beat Morgoth#they wouldn’t recognize the survivors
298 notes
·
View notes
Text
DC does not age Tim Drake because they fear he would not survive Twink Death™️
#Tim needs a loop around like Jason#white boys just have lower survival ratings and that’s sad for my boy#tim drake#red robin#robin#dc#dc comics#batfam#batman
229 notes
·
View notes
Text

in which the metaverse is a dangerous place
#my art#persona 5#goro akechi#joker p5#p5 spoilers#p5r spoilers#i was going to draw a partial background but i couldnt quickly find a ref for 3rdsempalace saferoom. lol#wasnt going to turn on my playstation or search thru a playthru so lazier version for u👍#i never draw blask with the mask or helmet on for a reason and that reason is hes goofy as fuck lol. this outfit man <-said with love#i drew his arm belt too high but whatever. is it better or worse that he didnt design the fit it just came from his psyche#anyway how did he survive in the metaverse for 3 years without healing skills. items only challenge.#(lavaeteinn costs 25% hp) (less relevantly it also has a godawful crit rate :/)#i had to revise his dialogue like 5 times to make him more of an asshole.i love him btw he sucks so bad#oh yeah. finally: robin hood is traced. i only drew him once for that animatic and that was enough. <3#anyway fuck school.shoutout persona five#comics
491 notes
·
View notes
Text
watching ajtl is like being told that you will be kicked down the stairs of a 500 story building, accepting that you will be kicked down the stairs of a 500 story building, then getting kicked down the stairs of a 500 story building, screaming crying and throwing up while tumbling all the way down, and finally arriving at the bottom to get a pat on the shoulder and a bandaid that says "congratulations for surviving" 😊
#a journey to love#一念关山#unpopular opinion maybe but actually the ending wasn't that bad since the narrative was doomed from the beginning. i cried a lot but i had#a good agonizing time. i only wish we had a special ep to show us yizhou with their kids & explain how tf they survived their BRUTAL deaths#also i will not lie i needed more of ltg and yy#show me their 10 year timeskip selves!!#all in all its a great drama that i recommend!! i rated it 8.5/10 and i havent rated a drama in a while so that says a lot#i miss my ruyi already... ill see if i can finish that fic im working on for her
79 notes
·
View notes
Photo


Creature of steel... watch how much ethanol I can drink
#Ultrakill#Minos Prime#MinosPhrime#Bacteriophage inspired fanart wasn't on my 2023 bingo but whatever#I also know ethanol isn't red but. Let him drink it like a fine wine#I don't even have twitter nor do I ever want to have twitter I'm just Fascinated by MinosPhrime's survival rate#Like it was found in mulch and yet has resistance to the phage equivalent of Instant Death Poison. What the fuck.#If anyone has twt feel free to tell them I say hi I guess#Cw:#Alcohol#Body horror#I was going to tag this shitpost but I spent too much time on it so#Hrokkall Art
351 notes
·
View notes
Text
I’ve always loved medicine bc it’s the perfect intersection of science and humanity—the two things I value above all else in this world. Truly adored it since I was in the cradle. But now I’m thinking about how so much of my journey to neurosurgery will have to involve KILLING my feelings essentially bc how do you survive otherwise
#Not to mention the surprisingly high suicide rate of surgeons that’s been brought to my attention lately#Honestly I just started my neuro internship and just saw my first patient in clinic#And on the day I did I was critical of my neurologist for being so robotic about it#Now I can see why#I’m still at a point where I can’t even do a chart review for a patient without feeling so fucking sad#And I can see how that can get unsustainable after a while#But it’s like if I kill the feelings that drive my passion for medicine to begin with then what’s the point#It’s not like I’m in it for the money or prestige bc that’s so dumb considering how long the schooling is#But literally how to deal#My supervisors at the clinic very much all speak about the dementia patients w a learned impartialness#But I don’t wanna be that way one day :( but how to be anything else and still survive#I’m pre med so I still have time and maybe my opinion will change and I’ll wanna do another specialty#But when it comes to this every specialty will involve human lives and navigating that regardless#That said I can see why surgeons are at higher risk or depression suicide etc#The whole point of this internship is to teach myself how to navigate this stuff but. Hate it#p#med tag
53 notes
·
View notes
Note
How had ryukitann got together? 🤔
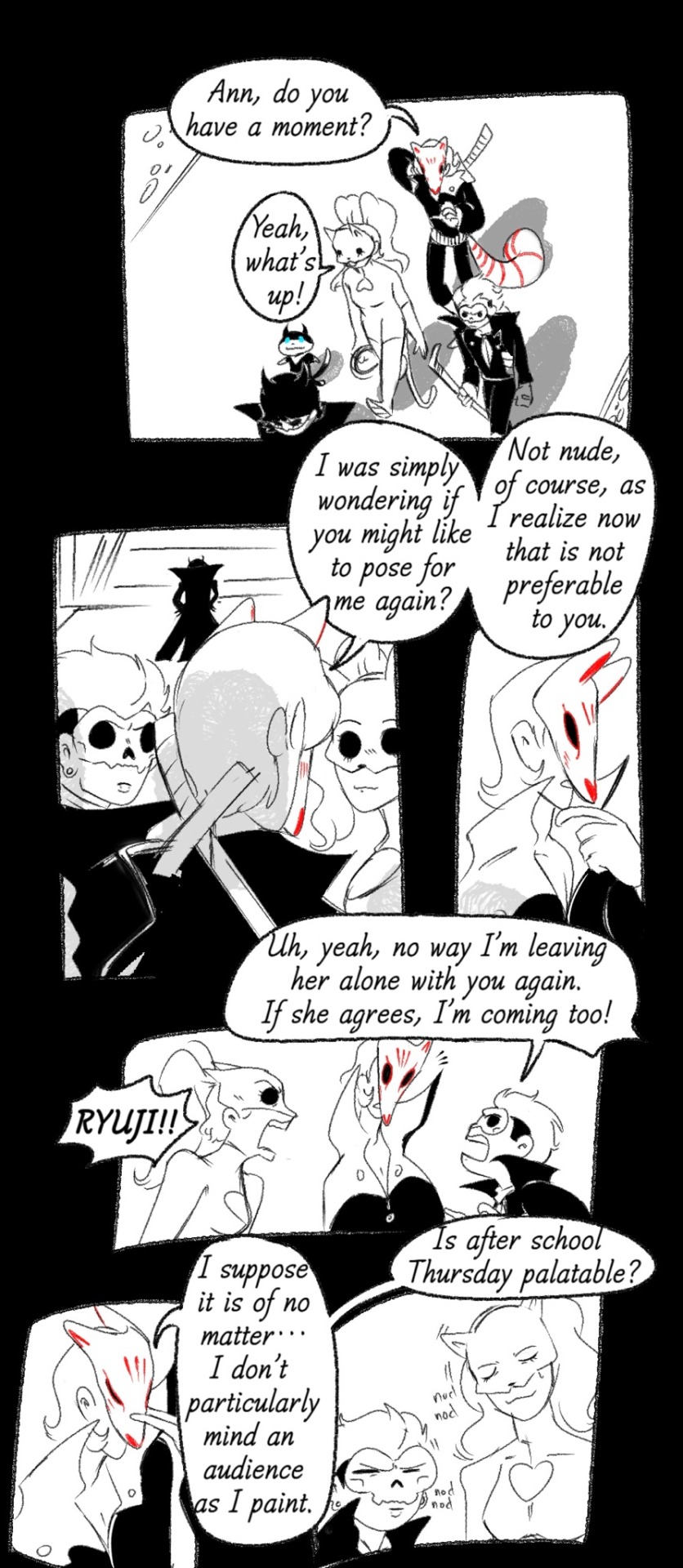




sorry this is a little rushed, but in general i think this is the gist of how they’d get together
#persona 5#ryuji sakamoto#yusuke kitagawa#ann takamaki#ryuann#ryukita#annkita#ryuannkita#PS SORRY IF IT SEEMS LIKE I POSTED TWICE. TUMBLR REALLY WOULD NOT LET ME INTO MY QUEUE I PROMISE#I remember trying to write fic for them and gave up#there are no non-E rated fics for these guys and that is so depressing man#I hold this ship so very close to my heart fr#it’s the only one that’s really survived from my first playthrough of p5#bc before I was into Shu///ake I was huge on Shu///yuu and polythieves in general#then I kinda settled into what I like now as I got more into the fandom#aNYWAY THO THANK U FOR THE ASK#my brainworms are progressing#I can see some people thinking ryuji is problematic here and. yes<3#I didnt have time or space really to like. make a bigger fallout before everything is resolved#so obviously intruding upon dates is not healthy but let’s just ignore that for my boi ryuji#long post#ask
381 notes
·
View notes
Note
Hey! How are you? If you don’t mind, I would like a trick!!
Hello there! Here is your post-Halloween trick, rated M.
Wet Wet Wet
Who thought this was a good idea? Draco vaguely remembered Potter grumbling about the cold. He looked so infuriatingly good in Draco’s borrowed hat and scarf, and the rest of the day was slightly fuzzy—Pansy was probably the one who offered the estate, and someone was weak enough to say yes.
Oh, no, that was probably him. Why did he have to mention the heated pool? Why, why, could he never keep his mouth shut. Now he had a practically-naked Potter a few laps away, laughing (did he always—with that laughter, the one that made Draco’s knees turn liquid), with his wet bloody eyelashes and his chest and his arms and his. His. Draco closed his eyes and could still see it.
“Darling,” Blaise said at his side. “Chin up. You don’t have to look so miserable.”
“Noted, thank you.”
A huff more exasperated than Draco deserved. “Just go in the water, silly. It’s really so nice.”
“Will you just—” Potter gave a particularly loud guffaw, and there was no way Blaise missed Draco’s flinch. The way his hands kept twitching at his sides. The next sigh was a good bit gentler.
“Draco,” he paused, shook his head. “Hey, Potter!”
Everything froze still. From between his teeth, “Blaise.”
“Yeah?” twisting towards him in an impossibly elegant motion, coming to rest his perfect chin on the pool’s edge.
Draco couldn’t breathe. “Blaise.”
“Did you know Draco can’t swim?”
“No chance,” Potter grinned, lifting his perfect eyes to where Draco was dying. “Is that true?”
Words failed him. “I,” he said, stupidly. Begging: “Blaise.”
“Too true. I heard he was so scared to go in the water as a child—(“Blaise!”)—that he tried to drown his instructor in the practice tub.”
Potter, amazingly, magnificently, laughed. “That’s definitely a lie.”
“Aw, you have such faith in him, do you?”
He pulled a little further out of the water, so his (wet, glistening, perfect) torso was leaning on the edge, and his face was close to Draco’s knee. “All I’m saying is, if Draco wanted out of swim lessons, he’d devise a much more nefarious plan than the practice tub.”
Yes, yes, nefarious and, ah, a bead of water running down Potter’s neck stole his entire presence of mind. Tongue darting out to lick—get a hold of yourself, Malfoy. Draco’s breathing was loud enough to startle him. He couldn’t remember what they were talking about.
“All yours,” Blaise was saying in the periphery, and Potter’s eyes were so bright. “Coming, Weasley? I promised to show you the wine cellar.”
“Perfect, mate,” Weasley hopped out, sopping wet and shaking himself wet-dogged-ly on the floor. Draco would normally mind, but Potter was looking at him. “Don’t let the little snake drown you, eh, Harry?”
Potter rolled his eyes, and his hand was—oh. He was offering it to, to Draco. Draco… wasn’t entirely sure he was conscious anymore.
The sound of their leaving was wet and inconsequential. Potter laughed, waving his hand in front of Draco’s face. “Well?” and Draco, ah, would probably go anywhere he’d, ah, direct, and found himself on his feet and preparing to jump before he remembered he was still fully clothed.
Torpedo-ing out of the jumper, the shirt, the jeans, till he was hopefully only in swim shorts, jumping so fast with his heart thundering in his chest: and Potter cheered, swimming around him in circles, shark-y and gorgeous and perfect, perfect.
“Well,” he was saying, “I suppose if you really can’t swim, then I’ll have to teach you from the beginning.” Drifting behind him to hold Draco’s shoulders, one arm snaking around his belly.
He’d been swimming since he was four, had even gone on a few competitions.
“Yes,” Draco choked out. “From the beginning.”
Potter fitted their hips together, his—oh god, oh god, semi-hard cock in the cleft of Draco’s arse. “Okay,” he said, so serious all of a sudden, skimming gently fingers on Draco’s jumping muscles. “All right. So, slowly, yeah? What do you, er, want to…”
Anything you want, Draco thought. “Anything you want,” was what he actually said. Potter made a low sound, crushed them even closer together. “Yes,” Draco said, and leaned his head back on Potter shoulder.
“Slowly,” Potter said, an order this time, and Draco shivered, nodded. Potter rewarded him with a tiny kiss to the place between his neck and his shoulder. His hand kept sneaking lower to the very-noticeable tenting in Draco’s shorts. “Slowly,” again, soft in his ear when Draco squirmed, gave this half-yelp, half-curse.
Leading them back until Potter was leaning against the wall. “Fuck,” he whispered, warm and ticklish just behind Draco’s ear, and when Draco jumped he laughed.
“Better than your old swimming instructor, hmm?”
Did other people still exist? “Yes,” Draco breathed, melting into his hand. His reward this time was a stroke, and every hair on his body rose.
This was a terrible idea—a brilliant one. Potter held him and Draco was seeing actual stars. The estate had more than just a heated pool—in fact, his old room should still be prepped. Maybe he could take Potter there and… ah. His toes curled with blistering, agonising pleasure.
“Potter,” Draco moaned, and stopped thinking altogether.

#Robin's trick or treat#drarry fic#muggle AU#rated M#nefarious and smitten draco#hot and wet harry#spoiler: no one drowns but one boy sure feels like he has#877 words#rockingrobin69#i'm surviving anon how are you??
77 notes
·
View notes
Text
Candela Obscura spinoff minigame called Fancy Man Does Arson in which you are a Fancy Man and the other player is The Obstacle and through d6-based Rollies you either do or do not do arson
#the fancy men who did arson are: howard margrove; nathaniel trapp; rajan savarimuthu; and malcolm trills#two professors and two military officers estranged from their wealthy families. someone let khary payton know it's his turn next#(they have a 50% survival rate thus far)#candela obscura#candela spoilers#cr spoilers
30 notes
·
View notes
Text

4 dancers party be like
253 notes
·
View notes
Last Seen Blogs

tachibanamomona
たちばなももな
acedefective7
Defective Detective

willie1990
Untitled

shash273
My Own Happily Ever After

valuepress
valuepress最新リリース