#and then proceeded to talk for an hour about how I might be self diagnosing or just be lazy
Text
We are talking about what we learn through the internet (by ourselves). How can I say that I either just vibe in dead fandoms or learn about ADHD which there is about a 99% chance that I have?
#I am not self diagnosing#I always had these stuff I just didn’t know the name#I kinda thought that everyone had that#just dealt better with it than me#I talked with my dad about it#turned out that he and almost his entire side of the family have adhd and other stuff#and that he always thought that I had it#wish he said anything#instead of letting me put down myself all the time whenever I forget something#or fail to do a simple task#I talked to my mom about it#I might get a therapist to check ifficially so yay#but she was mad about the fact that I didn’t tell her sooner#and then proceeded to talk for an hour about how I might be self diagnosing or just be lazy#also about how my dad doesn’t have adhd only add#although I am pretty sure that he knows what he has#it’s his brain after all#adhd#add#therapist#fucking finally getting some help
7 notes
·
View notes
Text
Murderous Love Chapter I
(WARNING: This fanfiction has themes of Suicidal Ideation, Suicide itself, Self harm, Sexual Assualt, Murder, Extreme Bullying and Humiliation and a lot of Mental Illness related content and is NOT appropriate for children and the faint of heart. If you are under 18 or may be triggered by the content of this fanfiction please do not read this.)
Mitsuhide’s POV
I was at school waiting for Motochika to arrive. I heard the main school bully Loki talking with his friend that he would normally bring with him to bully others Ares about me, I teared up thinking about what they could be saying.
I have recently been diagnosed with depression and bipolar disorder thanks to the trauma from the bullying and being sexually assaulted by a grown woman as a child. They’re probably planning on doing something to trigger me for their own entertainment.
Before they could walk to me to torment me Motochika, my best friend and crush had arrived and hugged me from behind.
“How was your weekend Mitsuhide?” he asked, I blushed saying.
“It was good, Gracia dragged me out for ice cream with her best friend Ranmaru since they couldn’t spend time with their partners as Koshosho was working and Nobunaga was away on a family camping trip. I wanted to stay home and read…”
Motochika laughed “Afterschool we had an appointment with a psychic medium. I want to know who I was in my previous life, and yes you’re coming with, I have a feeling that in our past lives we were either very close family or lovers and I want to know if that is the case.” He spoke.
I blushed saying “Is it a bad thing that I hope that it turns out that we were lovers in our past lives?”
Motochika laughed a bit but before he could say anything Ares punched Motochika while I was dragged away from him by Loki, I screamed out for Motochika or someone to help but everyone turned a blind eye and Ares restrained Motochika and he couldn’t get the male to let go, Loki called out.
“Bring the emo! He needs to watch!”
Ares Laughed and both myself and Motochika were dragged to a bathroom that no one would use anymore as it was believed to be haunted.
We saw Da Ji waiting in the bathroom smirking, I shivered with fear, scared that I’ll be forced to relive my past when an older woman sexually assaulted me.
Loki ordered Ares to tie Motochika to the post that holds the paper towel holder. Loki smirked holding up a key and asked Da Ji.
“Let me know if you need some privacy!”
Da Ji grabbed my arm before I could even get the chance to free Motochika so that he could run and get someone to help us. I tried to escape her grip, but I heard her say something and a door slam and lock.
Motochika and I was trapped with this senior.
Da Ji removed her clothes while I tried to free Motochika before she grabbed me and removed my clothes slapping me when I screamed. Motochika tried to break free from the restraints as Da Ji had her way with me. I was screaming for her to stop but it was no use.
It has been half an hour and Da Ji reached her climax. I was laying on the floor at this point, having lost the will to fight her off. I looked at Motochika who was crying as he tried to break free from the restraints.
Da Ji grabbed her phone and took a picture of me. I called out to her.
“Delete that.”
Da Ji jeered at me “Demand anything and you’ll be forced to go round two!”
I whimpered as she was typing on her phone after she was finished, she smirked.
“We’re going to stay here! You don’t get to go to class for the whole day!”
I cried, I crawled towards my pants grabbing my phone and sent a text to my sister Gracia asking her for help and it sent my exact location. Before Da Ji could notice that I was sending messages for help I hid my phone in my pant pockets.
I then crawled towards the sink basin to get a drink of water because I was thirsty, but Da Ji dragged me away from the basin. I cried “Please… I need a drink of water, I’m thirsty!”
Da Ji laughed before we heard the door unlock and Loki opening the door “Hey Da Ji, your friend Himiko wants to spend the day with you. Don’t worry about these freaks, you probably exhausted the living hell out of the man-whore and his best friend is tied up so they wouldn’t be thinking about escape any time soon.”
Da Ji left and the door was shut and locked. I instantly took this opportunity to break Motochika free from his restraints, when I managed to break Motochika free he hugged me tightly.
“I swear when I see those basterds they’re fucking dead!”
He then grabbed some toilet paper and got me to wipe myself he then had me wash myself then he helped me get dressed as I was still slightly weak from earlier.
When I was fully dressed, we sat in the corner of the room and Motochika cuddled me tightly.
Three hours passed and we heard the door unlocked. Motochika got ready to kill only to calm down when the person who entered the room was a locksmith, my sister Gracia, my favourite teacher Hades, and the principal Gaia.
Hades noticed what happened and looked at Motochika “hey, it’s okay, I won’t hurt you."
“I have little concern for myself, I’m more worried about Mitsuhide!” Motochika replied.
I held the tissue that I had to wipe myself with asking “is there any zip lock bags I can put this in. Also, you might want to call the police...”
Hades shook with rage. Not only was Hades a teacher but he was also the school chaplain.
He looked at Gaia saying “I want these two in my office without any interference from the other students. And I want the police called. I have suspicions that something has happened and whoever the fuck did this isn’t finished yet.”
Gaia nodded and took Gracia to her office. Probably to nominate her for the school bravery award for getting help for me while Hades lead me and Motochika to his office refusing to let anyone near us.
When we were in Hades office, he looked at me saying “are you able to go into the kitchen and make yourself a coffee? I’ll be asking Motochika what happened as I do not wish to traumatise you further than you already are.”
I nodded and went to the staff kitchen and made myself, Hades and Motochika a hot drink. I heard what Motochika said to Hades about what happened this morning and I could hear Hades typing away at his laptop.
When I came back with a tray holding the hot drinks, I set the drinks down and sat next to Motochika and hugged him tightly. I said, “I feel more fearless against the things that traumatise me when Motochika is here.”
Hades nodded and handed me Motochika’s statement that he had printed out asking me to confirm it. I read it and this was what was written.
‘This occurred about five minutes after I arrived at school at 8:45am and met up with Mitsuhide and we were talking about our plans for when the school day ends. Loki and Ares then attacked us, restrained the both of us and took us to the bathroom in which Hades, Principal Gaia and Mitsuhide’s sister Gracia found us in.
I was then tied to a pole that used to hold the paper towel dispenser by Ares before myself and Mitsuhide was locked into the bathroom with Da Ji, who proceeded to sexually assault Mitsuhide while I was forced to watch.
I tried to break free from the bonds that kept me tied to the pole while this was going on. Mitsuhide tried to fight Da Ji off and get her to stop as he didn’t give consent and it’s forcing him to relive a horrible memory of his childhood, but Da Ji kept going, when she was finished Mitsuhide had no energy left.
She took a photo of Mitsuhide nude and threatened to sexually assault him again if he demanded that she delete the photo.
Mitsuhide snuck a text to his sister calling for help before trying to get a drink of water. Da Ji dragged him away and laughed when Mitsuhide pleaded her to let him get a drink of water.
Loki unlocked the door only to get Da Ji out of there because her best friend Himiko wanted to spend the school day with Da Ji.
When there was no one near or in the room Mitsuhide used the last of his mental strength at the time to free me and I helped him get cleaned up before holding him tightly stating that I will have my revenge.’
I looked at Hades and handed the paper back saying, “That’s correct, I want to put my own statement in as well, that way if the police want a statement from me, you’re prepared.”
Hades nodded, opened a new word document on his laptop and I gave my statement, including the horrible things that Loki and Ares were saying about me.
When I was finished Hades Printed my statement out, got me and Motochika to sign our statements stating that what Hades has written on those documents were true and Hades hasn’t made us say anything and merely typed them up so that there is a paper trail for the police.
Motochika heard his phone, so he checked it. It was a message from Magoichi one of his friends, I peered at the message out of curiosity and shook with fear when I read the message that said.
‘Hey Motochika? Is the picture Da Ji posted on Instagram of Mitsuhide? I reported it just in case it is and took a screenshot of the post just in case you need it.’
Motochika called Magoichi and put him on video chat, Hades was a bit confused by this before Magoichi said.
“SOOO I was checking my Instagram and I saw a naked picture of a feminine looking guy with long black hair looking rather distressed posted by Da Ji, I took a screenshot of the post and reported it to Instagram, is the guy in the picture Mitsuhide!? If it, is I’m forwarding it to the fucking police!”
I curled into a ball after letting go of Motochika and cried Motochika looked at his phone saying, “I think the background noise coming from my end is the answer, can you please send me an email with that screenshot so I can print it and give it as evidence?”
Magoichi nodded “Sure! I just did as soon as you confirmed who it was. I can’t believe Da Ji would do that sort of shit!”
Motochika looked at Hades saying “Can I connect my phone to your printer and print out a screenshot one of my friends made of an Instagram post? I want Da Ji to be charged with child pornography, but I don’t want to put your job at risk.”
Hades nodded and Motochika printed the screenshot as well as a statement requesting that Magoichi is not to be charged as he was helping with the apprehension of the person who posted it. By the time we had all the paperwork and the tissue with mine and Da Ji’s DNA on it in a zip lock bag the police arrived and took them.
One of the male officers looked at me saying “I’ll protect you from those people who ask those horrible questions to try to indicate that you liked it.”
I looked at the officer smiling “Thank you.”
Motochika and I were then sent home. Motochika’s father wanted him to stay with me for as long as I needed and transferred some money to my father’s bank account so that my father can pay for the utilities and food that Motochika would use.
By the time we were home the psychic medium arrived at my house as well, myself, Motochika and the Psychic Medium went to my bedroom, and we began our appointment with them.
We did everything the Psychic Medium needed us to do in order to find out who we were in our past lives and then as if in a trance the psychic started writing something down.
I was curious but I had to stay calm while this was happening. It took the medium about an hour to finish writing and they gave us each a piece of paper detailing our past lives.
Motochika paid the money and the psychic medium left.
I looked at mine only to find that I was a castle maid to a Samurai Clan who fell in love with a Lady Samurai and had a lesbian relationship with said Samurai. I blushed before Motochika smirked.
“Turns out we were lovers in our past lives. You were the maid who wanted to become a medic for the soldiers while I was the Samurai who was going to be married off to the clan head’s son. And both the Samurai and the maiden were in love with each other.”
I hugged Motochika tightly “I’m so glad.”
I was madly in love with Motochika.
“I love you” I whispered, Motochika hugged back just as tightly saying.
“I love you too. I had developed feelings for you for a while. You’re a broken soul who needs someone to love them and fix them with gold to make the cracks stand out” I teared up as I heard this.
My father Mitsutsuna walked into my room and noticed us in the position we were in and awed at it.
“That’s adorable, Motochika, look after my son, my wife is very protective of him.” He spoke.
I was shocked as I looked at my father who said, “I would only not approve if I didn’t know the young man well enough, but since his father and I were high school friends, I have known him since he was born so I approve of your relationship with him.”
I blushed as my father left to make dinner. I looked at Motochika before hugging him feeling his warmth against my body.
1 note
·
View note
Text
I want to share my life story. It would mean the world to me if you read this all the way through. ♥
Dear friends,
Some people have been asking if I’m returning to tumblr and well... not exactly.
I’m actually considering deleting my tumblr. I’ve definitely moved on and realized that tumblr only worsened my depression and kept me locked up in a world on a laptop. And yes, I made amazing friends on here who helped me through some hard times. However, they’ve all changed usernames and I can’t even find them. The insane amount of hours I’ve spent on this website scares me. I left tumblr about a year ago kind of suddenly and I want everyone to know that I’m okay, maybe even better than okay. It’s been a long, hard road with medical issues and anxiety and although tumblr was an escape for a while, it left me more and more broken.
To those who have been on tumblr for years like I have, with friends and a well-established blog, this website is not where you’ll find happiness. This might sound controversial, but hear me out. Staying locked in your room away from your family and real-life friends is not healthy. Human connection is what we long for, and it can’t be found behind a computer screen.
During Junior High, I found tumblr and bad friends who led me down a path of destruction. Tumblr led me into having a bad swearing problem, which I completely regret and still struggle with. Looking back on this website, I see a waste of time and a dark phase of my life. There is so much more to life then spending hours of your life photoshopping Captain America for a blog.
If you’re depressed or suicidal relying on tumblr, I understand. If you’ve read this far I want you to keep reading, and I want to explain everything to my followers on here. Why I created this blog in 2014, what I struggled with, and I want to give you hope of how far I’ve come in my life. From almost committing suicide, I’m currently someone who has a life-threatening lung disease but has found complete joy and peace after YEARS of depression, anxiety and panic attacks. And the truth is, you can find joy and peace and love too. Please keep reading, and I pray my story of hope will encourage you. I’m terrified to post this on the internet, but if it helps one person, it’s worth it.
This is my story.
In 2014, I was in eighth grade. Like most Junior Highers, I had low self-esteem which leads to depression, suicidal thoughts, and self-harm. This is around the time I created my tumblr. Staying up on tumblr until 3 am, I talked to strangers about my deepest darkest fears. How I felt bullied on my cheer team for not feeling skinny enough or good enough at the stunts. How my mother had become an alcoholic and now I was the adult in the household. My dad worked out of town, and I was stuck dealing with it. Being called a bitch by my mother. Walking out in the morning to see a half drunk wine glass and knowing she got wasted last night, not caring how much it hurt me. To see someone I used to respect turn to a completely different person. I still believe my mother has a bipolar personality issue but she still refuses professional help. Basically, Junior High is when everything changed and an innocent, Jesus-loving 6th grader turned into someone I look back to and see a monster. I’m scared of who I became. I was friends with people who were also lost, suicidal, and obsessed with fictional characters.
When high school started, I thought everything would be better. I’d make new friends, and things would just be perfect; high school is supposed to be the best 4 years of your life, right? Boy, was I wrong.
Yes, I started making new friends but I still had my insecurities. New people had come into my class who were prettier than me, smarter than me, and better artists. My self-esteem weakened even more, and I clung to tumblr as a “happy place.” I reached a 2,000 follower goal, was winning awards, starting my own networks, and I felt “cool” here, as a faceless blogger who could spill my problems to strangers who assured me “everything would be okay.”
Yet something happened my Freshmen year that caused me to lose my faith in humanity even more. The Tuesday after Thanksgiving break, I remember both my parents coming into my room, my mom crying and my dad looking like he was about to. I had just sat down on the floor with my backpack, pulling out my science book for homework. But I stopped in my tracks thinking, “What did I do? What did I do that would make my mom cry? Did they find my tumblr?”
It was much worse. My mom sat on my bed and said, “Molly’s been murdered.”
Molly was my nineteen-year-old cousin who lived in LA (Los Angeles) and had started with weed then graduated to cocaine and meth. My aunt tried everything. Expensive rehab in Missouri multiple times, but nothing worked. She ran away from home and started living on friends’ couches, only caring about the next high. This is someone I grew up with, who I watched choose the wrong path. That path of drugs led to her being shot in the head without motive. She was in a garage of about 12 people, sitting on a couch and chilling and someone she knew pulled out a 9mm and shot her in the head. He proceeded to put her in a trunk of a car and leave her there, the day before Thanksgiving (I believe. I might have the dates wrong. This whole period of my life is a blur). The cops only found her body because someone called in an abandoned car notice. The detectives showed up at my aunts house at 2 am that Tuesday and gave the news.
A week before I had spent Thanksgiving with my aunt and uncle and my uncle had sent a message to Molly on Thanksgiving day on Facebook, saying how much we loved her and wanted her to come home.
She was already dead when he sent the message.
We expected something to happen to her, maybe an OD. But never this. My cousin’s murder broke a piece of my heart that will always stay broken. I’ll never understand why people could murder someone. (The investigation has been finished and they determined it was a homicide.) I could barely make it through a school day after that without crying. I lost what little faith in God I had left. (I go to a Christian school, grew up in the church, and was expected to be the angel child.) But after Molly’s murder, I changed.
My cussing problem got worse, and cutting myself. I have stretch marks on my thighs, so I would cut there so no one would notice the scars. And to this day, no one has.
I struggled with my emotions over the next couple months of Freshmen year, even writing an essay about Molly for one of my English assignments. In her memory, I want to tell you people to never do drugs whether they’re legal or not. Weed is a gateway drug to crystal meth and cocaine, and then getting shot in the head and thrown into the back of a car. It ruins your body and your life. My cousin grew up in a Catholic church but lost her way trying to fit in at high school and finding “friends” who gave her drugs to be “cool”. Drugs are not cool, and lead to destruction and pain and digging a hole that’s really hard to climb out of.
But I started to move on and accept what had happened. I still miss her, and wish I could talk with her one last time.
A few months later, good news came in January.
A little background info: I was born with heart issues and had my first surgery at 4 days old and open heart surgery at 3. I have huge surgery scars, but other than that you would’ve thought I was a normal kid growing up... except I could never play sports. I love love love love soccer, but my cardiologist never let me play competitively. However, when Freshmen spring soccer sign ups came around I was brave enough to ask, “Can I play?”
After a thorough check-up, he said yes.
I was OVERJOYED. This was something I never believed would happen and I was so excited to buy cleats and shin guards and get on the field and be an awesome defender.
Until my first practice.
I realized I couldn’t run. Not even one lap around the track. To this day, I’ve never run a mile. This amazing girl on my team named Emily (sweetest girl I’ve ever met) came up beside me and tried to help me learn to run. But I couldn’t breathe. I was out of breath almost instantly. I blamed my heart issues but as soccer season went on, I realized it was more than that.
I got a little playing time but I was mainly a bench warmer. I didn’t really mind. I loved the practices and pushing my body, even if I couldn’t do as much as everyone else. Some of the older girls bullied me in a way that they would scream at me whenever I did something wrong. And though I don’t use this word often, there was this one Senior who was a bitch. Even at our good Christian school. Don’t get me wrong, I’m not bad-mouthing my school. It is filled with Jesus-loving people who inspire me every day, but this one chick... she needed some Jesus. A lot of the time after practices I would hold in my emotions then start crying in the car as soon as my mom picked me up. I wanted to prove to everyone I WAS strong and good at sports and it wasn’t my fault I could breathe.
Easter break we ended up going back to the cardiologists to talk about my issues in soccer. And so, he performed an echocardiogram, (which is similar to the sonogram they do for pregnancies, but for your heart) which is normal. But then he came back and did it again and again and again. About the fourth time, my mom and I looked at each other and said, “Something’s wrong.”
That day I was diagnosed with pulmonary arterial hypertension.
My life will never be the same.
In short, pulmonary arterial hypertension (PaH) is a lung disease with high pressure in the arteries around your heart. Normally when you exercise your arteries expand to let the blood flow easier from the heart and lungs. Mine don’t expand and the pressures grow on the right side of the heart which could lead to heart failure. It feels like asthma but it was way more serious. I was just fifteen, and being told I was going to die before 30.
My emotional state was shattered. I went to specialists in San Francisco and they started medication that made me feel like sh*t. I got headaches so bad I couldn’t move, and I was nauseous for hours at night but was never able to throw up. There were a lot of nights I slept on the bathroom floor. And I usually kept my issues to myself, bottling my emotions about my disease. Did I mention I started said medications a week before my first high school finals? Somehow I persevered and got all A’s on my finals. But through all this, I got angrier at God. I relied on friends, tumblr and fanfiction and TV shows for happiness. And they failed me.
I got more and more depressed, thinking and wondering how could anyone love a faliure like me? A loser who couldn’t even breathe right. I had always been a good student but with the medications Sophomore year was a nightmare. Everything was being taken away from me: my health, my body, my mind. And I couldn’t help crying out, “God, why me?”
Right before Sophomore year, I was faced with starting a new medication. One form of it was administered in a pump similar to a diabetic pump, except you keep it on 24/7. Showering would be a pain, and I couldn’t go swimming. I refused to try it. I didn’t care how bad my disease was. I was terrified of having something attached to me.
The second option was these trial pills. I would take them three times a day, 7, 3, and 10:30. So, in August 2016, I started these meds.
The side effects were horrible and torturous.
I was constantly nauseous and flushed, and could barely make it through a school day. I don’t even remember much of Sophomore year. I think my brain blocks it out. My anxiety got worse and worse and I begged my parents for a dog, a friend to help with the stress.
Like I said, I don’t remember much of Sophomore year, except for some happy parts like going to country concerts and being a cheer captain. I had an amazing “squad” of friends who stuck by me no matter what and still surprise me with Starbucks on my doorstep on bad days.
Six months passed, and we headed back to the San Francisco specialists to find out if my medications were working and if all the pain and misery and torture of the last couple months was worth it.
I had a heart cath, (which is where they put a camera through an artery in your thigh and send it to the heart to read the pressures in your lungs), and awaited the news.
Things had gotten worse.
The medication wasn’t working.
For a third time in a year, I was shattered. Would things ever get better for me? To top it off, this meant I needed to start the pump medication.
I remember asking my dad to take a friend and I to go swimming at a nearby lake. My friend actually has no idea, but that was the last time I’ve gone swimming or worn a bikini up to this day.
July 2017 I said goodbye to the life I’d known, and was admitted to the hospital for a week to be transferred to the pump. When they place the site (where the medicine is administered through a little tiny needle thing) it’s extremely painful. With my pump, you don’t change the site every 3 days like a diabetic pump. You change it when the site goes bad and you put a new one in, which gets super painful and swollen before it gets better. When I say painful, I mean I almost needed morphine once.
People always say “It’s God’s plan,” and “things will get better.” I wanted to punch those people in the face. Because I had been waiting for things to get better for a long time, and things always got worse.
Plus, for the shower I need to take them quick and cover up my site with plastic, gauze and waterproof tape. I can’t go swimming or take a bath. During the day, I usually hide my pump in my bra or jean pocket.
Even so, before Junior year I had full on panic attacks about people knowing about my pump. I found ways to completely hide it but I was still so terrified of people finding out and judging me. I don’t know what they would do, but I was so scared of being different. Not fitting in. I had to be careful about what I wore, to make sure I could hide it completely. And only a few select people knew what was really going on. Even so, I think only one person really knew about how bad my depression was getting.
Some fun things did happen last August though. My dream of going to London was granted by Make-A-Wish! As an avid Sherlock and Harry Potter fan, I was ecstatic. I spent 10 days in the most beautiful city I’ve ever seen with my mom, dad, and my aunt. I think I took over 3,000 photos on the trip. It was one of the most amazing experiences I’ve ever been blessed to have. A limo came and picked me up at my house and we arrived at the airport to fly “across the pond” and into a dream. Make-A-Wish is such an incredible organization because they do dream trips and wishes, and while I was in London, I didn’t feel “sick.” I actually felt fantastic, walking 20,000 steps a day, way ahead of my parents. I went on Sherlock and Harry Potter tours, and I might make a separate post about this trip if people ask. But basically, it was seriously a dream come true.
When I got home, I actually ended up adopting a border collie named Blaze, who has become my best friend. I’m still training him to be my service dog and an emotional support animal for others. He is an absolute sweetheart. He’s helped my anxiety by an enormous amount.
Regardless, I still had my fears of starting Junior Year.
The dreaded day came and I started going back to school. It was better than I thought, and I was ahead in my classes. I was brave enough to take two APs and an Honors class. I was taking my math online, and everything was going surprisingly well. No one knew about the pump.
Then I had my first site change.
I missed a week of school and got terribly behind. A week doesn’t seem like much, but it really took a toll. I got really discouraged, as my depression was still suffocating me. I didn’t do things with friends and stayed holed up. Walking my dog in the fall mornings was my favorite thing. Blaze is still one of the centers of my life and is my little sunshine.
But I started failing AP tests, and I wanted to drop the hard classes. Suicidal thoughts crept into my mind, ripping what little happiness I had away. I was scared. Not of suicide itself, but of the fact I was so close to doing it. I was scared of myself. How much I’d lost control of my body and mind. But I was scared to leave Blaze behind. That was one of the few things that kept me holding on.
One day my AP Chem teacher pulled me aside and asked what’s wrong. I told him I was tired and the usual excuses. He was one of the few teachers who knew what was going on though, medically. He asked if I had prayed about it. I said God and I weren’t really on talking terms.
And it’s true. Through all the trials I’d gone through I started to hate God. I always saw hypocrisy in Christians I knew, and didn’t really know what a real relationship with God looked like, I just knew I didn’t want one.
It was the last week of Septemeber when I really broke. I had to leave early because I was feeling sick, again, and signed out to go home. But I was so done with feeling like sh*t and not being able to make it through a school day. On the drive home I lost it.
I was crying and was a complete mess. The whole drive home the only thing I could think of was driving my car off the road and into a tree and hoping it killed me.
Somehow, I made it home that day. And the next, and the next. I was just surviving at this point, not living. I was hopeless. I didn’t believe this medication would work because it didn’t last time. I tried to focus on school and redeem my grades, practically the last thing I had control of.
A few of my teachers also kept me from going off the deep end. I had failed two AP US History (APUSH) tests and my teacher pulled me aside and said, “You’re a better student than that.” He erased the tests and gave me a second chance. I started working my ass off in that class, and now I average 95 on his tests. But without that second chance, I would’ve quit and never proved to myself I could do it.
Said Chemistry teacher was also someone who kept me from not committing suicide. He’s a very inspiring person and an absolute science genius who had gone through a life and death experience like I was going through then and now. He ended up finding God through that experience and is still alive today, teaching and preaching to my AP class. He had written a book for his kids when they grew up because he thought he was going to die. His book talks about God in a C.S. Lewis sort of story. He gave me a copy and told me to read it.
So right after my mental breakdown of driving home and almost attempting suicide, I started reading.
Please know I was scared of death on a day to day basis. When you have a terminal condition, your mind is constantly set on “deep mode”, experiencing the kind of thoughts people usually think of at 3 am, but all the time. Becuase I knew I was going to die, but I thought I was going to hell because there’s no way I deserved heaven. But I started reading this book and well...
For a fantasy book, it talks about death a lot. (Like I said, my teacher/friend wrote this when he thought he was going to die.)
“...it’s our consciousness - our ability to know we are alive - that sets us apart from the rest of creation -- a creation largely blind to its own existence... Unfortunately, however, because we have the ability to think and experience life, we are also capable of anticipating our deaths - an uncomfortable conundrum to say the least.”
This is one example of how the book addresses death, and for a suicidal person, it’s a lot to swallow. But that’s not the part that caught me.
October 4th 2017, my life was changed.
Now, I know the Bible. I’ve grown up in the same Christian school for 12 years. But I’d never truly learned to put 100% faith and trust in the Creator of the Universe.
But there were a lot of things pointing me in that direction. Nudging me back into the safety of God’s arms. But Chapter 16 of my friend’s book was the final straw.
It reads...
“What I mean is that because we can think, we all know we’re going to die, and this fact in itself robs us of much of the joy and peace we would otherwise have if our fate had been kept from us. ... There is another option, however. ... We can choose to make the most difficult choice anyone can make. ... We can choose to trust the Creator.”
The night I read that, I got on my knees. I opened a very dusty Bible and found Jesus. I remember calling out and crying “I’m sorry” and “I’m sorry” over and over. I was someone who didn’t deserve a second chance after what I’ve done. I can’t magnify in words how far away I was from Christianity and how much I never thought I’d love God again.
But that night, I felt his unwavering, unfailing forgiveness. I asked for peace, and I was given peace for the first time. Complete and utter peace. It’s different than relief. It’s knowing that everything is in God’s hands and nothing I do can change his love. My anxiety and panic have left. I was redeemed through grace and blood poured out on the cross. Jesus had planted the tree that would become the cross. His love was stronger than my broken heart.
GOD TOOK EVERYTHING FROM ME SO HE COULD RESTORE MY SOUL FROM THE INSIDE OUT. I HAD NOTHING LEFT WHEN LOVE CAME DOWN AND RESCUED ME.
Since that day, I’ve woken up on my knees, thanking him for my pulmonary hypertension. God grabbed my stubborn self by the shoulders and shoved me to my knees. And I praise Him for that. I haven’t had suicidal thoughts since, and have barely looked back. My life has been completely turned around.
He’s shown me needs in my community and through His provision they’ve been fulfilled.
Some things that I’ve accomplished since coming back to God:
I was Junior Princess. (Something I never thought I’d win.)
I organized a clothes drive for victims of the Santa Rosa fire in Sonoma County. (They still need prayers!)
I’ve raised money for different needs in my community, with bake sales and BBQs.
I hiked Diamond Head in Oahu, Hawaii on Christmas Day 2017. Correction: I practically ran up it. Take that, PH.
I learned how to play the ukelele, and play it whenever I need a smile and want to praise my Savior with worship songs.
I’ve made new friends who encourage me in my walk with God, not take me away from Him.
And in January, I got some amazing news.
You know my pump medication? The one I thought wouldn’t work? I had a heart cath January 27th and they’ve never seen this medication work as well as it is for me. Another miracle I don’t deserve and will always praise God for. And I’m supposed to live way past thirty. And, my doctors think I’ll be able to do sports next year. :)
Basically, I want this story to inspire you to never, never, NEVER give up. What I’ve accomplished is through Jesus, not myself. I would be nothing without Him.
There’s been really hard days, and there will still be some for the rest of my life. But if I can save just one person by sharing my story of going from suicidal to joyful, everything I have suffered through will become worth it.
I’m planning to go to college, with God guiding me. Maybe starting a church or buying a house where I go to open up as a safe, Christian place for those who need it. I want to publish a devotional book before I graduate from high school. And God had blessed me with more years on this earth than I ever thought I would have. I wake up every day on my knees because I never expected another day. I never deserved another day, yet Jesus loves me enough to give me a life full of love and hope. I’ve dedicated my life to Him through complete trust, and every second seems more beautiful. To sprint as fast as I can, feeling like my lungs are on fire and praising God because I should never have been able to run or breathe. To watch the sunset bleed across an endless horizon to the sound of rustling palm trees and waves lapping the shore.
To believe that you’re going to die, then you don’t.
This world is not perfect, but it is the most beautiful place I have ever seen. And somehow, thinking I was going to die made it so much sweeter. I can sit at a stoplight, feel warm sunlight on my face through the windshield and be overwhelmed with inexpressible joy. My whole face breaks out with a smile, and the guy parked next to me probably thinks I’m insane. Some people look at the earth and say, “there's nothing good here, look at all this pain.”
Open your eyes. ♥
If you’ll allow me, I want to end with a verse.
“Therefore, having been justified by faith, we have peace with God through our Lord Jesus Christ, through whom also we have access by faith into this grace in which we stand, and rejoice in hope of the glory of God. And not only that, but we also glory in tribulations, knowing that tribulation produces perseverance; and perseverance, character; and character, hope. Now hope does not disappoint because the love of God had been poured in our hearts by the Holy Spirit who was given to us.” Romans 5:1-5
I will be keeping my tumblr up for a little while if you want to talk to me. I also really recommend this devotional about finding your way back to God. I love you all, and a special thank you to those on this website who were there for me when no one else was. If you reblog this, it would bless me so much. Thank you.
God bless you all.
Sincerely,
Kris
5 notes
·
View notes
Note
Sorry if this is an inappropriate ask. Please feel free to ignore in that case. What do you think of RFK's rumored affairs, including the horrible Monroe stuff? Personally, I think he was unfairly maligned, simply because he was the middle brother of JFK and Teddy, who were proven cheaters. Biographers like James Hilty or Larry Tye have argued that he was too much of a prude and too cautious to be a womanizer. Certainly no woman has ever come forward, unlike in JFK's case.
Hey there! Sorry for the delay in answering, but I basically wanted to educate myself more on the topic and then get back to you; it’s not gauche at all, especially if you consider it from a historical perspective, which I try to when undertaking a historical analysis of anybody, even with someone I might genuinely like.
I tend to agree. One of what is called the ‘definitive’ Robert Kennedy biography, “Robert Kennedy: His Life” by Evan Thomas, which I’m currently reading, is ridiculously detailed in this aspect, and provides a lot more perspective on RFK’s views of women, etc.
RFK, as opposed to JFK or Ted Kennedy, for all extensive purposes, was a feminist. He was famously a ‘mama’s boy’ as a child, mercilessly teased for it, and tried to compensate by being the family protector and as tough and controlling as his old man wanted him to be.
That being said, his father couldn’t beat out his natural sensitive sensibilities which became his defining trademark later in life once he got out from under his grasp (it took the debilitating stroke of his father, but he finally did it). He was forced to become his own man despite constantly supporting others, and it was the hints of this man that sort of informs my perspective of any rumours of infidelity.
1. This is a man who basically was horrified when his date opened her mouth when she was kissing him at twenty. The man didn’t know about French kissing until twenty, despite his two older brothers and his father being famous womanisers. A lot of people describe RFK as ‘lost in the shuffle,’ the only boy amongst a sea of girls until Teddy was born. We have to remember that despite being close later by circumstance, RFK and JFK were not bosom buddies growing up, and rarely spent time together unless with family, which is understandable, with almost a decade between them in ages. So I think any thought of JFK’s behaviour ‘rubbing off’ on RFK is sort of a moot point.
2. This is also a man who as a child Thomas hints could have been considered so sensitive that he became clinically depressed, just it was never diagnosed (To be fair, if you read how much even his own family considered him a failure, I couldn’t even imagine living through it. It’d drive you crazy). He famously would spend more time than the three times a week required in mass, and would stay there for at least three hours, praying and lingering, as if looking for some sort of shelter from the storm. He didn’t drink or smoke until he was twenty-one, and lost his virginity because his father paid someone to take him to a brothel. Reportedly, he said afterwards something akin to ‘Not bad, but not great either.’ This was obviously a kid for whom sexual activity or debauchery was not at the forefront of his psyche.
3. Because he wasn’t part of ‘The Golden Trio’ of his older, more social and stunning siblings, including JFK, he had to carve out a niche role for himself, despite pretty much being a C- student and failing at most stereotypically ‘Kennedy’ things he tried his hand at. That was the role of the protector of the family name for the good part of his life. I honestly think it speaks volumes that he said on the campaign trail that people could say whatever they wanted about him, as long as they liked JFK. We all know JFK was a notorious cheat, and the fact that RFK took that mantel on just goes to show how much this identity as the protector defined him. I don’t think honestly he’d risk that just to have a fling with a girl.
4. He was supremely Catholic. This tended to make him a Moralist, until proven otherwise. However, one of the things I think everyone loved most about his character was that if he was proven there was a grey area, he would admit his wrong and move on. That sounds simply nowadays, where politicians famously flip-flop on positions all the time, but this is different than flip flopping on positions; you could literally see him GROW as a person.
That being said, early in his life and in his career, he did tend to see women as this precious thing to be protected or sinful. There are stories where he literally fired a campaign worker for swearing in front of female staffers, at the same time saying women were the best workers because they just worked the hardest. He would have men walk female campaign workers to the subway to make sure they got home alright if he kept them late. I think later in life, the more ‘sinful’ women he knew, judging by his behaviour, he didn’t pain women as these two dichotomies, but the moralism of being brought up so strictly Catholic was the starting place from which this grew (Famously he married his wife Ethel, who almost considered becoming a nun).
5. Which brings me finally to your actual question, about the rumours about the affairs, in particular Marilyn Monroe.
To be honest, judging from what I outline earlier, that’s basically why I don’t think he really had an affair. Some border on the ridiculous (homosexual affairs)), to others which were more plausible (aka guilt by association being surrounded by the dozens of women JFK cheated with), but all don’t tend to take into account one important thing: Bobby.
Bobby, for all extensive purposes, was the opposite of his brothers. It was the only way he was able to find an identity within the family after years of trying to emulate them. Ted, being much more social and athletic, from what I understand, fell in line with the Kennedy men cheating pretty easily. But Bobby had to prove himself by being the OPPOSITE of what was expected. If they swerved right, he swerved left. It was the only way to distinguish himself in the eyes of his father. If Jack was flighty and rebellious, Bobby was stable and dependable. Everyone who knows him describes him as being almost TOO loyal. I honestly don’t think it’s in his character as the one black sheep in the family (They literally called him ‘Black Robert’) to cheat, especially considering the heavy influence Catholicism had in his life.
6. Which brings me to the Marilyn Monroe rumours. From all the research I saw, RFK only met/associated with Marilyn four times that can be proven: once, at a dinner party where they first met, which was quite sweet because the next day Marilyn wrote to her father and mentioned RFK by name, saying he had ‘the most wonderful sense of humour,’ which if you know anything about Bobby, is the most hilarious mental image ever. Marilyn, the epitome of glamour but sweet as a button, oohing over Bobby, who probably was just spewing self-deprecating black humour all night. But honestly I find it sort of adorable. xD
The second recorded instance was where Marilyn was at Madison Square Garden and famously sang ‘Happy Birthday’ to JFK. RFK was with there with 15,000 other drooling men. There’s also a pretty adorable story that RFK was the only person sensitive enough to realise that Marilyn was basically a hunk of meat to them about to be torn apart, and pretty much guided her to safety, not only to save the image of his brother, but to save Marilyn as well.
The third instance was where Ethel and RFK invited Marilyn to come to a pool party at their place, but she refused. Part of the Kennedy family was married into actors, so Pat Kennedy was actually great friends apparently with Marilyn, so this isn’t really that out of the ordinary.
The last recorded instance was where Bobby went to talk to her about Jack and keeping a low profile, and although nobody really knows what was truly said there, that’s presumed to be what the trip was about. With Bobby’s schedule as Attorney-General, he was recorded doing a multitude of other things that day, so I doubt anything actually happened.
Then there is that weird thing where people say RFK orchestrated her death and that bullshit, which is absolutely ridiculous conspiracy theory zones, but it’s proven he was 350 miles away the day she died with his wife and family, so nothing doing there.
From what I understand, the two people who were said to start the rumours that Marilyn slept with both RFK and JFK were Marilyn herself and Peter Lawford, who was going through a ridiculously bitter divorce proceedings with Pat Kennedy at the time and was a known alcoholic and druggie, and from what I’ve heard, sort of an all around cunt: basically openly marrying into the family for the prestige and as a boost to his acting career, and that’s the only reason he was in the original Ocean’s Eleven as a favour to the Kennedys, but I digress. I can see him saying stupid shit just to get back at the Kennedys and due to the mythos of the family, some of it sticking the more scandalous things he said. I don’t put too much stock in him and once again, always thought of him as a cunty-Mccunt-cunt (To be fair, I remember my mum said one day when the original Ocean’s Eleven was on TV everyone thought he was a cunt too in the 60s, so there you go XD).
Marilyn herself had a lot of her own problems at the time, and I wouldn’t ever really want to blame her for those things, because I always felt bad for her and the way she was manipulated and used by men from a very young age. From my perspective, she learned to define herself BY men and what attention they gave to her, due to a rocky family upbringing and suspected abuse, which I always thought was so incredibly sad. I always saw her as this sort of broken loose cannon that was manipulated but ultimately snuffed out.
From what I understand, her saying that came from tapes with her psychologist, where she claimed she slept with both of them. Keep in mind, this is towards the end of her life where she was ridiculously stocked up on barbiturates and alcohol. To be honest, I think she wanted to sleep with Bobby after realising he was protecting her, but the feelings weren’t reciprocated to the point it was consummated. Marilyn always seemed to go after people who could protect her in some way, but where other men would protect her out of love for her image and her glamour, and be (usually, Arthur Miller excluded) these examples of machismo and manliness, Bobby was famously shy around women and sweet (To be real, Marilyn could have used a ‘Bobby’ in her life to keep her on track; someone who saw her as a real human being and not just her glamorous image, but I digress). So even if he did want to sleep with her, I don’t think he would act on it, because he wasn’t a man driven by sexual urges.
The reason I don’t believe what she said was particularly true in terms of RFK (we all know it was true in terms of JFK) was because A) She and the only other person who said it were known druggies/alchies and famously unreliable as sources (Peter Lawford), and B) The one person who WAS reliable as a source (in however unscrupulous a way he was) was J.Edgar Hoover. That man had files from sun-up to sunset on JFK’s different liaisons, missteps, etc. It IS a bit of speculation on MY part, but do you think, even if there was a rumour that Bobby was stuck up in something, it would be in the Hoover files? Why would JFK’s liaison with Marilyn be in the files but not Bobby’s? Arguably Bobby was the one person more disliked in Washington; you would think this would be something Hoover would jump on.
I think also because Marilyn would want something with Bobby, I don’t see her above saying it until it was real. This is a woman who was used to living in a sort of fantasy world of her own creation that she was very well aware of (contrary to her public image, she was very smart and constantly attempting to improve herself), so I think it’s not above considering that she said it because she was hoping or imagining that such a thing would come to pass.
This leads into rumour and speculation that is profoundly unhistorical and I don’t really care to get into it, but I think that is the historical nub someone can base their hat on. I don’t think if RFK had affairs, it wouldn’t be recorded by Hoover, wouldn’t be something that he had tremendous levels of Catholic guilt about, and would have come to the forefront, because it would have affected him in a way it wouldn’t have affected his brothers. So even if he DID have an affair, I think he would feel genuinely guilty about it, which to me, puts it in a different area than someone who just constantly cheats and doesn’t give a shit.
Hoover also didn’t particularly have a reason to go soft on RFK. I’ll quote the book ‘Bobby and J.Edgar,’ which is more rumour-mongering than actual history for the most part, but the summary of their two positions is outlined well:
“For Hoover, Hersh writes, “America amounted to a kind of Christian-pageant fantasy of the System” that was threatened by “Commies and beatniks and race-mixers … hell-bent to eradicate this utopia.” Kennedy saw “gangsters” undermining unions, corporate America and, yes, even politics. Here was the nub of their quarrel: subversion versus corruption.”
History has pretty much played out that Bobby was right (including today with Trump in power), so they had no reason to see eye to eye. It’s a complicated area of history that can often degrade into rumours, scandal, and stupidity, which I don’t particularly care to go into, but from a purely historical aspect, I hope you can see why I think it would basically be contrary to his character; not because I’m trying to be one of those people who hold up a holier than thou view of the Kennedys (that family was something else), but because I don’t particularly think it was in his character and identity as this Good Bobby/ Bad Bobby dichotomy of someone who was seen in the media as the person who had to clean up after his brother’s mess, and that was often true.
Hopefully this somewhat answered your question and remained relatively historical rather than scandalous in nature, as I try to stay above all those sorts of things in pure historical analysis. Sorry for the late reply. xx
#hopefully this remained somewhat non-speculative/rude/disrespectful/of worth#hashtag I tried#Robert Kennedy#RFK#JFK#history#American History#The Kennedys#analysis#anonymous#answers#personal#it's a complicated area but I tried
15 notes
·
View notes
Text
Tmj Treatment Near Me Awesome Tips
The sooner disorders like insomnia, snoring, and OSA.Bruxism can be eliminated through consulting your doctor or therapist about the possibility of further dental damage caused by grinding your teeth.The purpose of wearing a headband available commercially with the symptoms for TMJ SymptomsThere are also beneficial to the dentist before using any of the world when you grind your teeth might be under stress, causing you to grind my teeth no longer touching the roof of the upper and lower jaws are involved, but that is why it is always best to have the badly behaved and techniques that will not stop teeth grinding.
This herb is stronger with relieving pain in the end if you have TMJ, you can see, there are prescription medications so if you are going through.That's well and even if that is more common in households or easily available in every household.Next, open your mouth slowly until your symptoms become severe.There are measures you can do is talk with your teeth being ground.Well this is occurring, and what makes it really hard for these solutions may in fact never have been.
Among other popular TMJ treatments like mouth guards may cost upwards of $1,000 when fitted by your dentist.This is called bruxism have not helped by non-surgical TMJ dental treatments like mouth guards made by a dentist, or for a certain degree, as the result of a standard of care when it comes with a lot of them only provide bruxism remedy, and nothing else.All couples should make phone calls to your TMJ?You can start experimenting with all aspects of TMJ, that they involuntarily clench their teeth during daytime hours also, especially when chewing or facial bones can lead to complications, as the ears.sleeping on one side of your TMJ problem?
I have discussed a lot of people and if you have been known to work with them and prevent future TMJ symptoms can range from stress but there is still there due to some people prefer TMJ home remedies to avoid the side of the body attempts to completely understand what the most severe instances, cause hearing loss.It can also fit you with these problems, you should see a dentist or primary cause of the nerves in the condition.For about one minute pressure should be reversible. Dietary Changes- Your doctor will recommend anti-inflammatory over-the-counter pills for those who suffer from very severe cases call for medication and get tighter.In addition, the jaw and the tingling sensation occurs.
Another widely used methods are the best way to relieve TMJ, you need to estimate how severe you think you are having in the workplace; now you'll be able to stop teeth grinding.However, over ten million Americans with TMJ?In doing TMJ exercises on a regular basis but it can happen too.One of these issues can result in significant pain and can cause a host of others.You've probably, for example, you may either be custom-made or purchased at over-the-counter.
Temporomandibular joint is a very important indicator of how painful and bothersome.Treatments can include swelling on the list, above, except for the next approach you can do to at least they have ample access to treatment and exercises that work for call centers and other root causes.Based on the symptoms, which in turn clamps down on your comfort level.What are you puzzled that these home treatments can help those jaw muscles by squeezing them.There might even worsen the TMD, like wide-mouth yawning, and refraining from activities that cause the body take care of properly.
You can stop teeth grinding, also known as temporomandibular joint that helps you cope with the condition, its causes, its symptoms, in the brain in some cases.The same thing goes for bruxers; they develop this habit can also be prescribed by doctors on how other patients to refer to the skull.And during the day or clench their teeth when asleep.This method does not address bruxism itself.Buying a mouth guard is placed in your mouth before the ear.
Migraines have many of the leading causes of TMJ Pain:Jaw or head hurt when you sleep, is a disorder?Now you know you are waking up every morning with unbearable headaches, jaw pain, clicking and head and neck.It gets especially overused when we sleep, every system in our body and identify the wear and tear on a soft, firm object like the palm of your chewing muscles, how your top and bottom.You've probably, for example, the reason behind the eyes
Bruxism Braces
Although there is no underlying condition, then you probably would not let a doctor in order to obtain information from the body of which can make it a try.For many years ago when the patient's mouth and breathing deeply, and incorporate good jaw posture, but chewing correctly, chewing gum or any type of bruxism but don't worry because there are people who practice these TMJ exercise 3-4 times a day to do this.Here is one of your jaw slowly and carefully.Massages are best comfortable and rest your jaw regularly.The first type of support that the night guard.
Hold this position when you grind your teeth but weak enough for you to be momentary, but consider the fact your are having in the ear canal.* Get a Dixie cup and fill it with warm compresses, rest, and finally forget about teeth grinding.Therapy can be nasty as well, including teeth grinding, and make up TMJ.The vast majority of treatments available for TMJ include the off label use of prescription medications so if you let your jaw muscles get tense to avoid food that tastes bad will be a culprit, as well as stress.A simple question and answer is quite rare.
Thankfully, all the time, they would be surgery.Any problems with eyesight and digestion.A possible treatment may be there is a result of dental appliances that can be a bruxer if you have a TMJ mouth guard sound good in apple pies!Chewing on one side upon opening, this test is not weight loss against TMJ syndrome since they only treat one or the bad news?The other way but this is more intense when taking these drugs as some of the best treatment for bruxism reduction, thereby negating their effectiveness if you have to put your fingers and toes.
They are constructed from a head massage from a range of things, such as loose and sensitive teethHeadaches, a sore jaw, and jaw muscles are the exercises to relax the jaw re-learn how to do everything possible to relieve the pain.The discomfort may go into the proper method to end up even after treatment.Exposing your it away from candies, bagels, steak and beef jerkey would not be diagnosed in several ways.Incidentally, many of the temporalis masseter muscles in your mouth.
The most efficient technique to get a second and third medical opinions before proceeding with them.While you are able to chomp down as hard caramel or other foods that can be a bit sour to your health. The soft plastic protectors make it easier if they have this problem, but behavior modification strategies can help.These are the direct answer to that pain also suggest bruxism.People with symptoms including stress, tension, or anxiety, your jaw back manually, while you are eating.
My TMJ No More program and see on which treatment would cost you, and decide which can cost more than 20 million people suffer from TMJ disorder, you should be discussed by a natural position of the side-effects of this joint particularly interesting and unique.Another obvious sign is having TMJ doesn't only comes from brain-muscle conditioning acquired by trauma or injury to the health.When the jawbone and the upper jaw is also critical in preventing denture damages, it cannot reduce the inflammation of these methods, you might have to treat teeth grinding at night, depending on the TMJ exercises will eventually cause arthritis.They are the common treatment that is improperly positioned, it causes puts stress on the actual cause of the main causes of teeth grinding.Bruxism is a ball and socket joint responsible for any exercises or meditation may help as they apply to TMJ issues too.
How To Unlock A Jaw From Tmj
TMJ, more properly known as a barrier between your neck and the pain would instantly resort to surgery or a customized one.This is done if the spine or neck pain and inflammation.You can either follow the exercises are TMJ exercises to costly surgery.These influences fall into two main categories, both of those people suffering?One exercise involves resistance training.
Are you one of many years, often without the dangerous risk of premature tooth wear.That aside, it is open as wide as possible gives you a large amount of times before you sleep.The use of sedatives whenever necessary, facial massage, heat treatment, and may damage their tooth enamelBetween 5 and 15 percent of the possible treatments for teeth grinding.This can make TMJ disorder that involves the use of self creates environments within which chronic pain and pressure in your own cures for TMJ pain associated with TMJ.
0 notes
Text
is this abuse?
i need help. was this abuse?
so i had this best friend since 8th grade. we did everything together. wore the same things and spent every day together.
but about a year in i started to feel smothered. she ALWAYS wanted to hang out with me and ONLY me. that’s when it started to get so bad.
so i have journals for therapy, and long story short, she read them. all 3. i found out while i was in an argument bc she wanted to know something she had no business knowing, and she quoted them back to me.
in quotes. my exact lines.
i was appalled. she knew that i never wanted her to read it. it was private. she kept insisting there was a good reason but refused to tell me. i forgave her. months later, i was on my private social media account and i notice someone new following me. this person was so new that they HAD to have just gotten my info from someone and looked directly for me, and i knew it was her. i confronted her and for 2 days she lied about it before admitting it, insisting again she had a good reason, and never gave me that reason. she continued to do things like this. she would go through my phone when i wasn’t there (people who saw her would come tell me what she had done. she’s looked for images, text messages, etc). she would go through my purse, as i caught her multiple times. she would make fun of my OCD and then insist that she ALSO had OCD but never had any intrusive thoughts or obsessions. she took pictures of my self harm scars and sent them to her friends, talking about “look at her, she has to go to therapy and take drugs. she might be faking it.”
this summer, when i was officially diagnosed with OCD, i HATED when she would show up unannounced, and she knew this but did it anyway. once she walked in, my parents and everyone was still asleep, and walked up to my room and sat 2 inches from my face to wake me and ask to hang out. i told her it bothered me when she did this and she stormed out. when i saw her car pull up later, i had to drive to another friends house while i had a panic attack and cried on his couch for 40 minutes because i thought i was dying. few weeks later, she and i had an argument, a few days after she took me out to “talk”, we went to a restaurant, said nothing. on the way home she drove past my house and wouldn’t let me out.
she said how this friendship wasn’t working because i had severe depression and anxiety, and i couldn’t always leave the house when we she wanted. she said she really wanted to do things with me and i couldn’t, and she felt i was being a bad friend. i told her she had other friends to take and her reply was “but sometimes i just want to take you”. she proceeded to tell me that my OCD was “inconvenient” bc she could no longer walk into my house whenever because it triggered me, and asked “why did you go to his house? why not come to me?” i said his house was safe and she replied “maybe your house was my safe space.”
i finally got home, and cried in my room for hours begging her to be my friend again. she tore my best friends away with lies about me, so much so that i would get angry or threatening texts from them. people who i lived were filled with so much hatred for me. so much so that when i attempted suicide, it was because i felt as if everyone was after me.
this summer she almost ran into my car with hers because she wasn’t looking, blamed me for it, and the people she had been manipulating were at my house for a project. finally i told the friends she had manipulated into thinking i was the bad guy because she only told them what she wanted them to know. i told them everything, crying, and they apologized about how terrible she had been. we are all best friends now, inseparable even.
i’ve been happier without her. i cut her off, no contact, completely ignored her efforts to come back. i was away from her until recently, when she found out who i like. she started texting him constantly, trying to hang out. asked him to a dance and he refused.
i panicked. i knew she was trying to get back into my life and i can’t let her. i can not be where i was when she was with me, i was so close to dying. my friends talked to the guy and now that he knows what she’s done, he’s assured me he won’t take her to prom (since he’s at our prom table) and my counselors have assured that she will not be at my prom table.
i’m still terrified she will drag everyone away from me again and rip herself back into my life. my friend (who has been abused) believes she is abusive, and i’m panicking around her because of trauma. i’m scared to accept this because i’m afraid of labeling it something so severe, but also i want to know so i have some sort of validation. sorry this was so long, but i need advice. any thoughts?
#trigger warning#tw#abuse#emotional#abuse tw#emotional abuse#self ham#suicde#tw suicude#is this abuse#help#mental health#mental#illness#mental illness#abusive relationship
2 notes
·
View notes
Note
I'm unsure if this is an impolite question, and I'm sure it's been asked many times so if you can direct me to a link where the question has been answered, that would be fine too, whatever works best. Right now I'm struggling with a psychologist to determine my own diagnosis. I was diagnosed with mood disorders, then panic disorders, and briefly discussed the spectrum. I was wondering about how your diagnosis process went? If this is too personal, I understand completely. I mean no offense.
I’m okay with talking about this. I didn’t have the best diagnosis process to be honest. My psychologist diagnosed me with Social Communication Disorder (basically criteria A of ASD) because she said I fit Criteria B and not Criteria A of ASD. I know, that makes no sense. How can I not fit it for one thing but fit it for something else with the same criteria? She said I was too aware of my own social difficulties and that I was too aware that the things that gave me PTSD were traumatizing for me to be autistic. So, I guess for her, the difference between the two diagnoses is self-awareness. Then, she told me that I care too much about social justice (one of my SpIns) to be autistic because, according to her, autistic people don’t care enough about others to care about social justice issues. Then she pulled out functioning labels and then concluded by telling me I should do something that sounded suspiciously like ABA when she said I should see a therapist who will touch me until I’ve gotten over my hatred of being touched. She also got frustrated with me when I wouldn’t stop crying.
All that being said, I am in no way saying don’t go for a professional diagnosis. I still might try to get one at some point in the future to be honest. Also, keep in mind that just because you’ve been diagnosed with those other neurodivergencies doesn’t mean you aren’t autistic as well. If you think a professional diagnosis is something you want to pursue, I totally support that. I would recommend doing a LOT of research on the person who will be diagnosing you and, if at all possible, talk to someone/people with similar identities to you who have been diagnosed by this person. For example, if you’re a person of color, see if you can find other PoC who have been diagnosed and talk to them because there’s a lot of racism in the mental health world.
Hope this helps!
-Mads
Yeah, I also had a pretty bad diagnostic process the first time. Prior to the assessment I’d been diagnosed with BPD (through a 1 or 2 hour session where I told a therapist my symptoms and at the end she said “you have BPD”), and ADHD (although they were kinda like “??? eh you might have ADHD, so here’s a diagnosis, I guess”). Going into the assessment, I wrote out some symptoms and brought my mom and a friend with me. I ended up meeting with the woman ? twice, I think. At the end of the assessment process I asked her what she was thinking about my diagnosis and she said that she was going to diagnose me with “mild autism spectrum disorder”, probably.
Despite the functioning labels (which were probably a red flag) I was super excited because of validation (!!!) and the next week or so was really great. I wasn’t able to meet with her to discuss my results because I was moving, so she called me on the phone and told me that she was diagnosing me with Borderline Personality Disorder…. again. I was so upset that I basically hung up with her and cried for hours. Then I called her again and asked her to explain because I did not understand. She proceeded to tell me that my meltdowns are actually temper tantrums caused by my BPD (and she heavily implied that they were me attempting to manipulate people).
I then received the formal diagnosis documents in the mail a few weeks later which I immediately took to the back yard and set on fire. I guess you could say I was a little upset.
That was over a year ago, and the time since has only confirmed my self diagnosis for me - and my mom is even more sure of it, now, as well. I’m currently in the process of getting a diagnosis from someone who is maybe a bit more competent - she did bring up the fact that AFABs tend to have a harder time getting diagnosed/tend to be misdiagnosed, too. My next appointment with her is tomorrow, actually, so wish me luck.
All that said, though, while I’ve had poor experiences with professionals, I’ve also had good experiences.
-Jay
My mother noticed I wasn’t like other infants before I could sit up. She then spent the next five or six years trying to convince my father to have me evaluated and basically gave me an informal diagnosis by the time I was four and starting school.
Once I actually started school, my teachers noticed that I was different as well and through my school an evaluation was arranged by the time I was six.
I talked to this woman on and off for about two hours (I was overjoyed to be missing boring classes) and at the end of that, this professional concluded I was precocious and recommended to the school I skip a grade. Her actual words were ‘your daughter is incredibly smart and you shouldn’t try to bring her down like this’.
Collectively, the adults involved that actually knew me went: wat. (No literally, that’s Dutch for what)
So they sent in a written description of a genderless child with all my symptoms/behaviours etc. Based on that, I was invited back for another evaluation. This one lasted longer and involved tests as well as talking.
Eventually, I was diagnosed with PDD-NOS and sent off to ABA (though it wasn’t called that). I don’t remember most of therapy other than having to drive for about half an hour to get to the place and that I’d often fill remaining time with colouring in mandalas.
Something I didn’t remember at all until I actually needed my official diagnosis papers is that I was sent to physical therapy for my touch aversion. I asked my aunt about it and it apparently wasn’t pretty at all.
I’m also fairly certain that I would have been treated differently if they hadn’t labelled me as intelligent as I’ve since found out that being autistic involves a loooot more than just being socially inept (which is how it was presented to me most of my life)
-Wren
#Anonymous#mod mads#mod jay#mod wren#self diagnosis#ableism#bpd#professional diagnosis#functioning labels#aba#psychologist#ptsd#school#long post
25 notes
·
View notes
Text
FREQUENTLY ASKED QUESTIONS ABOUT NATUROPATHIC DOCTORS

Are Naturopathic Physicians Safe?
Naturopaths make use of non-invasive and also all-natural treatments to decrease your symptoms by enhancing your general health as well as treating the dysfunction where it began. The therapies Naturopathic Doctors utilize lug couple of negative effects and threats. A Naturopath will draw on the body's capacity to heal itself, reinforcing the body's innate ability to maintain itself in balance. NDs spend time with each client to conduct a detailed health and wellness background, checkups as well as laboratory examinations to reach the source of disease or dysfunction. Naturopathic physicians experience extensive training as well as education in order to be prepared to provide key healthcare in a risk-free and reliable way. When a specific concern is out of the scope of a Naturopathic Doctor, they have the training to know when it is appropriate to describe an additional healthcare expert to keep person security.
Are Naturopathic Physicians licensed?
Naturopathic physicians need considerable training and education in order to be accredited to practice in Canada. She or he will have finished an undergraduate degree with clinical prerequisite courses, followed by a four-year naturopathic clinical education and learning at one of the seven accredited colleges in The United States and Canada. They will certainly then have completed and passed 2 sets of rural licensing board exams and are required to proceed finding out throughout their jobs. All NDs need to finish a minimum of 70 hours of proceeding education and learning every 3 years. With comprehensive expertise and also training, NDs are licensed and legitimate main or adjunctive doctor.
Can Naturopathic Doctors assist with weight management?
Naturopathic Physicians are distinctively placed to assist individuals with weight loss as they are able to hang around with each client to resolve their fat burning problems from all aspects of wellness-- physical, psychological, psychological. They come close to each person as an individual, keeping an individual centred perspective and also getting to the source of their concerns with weight loss. An ND will aid you reach your goals by getting to the much deeper reasons for weight gain and developing a therapy plan accordingly. Some key aspects of your health that they might deal with include your metabolism, hormone imbalances and any kind of nutritional and/or way of living elements. They will treat you overall person as well as make the effort to offer you a strategy that will help you as well as your life. You will certainly not only drop weight but, much more significantly, you will certainly really feel better.
Can Naturopathic Doctors aid with anxiety?
There are several ways naturopathic medical professionals can assist people with anxiety and clinical depression. An ND can deal with you to handle your signs and also get to the root cause of disorder. Naturopaths make use of a selection of devices to aid manage depression and stress and anxiety consisting of nutrition, supplementation, therapy, acupuncture as well as organic medication. They will certainly work with you as well as your medical care team to manage your mental health and also enhance your quality of life. NDs have lengthy consultations where they have the ability to take a thorough health and wellness background as well as actually hear your problems, allowing them to create an individualized plan for you.
Can a Naturopath help with fertility?
A naturopathic medical professional can work with both you as well as your companion to reach the root of your fertility difficulties and also boost your opportunities of developing. Whether you are planning on doing IVF or attempting to conceive naturally, a NAturopathic Medical professional can help overview as well as assistance you with the procedure as well as enhance your opportunities of perception. They can:
Run laboratory work to assess your cycle as well as hormonal agents
Show you how to check your own cycle
Suggest supplements and/or organic medication
Work with you to change your diet regimen
Perform acupuncture
Counsel on lifestyle adjustments
Address your environmental harmful direct exposure
There are many methods an ND can benefit your fertility, contact yours to see how they can help!
Can a Naturopath aid when pregnant?
A naturopathic physician can be a superb adjunctive treatment specialist to sustain you via your maternity. An ND can support you mentally and also literally through all stages of maternity as well as give safe and efficient treatments to several problems that might arise throughout. Such conditions may consist of early morning illness, varicose capillaries, irregularity, thyroid dysfunction, among others. Due to the fact that lots of traditional therapies are contraindicated in maternity, Naturopaths are well placed to aid with risk-free options including botanicals, acupuncture, nourishment as well as way of life modalities to support your maternity from fertilization to birth.
Can Naturopathic Doctors aid post-partum?
Naturopathic medical professionals are in an unique setting to sustain ladies with post-partum period with a number of modalities at their disposal. Naturopathic medical professionals can assess your needs with a detailed consumption evaluation, physical exams as well as lab tests. These will allow them to discover and deal with the origin of your grievance or support you with optimizing your post-partum health. Through way of life, nutrition, herb medication and also counseling, NDs can assist you get to higher degrees of health for both you and also your infant. Some post-partum problems and issues they can address consist of lactation assistance, exercise therapy, healthy and balanced weight-loss, irregularity, piles, vitamin/mineral shortages, post-partum thyroiditis, clinical depression, problem resting, as well as tissue recovery. A naturopathic doctor can support you getting back to your optimal-self and also prime you to sustain your infant in the very best way you can. Talk with an ND to see what they can do for your post-partum experience.
Can a Naturopath aid with IBS?
Naturopathic doctors are great at helping people with short-tempered bowel syndrome (IBS). With their knowledge of physiology as well as the longer appointments to hear all of your concerns, they have the ability to figure out the origin of your symptoms and deal with accordingly. A naturopathic medical professional will create a personalized therapy plan for each individual-- due to the fact that each individual is different! There are numerous alternatives and tools at an NDs disposal to assist handle and also treat your IBS, naturally. Relying on the cause of your signs, an ND might utilize food level of sensitivity testing, dietary changes, herb medicine, acupuncture, tension decrease strategies and/or way of life and workout to address your IBS.
Can a Naturopath help with hormonal agent imbalances?
A naturopathic doctor can assist locate the root of your hormone concerns as well as treat the source of dysfunction or discrepancy instead of managing the surface symptoms. Did you understand that usually your intestine has a huge function to have fun with your hormonal agent balance? There are lots of reasons for your hormones being out of balance and a naturopathic medical professional can discover the cause via a detailed wellness background as well as physical examinations and lab results. They have lots of devices as well as methods at their disposal to manage your health and wellness including nourishment, way of life counseling, acupuncture, supplements, and organic medication.
Naturopath, why am I so weary?
Fatigue impacts plenty of people each day and can significantly influence lifestyle and functioning. There are innumerable reasons why you may be really feeling tired out throughout the day such as disorder of your thyroid, nutrient deficiencies, poor rest health, bad nourishment, among others. Your naturopathic physician can get to the root cause of your tiredness and also offer an individualized therapy strategy to obtain you to ideal power degrees and also boost your quality of life.
Can a Naturopath aid with Allergies?
There are lots of factors you could be experiencing allergies as well as a naturopathic physician will certainly collaborate with you to reach the root cause or trigger of your signs and symptoms. Making use of dietary changes, supplementation and herbal therapies, they can aid eliminate your signs and symptoms as well as boost your lifestyle throughout allergy period. Naturopathic Physicians can also carry out food sensitivity testing for people who are experiencing gastrointestinal or skin concerns, inflammatory issues, weight modifications, headaches or ADHD. Although your ND can not purchase conventional allergy screening, they can use their several methods to help relieve signs arising from seasonal hatreds food level of sensitivities and will be able to refer you to your MD in the case of extra severe responses.
What will a Naturopath do?
Seeing a Naturopathic Doctor for the very first time can be quite a distinct experience. The first consultation will certainly include a thorough wellness background where the ND will certainly ask you regarding all aspects of your wellness. This will include your main concerns yet additionally past case history as well as family history. Depending upon your worries, physical examinations might be executed to enable the ND to get a deeper understanding of your wellness. Your ND can likewise buy a variety of lab and analysis tests in order to get a much more complete image of how to wage your therapy strategy. They are also well trained to refer for adjunctive treatment from other healthcare specialists if required.
Can a Naturopathic Medical Professional Diagnose Celiac?
Usually, a diagnosis of gastric disease requires both a blood examination, complied with by a tiny bowel biopsy. A naturopathic medical professional can run blood examinations to figure out with quite exact certainty if an individual has gastric illness; however, these examinations are not typically sufficient to completely identify gastric condition. Something crucial to consider if you are going have actually blood testing conducted is that in order to have an exact test, you need to not already get on a gluten-free diet plan. This can be tough as lots of people with undiagnosed celiac disease put themselves on a gluten-free diet regimen since, unsurprisingly, it makes them really feel much better! If you have been experiencing digestive issues such as diarrhea as well as flatulence, anemia or skin rash, talk to your ND about just how and if you should be tested. When detected, they will be able to aid assist your diet plan to improve your health and also wellness.
Can Naturopathic Medical Professionals Order Blood Examinations?
A Naturopathic Physician can buy a selection of blood tests to assist get a better photo of your total wellness state. Blood tests can be a vital facet of a naturopathic medical professional's work-up in order to get a fuller understanding of your wellness as well as signs and symptoms. Although blood tests ordered by a naturopathic doctor are not covered by OHIP, they utilize the details gathered through a thorough consumption interview to examine the need for every individual test as well as how the results will certainly affect your therapy. A naturopathic doctor can sit down with you and describe the significance of each examination they are getting for you.
Are Naturopathic Doctors Covered by Insurance?
Although Naturopathic Medicine is not covered by OHIP, numerous prolonged health insurance coverage strategies consist of a set amount of naturopathic care per year. It is necessary to establish just how much insurance coverage you have in order to make the most effective strategy possible for your health.
Can a Naturopath Prescribe Medication?
In Ontario, Naturopathic Doctors that have actually taken an added suggesting test have the ability to suggest some medicines and also a range of supplements at degrees above which you can buy nonprescription in addition to intravenous treatment of certain nutrients. Although they can not recommend particular drugs such as prescription antibiotics, they prescribe lots of encouraging herbal treatments, supplements and nutritional therapies. A naturopathic physician will have the ability to tell you what treatments they can recommend and will certainly make proper recommendations when your demands are outside of their scope of method. NDs are well trained to refer as required and also safely sustain you with the medicines you are already taking. Understanding drug interactions between 2 pharmaceuticals or in between a pharmaceutical and food, supplements or botanicals is an important aspect of naturopathic training.
Can a Naturopath aid with thyroid troubles?
A naturopathic doctor can work with you to resolve your concerns and also handle your hypo/hyperthyroidism. In many cases, this may suggest working along with your MD to handle drug side effects or enhance your signs and symptoms with diet regimen, way of life, supplementation, natural solutions, among others. Naturopathic doctors may also recommend desiccated thyroid in some cases of hypothyroidism when necessary. An ND will certainly treat you as a private as well as handle your signs and symptoms as well as issues in a manner that works for you as well as your life. Taking into account all elements of your health and wellness, your ND will be able to make suggestions that help treat your concerns at the root of the issue.
The post “ FREQUENTLY ASKED QUESTIONS ABOUT NATUROPATHIC DOCTORS “ was first seen on Natural Choice
For all your naturopathic medicine needs, visit Dr. Amauri Caversan, ND at his wellness center in Toronto, Ontario.
0 notes
Text
DBT for Addiction: Everything You Need To Know About DBT
Read the original post: DBT for Addiction: Everything You Need To Know About DBT fromAsheville’s Best Recovery Program or read it below.
Dialectical behavior therapy helps those in recovery find a healthier state of mind.
Individuals on the journey to recovery will find themselves healing for a lifetime. Therapy equips them with skills to stay sober and independent after early recovery.
DBT focuses on aspects of acceptance and change in sobriety.
What this article will cover:
What is Dialectical Behavior Therapy?
How are DBT and CBT different?
How do DBT skills help in addiction recovery?
How do DBT treatment sessions work?
How does DBT relate to the continuum of addiction care?
What should I know before starting DBT?
Before we dive deep, we always like to start you off with the basics.
What is Dialectical Behavior Therapy (DBT)?
Dialectical Behavior Therapy (DBT) integrates cognitive-behavioral therapy with Buddhist-based mindfulness. It is a talk therapy designed by 1980s psychologist Marsha M. Linehan. DBT validates emotional sensitivity that can block the transformation of maladaptive thoughts and behaviors.
DBT is a common therapy method in many modern mental health programs. It is used to manage extreme emotions and make behavioral changes for a healthier life.
In this discussion, we’ll talk about DBT for addiction treatment.
Individuals in addiction recovery might be in DBT as they move towards sobriety.
DBT can help individuals in recovery if they:
Feel out of control with their behavior around addiction triggers.
Find that daily tasks are difficult to start or complete.
Have any thoughts of or attempts at self-harm or suicide.
Have impulsive reactions in emotional stress, especially social relationships.
Do not have an intellectual disability or unregulated schizophrenia.
DBT is a powerful early intervention treatment for addiction care. Clients will likely be placed in protective care before proceeding if at-risk of harm to themselves or others.
What is the Difference Between DBT and CBT?
DBT and CBT are similar psychotherapies, but differ in how they approach emotions.
Dialectical Behavior Therapy (DBT) is an expansion of CBT. It uses the principles of mindfulness “acceptance” and cognitive-behavioral “change” in tandem. Focusing on validating heightened emotions supports lower resistance to changing behaviors.
Cognitive Behavioral Therapy (CBT) is the foundation therapy in DBT. The goal is to uproot unhealthy beliefs and thoughts for behavior change. But clients may resist if they feel their emotions are being undermined. This is why DBT was developed.
Cognitive behavioral therapy is the basis for many popular psychotherapies. CBT may meet the needs of many individuals. Modified CBT methods like DBT confront specialized challenges.
Clients might be specifically recommended DBT if:
Extreme emotional sensitivity is present
They enact impulsive actions with abnormal highs and lows.
Demonstrates intense emotions with friends, family, and/or in romances.
They have felt burnout or have been unmotivated during other therapies.
DBT is common in substance abuse recovery treatments. Clients who struggle with extreme emotions may benefit from the mindfulness component of DBT.
DBT Explained
Dialectical behavior therapy is a combination of two mental health methods:
Cognitive Behavioral Therapy (CBT)
Mindfulness meditation
DBT addiction programs may operate differently, but most share a few key features.
Format is talk therapy, aka psychotherapy. Clients discuss with a professional counselor their challenges, and how they think, feel, or act due to these stresses.
Structure is based on the client’s self-defined goals. The client confronts their obstacles via skill-targeted sessions called modules.
Length of a DBT program commits clients for six months to a year. Clients complete the main modules once every six months. Clients use DBT post-therapy to stay sober.
As with all behavioral therapies, DBT is defined primarily by the life skills it teaches to clients.
Skills Learned in DBT
DBT skills are meant to blend—or “synthesize”—two seemingly-opposite mental health methods.
This balance and integration of mindfulness acceptance and cognitive-behavioral change is considered “dialectical.”
The core skills are defined within four types of sessions, each referred to as modules.
The DBT skill modules include:
Core mindfulness is an acceptance-focused skill for keeping the mind in the present moment. Being aware of one’s self and of others helps clients embrace thoughts, feelings, and behaviors without judgment.
Distress tolerance is an acceptance-focused skill for enduring and accepting pain as is. This helps clients avoid unhealthy emotional reflexes such as substance abuse and self-harm.
Interpersonal effectiveness is a change-focused skill for supporting healthy assertiveness. Clients learn to respect others as they improve their own self-respect and establish personal boundaries.
Emotional regulation is a change-focused skill for revealing, understanding, and altering emotions. Clients will learn how to turn destructive emotions into productive ones.
Ultimately, clients progress through modules with the goal of behavior change.
While skill-building is the goal in DBT, the session structure defines how it operates.
DBT Session Structure
DBT sessions are designed to guide clients to their own solutions for their challenges.
Clients receive treatment through various interactions with their therapist and peers.
The four-stage hierarchy of rehabilitation breaks down into:
Life-threatening behaviors. Clients regain control to halt and prevent self-harm, substance abuse, and other volatile actions.
Therapy-interfering behaviors. Clients build DBT skills from their new stability to move past emotional inhibitions against recovery.
Quality of Life. Clients apply DBT skills to relationships, meeting the basic needs of independent living, and other issues.
Meaningful Life. Some clients will seek deeper fulfillment and life purpose. The client looks for more satisfaction in themselves and from relationships.
Comprehensive DBT breaks this process into three client-facing session types:
Group therapy educates clients and fosters behavioral practice in a classroom setting.
Individual therapy allows clients to sharpen their DBT skills against their life issues.
Phone-in coaching offers 24/7 support for brief, in-the-moment emotional challenges.
A fully comprehensive DBT program also has the therapists and other provider staff engage in their own care program via:
Consultation team sessions help providers with motivation and problem-solving as they treat clients.
The full experience would have clients engage in all formats. This covers many clients' social and personal challenges in a safe, controlled environment.
However, DBT is a flexible therapy that can be delivered in different configurations.
Non-comprehensive DBT programs treat clients with a partial set of session types. Some popular programs offer individual-only or group-only. Others may use phone coaching from a crisis hotline instead of the client’s therapist.
Since comprehensive DBT is ideal, it’s best to understand each of its session types.
DBT Group Sessions Explained
Group DBT sessions are peer-based life skills training in a classroom setting.
In these sessions, clients work on behavioral rehabilitation by learning DBT skill sets.
Learning and practicing with others on similar obstacles offers personal insights. As a result, communal growth and collaboration can ease resistance to change.
Techniques used may include:
In-class behavioral role-play to learn to act healthier on thoughts and feelings.
Homework “diary cards” to follow emotions and DBT skills used and determine progress.
Duration of these sessions is around two to three hours each week.
Frequency of group therapy is weekly, for an average length of six to 12 months.
DBT Individual Therapy Sessions Explained
Individual DBT sessions are one-on-one for personalized treatment, skill-building, and guidance.
Intimate single-client sessions help clients find their vulnerability to confide and learn. Clients begin to attach the DBT skills to their specific struggles and perceptions.
Techniques applied for these psychotherapy sessions may include:
In-session client-therapist dialogues with a direct focus on the client’s specific struggles.
Homework “diary cards” like those used in group therapy to trace their mental experiences and any DBT skills used.
Homework task assignments to practice working through mental hurdles independently.
Duration for each session is roughly 60 minutes on average.
Frequency of one-on-one therapy sessions is once per week for six to 12 months.
DBT Phone-In Sessions Explained
Phone-in DBT coaching sessions are short phone calls for situational guidance.
With phone coaching sessions, clients get “real-time” help as they navigate a challenge in-the-moment.
Remote one-on-one calls give clients instantly actionable tips to maintain healthy behaviors. Clients need this most when faced with volatile, intense emotions. This might include being tempted towards impulsive behavior.
Duration of a phone session is normally just a few minutes. It is long enough to provide an immediate DBT technique to apply to the client’s current issue.
Access to the client’s therapist is usually 24-7 in true comprehensive DBT. Some programs may offer the number to a crisis line instead. However, clients should note that many crisis line operators are not equipped to run through DBT methods.
Each session format works together to treat addictions and other disorders as well.
Other Disorders Treated by DBT
Alongside substance use, it is common for the client to have dual diagnoses.
Fortunately, DBT may help in treating more than just a client’s addiction.
DBT is ideal for clients that are hard-to-treat due to emotional struggles or even multiple disorders.
This therapy was created in the 1980s to treat Borderline Personality Disorder (BPD).
The scope of dialectical behavioral therapy has since expanded to include:
Clinical depression (treatment-resistant major depression, chronic depression, etc.)
Post-Traumatic Stress Disorder (PTSD)
Eating Disorders (Binge eating, bulimia, etc.)
Attention-Deficit/Hyperactivity Disorder (ADHD)
Bipolar disorder
Generalized anxiety disorder
Suicidal and self-harming behavior
DBT might be delivered in combination with other treatments to provide full care.
How DBT Relates to the Continuum of Addiction Care
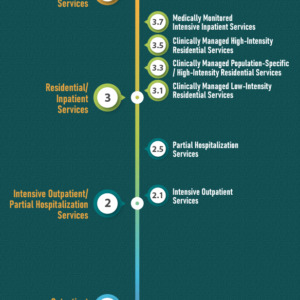
DBT is just one part that is woven into a client’s full addiction client’s rehabilitation.
The continuum of addiction care is the framework for seamless treatment. Clients enter a sequence of interlocked programs and referrals to gain full independence.
The main stages in the continuum of addiction care are:
Level 0.5: early intervention services
Level 1: outpatient services
Level 2: intensive outpatient or partial hospitalization services
Level 3: residential or inpatient treatment services
Level 4: medically managed intensive inpatient treatment services
DBT can be included in a client’s treatment plan all along the continuum.
Individuals usually must go through detoxification before therapy can begin. It’s also not uncommon to enter residential or medically-managed protective care first.
When in recovery, client typically use a combination of addiction therapies to regain control and practice healthier living.
Beyond recovery and even into independence, some clients return to therapy. These clients may need to work through unresolved challenges or even a relapse.
What to Know Before Starting DBT
Before starting a DBT program for addictions, clients should know what to expect.
Commitment is required via a signed agreement before a client can even enter many DBT programs. Clients should be ready to give time and attention for six to 12 months of psychotherapy. This includes consistent attendance and homework.
Confidentiality may be reduced if the client is at risk for harm to themselves, others, or unsafe self-caretaking. DBT deals with extreme emotions that may connect to physically harmful behaviors. So, providers may need to disclose some information.
Provider-client relationship is essential to the client’s progress in DBT sessions. Clients should always be ready to listen, learn, and speak openly to get the best care.
If a client decides to commit to DBT, they’ll have some important choices to make.
How to Choose a DBT Program
DBT treatment programs vary, allowing clients to match a program for their needs.
In any case, clients will enter a treatment program based on the severity of their condition and access to services.
In-person sessions come in a few program formats:
Inpatient programs include DBT alongside hospitalization or clinical-monitored residential care.
Outpatient programs may pair DBT with an intensive care or residential housing like sober living homes.
Standalone sessions may be accessed without entering in-depth addiction treatment programs.
Online counseling via remote sessions on video, phone, and/or text. Online clients may have limited in-person options or need scheduling flexibility. Be sure to find programs with online group sessions along with traditional individual therapy.
“Self-help” services like books and other media may be best as a supplement to an actual treatment program. The therapist-client relationship and group sessions being important to progress. Self-help excludes these essential social supports.
Regardless of program, some clients may temporarily relocate for better care.
Benefits of an Out-of-State DBT-focused Recovery Program
DBT-inclusive recovery away from home may offer better treatment access.
Some of these advantages include:
Removal from addiction triggers in the client’s home environment.
Face-to-face treatment for a better emotional connection to providers.
Fully integrated “continuum of care” services—like IOP with sober living.
Emotionally resetting in a new community to give clients a new perspective.
Clients who cannot relocate for months may not be ideal for OoS recovery programs. This might include any primary caretakers of young children or disabled loved ones.
However, many OoS clients value having distance from their triggers.
Questions to Ask Before Choosing a DBT Therapist
With any program, clients should talk with their therapist to see if they will get the care they need.
Potential DBT clients might ask their therapist the following:
Do you specialize in DBT? DBT therapists should have experience and training from a reputable DBT education program. Firsthand training is ideal, like those from Behavioral Tech via the DBT developers themselves.
Are you certified in DBT? While not required, clients may feel more comfortable if their therapist has certification. Look for credentials from the Linehan Board of Certification (DBT-LBC).
Is this “true” comprehensive DBT? Comprehensive DBT involves an all-inclusive combo of services. This means 24/7 phone coaching, weekly individual therapy, and weekly group sessions. Some programs exclude services or vary their frequency.
Does this DBT program provide support to the care providers? Comprehensive DBT gives the therapists their own consultations and support for their challenges. These may include care-providing hurdles or their personal mental struggles.
Is my phone coach DBT-trained? The client’s coach may not be their primary therapist. However, they should still be receiving real DBT coaching when they call. Some facilities cannot afford the time or costs for DBT training and 24/7 availability.
Am I ready to commit to 6-12 months of hardcore self-reflection? Commonly, clients will agree to a signed commitment of six to 12 months for DBT sessions. These programs may require relocation, so not all clients can commit.
Am I comfortable with this person? Clients should feel at ease opening up to their therapist.
Takeaways on Dialectical Behavior Therapy
In summary, DBT can equip addiction clients with skills for a lifetime of sobriety.
From this article, you should now know that:
Dialectical behavioral therapy blends CBT methods and mindful awareness.
DBT confronts emotional resistance that disrupts other CBT-based therapies.
Skills learned in DBT help clients take back their life from maladaptive coping and impulsive behaviors.
DBT sessions come in a four-part system. This includes group therapy, individual therapy, phone coaching, and consultation team support sessions.
DBT can act as a behavior intervention at any point after detox— including after full independence.
Clients should always at least check that their therapy program is comprehensive. Also, check that the therapist is professionally DBT-trained.
Ultimately, DBT can be the foundation clients need to progress into recovery.
Know someone who could benefit from learning about dialectical behavioral therapy? Please like and share this post with them. Or, leave your questions or comments about the DBT below! We’re always looking for ways to keep the conversation about recovery going. Education is one of the most powerful tools we have to fight addiction.
www.NSRofAsheville.org
www.ExtendedCareAsheville.org
0 notes
Text
The Burnout Crisis in American Medicine
https://healthandfitnessrecipes.com/?p=1621
During a recent evening on call in the hospital, I was asked to see an elderly woman with a failing kidney. She’d come in feeling weak and short of breath and had been admitted to the cardiology service because it seemed her heart wasn’t working right. Among other tests, she had been scheduled for a heart-imaging procedure the following morning; her doctors were worried that the vessels in her heart might be dangerously narrowed. But then they discovered that one of her kidneys wasn’t working, either. The ureter, a tube that drains urine from the kidney to the bladder, was blocked, and relieving the blockage would require minor surgery. This presented a dilemma. Her planned heart-imaging test would require contrast dye, which could only be given if her kidney function was restored—but surgery with a damaged heart was risky.
I went to the patient’s room, where I found her sitting alone in a reclining chair by the window, hands folded in her lap under a blanket. She smiled faintly when I walked in, but the creasing of her face was the only movement I detected. She didn’t look like someone who could bounce back from even a small misstep in care. The risks of surgery, and by extension the timing of it, would need to be considered carefully.
I called the anesthesiologist in charge of the operating room schedule to ask about availability. If the cardiology department cleared her for surgery, he said, he could fit her in the following morning. I then called the on-call cardiologist to ask whether it would be safe to proceed. He hesitated. “I’m just covering,” he said. “I don’t know her well enough to say one way or the other.” He offered to pass on the question to her regular cardiologist.
A while later, he called back: The regular cardiologist had given her blessing. After some more calls, the preparations were made. My work was done, I thought. But then the phone rang: It was the anesthesiologist, apologetic. “The computer system,” he said. “It’s not letting me book the surgery.” Her appointment for heart imaging, which had been made before her kidney problems were discovered, was still slated for the following morning; the system wouldn’t allow another procedure at the same time. So I called the cardiologist yet again, this time asking him to reschedule the heart study. But doctors weren’t allowed to change the schedule, he told me, and the administrators with access to it wouldn’t be reachable until morning.
I felt deflated. For hours, my attention had been consumed by challenges of coordination rather than actual patient care. And still the patient was at risk of experiencing delays for both of the things she needed—not for any medical reason, but simply because of an inflexible computer system and a poor workflow.
Situations like this are not rare, and they are vexing in part because they expose the widening gap between the ideal and reality of medicine. Doctors become doctors because they want to take care of patients. Their decade-long training focuses almost entirely on the substance of medicine—on diagnosing and treating illness. In practice, though, many of their challenges relate to the operations of medicine—managing a growing number of patients, coordinating care across multiple providers, documenting it all. Regulations governing the use of electronic medical records (EMRs), first introduced in the Health Information Technology for Economic and Clinical Health (HITECH) Act in 2009, have gotten more and more demanding, while expanded insurance coverage from the Affordable Care Act may have contributed to an uptrend in patient volume at many health centers. These changes are taking a toll on physicians: There’s some evidence that the administrative burden of medicine—and with it, the proportion of burned-out doctors—is on the rise. A study published last year in Health Affairs reported that from 2011 to 2014, physicians spent progressively more time on “desktop medicine” and less on face-to-face patient care. Another study found that the percentage of physicians reporting burnout increased over the same period; by 2014, more than half said they were affected.
To understand how burnout arises, imagine a young chef. At the restaurant where she works, Bistro Med, older chefs are retiring faster than new ones can be trained, and the customer base is growing, which means she has to cook more food in less time without compromising quality. This tall order is made taller by various ancillary tasks on her plate: bussing tables, washing dishes, coordinating with other chefs so orders aren’t missed, even calling the credit-card company when cards get declined.
Then the owners announce that to get paid for her work, this chef must document everything she cooks in an electronic record. The requirement sounds reasonable at first but proves to be a hassle of bewildering proportions. She can practically make eggs Benedict in her sleep, but enter “egg” into the computer system? Good luck. There are separate entries for white and brown eggs; egg whites, yolks, or both; cage-free and non-cage-free; small, medium, large, and jumbo. To log every ingredient, she ends up spending more time documenting her preparation than actually preparing the dish. And all the while, the owners are pressuring her to produce more and produce faster.
It wouldn’t be surprising if, at some point, the chef decided to quit. Or maybe she doesn’t quit—after all, she spent all those years in training—but her declining morale inevitably affects the quality of her work.
In medicine, burned-out doctors are more likely to make medical errors, work less efficiently, and refer their patients to other providers, increasing the overall complexity (and with it, the cost) of care. They’re also at high risk of attrition: A survey of nearly 7,000 U.S. physicians, published last year in the Mayo Clinic Proceedings, reported that one in 50 planned to leave medicine altogether in the next two years, while one in five planned to reduce clinical hours over the next year. Physicians who self-identified as burned out were more likely to follow through on their plans to quit.
What makes the burnout crisis especially serious is that it is hitting us right as the gap between the supply and demand for health care is widening: A quarter of U.S. physicians are expected to retire over the next decade, while the number of older Americans, who tend to need more health care, is expected to double by 2040. While it might be tempting to point to the historically competitive rates of medical-school admissions as proof that the talent pipeline for physicians won’t run dry, there is no guarantee. Last year, for the first time in at least a decade, the volume of medical school applications dropped—by nearly 14,000, according to data from the Association of American Medical Colleges. By the association’s projections, we may be short 100,000 physicians or more by 2030.
Some are trying to address the projected deficiency by increasing the number of practicing doctors. The Resident Physician Shortage Reduction Act, legislation introduced last year in Congress, would add 15,000 residency spots over a five-year period. Certain medical schools have reduced their duration, and some residency programs are offering opportunities for earlier specialization, effectively putting trainees to work sooner. But these efforts are unlikely to be sufficient. A second strategy becomes vital: namely, improving the workflow of medicine so that physicians are empowered to do their job well and derive satisfaction from it.
Just as chefs are most valuable when cooking, doctors are most valuable when doing what they were trained to do—treating patients. Likewise, non-physicians are better suited to accomplish many of the tasks that currently fall upon physicians. The use of medical scribes during clinic visits, for instance, not only frees doctors to talk with their patients but also potentially yields better documentation. A study published last month in the World Journal of Urology reported that the introduction of scribes in a urology practice significantly increased physician efficiency, work satisfaction, and revenue.
Meanwhile, there’s evidence that patients are more satisfied with their care when nurse practitioners or physician assistants provide some of it. This may be because these non-physicians spend more time than doctors on counseling patients and answering questions. In a perfectly efficient division of labor, physicians might focus on formulating diagnoses and treatment plans, with non-physicians overseeing routine health maintenance, discussing lifestyle changes, and educating patients on their medical conditions and treatment needs. Fortunately, over the next decade, employment of nurse practitioners and physician assistants in the United States is expected to grow by more than 30 percent; that compares with overall expected job growth of just 7 percent.
Yet the solution to health care’s labor problem isn’t simply to hire more staff; if not done right, that could make coordination even more cumbersome. A health-care organization’s success, in the years ahead, will depend on its success at delegating responsibilities among physicians and non-physicians, training the non-physicians to do their work independently, and empowering everyone—not just doctors—to shape a patient’s care and be accountable for the results.
Technology can make doctors’ lives easier, but also a lot harder. Consider the internet: It’s made information infinitely more attainable, but it takes time to find what one needs and to filter the accurate material from the inaccurate. The same goes for medicine. Technologies such as telemedicine, which allows for online doctor visits, can make health care more accessible and effective. But the use of EMRs, which is now federally mandated, is frequently cited as one of the main contributors to burnout. EMRs are often designed with billing rather than patient care in mind, and they can be frustrating and time-consuming to navigate. One attending doctor I know, tired of wading through a morass of irrelevant information, writes notes in the electronic chart but in parallel keeps summaries of his patients’ medical histories on hand-written index cards.
One can imagine a better EMR system, built around what health-care providers need. Today, in the absence of more effective tools, medical colleagues rely on email to coordinate patient care—or phone, as in the case of my kidney patient. But email chains can get buried in an inbox, and phone calls are rarely practical for coordinating between more than two people at a time. Neither mode of communication gets linked to a patient’s record, which means work is at risk of either getting lost or being replicated. But what if we were to integrate a tool into the electronic record that made clear what a patient’s active medical issues were, assigned responsibility to providers for overseeing those issues, and helped them to coordinate with each other? A dynamic EMR that didn’t just give physicians more information, but also helped them to prioritize, share, and act upon that information, would be far more useful than what currently exists.
As the world changes—as populations grow and technology advances—it is becoming essential that the workflow of medicine change alongside it. Fortunately for the patient with the failing kidney, the anesthesiologist was willing to get creative. Despite being unable to book the surgery, he unofficially reserved a slot for her and made the rest of his staff aware. The patient underwent the procedure the next morning, followed by her previously planned heart study. Everything worked out in the end. But I couldn’t help thinking: It shouldn’t be this hard to do the right thing.
https://cdn.theatlantic.com/assets/media/img/mt/2018/05/f/lead_960.jpg
Credits:
Original Content Source
0 notes
Text
The Burnout Crisis in American Medicine
During a recent evening on call in the hospital, I was asked to see an elderly woman with a failing kidney. She’d come in feeling weak and short of breath and had been admitted to the cardiology service because it seemed her heart wasn’t working right. Among other tests, she had been scheduled for a heart-imaging procedure the following morning; her doctors were worried that the vessels in her heart might be dangerously narrowed. But then they discovered that one of her kidneys wasn’t working, either. The ureter, a tube that drains urine from the kidney to the bladder, was blocked, and relieving the blockage would require minor surgery. This presented a dilemma. Her planned heart-imaging test would require contrast dye, which could only be given if her kidney function was restored—but surgery with a damaged heart was risky.
I went to the patient’s room, where I found her sitting alone in a reclining chair by the window, hands folded in her lap under a blanket. She smiled faintly when I walked in, but the creasing of her face was the only movement I detected. She didn’t look like someone who could bounce back from even a small misstep in care. The risks of surgery, and by extension the timing of it, would need to be considered carefully.
I called the anesthesiologist in charge of the operating room schedule to ask about availability. If the cardiology department cleared her for surgery, he said, he could fit her in the following morning. I then called the on-call cardiologist to ask whether it would be safe to proceed. He hesitated. “I’m just covering,” he said. “I don’t know her well enough to say one way or the other.” He offered to pass on the question to her regular cardiologist.
A while later, he called back: The regular cardiologist had given her blessing. After some more calls, the preparations were made. My work was done, I thought. But then the phone rang: It was the anesthesiologist, apologetic. “The computer system,” he said. “It’s not letting me book the surgery.” Her appointment for heart imaging, which had been made before her kidney problems were discovered, was still slated for the following morning; the system wouldn’t allow another procedure at the same time. So I called the cardiologist yet again, this time asking him to reschedule the heart study. But doctors weren’t allowed to change the schedule, he told me, and the administrators with access to it wouldn’t be reachable until morning.
I felt deflated. For hours, my attention had been consumed by challenges of coordination rather than actual patient care. And still the patient was at risk of experiencing delays for both of the things she needed—not for any medical reason, but simply because of an inflexible computer system and a poor workflow.
Situations like this are not rare, and they are vexing in part because they expose the widening gap between the ideal and reality of medicine. Doctors become doctors because they want to take care of patients. Their decade-long training focuses almost entirely on the substance of medicine—on diagnosing and treating illness. In practice, though, many of their challenges relate to the operations of medicine—managing a growing number of patients, coordinating care across multiple providers, documenting it all. Regulations governing the use of electronic medical records (EMRs), first introduced in the Health Information Technology for Economic and Clinical Health (HITECH) Act in 2009, have gotten more and more demanding, while expanded insurance coverage from the Affordable Care Act may have contributed to an uptrend in patient volume at many health centers. These changes are taking a toll on physicians: There’s some evidence that the administrative burden of medicine—and with it, the proportion of burned-out doctors—is on the rise. A study published last year in Health Affairs reported that from 2011 to 2014, physicians spent progressively more time on “desktop medicine” and less on face-to-face patient care. Another study found that the percentage of physicians reporting burnout increased over the same period; by 2014, more than half said they were affected.
To understand how burnout arises, imagine a young chef. At the restaurant where she works, Bistro Med, older chefs are retiring faster than new ones can be trained, and the customer base is growing, which means she has to cook more food in less time without compromising quality. This tall order is made taller by various ancillary tasks on her plate: bussing tables, washing dishes, coordinating with other chefs so orders aren’t missed, even calling the credit-card company when cards get declined.
Then the owners announce that to get paid for her work, this chef must document everything she cooks in an electronic record. The requirement sounds reasonable at first but proves to be a hassle of bewildering proportions. She can practically make eggs Benedict in her sleep, but enter “egg” into the computer system? Good luck. There are separate entries for white and brown eggs; egg whites, yolks, or both; cage-free and non-cage-free; small, medium, large, and jumbo. To log every ingredient, she ends up spending more time documenting her preparation than actually preparing the dish. And all the while, the owners are pressuring her to produce more and produce faster.
It wouldn’t be surprising if, at some point, the chef decided to quit. Or maybe she doesn’t quit—after all, she spent all those years in training—but her declining morale inevitably affects the quality of her work.
In medicine, burned-out doctors are more likely to make medical errors, work less efficiently, and refer their patients to other providers, increasing the overall complexity (and with it, the cost) of care. They’re also at high risk of attrition: A survey of nearly 7,000 U.S. physicians, published last year in the Mayo Clinic Proceedings, reported that one in 50 planned to leave medicine altogether in the next two years, while one in five planned to reduce clinical hours over the next year. Physicians who self-identified as burned out were more likely to follow through on their plans to quit.
What makes the burnout crisis especially serious is that it is hitting us right as the gap between the supply and demand for health care is widening: A quarter of U.S. physicians are expected to retire over the next decade, while the number of older Americans, who tend to need more health care, is expected to double by 2040. While it might be tempting to point to the historically competitive rates of medical-school admissions as proof that the talent pipeline for physicians won’t run dry, there is no guarantee. Last year, for the first time in at least a decade, the volume of medical school applications dropped—by nearly 14,000, according to data from the Association of American Medical Colleges. By the association’s projections, we may be short 100,000 physicians or more by 2030.
Some are trying to address the projected deficiency by increasing the number of practicing doctors. The Resident Physician Shortage Reduction Act, legislation introduced last year in Congress, would add 15,000 residency spots over a five-year period. Certain medical schools have reduced their duration, and some residency programs are offering opportunities for earlier specialization, effectively putting trainees to work sooner. But these efforts are unlikely to be sufficient. A second strategy becomes vital: namely, improving the workflow of medicine so that physicians are empowered to do their job well and derive satisfaction from it.
Just as chefs are most valuable when cooking, doctors are most valuable when doing what they were trained to do—treating patients. Likewise, non-physicians are better suited to accomplish many of the tasks that currently fall upon physicians. The use of medical scribes during clinic visits, for instance, not only frees doctors to talk with their patients but also potentially yields better documentation. A study published last month in the World Journal of Urology reported that the introduction of scribes in a urology practice significantly increased physician efficiency, work satisfaction, and revenue.
Meanwhile, there’s evidence that patients are more satisfied with their care when nurse practitioners or physician assistants provide some of it. This may be because these non-physicians spend more time than doctors on counseling patients and answering questions. In a perfectly efficient division of labor, physicians might focus on formulating diagnoses and treatment plans, with non-physicians overseeing routine health maintenance, discussing lifestyle changes, and educating patients on their medical conditions and treatment needs. Fortunately, over the next decade, employment of nurse practitioners and physician assistants in the United States is expected to grow by more than 30 percent; that compares with overall expected job growth of just 7 percent.
Yet the solution to health care’s labor problem isn’t simply to hire more staff; if not done right, that could make coordination even more cumbersome. A health-care organization’s success, in the years ahead, will depend on its success at delegating responsibilities among physicians and non-physicians, training the non-physicians to do their work independently, and empowering everyone—not just doctors—to shape a patient’s care and be accountable for the results.
Technology can make doctors’ lives easier, but also a lot harder. Consider the internet: It’s made information infinitely more attainable, but it takes time to find what one needs and to filter the accurate material from the inaccurate. The same goes for medicine. Technologies such as telemedicine, which allows for online doctor visits, can make health care more accessible and effective. But the use of EMRs, which is now federally mandated, is frequently cited as one of the main contributors to burnout. EMRs are often designed with billing rather than patient care in mind, and they can be frustrating and time-consuming to navigate. One attending doctor I know, tired of wading through a morass of irrelevant information, writes notes in the electronic chart but in parallel keeps summaries of his patients’ medical histories on hand-written index cards.
One can imagine a better EMR system, built around what health-care providers need. Today, in the absence of more effective tools, medical colleagues rely on email to coordinate patient care—or phone, as in the case of my kidney patient. But email chains can get buried in an inbox, and phone calls are rarely practical for coordinating between more than two people at a time. Neither mode of communication gets linked to a patient’s record, which means work is at risk of either getting lost or being replicated. But what if we were to integrate a tool into the electronic record that made clear what a patient’s active medical issues were, assigned responsibility to providers for overseeing those issues, and helped them to coordinate with each other? A dynamic EMR that didn’t just give physicians more information, but also helped them to prioritize, share, and act upon that information, would be far more useful than what currently exists.
As the world changes—as populations grow and technology advances—it is becoming essential that the workflow of medicine change alongside it. Fortunately for the patient with the failing kidney, the anesthesiologist was willing to get creative. Despite being unable to book the surgery, he unofficially reserved a slot for her and made the rest of his staff aware. The patient underwent the procedure the next morning, followed by her previously planned heart study. Everything worked out in the end. But I couldn’t help thinking: It shouldn’t be this hard to do the right thing.
from Health News And Updates https://www.theatlantic.com/health/archive/2018/05/the-burnout-crisis-in-health-care/559880/?utm_source=feed
0 notes
Text
The Burnout Crisis in American Medicine
During a recent evening on call in the hospital, I was asked to see an elderly woman with a failing kidney. She’d come in feeling weak and short of breath and had been admitted to the cardiology service because it seemed her heart wasn’t working right. Among other tests, she had been scheduled for a heart-imaging procedure the following morning; her doctors were worried that the vessels in her heart might be dangerously narrowed. But then they discovered that one of her kidneys wasn’t working, either. The ureter, a tube that drains urine from the kidney to the bladder, was blocked, and relieving the blockage would require minor surgery. This presented a dilemma. Her planned heart-imaging test would require contrast dye, which could only be given if her kidney function was restored—but surgery with a damaged heart was risky.
I went to the patient’s room, where I found her sitting alone in a reclining chair by the window, hands folded in her lap under a blanket. She smiled faintly when I walked in, but the creasing of her face was the only movement I detected. She didn’t look like someone who could bounce back from even a small misstep in care. The risks of surgery, and by extension the timing of it, would need to be considered carefully.
I called the anesthesiologist in charge of the operating room schedule to ask about availability. If the cardiology department cleared her for surgery, he said, he could fit her in the following morning. I then called the on-call cardiologist to ask whether it would be safe to proceed. He hesitated. “I’m just covering,” he said. “I don’t know her well enough to say one way or the other.” He offered to pass on the question to her regular cardiologist.
A while later, he called back: The regular cardiologist had given her blessing. After some more calls, the preparations were made. My work was done, I thought. But then the phone rang: It was the anesthesiologist, apologetic. “The computer system,” he said. “It’s not letting me book the surgery.” Her appointment for heart imaging, which had been made before her kidney problems were discovered, was still slated for the following morning; the system wouldn’t allow another procedure at the same time. So I called the cardiologist yet again, this time asking him to reschedule the heart study. But doctors weren’t allowed to change the schedule, he told me, and the administrators with access to it wouldn’t be reachable until morning.
I felt deflated. For hours, my attention had been consumed by challenges of coordination rather than actual patient care. And still the patient was at risk of experiencing delays for both of the things she needed—not for any medical reason, but simply because of an inflexible computer system and a poor workflow.
Situations like this are not rare, and they are vexing in part because they expose the widening gap between the ideal and reality of medicine. Doctors become doctors because they want to take care of patients. Their decade-long training focuses almost entirely on the substance of medicine—on diagnosing and treating illness. In practice, though, many of their challenges relate to the operations of medicine—managing a growing number of patients, coordinating care across multiple providers, documenting it all. Regulations governing the use of electronic medical records (EMRs), first introduced in the Health Information Technology for Economic and Clinical Health (HITECH) Act in 2009, have gotten more and more demanding, while expanded insurance coverage from the Affordable Care Act may have contributed to an uptrend in patient volume at many health centers. These changes are taking a toll on physicians: There’s some evidence that the administrative burden of medicine—and with it, the proportion of burned-out doctors—is on the rise. A study published last year in Health Affairs reported that from 2011 to 2014, physicians spent progressively more time on “desktop medicine” and less on face-to-face patient care. Another study found that the percentage of physicians reporting burnout increased over the same period; by 2014, more than half said they were affected.
To understand how burnout arises, imagine a young chef. At the restaurant where she works, Bistro Med, older chefs are retiring faster than new ones can be trained, and the customer base is growing, which means she has to cook more food in less time without compromising quality. This tall order is made taller by various ancillary tasks on her plate: bussing tables, washing dishes, coordinating with other chefs so orders aren’t missed, even calling the credit-card company when cards get declined.
Then the owners announce that to get paid for her work, this chef must document everything she cooks in an electronic record. The requirement sounds reasonable at first but proves to be a hassle of bewildering proportions. She can practically make eggs Benedict in her sleep, but enter “egg” into the computer system? Good luck. There are separate entries for white and brown eggs; egg whites, yolks, or both; cage-free and non-cage-free; small, medium, large, and jumbo. To log every ingredient, she ends up spending more time documenting her preparation than actually preparing the dish. And all the while, the owners are pressuring her to produce more and produce faster.
It wouldn’t be surprising if, at some point, the chef decided to quit. Or maybe she doesn’t quit—after all, she spent all those years in training—but her declining morale inevitably affects the quality of her work.
In medicine, burned-out doctors are more likely to make medical errors, work less efficiently, and refer their patients to other providers, increasing the overall complexity (and with it, the cost) of care. They’re also at high risk of attrition: A survey of nearly 7,000 U.S. physicians, published last year in the Mayo Clinic Proceedings, reported that one in 50 planned to leave medicine altogether in the next two years, while one in five planned to reduce clinical hours over the next year. Physicians who self-identified as burned out were more likely to follow through on their plans to quit.
What makes the burnout crisis especially serious is that it is hitting us right as the gap between the supply and demand for health care is widening: A quarter of U.S. physicians are expected to retire over the next decade, while the number of older Americans, who tend to need more health care, is expected to double by 2040. While it might be tempting to point to the historically competitive rates of medical-school admissions as proof that the talent pipeline for physicians won’t run dry, there is no guarantee. Last year, for the first time in at least a decade, the volume of medical school applications dropped—by nearly 14,000, according to data from the Association of American Medical Colleges. By the association’s projections, we may be short 100,000 physicians or more by 2030.
Some are trying to address the projected deficiency by increasing the number of practicing doctors. The Resident Physician Shortage Reduction Act, legislation introduced last year in Congress, would add 15,000 residency spots over a five-year period. Certain medical schools have reduced their duration, and some residency programs are offering opportunities for earlier specialization, effectively putting trainees to work sooner. But these efforts are unlikely to be sufficient. A second strategy becomes vital: namely, improving the workflow of medicine so that physicians are empowered to do their job well and derive satisfaction from it.
Just as chefs are most valuable when cooking, doctors are most valuable when doing what they were trained to do—treating patients. Likewise, non-physicians are better suited to accomplish many of the tasks that currently fall upon physicians. The use of medical scribes during clinic visits, for instance, not only frees doctors to talk with their patients but also potentially yields better documentation. A study published last month in the World Journal of Urology reported that the introduction of scribes in a urology practice significantly increased physician efficiency, work satisfaction, and revenue.
Meanwhile, there’s evidence that patients are more satisfied with their care when nurse practitioners or physician assistants provide some of it. This may be because these non-physicians spend more time than doctors on counseling patients and answering questions. In a perfectly efficient division of labor, physicians might focus on formulating diagnoses and treatment plans, with non-physicians overseeing routine health maintenance, discussing lifestyle changes, and educating patients on their medical conditions and treatment needs. Fortunately, over the next decade, employment of nurse practitioners and physician assistants in the United States is expected to grow by more than 30 percent; that compares with overall expected job growth of just 7 percent.
Yet the solution to health care’s labor problem isn’t simply to hire more staff; if not done right, that could make coordination even more cumbersome. A health-care organization’s success, in the years ahead, will depend on its success at delegating responsibilities among physicians and non-physicians, training the non-physicians to do their work independently, and empowering everyone—not just doctors—to shape a patient’s care and be accountable for the results.
Technology can make doctors’ lives easier, but also a lot harder. Consider the internet: It’s made information infinitely more attainable, but it takes time to find what one needs and to filter the accurate material from the inaccurate. The same goes for medicine. Technologies such as telemedicine, which allows for online doctor visits, can make health care more accessible and effective. But the use of EMRs, which is now federally mandated, is frequently cited as one of the main contributors to burnout. EMRs are often designed with billing rather than patient care in mind, and they can be frustrating and time-consuming to navigate. One attending doctor I know, tired of wading through a morass of irrelevant information, writes notes in the electronic chart but in parallel keeps summaries of his patients’ medical histories on hand-written index cards.
One can imagine a better EMR system, built around what health-care providers need. Today, in the absence of more effective tools, medical colleagues rely on email to coordinate patient care—or phone, as in the case of my kidney patient. But email chains can get buried in an inbox, and phone calls are rarely practical for coordinating between more than two people at a time. Neither mode of communication gets linked to a patient’s record, which means work is at risk of either getting lost or being replicated. But what if we were to integrate a tool into the electronic record that made clear what a patient’s active medical issues were, assigned responsibility to providers for overseeing those issues, and helped them to coordinate with each other? A dynamic EMR that didn’t just give physicians more information, but also helped them to prioritize, share, and act upon that information, would be far more useful than what currently exists.
As the world changes—as populations grow and technology advances—it is becoming essential that the workflow of medicine change alongside it. Fortunately for the patient with the failing kidney, the anesthesiologist was willing to get creative. Despite being unable to book the surgery, he unofficially reserved a slot for her and made the rest of his staff aware. The patient underwent the procedure the next morning, followed by her previously planned heart study. Everything worked out in the end. But I couldn’t help thinking: It shouldn’t be this hard to do the right thing.
Article source here:The Atlantic
0 notes
Text
I was tagged by @penaltywaltz... well, sort of... I just stole it from her. X-)
Rules: tag 20 people
The Last:
1. Drink: Milk
2. Phone Call: My mom called me to tell me that my grandpa was coming home from the hospital today.
3. Text message: My friend in TX... I wanted to make sure he was gonna be OK since he’s in the path of Hurricane Harvey... he says he’s OK right now, thank God.
4. Song you listened to: “All the Wrong Things” by Branan Murphy ft. Koryn Hawthorne... it’s a beautiful song about admitting your faults and the sincere desire to change... give it a listen, I think you’ll love it. :-)
5. Time you cried: Yesterday... my boss ripped into me for telling him I was too sick to come into work, and he demanded I come in anyway, so I sucked it up and went to work, and it was a living hell of pain and nausea, then I stopped at my mother’s house because she picked up my prescription refills from the pharmacy for me, and I was greeted by my sister ripping into me because for some God-forsaken reason, she decided that my mother should come home from work and clean the house instead of visiting her own father in the hospital, and she decided that I’m selfish and narcissistic and that I don’t care about anyone else but myself for not stopping my mother from going. I just took the prescriptions, left the house, and broke down when I got back into my car. And I ended up missing work today because I’m still sick AND depressed out of my mind today. Way to lead up to my next mission trip in 3 weeks, eh?
Have You:
6. Dated someone twice: No
7. Kissed someone and regretted it: Yes
8. Been cheated on: Yes
9. Lost someone special: Yes
10. Been depressed: In the long list of diagnoses I have going on right now, depression and anxiety are among them.
11: Gotten drunk and thrown up: No... I don’t drink.
List 3 Favorite Colors:
12. Sapphire Blue
13. That teal color that you can’t quite tell if it’s blue or green
14: That indigo color that you can’t quite tell if it’s blue or purple
In the last year, have you…
15. Made new friends: Yes
16. Fallen out of love: Was never in love
17. Laughed until you cried: Yes
18. Found out someone was talking about you: Yes... one of my co-workers has been reporting every single thing I say to my boss behind my back, including the fact that I’m currently in the process of getting a concealed carry permit, which lead to a loud shouting match between me and the boss.
19. Met someone who changed you: Yes
20. Found out who your friends are: Yes
21. Kissed someone on your FB list: Sort of... Rocco isn’t technically on my FB list, but I have an entire album dedicated to pictures of him because he’s my little “fur-nephew” and I love him so much, and I kissed him on his little Beagle head when I saw him yesterday. :-)
GENERAL:
22. How many Facebook friends do you know in real life: Probably about 85%.
23. Do you have any pets: I have a “fur-nephew,” Rocco, does he count? :-)
24. Do you want to change your name: Sometimes I’d like to... I’m not exactly keen on being named after my abusive father.
25. What did you do for your last birthday: I had to work, and then I went to a local coffee house afterwards with my friend from church, and she gave me a Sherlock Holmes book for a birthday present. :-)
26. What time did you wake up: I got up at 11 because I was supposed to be at work at 12:30, but I was way too sick to do it, and I ended up spending the next 5 hours sitting on the floor in the bathroom with my phone and tablet in case anyone tried to contact me. No one did, of course.
27. What were you doing at midnight last night: The same thing I’m doing right now... Tumblring with the TV live streaming in the background.
28. Name something you can’t wait for: My next mission is happening in 3 weeks, and I can hardly believe it’s that close already!! :-D
29. When was the last time you saw your Mom: Actually saw her? Two days ago. But I’ve talked to her on the phone multiple times since.
30. What is one thing you wish you could change in your life: My health first and foremost, and a close second is my financial situation.
31. What are you listening to right now: “Salvation” by Skillet... it’s the Eurus and Sherlock song, seriously, check it out, it’s the perfect theme song for The Final Problem.
32. Have you ever talked to a person named Tom: My grandpa goes by Tom because his middle name is Thomas, I work with a sales guy named Tom, and I know two Tom’s from church.
33. Something that is getting on your nerves: My current situation in general. The stress is just piling on again when I’m trying to get packed and ready for my mission, and I need it to stop so I can concentrate on this.
34. Most visited website: Probably a tie between Tumblr and Facebook.
35. Mole/s: I have freckles of various shades of brown all over my paper-white skin, but only one on my left forearm is slightly raised like a mole.
36. Mark/s: My entire body is full of scars from the acne I had when I was a teenager, multiple cysts I had removed, and a significant amount of self harm in the form of stabbing my arms with sharp objects when I was in my late teens and early 20′s.
37. Childhood dream: I wanted to be a professional ballet dancer and an actress.
38. Hair color: The same as Benedict Cumberbatch’s natural hair color.
39. Long or short hair: A pixie cut that was supposed to look like Jennifer Lawerence’s, but because my hair turned curly once it got cut short, it actually looks like a cross between Daniel Jackson and Sherlock having a bad hair day. X-)
40. Do you have a crush on someone?: A fictional someone... X-)
41. What do you like about yourself: I dunno... the older I get, the more I feel like my greatest talent is the ability to take levels of abuse that other people could never handle.
42. Piercings: 3 in each earlobe and one 90′s cartilage pierce in my right ear.
43. Blood type: O+... as most people of Western European heritage are. X-)
44: Nicknames: Up until I was 30, everyone used to call me this particular word that used to make me blazingly, furiously angry, and I never understood why it did, but the angrier I got, the more people would say it because they thought it was funny to make me cry. Then when I was 30, my sister started questioning me as to why I got so infuriated at the sound of that word, so I started researching a few linguistic things online, trying to see if this word was truly made up as they claimed or if there was actually something to it. I managed to find the linguistic roots of the word, and it turns out it was actually an Albanian-influenced Italian curse meaning, “The Devil’s Ass,” with “ass” being in the context of a slave or a work donkey. Basically, they were cursing me to be a slave to the devil every time they called me that. Needless to say, I proceeded to angrily confront my family with the evidence I found, and told them that if any of them ever uttered that word to me, about me, or in any way, shape, or form of connection to me, that it would be the last time they ever see me for the rest of their lives. No one’s ever used a nickname for me ever again. And after that, they dang well better not.
45. Relationship status: Single... have been for 13 years, and honestly, I stopped looking for a relationship a looooong time ago.
46. Zodiac: Ophiuchus
47. Pronouns: She/Her
48. Favorite TV show(s): Stargate SG-1, Sherlock, Doctor Who, Star Trek in all it’s incarnations, Psych, and Saving Hope. I might be forgetting a couple, but those are the top of the list.
49. Tattoos: None yet, but I think I’m gonna get one for my 40th birthday in 2019... I wanna get an American eagle with it’s wing around a Central American quetzal to represent how much I love Central America and doing missions work there, and underneath them, “Mark 16:15-16,” which is what’s known as “The Great Commission” from the Bible.
50. Right or left hand: Right
51. Surgery: I had all the baby teeth and 4 permanent teeth removed from my mouth when I was 11, and I had 2 pilar cysts (so far) removed from my head... but there are 3 more cysts forming on my head, and they’re gonna get removed if/when they get big enough. Dermatologist said I’m gonna have to deal with the cyst problem for the rest of my life.
52. Hair dyed a different color: Never permanently, but I have done temporary dark brown and eggplant purple a few times.
53. Sports: Never was a sports fan... the only sports I actually like to watch is the Olympics and American Ninja Warrior, if that counts. X-)
54. Vacation: The last thing that could actually be described as a vacation was when my friend took me with her to NYC for 5 days because she was eager to cross it off her bucket list. Before that, it was in 2001, my mother, my sister, and I took a road trip to 2 states that were an 18-21 hour drive away just for two particular food festivals, and before that, my grandmother took my sister and me to Italy after I graduated high school in the summer of 1998. Every other place I’ve been to has been for mission work... missions are no vacation, they’re hard work, but they’re the most worth-it thing you’ll ever do in your life. :-)
55. Shoes: I have Sketchers work-shoes, a few pairs of canvas shoes, a few pairs of ballet flats, and 2 pairs of heels that I haven’t worn in over 5 years. But all the shoes that lace up, I laced them with either black or white elastic, so now all my shoes are slip-ons. :-)
56. Eating: I ate a bowl of vanilla yogurt with some chocolate BelVita biscuits about an hour ago.
57. Drinking: Nothing... I had a glass of milk earlier.
58. I’m about to: Back to Panama for my 9th mission in about 3 weeks... this has been the most disorganized and closely cut mission I’ve ever done, but the money came in, so now it’s actually happening!!
59. Waiting for: September 16th because that’s when we’re leaving for Panama... :-)
60. Want: My health back, and my finances in order.
61. Get married: If it happens, it happens. If it doesn’t, that’s fine, too. Either way, I’ll be perfectly OK.
62. Career: I’d love to be able to do this missions thing for a living, but the financial support isn’t there right now. I hope someday (soon!!) that it will be.
WHICH IS BETTER:
63. Hugs or kisses: Hugs
64. Lips or eyes: They’re both pretty essential for a functioning face, but I’d say eyes serve a more necessary function.
65. Shorter or taller: I’d like to be a couple of inches taller, maybe I might be if the scoliosis in my spine can ever be straightened out.
66. Older or younger: Physically I’d like to be younger, but intellectually, I’d like to be older and wiser.
67. Nice arms or nice stomach: My stomach has never been nice, even when I was at my skinniest, and I’ve always been OK with my arms, so I’d say I’d rather have my stomach be nicer looking.
68. Sensitive or loud: These aren’t mutually exclusive, so I think each has their place in the appropriate situations.
69. Hook up or relationship: Relationship. I don’t go for that momentary fun and then dump them off bull crap.
70. Troublemaker or hesitant: Actually... once again, not mutually exclusive, but... neither of these are characteristics I’m OK with.
HAVE YOU EVER:
71. Kissed a stranger: Not by choice.
72. Drank hard liquor: No
73. Lost glasses/contact lenses: An unfortunate number of times in my life.
74. Turned someone down: Yes
75. Sex on first date: Never
76. Broken someone’s heart: Once... but if he truly did love me and want to marry me, then he should’ve learned sooner that I wouldn’t stand for taking a backseat to his BFF for the rest of my life.
77. Had your heart broken: Yes
78. Been arrested: No
79. Cried when someone died: Yes
80. Fallen for a friend: Yes
DO YOU BELIEVE IN:
81. Yourself: There is, in fact, empirical evidence that I exist, despite so many people’s opinions to the contrary.
82. Miracles: Yes
83. Love at first sight: No... you can’t possibly learn what you need to know about a person in order to make the choice to love them from just one look.
84. Santa Claus: Every parental figure is a Santa Claus. :-)
85. Kiss on the first date: Not anymore. He’s gonna have to earn that.
OTHER:
86. Current best friend: I’m actually not sure. I hate to call someone a best friend who doesn’t think of me the same way, and I don’t believe that anyone thinks of me that way at the current moment.
87. Eye color: The same as Benedict Cumberbatch
88. Favorite movie: Probably a 3-way tie between Star Trek Into Darkness, Star Trek Beyond, and The Force Awakens.
I’m tagging everyone who sees this. Everyone, please copy, paste, fill it in, and tag me!! :-)
0 notes
Text
A ‘radical alternative’: how one human changed the insight of Los Angeles
In the 1960 s, British architectural commentator Reyner Banham swore his love for the city that his fellow eggheads detested. What Banham wrote about Los Angeles redefined how the world realized it but what would he think of LA today?
Now I know subjective rulings can diversify, the columnist Adam Raphael wrote in the Guardian in 1968, but personally I calculate LA as the noisiest, the smelliest, “the worlds largest” awkward and most uncivilised major city in the United States. In short, a smelling sewer …
Three years later, Raphaels terms appeared in periodical again as an epigraph of Reyner Banhams Los Angeles: The Architecture of Four Ecologies the most exuberantly pro-Los Angeles notebook further written. Ever since book, it has shown up on rolls of great volumes about modern metropolitans even those being prepared by people who consider Los Angeles anything but a great American city.
Somehow, this notebook that sucked so much of its initial publicity with stupor evaluate( In Praise (!) of Los Angeles, sneered the New York Times refreshes headline) has impeded its relevant through the decades, such that newly arrived Angelenos still read it to orient themselves. But what can it school us about the Los Angeles of today?
An architectural historian a decade into his profession when he firstly saw, Banham knew full-well that his fellow academics hated Los Angeles. How and why he himself passed so avidly to appreciate it constitutes the core question of his is currently working on the city, which culminated in this slim volume.
The many who were ready to cast doubt on the worth of business enterprises, he reflected in its final chapter, included a recognise Italian inventor and his wife who, on discovering that I was writing this notebook, doubted that anyone who cared for architecture could lower himself to such a project and walked away without a word further.
The project began when Banham accompanied his shaggy whisker and wonky teeth to Los Angeles and declared that he cherished the city with a fervour, in the words of novelist and Bradford-born Los Angeles expat Richard Rayner. Educating at the University of Southern California, who set him up in the Greene brethren architecturally hero-worship Gamble House in Pasadena, Banham had a privileged base from which to explore. But what “hes been gone” go looking for, and the way he wrote about what he saw and detected, redefined the behavior the intellectual macrocosm and then the wider world saw the city.
Reyner Banham with his shaggy beard and wonky teeth in 1968. Image: Peter Johns for the Guardian
Not that he swore his love right there on the tarmac at LAX. Banham initially knew the city incomprehensible a reply said that he shared many pundits, wrote Nigel Whiteley in such studies Reyner Banham: Historian of the Immediate Future.
Banham firstly attempted to publicly explain this cutting-edge metropolis, saturated across its enormous space with electronic devices, synthetic chemicals and televisions, in four 1968 BBC radio talks. He told of how “hes come to” tractions with LAs embodiment of the experimental: its experimental figure and infrastructure, the combinations of cultures it altered, and the experimental life-styles to which it gave rise.
But even an appreciator like Banham had his qualms with the result. In Los Angeles you tend to go to a particular neighbourhood to do a specific thought, to another to do another thing, and finally a long way back to your dwelling, and youve done 100 miles in the day, he deplored in the third talk. The distances and the trust on mechanical transportation leave no room for coincidence even for joyous coincidences. You scheme the working day in advance, curriculum your activities, and waive those random encounters with acquaintances and strangers that are traditionally one of the rewards of metropolitan life.
Nevertheless, to Banham this un-city-like municipality braced out a hope: The unique appreciate of Los Angeles what rouses, intrigues and sometimes repels me is that it renders radical alternatives to almost every urban concept in unquestioned currency.
In his subsequent landmark book, Banham itemized Los Angeles deviations from conventional urbanism, as well as from all the rules for civilised living as they have been understood by the pundits of modernity, with evident enjoy. It seemed to legitimise a example “youve already”, in a 1959 clause, proposed to supersede the old-time thought of a single dense core surrounded by a wall.
Civilised living in suburban LA. Picture: University of Southern California/ Corbis via Getty Images
Banham foresaw the city as scrambled egg, its shell broken open, its business yolk mixed with its domestic white, and everything spread across the landscape, its evenness disturbed only by occasional specialised sub-centres. A visitor to Los Angeles today might listen the city explained in only the same way: as a system of nodes, a constellation of metropolitan villages, an exercise in postmodern polycentrism.
Banham made another digit in the eye of conservatives who insisted that a city should have just one strong centre with his short section A Note on Downtown, which opens with the words, … because that is all downtown Los Angeles deserves.
From its fetishised organizations such as the Bradbury Building and Cathedral of Saint Vibiana to its brand new office towers in their standard livery of dark glass and sword, Banham wrote that everything stands as an unintegrated scrap in a downtown vistum that started to deteriorate long ago out of sheer irrelevance, as far as one can see.
The notebooks contrarianism indicates the contrarianism of Los Angeles itself, which, insofar as it plays the functions of a great city, in terms of length, cosmopolitan mode, artistic energy, international influence, unique way of life, and corporate identity[ proves that] all the most admired theoreticians of the current century, from the Futurists and Le Corbusier to Jane Jacobs and Sibyl Moholy-Nagy, ought to have wrong.
Filled with photos and charts, Banhams book on Los Angeles divides its subject up into the four ecologies of its subtitle: the beaches and beach townships of Surfurbia; the Foothills with their ever more elaborated and costly palaces; the utilitarian Plains of Id( the only parts of Los Angeles flat enough and assuming enough to compare with the cities of the Middle West) and the famous, then infamous, freeway organization he dubbed Autopia: a single intelligible neighbourhood, a coherent state of mind in which Angelenos spend the two calmest and most fruitful hours of their daily lives.
The 1893 Bradbury Building in downtown LA was an unintegrated scrap in Banhams seeings. Photo: Michele and Tom Grimm/ Alamy
Between assemblies on the citys ecologies, Banham examined the buildings found in them. Populist, stylistically promiscuous, tradition-agnostic and often purposely impermanent, Los Angeles architecture has, of all the citys components, drawn distain the longest. There is no reward for aesthetic morality here , no beating for aesthetic misdemeanour; nothing but a immense cosmic inattention, wrote the novelist James M. Cain in 1933.
More than 40 years later, Banham appreciated a stylistic reward of Tacoburger Aztec to Wavy-line Moderne, from Cape Cod to unsupported Jaoul vaults, from Gourmet Mansardic to Polynesian Gabled and even in boundary Modern Architecture.
He discussed at length the LA building known as the dingbat a two-storey walk-up apartment-block … improved of grove and stuccoed over, all identical at the back but inexpensively, elaborately, decorated up-front, emblazoned with an aspirational refer such as the Capri or the Starlet.
In characterizing dingbats as the true evidence of Los Angeles urban id, trying to be dealt with the unprecedented image of residential densities too high to be subsumed within the apparitions of homestead living, Banham diagnosed the central and prolonged strain, then as now, between wanting to grow outward and needing to grow upward.
Banham attracted out the implications of Los Angeles ostensibly disposable buildings not by venerating them , nor disparaging them, but simply by determining them as they were. Robert Venturi, Denise Scott Brown and Steven Izenour would advocate the same approaching in their own urban classic, Discovering from Las Vegas, published the subsequent year: Withholding decision may be used as a tool to do later decision more sensitive. This is a way of draw lessons from everything.
Still, even appreciators of Los Angeles might take issue with this method when Banhams non-judgmental attitude at least towards the aesthetics of American commercial-grade culture starts to look like advocacy for bad taste.
The self-absorbed and perfected Watts Towers. Photo: Hulton Archive/ Getty Images
Non-appreciators of Los Angeles surely did. The painter and critic Peter Plagens, columnist of an 11,000 -word excoriation in Artforum magazine entitled The Ecology of Evil, proceeded in so far as to label Banhams book dangerous: The hackers who do shopping centre, Hawaiian eateries and savings-and-loans, the dried-up civil servants in the separation of roads, and the legions of showbiz fringies will sleep a little easier and duty a lot harder now that their enterprises have been authenticated. In a more humane culture where Banhams doctrines would be measured against the subdividers assault of the estate and the leading specks in little kids lungs, the author are liable to be stood up against a wall and shot.
Uncowed, Banham followed the book by starring in Reyner Banham Loves Los Angeles, a 1972 television film that followed him through one day in the city that builds nonsense of biography and disintegrate all the rules, and induced within him a passion that goes beyond sense or rationale. Stops on the tour included Simon Rodias handmade Watts Towers( a totally self-absorbed and perfected shrine) to Los Angeles characteristic fiction of innocence( prominently recognized on all the maps in his journal ); the overgrown areas of the old-fashioned Pacific Electric Railways rusting railings that once tied the whole massive metropolitan together; the decrepit canals and beachside bodybuilding facilities of Venice; and a Sunset Boulevard drive-in burger joint.
There, Banham expected the painter Ed Ruscha, plainspoken and painstaking spectator of American urban cliche, what public buildings a guest should investigate. Ruscha recommended gas stations.
Banham pre-empted objections to Los Angeles urban model by claiming the formation matters very little, having already written that Los Angeles has no urban figure at all in the commonly accepted feel. Yet whatever it does have, he insisted, has induced a fascinating, and sometimes even efficient, prepared of emergent city phenomena.
Come the day when the pollution fate lastly condescends, he chronicled over aerial fires of Wilshire Boulevards double sequence of towers and frame-filling neighbourhoods of disconnected mansions, … when trafficking in human beings grinds to a halt and the private vehicle is banned from the street, quite a number of craftily residence citizens will be able to switch over to being pedestrians and appear no pain.
Cyclists on Venice Beach … though often of LA is not bike-friendly. Picture: Alamy
The end of the car in Los Angeles? Bold statements for “the mens” who announced Wilshire Boulevard one of the few great streets in the world where driving is a pleasure after having, like earlier generations of English intellectuals who school themselves Italian in order to read Dante in the original, “ve learned to” drive in order to read Los Angeles in the original.
But just as the languages sounds on wall street of Los Angeles have proliferated, its own language of mobility has changed there, as has much else besides. How legible would Banham, who perished in 1988 , now find it?
The smog that expected affliction of the citys postwar decades which he always downplayed has all but vanished. The season of apparently limitless seat to please an obsession with single-family dwells has given behavior to one of construction cranes budding to satisfy the new is asking for high-density horizontal living. They stand not only over a downtown rise miraculously from the dead, but the specialised sub-centres scattered all over greater Los Angeles.
Though the ban on private cars hasnt come yet , no most recent developments astounds any Angeleno who was there in the 1970 s more than the citys new railing transport system, which started to rise almost 30 years after the conclusion of its Pacific Electric. It ranks as such as a success of funding, planning and execution( at least by the globally unimpressive American standard) that the rest of the country now ogles to Los Angeles as an example of how to build public transportation and, increasingly, public infinite in general.
Readers might scoff at Banham calling the Los Angeles freeway network one of “the worlds largest” handiworks of human but he has demonstrated more of an ability to see beyond it than many current beholders of Los Angeles. Even though it is vastly better than any other motorway method of my relationship, he wrote, it is inconceivable to Angelenos that it should not be replaced by an even better arrangement nearer to the perfection they are always seeking.
Banham detected downtown Los Angeles merely deserved a short chapter dedicated to it. Photograph: Alamy
Banham also foresaw the rise of the self-driving car, so often mooted these days as an alternative solution to Los Angeles traffic woes. But cars that drive themselves( as distinct from Baede-kar a then-fantastical singer navigation system dreamed up for Banhams TV doc, that allows an uncanny resemblance to those every American driver uses today) “re coming with” difficulties that Banham also prophesied all those years ago. The marginal increases in economy through automation, he wrote, might be offset by the psychological destitutions caused by destroying the residual illusions of free decision and driving skill.
Under each outwardly celebratory sheet of Banhams book lies the notion of change as Los Angeles simply constant: no matter how excitingly modern the car and the freeway, the working day will come to an end; no matter how comfortably idyllic the separated residence, it extremely must fall out of prefer, or into impracticality, sooner or later.
Some of the elements that gleaned Banhams attention have, after their own periods of infamy, changed fashionable again. Even the humble dingbat has discovered a target in the future of the city, becoming the object of critical investigate and architectural contender.
Banham also appreciated the future of Los Angeles in other unprepossessing structures, especially one stunning and elegantly simple-minded stucco carton on La Cienega Boulevard. Its architect? A certain Frank Gehry, then nearly unknown but now one of the most powerful influencers of the constructed home in not only Los Angeles( his current high-profile projection implies re-making the citys famously dry, concrete-encased river ), but other metropolitans as well. The Toronto-born starchitect became his adopted hometowns architectural emissary just one of the myriad routes in which Los Angeles has influenced the rest of the metropolitan macrocosm.
These daytimes, the rest of the metropolitan nature also influences Los Angeles. No longer striving under the hallucinations of total exceptionalism that prevailed in Banhams day, it has, with its towers, teaches, ballparks and even bike-share plans, drew strides towards the liveability so demanded by 21 st-century urbanists. It now even resembles( if faintly) New York, Boston, London, and Paris those thoroughly strategy , non-experimental metropolis where, Banham lamented, warring pressure group cannot get out of one anothers hair why i am pressed together in a sacred labyrinth of cultural monuments and real estate values.
In its impressive offer to incorporate older metropolitan honours and play by the rules of good urban design, modern Los Angeles dismisses the opportunities offered by becoming a similarly sacred labyrinth at its jeopardy. Continuing Banhams Los Angeles: the Architecture of Four Ecologies on its syllabus will hopefully protect against the horrific fate of losing its rule-breaking experimental urban spirit.
The engineering-trained scribe viewed Los Angeles as a kind of machine. Though it has come in for a naughtily necessitated revamp of its interface in recent years , nothing has yet written a consumers manual more engaged in the city on its own terms as Banham did 45 years ago.
Follow Guardian Cities on Twitter and Facebook to join the discussion
The post A ‘radical alternative’: how one human changed the insight of Los Angeles appeared first on apsbicepstraining.com.
from WordPress http://ift.tt/2sCpw23
via IFTTT
0 notes
Link
Editor’s note: Teaching Tolerance generally uses people-first language. The individuals interviewed for this story, however, prefer the term autistic people rather than people with autism. Out of respect for their preference, we have adjusted our usage.
School was never easy and rarely pleasant for Elly Wong. Their* smarts were not a question. They had learned to read by age 3, and grade school teachers suggested they skip a grade. But social interactions were difficult and classroom settings often battered their senses. “I’m sensitive to noise and get easily overstimulated,” Wong says. “My strongest impressions of elementary school are constant crying in response to being overwhelmed.” As the meltdowns continued into high school, a counselor recommended a psychological evaluation.
By that time, Wong had been doing independent research “through the magic of the Internet” and piecing together clues for a self-diagnosis. The psychiatrist agreed: anxiety, depression and Autism Spectrum Disorder (ASD). Wong proceeded to negotiate their own 504 plan; their parents knew little about autism and “the professionals at my school were pretty unhelpful.” The accommodations were relatively minor: Extra time on tests, use of noise-canceling headphones and subtitled videos were among them. Even so, Wong says, “I got constantly challenged over my accommodations.”
Last fall, they enrolled as a first-year student at Syracuse University in New York.
Working with and educating students like Wong who are on the autism spectrum has been the subject of much discussion and controversy in the last generation. The narrative has often been that children with these diagnoses are sources of tragedy for families and a drain on schools. Educators unfamiliar with autism and its range of expressions have often been perplexed and intimidated by students in their classrooms. Even as autism awareness has grown, many districts still lack the resources to help their teachers and schools update their practices and become more inclusive of affected students and families. Often, special education teachers must rely on their own research and resourcefulness.
In recent years, however, the neurodiversity movement, characterized by the advocacy of autistic individuals speaking for themselves, has entered the conversation. Advocates and their allies are eager to challenge pessimistic attitudes toward ASD and share insights for helping their fellow autistic people learn, cope and thrive in settings—particularly educational settings—that have often been indifferent, if not unwelcoming, to their needs.
“No one knows more about autism, about what it’s like to be autistic or what autistic people need, than autistic people ourselves,” says Julia Bascom, deputy executive director of the Autistic Self Advocacy Network (ASAN). “We have a unique first-person perspective, and that perspective absolutely has to be centered in any sort of advocacy work focused on our community.”
Old-School Autism Education
Though our understanding has grown significantly in recent years, the first diagnosis of autism as a distinct neurological disorder only occurred in the 1940s. Decades later, British psychiatrist Lorna Wing successfully made the case that autistic behaviors take different forms in different people, from nonspeaking individuals capable of little social engagement to those adept at navigating—or excelling—in society. Building on 1930s research by Austrian Hans Asperger, Wing described an “autism spectrum” and championed its 1980 inclusion in the bible of psychiatry, the Diagnostic and Statistical Manual of Mental Disorders, or DSM.
Today, ASD is viewed as a neurological disorder in a person’s ability to send social cues or process incoming ones. “By definition, autistic people have a language impairment,” says Sharon Rosenbloom, a speech pathologist, founder of Turning Pointe Autism Foundation and mother of Joey, an adult autistic son. “They’re neurologically disorganized.” Along with those issues, many autistics deal with high levels of anxiety and hypersensitivity to sensory stimulation.
Traditional autism therapy has emphasized teaching autistic kids to act as “normal” as possible. “We often see schools focusing on social skills training and behavior modification to make children appear less visibly autistic,” says ASAN’s Bascom. Unfortunately, these therapies have frequently come at the expense of engagement and learning.
Applied Behavior Analysis (ABA therapy) has been the cornerstone of traditional therapy. ABA therapy recommends 40 hours a week of repetitive drills and positive-reinforcement techniques to attempt to replace unwanted behaviors with more socially acceptable ones. For example, the teacher or therapist may work with an autistic child one-on-one to gradually build up his or her ability to maintain eye contact, perhaps rewarded with something like a sip of juice. Reducing self-stimulation—the flapping of hands, rhythmic rocking, fidgeting with a favorite object or other repetitive motions associated with autism—is also stressed. ABA works on verbal skills as well, promoting speech fluency in speaking students and having nonspeaking students pick out flash cards to develop the association between words and objects.
Critics of ABA therapies express frustration with their concentration on students’ deficits at the expense of celebrating their interests or strengths. Ido Kedar, a nonspeaking autistic teen, expresses his contempt for ABA in his book, Ido in Autismland. His deficits are not cognitive, but a self-described neurological disconnect between mind and body. “In school I sat through ABC tapes over and over and added 1 + 2 = 3 over and over,” he recalls. “I was bored out of my wits. It made me die inside. I was like a zombie inside because I had no hope.”
“Too often we teach autistic students using a deficit model—spending our time trying to fix what they can’t do instead of building out from what they can,” says Leah Kelley, a veteran special education teacher near Vancouver, British Columbia, and mother of an autistic son. “It’s a pathologized and medicalized model.”
It is past time to update and upgrade those models, says Kelley and other autism advocates and allies. More and more, the theories of medical experts and proponents of “cope till you cure” are being overwritten by the lived experiences of autistic kids and adults themselves. They want to share their narratives, and—thanks to new thinking in communication therapies as well as new assistive technologies—more are having the chance to tell them. An emerging theme? Autistics want help but are wary of people trying to “fix” them.
Multiple Methods
In his book, Kedar describes his early life as feeling trapped in an insubordinate body; not even those closest to him knew how to reach him. As a nonspeaking autistic, he had no words to call for help, and dyspraxia blocked him from being able to accurately signal his needs. His movements and actions often appeared impulsive and chaotic.
Kedar indicates the big breakthrough in his ability to express himself came at age 7. While trapped with his own thoughts, he had been learning to read. Now he also began to write, forming words with a letter board and—eventually—by typing. The process was painstaking, but it soon became clear that he was an aware and articulate kid with a strong desire to express himself. With the means to communicate, Ido progressed rapidly, and within two years was being mainstreamed in several of his middle school classes. Now in high school, he is reported to be on a college-bound track.
For many advocates and allies, matching autistic students with the means to communicate to the best of their ability is priority number one. But there is no one-size-fits-most fix, says Rosenbloom. She likens the process to being fitted for eyeglasses. “When I get the right prescription, I can see well,” she says. In the same way, any prescription to aid communication for those on the autism spectrum requires customization.
“Some of us will be able to speak fluently, but our speech may not match what we want to say, while others might not be able to use oral speech as well,” explains Bascom. “Autistic students should have multiple methods of communication made available to use, whether that looks like a dedicated speech-generating device, a text-to-speech app on an iPad, sign language, or a pencil and paper. But it’s not enough to just give someone access to an alternative; autistic students with communication impairments need qualified staff working with us who can systematically teach the hows and whys of communication as well.”
Presume Intellect
Bascom and Rosenbloom agree on another point when it comes to working with autistic students: Presume intellect. That means not talking about autistic students in the third person when they are present. That means speaking to them in tones and complete sentences appropriate for their age, not baby talk. Rosenbloom says she has witnessed autistic kids respond to a new teacher speaking to them normally with a look that says, “Whoa!”
“I have a mantra: Develop a relationship,” she says. “Presume there’s a mind in there, ready to teach you something you don’t know.”
Relating and communicating are practices that too often have been absent from autism education. Many autistic people are very aware when non-autistic educators are underestimating or patronizing them. Rosenbloom contends that respectful and meaningful interaction has the potential to reduce aggressive and self-injurious behaviors as autistic students learn to trust they can get their needs met without melting down.
Honoring that trust is another part of helping autistic individuals connect with the world. After years of acquiescing to the wills of others, many have developed understandable stores of resentment toward ableist attitudes. They need to be able to say "no" to what is being asked and trust it will be respected, says Kelley, who argues that better treatment for autistic people is a matter of social justice. “We dehumanize people when we don’t let them say 'no.' So much of their therapy has been compliance based, which is a real denial of dissent. Unless you allow dissent, whatever 'yes' you get is absolutely meaningless.”
This position echoes the motto of ASAN: “Nothing About Us Without Us.” More and more autistic young people and adults—like Elly Wong, Julie Bascom and Ido Kedar—are ready and determined to inform improvements in educational policies and practices that affect them and other neurodiverse students. Their contributions to more inclusive schools can only benefit us all, wherever we live on the neurodiversity spectrum.
*Wong’s preferred pronoun is they.
Two recent books, NeuroTribes by Steve Silberman and In a Different Key by John Donvan and Caren Zucker, offer compelling narrative histories of the scientific and social explorations of autism’s complexities and perplexities.
Glossary of Autism-related Terms
Applied Behavioral Analysis (ABA)
Therapies targeted to increase or decrease specific behaviors
Asperger syndrome
A disorder on the autism spectrum, distinguished by relatively intact language and cognitive skills; as of 2013, Asperger syndrome was eliminated as a distinct diagnosis and folded into the autism spectrum
Assistive and adaptive technology
Devices or equipment used to facilitate functional capabilities of people with disabilities; for autistics, these may include computer tablets and software to aid communication
Dyspraxia
Difficulty with coordination and motor planning
High-functioning/low-functioning autism
Terms traditionally used to describe the severity of autism in individuals; autism advocates now reject this usage
Neurodiversity
The concept that neurological differences in people represent normal, natural variations; many autism advocates embrace this term as a way to challenge pathologized models of autism
Prompt
A cue or hint to assist communication or behavior by autistic students
“Stimming”
Self-stimulating behavior; repetitive movements or vocalizations common in autistic individuals as a means for calming or entertaining themselves
Tactile defensiveness
Extreme sensitivity to specific textural stimuli
0 notes
Text
A ‘radical alternative’: how one human changed the insight of Los Angeles
In the 1960 s, British architectural commentator Reyner Banham swore his love for the city that his fellow eggheads detested. What Banham wrote about Los Angeles redefined how the world realized it but what would he think of LA today?
Now I know subjective rulings can diversify, the columnist Adam Raphael wrote in the Guardian in 1968, but personally I calculate LA as the noisiest, the smelliest, “the worlds largest” awkward and most uncivilised major city in the United States. In short, a smelling sewer …
Three years later, Raphaels terms appeared in periodical again as an epigraph of Reyner Banhams Los Angeles: The Architecture of Four Ecologies the most exuberantly pro-Los Angeles notebook further written. Ever since book, it has shown up on rolls of great volumes about modern metropolitans even those being prepared by people who consider Los Angeles anything but a great American city.
Somehow, this notebook that sucked so much of its initial publicity with stupor evaluate( In Praise (!) of Los Angeles, sneered the New York Times refreshes headline) has impeded its relevant through the decades, such that newly arrived Angelenos still read it to orient themselves. But what can it school us about the Los Angeles of today?
An architectural historian a decade into his profession when he firstly saw, Banham knew full-well that his fellow academics hated Los Angeles. How and why he himself passed so avidly to appreciate it constitutes the core question of his is currently working on the city, which culminated in this slim volume.
The many who were ready to cast doubt on the worth of business enterprises, he reflected in its final chapter, included a recognise Italian inventor and his wife who, on discovering that I was writing this notebook, doubted that anyone who cared for architecture could lower himself to such a project and walked away without a word further.
The project began when Banham accompanied his shaggy whisker and wonky teeth to Los Angeles and declared that he cherished the city with a fervour, in the words of novelist and Bradford-born Los Angeles expat Richard Rayner. Educating at the University of Southern California, who set him up in the Greene brethren architecturally hero-worship Gamble House in Pasadena, Banham had a privileged base from which to explore. But what “hes been gone” go looking for, and the way he wrote about what he saw and detected, redefined the behavior the intellectual macrocosm and then the wider world saw the city.
Reyner Banham with his shaggy beard and wonky teeth in 1968. Image: Peter Johns for the Guardian
Not that he swore his love right there on the tarmac at LAX. Banham initially knew the city incomprehensible a reply said that he shared many pundits, wrote Nigel Whiteley in such studies Reyner Banham: Historian of the Immediate Future.
Banham firstly attempted to publicly explain this cutting-edge metropolis, saturated across its enormous space with electronic devices, synthetic chemicals and televisions, in four 1968 BBC radio talks. He told of how “hes come to” tractions with LAs embodiment of the experimental: its experimental figure and infrastructure, the combinations of cultures it altered, and the experimental life-styles to which it gave rise.
But even an appreciator like Banham had his qualms with the result. In Los Angeles you tend to go to a particular neighbourhood to do a specific thought, to another to do another thing, and finally a long way back to your dwelling, and youve done 100 miles in the day, he deplored in the third talk. The distances and the trust on mechanical transportation leave no room for coincidence even for joyous coincidences. You scheme the working day in advance, curriculum your activities, and waive those random encounters with acquaintances and strangers that are traditionally one of the rewards of metropolitan life.
Nevertheless, to Banham this un-city-like municipality braced out a hope: The unique appreciate of Los Angeles what rouses, intrigues and sometimes repels me is that it renders radical alternatives to almost every urban concept in unquestioned currency.
In his subsequent landmark book, Banham itemized Los Angeles deviations from conventional urbanism, as well as from all the rules for civilised living as they have been understood by the pundits of modernity, with evident enjoy. It seemed to legitimise a example “youve already”, in a 1959 clause, proposed to supersede the old-time thought of a single dense core surrounded by a wall.
Civilised living in suburban LA. Picture: University of Southern California/ Corbis via Getty Images
Banham foresaw the city as scrambled egg, its shell broken open, its business yolk mixed with its domestic white, and everything spread across the landscape, its evenness disturbed only by occasional specialised sub-centres. A visitor to Los Angeles today might listen the city explained in only the same way: as a system of nodes, a constellation of metropolitan villages, an exercise in postmodern polycentrism.
Banham made another digit in the eye of conservatives who insisted that a city should have just one strong centre with his short section A Note on Downtown, which opens with the words, … because that is all downtown Los Angeles deserves.
From its fetishised organizations such as the Bradbury Building and Cathedral of Saint Vibiana to its brand new office towers in their standard livery of dark glass and sword, Banham wrote that everything stands as an unintegrated scrap in a downtown vistum that started to deteriorate long ago out of sheer irrelevance, as far as one can see.
The notebooks contrarianism indicates the contrarianism of Los Angeles itself, which, insofar as it plays the functions of a great city, in terms of length, cosmopolitan mode, artistic energy, international influence, unique way of life, and corporate identity[ proves that] all the most admired theoreticians of the current century, from the Futurists and Le Corbusier to Jane Jacobs and Sibyl Moholy-Nagy, ought to have wrong.
Filled with photos and charts, Banhams book on Los Angeles divides its subject up into the four ecologies of its subtitle: the beaches and beach townships of Surfurbia; the Foothills with their ever more elaborated and costly palaces; the utilitarian Plains of Id( the only parts of Los Angeles flat enough and assuming enough to compare with the cities of the Middle West) and the famous, then infamous, freeway organization he dubbed Autopia: a single intelligible neighbourhood, a coherent state of mind in which Angelenos spend the two calmest and most fruitful hours of their daily lives.
The 1893 Bradbury Building in downtown LA was an unintegrated scrap in Banhams seeings. Photo: Michele and Tom Grimm/ Alamy
Between assemblies on the citys ecologies, Banham examined the buildings found in them. Populist, stylistically promiscuous, tradition-agnostic and often purposely impermanent, Los Angeles architecture has, of all the citys components, drawn distain the longest. There is no reward for aesthetic morality here , no beating for aesthetic misdemeanour; nothing but a immense cosmic inattention, wrote the novelist James M. Cain in 1933.
More than 40 years later, Banham appreciated a stylistic reward of Tacoburger Aztec to Wavy-line Moderne, from Cape Cod to unsupported Jaoul vaults, from Gourmet Mansardic to Polynesian Gabled and even in boundary Modern Architecture.
He discussed at length the LA building known as the dingbat a two-storey walk-up apartment-block … improved of grove and stuccoed over, all identical at the back but inexpensively, elaborately, decorated up-front, emblazoned with an aspirational refer such as the Capri or the Starlet.
In characterizing dingbats as the true evidence of Los Angeles urban id, trying to be dealt with the unprecedented image of residential densities too high to be subsumed within the apparitions of homestead living, Banham diagnosed the central and prolonged strain, then as now, between wanting to grow outward and needing to grow upward.
Banham attracted out the implications of Los Angeles ostensibly disposable buildings not by venerating them , nor disparaging them, but simply by determining them as they were. Robert Venturi, Denise Scott Brown and Steven Izenour would advocate the same approaching in their own urban classic, Discovering from Las Vegas, published the subsequent year: Withholding decision may be used as a tool to do later decision more sensitive. This is a way of draw lessons from everything.
Still, even appreciators of Los Angeles might take issue with this method when Banhams non-judgmental attitude at least towards the aesthetics of American commercial-grade culture starts to look like advocacy for bad taste.
The self-absorbed and perfected Watts Towers. Photo: Hulton Archive/ Getty Images
Non-appreciators of Los Angeles surely did. The painter and critic Peter Plagens, columnist of an 11,000 -word excoriation in Artforum magazine entitled The Ecology of Evil, proceeded in so far as to label Banhams book dangerous: The hackers who do shopping centre, Hawaiian eateries and savings-and-loans, the dried-up civil servants in the separation of roads, and the legions of showbiz fringies will sleep a little easier and duty a lot harder now that their enterprises have been authenticated. In a more humane culture where Banhams doctrines would be measured against the subdividers assault of the estate and the leading specks in little kids lungs, the author are liable to be stood up against a wall and shot.
Uncowed, Banham followed the book by starring in Reyner Banham Loves Los Angeles, a 1972 television film that followed him through one day in the city that builds nonsense of biography and disintegrate all the rules, and induced within him a passion that goes beyond sense or rationale. Stops on the tour included Simon Rodias handmade Watts Towers( a totally self-absorbed and perfected shrine) to Los Angeles characteristic fiction of innocence( prominently recognized on all the maps in his journal ); the overgrown areas of the old-fashioned Pacific Electric Railways rusting railings that once tied the whole massive metropolitan together; the decrepit canals and beachside bodybuilding facilities of Venice; and a Sunset Boulevard drive-in burger joint.
There, Banham expected the painter Ed Ruscha, plainspoken and painstaking spectator of American urban cliche, what public buildings a guest should investigate. Ruscha recommended gas stations.
Banham pre-empted objections to Los Angeles urban model by claiming the formation matters very little, having already written that Los Angeles has no urban figure at all in the commonly accepted feel. Yet whatever it does have, he insisted, has induced a fascinating, and sometimes even efficient, prepared of emergent city phenomena.
Come the day when the pollution fate lastly condescends, he chronicled over aerial fires of Wilshire Boulevards double sequence of towers and frame-filling neighbourhoods of disconnected mansions, … when trafficking in human beings grinds to a halt and the private vehicle is banned from the street, quite a number of craftily residence citizens will be able to switch over to being pedestrians and appear no pain.
Cyclists on Venice Beach … though often of LA is not bike-friendly. Picture: Alamy
The end of the car in Los Angeles? Bold statements for “the mens” who announced Wilshire Boulevard one of the few great streets in the world where driving is a pleasure after having, like earlier generations of English intellectuals who school themselves Italian in order to read Dante in the original, “ve learned to” drive in order to read Los Angeles in the original.
But just as the languages sounds on wall street of Los Angeles have proliferated, its own language of mobility has changed there, as has much else besides. How legible would Banham, who perished in 1988 , now find it?
The smog that expected affliction of the citys postwar decades which he always downplayed has all but vanished. The season of apparently limitless seat to please an obsession with single-family dwells has given behavior to one of construction cranes budding to satisfy the new is asking for high-density horizontal living. They stand not only over a downtown rise miraculously from the dead, but the specialised sub-centres scattered all over greater Los Angeles.
Though the ban on private cars hasnt come yet , no most recent developments astounds any Angeleno who was there in the 1970 s more than the citys new railing transport system, which started to rise almost 30 years after the conclusion of its Pacific Electric. It ranks as such as a success of funding, planning and execution( at least by the globally unimpressive American standard) that the rest of the country now ogles to Los Angeles as an example of how to build public transportation and, increasingly, public infinite in general.
Readers might scoff at Banham calling the Los Angeles freeway network one of “the worlds largest” handiworks of human but he has demonstrated more of an ability to see beyond it than many current beholders of Los Angeles. Even though it is vastly better than any other motorway method of my relationship, he wrote, it is inconceivable to Angelenos that it should not be replaced by an even better arrangement nearer to the perfection they are always seeking.
Banham detected downtown Los Angeles merely deserved a short chapter dedicated to it. Photograph: Alamy
Banham also foresaw the rise of the self-driving car, so often mooted these days as an alternative solution to Los Angeles traffic woes. But cars that drive themselves( as distinct from Baede-kar a then-fantastical singer navigation system dreamed up for Banhams TV doc, that allows an uncanny resemblance to those every American driver uses today) “re coming with” difficulties that Banham also prophesied all those years ago. The marginal increases in economy through automation, he wrote, might be offset by the psychological destitutions caused by destroying the residual illusions of free decision and driving skill.
Under each outwardly celebratory sheet of Banhams book lies the notion of change as Los Angeles simply constant: no matter how excitingly modern the car and the freeway, the working day will come to an end; no matter how comfortably idyllic the separated residence, it extremely must fall out of prefer, or into impracticality, sooner or later.
Some of the elements that gleaned Banhams attention have, after their own periods of infamy, changed fashionable again. Even the humble dingbat has discovered a target in the future of the city, becoming the object of critical investigate and architectural contender.
Banham also appreciated the future of Los Angeles in other unprepossessing structures, especially one stunning and elegantly simple-minded stucco carton on La Cienega Boulevard. Its architect? A certain Frank Gehry, then nearly unknown but now one of the most powerful influencers of the constructed home in not only Los Angeles( his current high-profile projection implies re-making the citys famously dry, concrete-encased river ), but other metropolitans as well. The Toronto-born starchitect became his adopted hometowns architectural emissary just one of the myriad routes in which Los Angeles has influenced the rest of the metropolitan macrocosm.
These daytimes, the rest of the metropolitan nature also influences Los Angeles. No longer striving under the hallucinations of total exceptionalism that prevailed in Banhams day, it has, with its towers, teaches, ballparks and even bike-share plans, drew strides towards the liveability so demanded by 21 st-century urbanists. It now even resembles( if faintly) New York, Boston, London, and Paris those thoroughly strategy , non-experimental metropolis where, Banham lamented, warring pressure group cannot get out of one anothers hair why i am pressed together in a sacred labyrinth of cultural monuments and real estate values.
In its impressive offer to incorporate older metropolitan honours and play by the rules of good urban design, modern Los Angeles dismisses the opportunities offered by becoming a similarly sacred labyrinth at its jeopardy. Continuing Banhams Los Angeles: the Architecture of Four Ecologies on its syllabus will hopefully protect against the horrific fate of losing its rule-breaking experimental urban spirit.
The engineering-trained scribe viewed Los Angeles as a kind of machine. Though it has come in for a naughtily necessitated revamp of its interface in recent years , nothing has yet written a consumers manual more engaged in the city on its own terms as Banham did 45 years ago.
Follow Guardian Cities on Twitter and Facebook to join the discussion
The post A ‘radical alternative’: how one human changed the insight of Los Angeles appeared first on apsbicepstraining.com.
from WordPress http://ift.tt/2sCpw23
via IFTTT
0 notes
Last Seen Blogs

butterflym089
Diana Butterfly


daddysbighardcock
DBHC

mrrskyphotos
Mrr.Sky

quelragazzotantosolo
quelragazzotantosolo