#nhs emergency funds now
Text
By: Christina Buttons
Published: May 13, 2024
A guide to the international debate on youth medical transition, where medical authorities in the United States depart from a growing international consensus.
The world is reacting to the U.K.'s Cass Review and associated systematic evidence reviews, which found "remarkably weak" evidence supporting medical interventions for gender transition in minors. Released on April 9, 2024, the final report from the national gender clinic service for those under 18—following four years of meta-analyses of the available literature—dealt a major blow to the gender-affirming model of care and marked its termination in England.
NHS England, which commissioned the report, expressed gratitude to Dr. Hilary Cass and committed to implementing her recommendations. These advocate for primarily relying on psychotherapy to address gender-related distress in minors and discontinuing the use of puberty blockers as part of England’s publicly funded healthcare system. The NHS predicted the landmark review would have "major international importance and significance"—a prediction that has proven correct. Just one month later, we are already beginning to see its impact.
What’s New
Scotland and Wales
In response to the Cass Review, Wales and Scotland have joined England in halting new prescriptions of puberty blockers for minors under 18 diagnosed with gender dysphoria. Additionally, in Scotland, cross-sex hormones will not be available to those under 18. In the last few years, beyond the U.K., Sweden, Finland, and Denmark have adopted a more cautious approach by placing restrictions on medical interventions for the treatment of gender dysphoria in minors. Norway has also signaled intentions to follow a similar path.
Germany
Now, Germany has emerged as the latest country to initiate steps towards placing restrictions on gender transition treatments for minors. Earlier this week, the German Medical Assembly, a pivotal body representing medical professionals across the country, passed a resolution that calls for the restriction of puberty blockers, cross-sex hormones, and surgeries for gender dysphoric youth to strictly controlled research settings. Another resolution passed that stated minors should not be permitted to "self-identify" into a chosen sex without first undergoing a specialist child and adolescent psychiatric evaluation and consultation.
While national restrictions have not yet been formalized, experts in gender medicine research are describing this update as a “major development” — especially considering that Germany has been one of the most permissive countries on this issue.
Read the SEGM Analysis
Belgium
Additionally, in Belgium, leading physicians are advocating for significant reforms in the treatment protocols for gender dysphoria in children and adolescents. According to an April 2024 report authored by pediatricians and psychiatrists P. Vankrunkelsven, K. Casteels, and J. De Vleminck from Leuven, there is a pressing need to follow the precedents set by Sweden and Finland, where hormones are regarded as a last resort. Their findings and recommendations were published in a prestigious medical journal associated with Dutch-speaking medical faculties in Belgium and their alumni associations.
International Bodies
International bodies such as the United Nations (UN) have also responded to the Cass Review. The United Nations Special Rapporteur on violence against women and girls, Reem Alsalem, issued a statement on the UN’s website declaring that the Review’s recommendations are essential for protecting children, especially girls, from harm.
In addition, the European Society of Child and Adolescent Psychiatry (ESCAP), a prominent umbrella association of 36 Child and Adolescent Psychiatry societies worldwide, recently issued a policy statement on child and adolescent gender dysphoria. They urged healthcare providers to "not to promote experimental and unnecessarily invasive treatments with unproven psycho-social effects and, therefore, to adhere to the ‘primum-nil-nocere’ (first, do no harm) principle."
These responses stand in stark contrast to that of World Professional Association for Transgender Health (WPATH), a body-modification advocacy organization. WPATH emailed a statement to its subscribers in response to the Cass Review, vehemently rejecting its findings and adhering to its ideological beliefs. WPATH criticized the Cass Report as “harmful” and "rooted in a false premise" that suggests distressed children can be helped without "medical pathways.”
United States
In response to the Cass Review, the American Academy of Pediatrics (AAP) and the Endocrine Society (ES) recently provided statements to WBUR, doubling down on their endorsement of the gender-affirming model of care and medical interventions for minors. Both blamed “politics” for spreading “misinformation.” Meanwhile, prominent gender clinicians have expressed to WBUR that they are “perplexed and concerned” by these organizations’ statements, given the Cass Review’s findings.
WPATH, AAP, and ES continue to mislead the public by claiming that the gender-affirming model of care adheres to the principles of evidence-based medicine (EBM), despite clear evidence to the contrary. Their recommendations for medical interventions are not grounded in robust evidence but rather rely on "circular referencing" of each other’s guidelines, effectively creating a citation cartel.
Comprehensive Overview of the International Debate On Youth Transition by Country
In recent years, there has been an ongoing debate about the best approach for treating gender-distressed youth, addressing the global increase in young people, primarily adolescent females, seeking services from gender clinics. Countries with pediatric gender clinic services have shown varied responses, ranging from highly medicalized treatment pathways to approaches that prioritize psychotherapy.
Nations such as the UK, Sweden, Finland, and Denmark have taken unified steps to heavily restrict medical transitions for minors, aligning their guidance with the results of systematic evidence reviews, with Norway similarly indicating moves in this direction. Elsewhere, medical and health authorities remain divided on best practices, although there are signs of some reevaluating their positions on the medical transition of minors. This guide will highlight significant updates and changes observed in these practices over recent years.
The Netherlands
In the Netherlands, the birthplace of the Dutch Protocol—the highly medicalized approach to treating youth with gender dysphoria—is facing increased scrutiny. As of 2023, there is a growing debate within medical, legal, and cultural realms about the practice of youth gender transitions.
On February 15, 2024, the Dutch Parliament ordered an investigation into the physical and mental health outcomes of children who have been prescribed puberty blockers. Despite these developments, the guidelines for treating gender dysphoria have not yet been updated.
In April 2024, Amsterdam UMC, the Dutch clinic that pioneered youth gender transition practices, issued a statement in response to the Cass Report. The clinic commended several elements of the report but expressed disagreement with its conclusion that the evidence supporting the use of puberty blockers is insufficient.
In May 2024, one of the Netherlands' national newspapers profiled the new policy statement from The European Society of Child and Adolescent Psychiatry (ESCAP) that advocated for a non-medicalized approach to treating child and adolescent gender dysphoria.
Norway
In 2023, the Healthcare Investigation Board of Norway (Ukom) issued recommendations urging the Ministry of Health and Care to instruct the Directorate of Health to revise the national professional guideline for gender incongruence, drawing on systematic evidence reviews. Additionally, the Ukom report proposed classifying puberty blockers, as well as hormonal and surgical interventions for children and young people, as experimental treatments. This classification would subject these treatments to more stringent regulations regarding informed consent, eligibility, and outcome evaluation. However, Norway has not yet issued any explicit new guidelines following these recommendations.
Denmark
In July 2023, Ugeskrift for Læger, the journal of the Danish Medical Association, reported a significant shift in Denmark's approach to treating youth with gender dysphoria. Instead of receiving prescriptions for puberty blockers, hormones, or surgery, most young people referred to the centralized gender clinic now receive therapeutic counseling and support.
France
In 2022, the National Academy of Medicine in France advised exercising "the utmost medical caution" for the use of puberty blockers and cross-sex hormones for children and adolescents, citing the risk of regret. Despite this caution, the prescription of these treatments remains permissible at any age with parental authorization.
A 2023 poll by the Journal International de Médecine found 84% of healthcare professionals in France are in favor of a moratorium on the administration of hormonal treatments for trans-identified minors.
In March 2024, French senators released a 369-page report advocating for the cessation of cross-sex hormones and puberty blockers on minors. Based on the findings of this report, lawmakers have drafted a bill that is set to be debated on May 28, 2024.
Italy
In January 2023, the Italian Psychoanalytic Society (SPI) wrote a letter to Italian Prime Minister Giorgia Meloni, expressing "great concern" over the "ongoing experimentation" with drugs designed to halt puberty in children and calling for a "rigorous scientific discussion."
In March 2024, the Vatican’s doctrine office, after five years of preparation, released a report approved by Pope Francis that declared gender-related surgeries to be "a grave violation of human dignity."
In April 2024, five Italian medical organizations released a joint position paper on managing adolescent gender dysphoria. This document, which extensively references WPATH, supports the medical transition of minors.
Sweden
In 2022, Sweden's National Board of Health and Welfare declared that the potential harms of puberty blockers and gender-affirming hormone treatments for individuals under 18 years of age surpass the possible benefits for this demographic. The board recommended that such treatments should primarily occur within a research setting to better assess their effects on gender dysphoria, mental health, and quality of life among young people. Additionally, it noted that hormone treatments could still be administered in exceptional circumstances.
In April 2023, a systematic review conducted by researchers from Karolinska Institutet, University of Gothenburg, Umeå University, and the Swedish Agency for Health Technology Assessment and Assessment of Social Services was published in Acta Paediatrica. This review assessed the existing evidence on hormonal treatment for individuals under 18 years old with gender dysphoria. The researchers concluded that such interventions “should be considered experimental treatment rather than standard procedure.”
Finland
Finland was the first Western country to conduct a systematic review of the evidence for youth gender transition, that led to a significant update of its guidelines in 2020. Observations from Finnish gender clinics showed that hormone treatments do not typically improve—and can worsen—the functioning of gender-dysphoric youth. In response, the country's Council for Choices in Health Care revised its guidelines to emphasize psychosocial support as the primary approach and restricted hormonal interventions to exceptional cases. These interventions are permitted before age 18 only if the individual's cross-sex identity is confirmed as permanent and causes severe dysphoria, the child fully understands the significance, benefits, and risks of the treatments, and there are no contraindications.
In October 2023, Dr. Riittakerttu Kaltiala, a leading Finnish gender clinician and researcher at Tampere University Hospital, wrote an op-ed in The Free Press, titled "Gender-Affirming Care Is Dangerous. I Know Because I Helped Pioneer It.” She highlighted concerns about the practice of pediatric medical transition in the U.S. and the lack of solid evidence supporting the efficacy of medical transition in reducing suicide rates among young people.
In February 2023, a landmark study from Finland revealed low suicide rates among trans-identified youth and found no evidence of benefits from gender reassignment. The study showed that, after accounting for psychiatric needs, there was no statistically significant evidence that gender-referred youth have higher suicide rates compared to the general population. The authors concluded that the risk of suicide related to transgender identity and/or gender dysphoria "may have been overestimated."
England
In January 2020, National Health Service (NHS) England formed a Policy Working Group (PWG) to conduct an assessment of the existing research on the use of puberty blockers and feminizing/masculinizing hormones in children and young people with gender dysphoria. This was aimed at shaping a policy stance on their continued application. The findings from these reviews were released in March 2021.
In February 2022, the interim report to the Cass Review was published, which had been commissioned by NHS England to evaluate the Gender Identity Development Service (GIDS) at the Tavistock and Portman NHS Foundation Trust, the UK's only national clinic for children and adolescents with gender dysphoria. The review highlighted significant concerns about the clinical decision-making framework, noting a lack of robust evidence and consensus on the most effective treatments.
In July 2022, NHS England announced it would close GIDS in Spring 2023, which was delayed until Spring 2024. Two new regional hubs opened in London and the north of England to move away from a single-service model.
In October 2022, the NHS England issued new draft guidance following their systematic evidence review, stating that there is "scarce and inconclusive evidence to support clinical decision-making" for minors with gender dysphoria, and for most who present before puberty, it will be a "transient phase" requiring psychological support rather than medical intervention.
In March 2024, NHS England announced that it would end the prescription of puberty blockers at gender clinics for children due to insufficient evidence regarding their safety and effectiveness. These treatments will now only be accessible through clinical research trials.
On April 9, 2024, the final 388-page report of the Cass Review was published, along with 9 studies (8 of which were systematic evidence reviews) by the University of York.
Ireland
In March 2023, HSE published a review of the interim Cass Report to assess Gender Identity Services for children and young people in Ireland.
In April 2024, the Health Service Executive (HSE) announced the development of a new clinical program for gender healthcare, scheduled over the next two years. They also stated that the final report for the Cass Review will be included as part of this process.
Canada
In January 2024, Alberta announced the implementation of measures that significantly restrict medical transitions for minors. This policy establishes Alberta as the only province in Canada to enforce such limitations on gender transition procedures for individuals under 18. Under the new regulations, minors are prohibited from undergoing any gender-related surgeries, and those aged 16 and younger are prevented from accessing puberty blockers or cross-sex hormones.
United States
The three main organizations that have issued guidelines on youth medical transition include the American Academy of Pediatrics (AAP), the Endocrine Society (ES), and the World Professional Association for Transgender Health (WPATH). Other groups, such as the American Medical Association, have either publicly supported “affirming” medical practices without presenting evidence, or have aligned themselves with the guidelines set by one or more of these three organizations. Notably, none of these organizations have yet conducted systematic reviews of the evidence, which are designed to avoid selective inclusion of studies and biased interpretations.
Leaders at the American Academy of Pediatrics (AAP) ignored five resolutions from its members over four consecutive years, each urging that youth transition guidelines be aligned with findings from systematic evidence reviews. In August 2023, the AAP Board of Directors finally agreed to conduct their own systematic review of the evidence and consider updating its guidance. At the same time, the Board "voted to reaffirm" its 2018 policy statement on gender-affirming care.
In 2022, Florida took the lead as the first state to curtail the widespread administration of hormonal and surgical interventions to the increasing number of gender-dysphoric youth. Early in the year, Florida’s public health authority commissioned an overview of existing English-language systematic evidence reviews. Based on the findings from this review, the Florida Boards of Medicine subsequently decided to halt the provision of gender-transition services to minors, unless conducted within research settings across the state.
As of April 2024, 24 states have now placed age restrictions on hormonal and surgical sex-trait modification interventions for minors. Democrats in four states (Texas, Louisiana, New Hampshire, and Maine) have voted in favor of age restriction laws or against turning their states into hormone sanctuaries.
Spain
In 2018, the Spanish Association of Paediatrics and the Spanish Society of Paediatric Endocrinology published a statement endorsing youth medical transition.
In 2022, the directors of Spain’s Society of Psychiatry, Association of Child and Adolescent Psychiatry, and Society of Endocrinology expressed their opposition to a proposed law that would enable minors to access medical transition procedures. El Mundo, the second-largest daily newspaper in Spain, highlighted this controversy on its front page with the headline: “Psychiatrists explode against the Trans Law: It can bring a lot of pain and regret to many people.”
Australia and New Zealand
In August 2021, The Royal Australian and New Zealand College of Psychiatrists (RANZCP) issued its first position statement focused on the mental health needs of individuals with gender dysphoria, followed by an update in September 2021. This statement was the first from a professional body that did not explicitly endorse a gender-affirming approach.
Australia has experienced considerable debate in recent years regarding youth medical transition. This topic has been extensively covered by Australian journalist Bernard Lane for his Substack, Gender Clinic News.
New Zealand's Ministry of Health was expected to release an evidence brief in early 2024, aimed at reviewing the current evidence on the safety of puberty blockers. Although the publication has been delayed, it is anticipated to be released soon.
In April 2024, Guardian Australia reported that neither New South Wales or Victoria have plans to make changes to puberty blocker prescribing or accessibility as a result of the Cass Review.
International Bodies
In July 2023, for the first time, international experts publicly weighed in on the American debate over "gender-affirming care." 21 leading experts on pediatric gender medicine from eight countries wrote a letter expressing disagreement with US-based medical organizations over the treatment of gender dysphoria in youth, urging them to align their recommendations with unbiased evidence “rather than exaggerating the benefits and minimizing the risks.”
In January 2024, the World Health Organization (WHO) updated its announcement on developing healthcare guidelines for “trans and gender diverse (TGD) people.” The WHO stated in an FAQ that it would not be making recommendations that impact minors. Importantly, they made the following admission: "[O]n review, the evidence base for children and adolescents is limited and variable regarding the longer-term outcomes of gender affirming care for children and adolescents" (January, 2024).
Further Information
For additional information, one of the studies that contributed to the Cass Review conducted a survey of European gender services for children and adolescents from September 2022 to April 2023. Additionally, a Wikipedia page provides an overview of the "legal status of gender-affirming healthcare" (for adults) in various countries worldwide.
If you found this guide helpful, I am working on developing an information-based website that will feature up-to-date data, counterarguments to activist claims, explainers on research, and useful resources related to gender pseudoscience.
#Christina Buttons#systematic review#Cass report#Cass review#gender affirming care#gender affirming healthcare#gender affirmation#medical scandal#medical corruption#medical malpractice#head in the sand#willful ignorance
13 notes
·
View notes
Text
It's with great difficulty that I put my pride aside here.
As a transgender man, currently living in the UK, it's hell. The waiting list of the NHS for my region is close to 6 years, my back is fucked due to binding my chest ("don't bind and exercise"... I work hospitality. I don't have a choice), to the point I ended up stuck in bed for 10h in tears due to spasms, unable to get an ambulance cause... the health system is not doing ok. I work in a café/bookshop; the mental exhaustion of having JK Rowling mentioned daily, debating trans rights to validating my existence, my family cutting all ties with me... it's rough mate. But it's life, my life.
I need help. If not to fund my transition going private (as this would average £1500 just to start...!), to at least afford a chiropractor for my back and neck so I can be able to move up to a full-time contract and save money, and for counselling.
Chiropractor is £40 initial cost for the examination, then £35 per treatment, which I'm hoping a course of 3 treatments should put me back on track.
Counselling is £20 a seance via my local volunteering counselling group.
My Pa*Pal
Every little help, even just a reblog would be greatly appreciated.
For people not living in the UK and for more context : many industries are striking right now (as they should. Get a union people!), the NHS is crumbling down, the government is fucked but hey, Harry wrote a book huh. Some people can't afford to put the heating on, people are queuing at the food bank and it's been 3 months that a friend of mine is sleeping on my sofa because the council, housing agents and homelessness emergency helpline are all backed up and virtually useless right now. Two other people I know had to face homelessness within the last month. Everything is ✨️fucked ✨️
I give back to the community the best I can : volunteering at my local LGBTQ+ charity, connecting people by having a coffee/chat monthly event to help reduce the isolation of elderly people, organising exhibitions about the queer history, bookfares... but it's only last week-end, when my back once again was being a pain due to the cold and humidity that I realised that I, myself, also need help, laying there in bed like a grumpy old man being so proud and stubborn it was low-key laughable...
So if you can help, thank you so much. If you can't, thank you for at least reading me ❤️
Fuck the government, fuck politics, strike like there's no tomorrow, fight for your rights, unionise, be loud, be proud, don't be a c*nt and hand in hand, I'll support you, you'll support me, and we'll get there together. Solidarity forever.

#lgtbq#lgbtq+#lgbt rights#queer rights#trans rights#transgender rights#uk#uk politics#trans man#ftm#fundraising#health#mental health#merlin fandom#signal boost#solidarity#solidarity forever#unionize#unionise#striking#nhs#loud and proud#trans joy#edited
287 notes
·
View notes
Text
my grandma had a fall last night and another this morning. Eventually an ambulance got to her at about 4.30pm today. She's going to be staying overnight in the ambulance, which is in a queue of ambulances outside the local hospital; this hospital has actually just stepped down from "critical incident" status, the fourth such they have declared since the start of 2024 (it's March 2024 as I write this) -- so this state of affairs is actually below the emergency threshold, this is a "normal" state of operation for a hospital in the UK in 2024.
This is ten years of the tories in power, slicing up the NHS so that what was once genuinely one of the best health services in the world is nowinto a bad joke. Maybe once there was fat to be cut, but they've gone through the muscle and half the bone; the structure is starting to collapse. And this is also the case for all social services. There are homeless people camping in tents around my city, something that hasn't happened since the 1980s but has been picking up in the last few years. There's plenty of money for persecuting asylum seekers or aiding the Israeli genocide in Gaza (where the RAF flies scouting missions for the IDF and the Royal Navy sorties alongside the US Navy to break the Houthi anti-genocide blockade) or contracting big tory donors to carry out work for the public sector at inflated margins or giving unlimited financial support to private train companies to break a strike; and because of this -- in order to facilitate this looting of the state sector, my grandma is staying overnight in a fucking ambulance.
The labour party is no better. They have essentially taken on a tory policy-set and right-wing nationalist ideology. The previous labour leadership were different -- and so were smeared in the press as friends of terrorists and as antisemites. Absurd lies to anyone who was paying attention, but an absurd lie repeated enough can trump the truth; "there's no smoke without fire" say the guys with the smoke machine. And so now we get migrant-bashing genocide-enabling austerity-mongering patriot scum leading the labour party. At least tony blair brought in surestart centres and raised a million children out of poverty.
It used to be the case that we had to argue that socialism was not possible by a reformist path, citing examples like Chile. Now it seems that basic social-democratic reforms are not even possible by a reformist path; "fund the NHS" becomes something approaching a transitional demand, and to most people who don't believe that political change is possible even this sounds like an absurd ultraleft slogan.
16 notes
·
View notes
Text
NHS maternity services are getting worse with two-thirds of units in England now deemed unsafe as staff and hospitals find themselves under “huge pressure”, a damning report has warned.
Some 65 per cent of maternity services are now regarded as inadequate or require improvement for safety, up from 54 per cent last year, the Care Quality Commission (CQC) has found. Of these, 15 per cent are inadequate.
When looking at overall ratings, one in 10 maternity units are now rated inadequate, while 39 per cent are under the rating requires improvement.
The worsening picture of maternity care in England follows major scandals in Shrewsbury and Nottingham uncovered by The Independent.
The report says the “overarching picture” is “one of a service and staff under huge pressure”. Staff cover “is often fragile, with the rotas relying on every consultant being available”.
It added: “On top of this, consultants face additional pressure from, for example, having to cover registrar rotas and extra on-call shifts to meet the needs of their service.”
One patient told the CQC: “I couldn’t move and asked someone to help me feed my baby and was told ‘you can do it yourself’ … [The midwife] also told me that she was very busy and had other patients that took priority – when I still couldn’t move.”
The report further pointed to issues with governance and lack of oversight from NHS boards, as well as delays to care and lack of one-to-one attention during labour. The report also highlighted poor communication.
The watchdog has said a similar picture has emerged for ambulance services, with 60 per cent deemed to be inadequate or requiring improvement on safety – double last year.
Mental healthcare was also highlighted as an area of concern with 40 per cent rated inadequate or required improvement for safety.
Inspectors pointed to a lack of beds, meaning people can be “cared for in inappropriate environments – often in emergency departments”.
“One acute trust told us that there had been 42 mental health patients waiting for over 36 hours in the emergency department in one month alone.” the report said.
In its wide-ranging report, the CQC warned that healthcare risks becoming a two-tier system, with society divided into those who can pay for care and those who cannot.
It said: “Getting access to services remains a fundamental problem… Along the health and care journey, people are struggling to get the care they need when they need it.”
Factors such as long waits for hospital treatment, waits to see GPs and for referrals, combined with a lack of staff, “increase the risk of a two-tier system of healthcare, with people who can’t afford to pay having to wait longer for care and risking deteriorating health”.
During a press conference watchdog officials said: “More and more people are entering that long-wait category and it's becoming harder to prioritise and deprioritise people, when as I say we are, they are seeing a number of people who, who have effectively not been sustained on electric backlogs arriving into A&E with a serious condition.”
Research by YouGov showed that eight in 10 of those who used private healthcare last year would previously have used the NHS, while another study found 56 per cent of people had tried to use the NHS before going private.
The CQC added: “People may also be forced to make difficult financial choices. We heard from someone who receives benefits who resorted to extracting their own tooth because they were unable to find an NHS dentist.
“They then had to pay £1,200 on a credit card for private treatment, doing without household essentials until the debt was paid.”
CQC chief executive Ian Trenholm said the ongoing strike action by NHS staff – who are unhappy with pay and conditions – has contributed to backlogs.
Sally Warren, director of policy at think tank The King’s Fund, said: “This comprehensive report reveals the sad reality that the quality of care that patients need and deserve is not being met in many parts of the NHS and social care.”
A Department of Health and Social Care spokeswoman said: “We are delivering on three major recovery plans to improve access to urgent and emergency, primary and elective care, and have made progress to significantly reduce the longest waits for routine treatment, despite pressures including industrial action.
“There are record numbers of staff working in the NHS and our historic Long Term Workforce Plan will retain and recruit hundreds of thousands more staff alongside harnessing technology to reform the way we work and save staff time.”
17 notes
·
View notes
Text
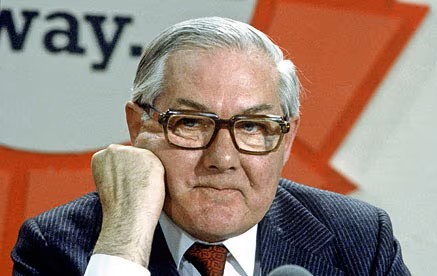
On September 7th, 1978, British Labour Prime Minister James Callaghan confirmed that he would not be calling an early election, despite the precarious stability of his minority government.
"…The government must and will continue to carry out policies that are consistent, determined, that don’t chop or change and that brought about the present recovery in our fortunes…We can see the way ahead…"
Opposition Leader Margaret Thatcher was not best pleased, referring to the government as chickens and stating;
"…The real reason he isn’t having an election is because he thinks he'll lose…"
Even Liberal leader David Steel, whose party had propped up the government through the Lib-Lab Pact, wasn’t happy, stating that the country was due for change and that an election was the only way to breathe life into the four-year-old parliament.
Callaghan had succeeded Harold Wilson in tricky circumstances in 1976. Inflation had peaked at 26% and unemployment was heading toward 1.5 million, a devastating figure in the context of the time although it would more than double by the mid 1980s under the Tories. Callaghan was forced to make unpopular cuts in government spending to comply with terms set out by the International Monetary Fund, after a financial crisis precipitated by the plunging Pound had necessitated an emergency loan. But it wasn’t all doom and gloom, the balance of trade was improving on the back of growing revenue and production from North Sea Oil, which was expected to make the country self-sufficient by 1980.
In the autumn of 1978, the government proposed that trade unions moderate the following year’s pay claims to 5% as a key part of the ongoing fight against inflation, which was by then hovering at 8%. The unions, however, rejected any limits proposed by the Callaghan government and vowed to pursue their right to free and unrestrained collective bargaining. The first major employer to concede over and above the government’s proposed ceiling was Ford Motor Company, which granted an increase of 17% after an initial ambit claim of 25%.
That December, the government received an unwanted Christmas present, when a motion in the House of Commons was carried condemning;
"…the arbitrary use of economic sanctions against firms and workers who have negotiated pay settlements beyond a rigid limit which Parliament has not approved…"
The Civil Service unions, now isolated under government control while private sector companies were free to set their own wage negotiation benchmarks without risk of sanction, prepared for militant action. The ensuing Winter of Discontent strikes created shortages of a number of essential commodities. NHS hospitals, ambulance services, rubbish collection, schools and even funeral and burial services were caught up in transport and related stoppages that created nationwide chaos.

At one point 200 000 workers were temporarily laid off, and rubbish piled high in the streets. By the end of January 1979, the strike ended with employers conceding to almost all of the various unions’ demands.
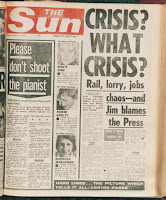
Into this chaotic atmosphere returned the PM from a summit with US President Carter, French President Valery Giscard d’Estaing and the West German Chancellor Helmut Schmidt. The meeting had been held in the sunny Caribbean Island of Guadeloupe. Callaghan, looking relaxed and unconcerned according to some reports, rather unwisely stated,
"…I don’t think that other people in the world would share the view that there is mounting chaos…"

He was rewarded by the famous What Crisis? headline in The Sun.
With an election looming, the government and Trades Union Congress finally made an attempt to publicly reconcile. The new Concordat, issued in February 1979, spelled out guidelines for a new cooperative approach toward dispute resolution, called for restraint in wage demands and set a joint ambition for an inflation rate of below 5% by 1982. It promised more measured picketing and more liberal union control over workforces. Callaghan called this a great step forward, while the Confederation of British Industry, unsurprisingly, said it was too little, too late.
Opposition Leader, Margaret Thatcher, soon seized a golden opportunity to take command of the agenda. She steamed in with motion of no confidence against the government on March 28th, 1979. The motion was passed by one vote, the first such successful motion since 1924. The subsequent general election paved the way for 18 years of Tory government.
Following the inevitable election loss, Jim Callaghan stayed on as Opposition Leader until 1980 when he was succeeded by Michael Foot. He subsequently served in the Lords as Baron Callaghan of Cardiff and passed away in 2005, aged 92.
#social history#uk politics#working class history#uk government#society#british culture#uk history#history#british prime ministers#trade unions#industrial action#protest
7 notes
·
View notes
Text
the nhs funding is so dire that they’ve advised medical practices to triage general appointments so now it’ll literally take months for people to be seen for anything deemed ‘non emergent’ by an online form… that’s actually insane to me
#it’s like checking the internet for symptoms and being told you’ll die or there’s nothing wrong with you when things can be the total#opposite in reality ?#and like this level of desperation is bc the govt is refusing to fund. they’re more concerned with funding racist wars I guess#mrow.org
5 notes
·
View notes
Text
i had a medical emergency erev shabbos & b”h it’s mostly calmed down now & it’s confirmed what i suspected was going on wif me (another autoimmune thing that’s extremely commonly comorbid with all my existing stuff)
so i can at least take a list of stuff and go over what happened with my very good and blessed GP and be like “for your consideration”
but was just thinking about how even though thankful i didn’t end up going to the chronically understaffed A&E on a friday night because
me and/or T absolutely would have ended up wif COVID or flu cos NHS IPC policies are broken since COVID “ended” (newsflash policymakers: it didn’t!)
and how the ambulance triage doctor strongly adviced me to go to urgent out-of-hours GP, and that would have been a mitzve as much as it was for me to call the emergency services too
but that decades of having to interact with the NHS and it’s structures is so traumatic. especially when you are read and categorised as a woman!!! and it literally stopped me from doing a mitzve for my own damn life!!!!!!
& was thinking about how before i got dx with Graves’ disease, when i lived in london, and my heart was going 200bpm when i was buying hairdye in boots
and i had to fly the next day, so me and my flatmate went to urgent care GP, and he told me with his whole chest i was having a panic attack because after waiting hours in the waiting room, my ECG was normal again
and like this is the whole reason i chose not to do a mitzve and go to the out-of-hours doctor. because my HR was 45bpm before i went to sleep and after the pre-fainting on erev shabbos but it was slightly higher again when i woke up and i just could not be arsed having a doctor dismiss me for something transient that is very clearly X thing from my symptoms, but won’t get captured on tests
this is what i mean when i say abolish the NHS but not in a tory way. cos as someone who was a nurse AND has been sick for a long time, no amount of funding will ever dismantle the NHS or is capable of disentangling it from the state. because it is literally *an arm of the state*. and don’t get me started on all the shit i witnessed over my 4 years as a nurse cos christ
3 notes
·
View notes
Text
Just had an American comment on my insta post about my displeasure regarding having seen a crappy GP and being prescribed something far less than what I actually needed.
They said that they ‘hate the healthcare you guys get over there’ meaning the UK.
Now…don’t fucking come at me badmouthing the NHS. Tbh, when it comes to emergency care, they are outstanding.
They’re only falling short in other areas because the shitty arsehole government don’t allocate enough money to it. There is nothing wrong with the healthcare, but there’s everything wrong with the lack of funding.
Don’t come at my country’s healthcare. Just don’t.
7 notes
·
View notes
Text
When a ship encounters a storm, the captain does not rip up the deck and cut off the lifeboats to make the ship move faster. Doing so might temporarily delay flooding, but it gives passengers no chance when an iceberg crashes against the hull. And yet that’s exactly what British governments have been doing ever since the financial crisis of 2008. One by one, the ropes holding on to our welfare services and public institutions have been severed. The current government, which has called on departments to find “efficiencies” to meet its unfunded tax cuts, is no different.
So what can we expect to happen if Liz Truss’s cabinet pursues these cuts? Already, Conservative MPs are extolling the benefits of an “insurance-based” health service, and seem to be preparing the ground for further waves of NHS privatisation. Yet Britain’s public sector has already been gnawed to the bone. How will departments “trim the fat”, as the levelling-up secretary Simon Clarke described the approach over the weekend? Is there even any fat left to trim?
Over the past decade, the dismantling of Britain’s welfare state often took the form of direct budget cuts. Spending on schools per pupil in England decreased by 8.3% in real terms between 2009 and 2019. Local authority funding from central government was slashed by 49.1% between 2010 and 2018. Many government departments also had their budgets cut by millions; the Department for Energy and Climate Change’s spending was hit by 23% in 2011.
In other areas, the public sector was hollowed out in more insidious ways. Although total healthcare spending was protected from direct cuts, for example, the soaring demand for health services caused by rising poverty and demographic ageing have not been matched by NHS spending increases. By the end of that decade, waiting times for emergency care and complex treatments had soared. The size of the civil service plunged by 19% between 2010 and 2016. Between 2010 and 2014 alone, government spending on outsourcing services in the UK doubled to £88bn, transferring colossal public resources into private hands.
This time around, the Conservatives don’t need to introduce pay freezes or productivity targets to encourage further privatisation and outsourcing. The dire situation of our public sector may guarantee that when faced with further budget cuts, the people running government departments feel they have no option but to contract more services out. The minority of patients who can afford to choose may opt for expensive private insurance over long NHS waiting lists, while those continuing to use public healthcare will grow frustrated with its inefficiencies and waiting times – and in many cases they will likely blame the health service, rather than the reasons for its decline.
Britain now faces a real risk that its welfare state will become a “dual system”, where a sizeable chunk of care is provided by private companies in parallel with a public healthcare system. Some may ask why this matters – if we still have a public health service, what’s the issue with the rich paying for private healthcare? The problem is that dual systems of welfare exacerbate inequality and frequently undermine the quality of public services. Moreover, once the principle of universal free public services is eroded, it becomes more difficult to make the argument for their existence in general. The case for a welfare state begins to fray.
In Chile, for example, reforms to the health system introduced under the Pinochet dictatorship created the option for wealthy citizens to pay into a private health fund, rather than the already underresourced National Health Service. This exacerbated the resource pressures the health service was already under. Not only did the private fund absorb the majority of contributions, despite covering only 16% of the population, but those it covered were disproportionately wealthier, younger and male, and so statistically “less likely to require sustained health services” . Many people with access to private services also continued to use the public system for routine treatment in order to protect no-claims bonuses. This compounded the pressures on the public system, as those able and paying for private insurance remained reliant on it. In other words: the introduction of a dual system of healthcare did not even work as it was intended.
Outside central government and the NHS, many local authorities are already at breaking point, with poorer local authorities struggling to provide and maintain basic services such as parks, libraries, refuse collection and children’s centres. And we’ve already seen how privatisation leads to the growth of predatory multinational companies that profit at the taxpayer’s expense. Given all this, it’s only fair to assume that further privatisation is precisely what the Truss government hopes to achieve through further cuts. The policies announced this week are a textbook case of how you scuttle the welfare state, and perhaps even sink it entirely.
8 notes
·
View notes
Text
101 Things You Should Know About the UK Tory Government
Thing 28
In Thing 18, I highlighted the failure of Health Secretary, Steve Barclay, to provide the £500 million emergency fund to help ease the A&E waiting times made available by his predecessor Therese Coffey.
In Thing 24, Steve Barclay was again the subject of debate when he stated that nurses were “out of step” with economic reality and their request for higher pay was neither “reasonable nor affordable”.
We now know why it is unaffordable.
“Steve Barclay astonished Treasury officials when he told Jeremy Hunt, the chancellor, that he would not ask for more money to offset the effects of inflation next year, promising to find efficiencies and savings instead.” (The Times: 14/11/22)
Is this a deliberate policy by the unelected Rishi Sunak to run down the NHS to such a sub-standard level of service that the public will no longer want to use it? Why else would Sunak appoint a health secretary who has been described as “a real nightmare, vindictive, arrogant, a bully, hostile to the NHS”?
The unions certainly think this is the case.
“Union boss accuses Tories of deliberately 'running down' NHS so someone can take it over." (Mirror: 13/11/22)
Even "Jeremy Hunt ‘accepts picture’ of NHS on brink of collapse." (Guardian: 13/11/22). Despite this Hunt is still demanding that the NHS must accept efficiency savings and play its part in fixing Britain’s broken economy.
It would seem the former Health Secretary Hunt and Steve Barclay have much in common.
“Mr Hunt presided over a time of particularly low investment in the NHS, due to the Cameron-led coalition government adopting austerity measures." (I: 18/11/22)
It's funny how history repeats itself.
2 notes
·
View notes
Text
If we can't spend more we can at least spend better
The case for Place Based Public Service Budgets
First published on LabourList 31st January
On Monday, Angela Rayner described the government’s announcement of £600m of new emergency local authority funding as a “cynical sticking plaster”. She’s right: the money is welcome but a drop in the ocean.
Almost every day another council faces bankruptcy or cuts services to the bare legal minimum, in just one part of the crisis engulfing England’s public services. Last autumn, the NHS was facing a £7bn shortfall, according to independent experts. Schoolchildren in deprived areas are falling behind. Our courts and prisons are clogged.
We must revive a radical New Labour policy
Labour’s leadership is clear that a government boxed in by record taxation, high national borrowing, and years of low growth will have no quick or easy financial fix.
A new report I have co-authored with Jess Studdert of New Local says that if we can’t spend more, we must spend better. It advocates reviving radical ideas for place-based public service budgets that were pioneered by the last Labour government.
The concept behind the ‘Total Place’ pilots launched in 2009 was simple. Find out how much money is spent on all public services in an area and work out how to spend it better. That might sound blindingly obvious, but it isn’t how public service funding worked then, and it isn’t how it works now.
Local spending is fragmented into siloes. Each silo is accountable to a different government department, each has different measures of success, and each is funded separately by the UK Treasury. Effective local coordination of spending is impossible.
This setup is deeply damaging to how our services work. The IFS recently found that the distribution of £245bn spent in England across the NHS, schools, local government, the police, and public health did not reflect local need.
Some services in some areas were relatively overfunded. Others were underfunded. The IFS concluded that “there may be benefits in providing greater flexibility to leaders to move spending between service areas”. Under the current system, that just isn’t possible.
Services lack funds or incentive to focus on prevention
Real people don’t live their lives in separate departments or services. They often know what would make a difference but instead of services shaped around their needs they find duplication and gaps. Studies have found families forced to interact with many overlapping agencies, while social workers get bogged down in administration.
An ex-offender is more likely to get into new trouble than receive joined-up support from prisons, probation, mental health, housing, and Job Centres. Almost every family has experienced the broken interface between the NHS and social care.
Too little is invested in early intervention : each service has an incentive to shift the costs of economic and social failure on to another. It is a Catch-22 which our report calls “the prevention penalty”: services have little motivation, or money, to fix problems which will later become another service’s crisis.
Some councils pioneer collaboration, despite the system
Total Place offers a way to break this vicious cycle. The proof is in those early pilots, which filled me with so much hope when I was Secretary of State.
The first-year pilots were taken up across England, by councils of all political stripes. They showed how to bring health and social care together, deal more effectively with substance abuse, create joined up children’s services, and improve access to many services. All offered better services for the same money.
The Coalition scrapped Total Place in 2010, opting for the deep and damaging austerity we have had since.
Occasional attempts have since been made to bring services together; some councils have pioneered new ways of working and enabled local people to shape services that meet their needs. These prove the principle works but they happen despite the system, not because of it.
Councils can’t save any more cash
There is no room for more savings in today’s local government. There is no scope for top-down ‘productivity’ drives which intensify the ‘doom loop’ of constant crisis fighting and prevent service improvements.
Labour sees the need for change. Shadow devolution minister Jim McMahon recently told the Institute for Government: “The question is how do you get more bang for your buck? There is something in looking at every pound you spend in an area and really requiring every part of Government to marshal around a single plan for a place.”
It will take radical reform and the creation of Place Based Public Service Budgets to realise that potential. All agencies would identify the total money spent in each locality and match this against the needs of local people and communities.
Coordinated by elected local authorities they would produce Local Public Service Plans that set out new ways of working – including ways of involving local people – and the improved outcomes to be achieved. Instead of working to top-down departmental targets, local partners would be held accountable for achieving the results they promise.
And instead of each service reporting to its parent department – a system that gives only the illusion of looking after public money – value for money would be bolstered by a new statutory local audit service and Local Public Accounts Committees. Together these would provide tougher scrutiny than exists at presents.
It will take political determination to push such changes through Whitehall’s entrenched and centralist culture. But for a party committed to improved public services, there are few other games in town.
The ‘Place Based Public Service Budgets – Making public money work better for communities‘ report by John Denham and Jessica Studdert, Deputy Director of New Local, and is published by NewLocal in association with the Future Governance Forum.
0 notes
Text
me listening to the nhs hold songs for the last 15m trying to get my psychology appointment to another date because im only in my home town tomorrow but its a day off idk if the front desk will be open or just emergencies but if i miss this apointment theyll take me out of the list because it will be the 3rd i miss but also a friend of mine said psychiatrists cant send you to psychology anymore but the general doctor or however its said in english also cant do it and then i have no clue what kind of fucking loop i have to take to try and get in nhs psychology again and also next year the far right is gonna become our goverment and they will for sure cut out funding to the already struggling nhs and for sure i wont be able to transition for another at least 4 years now that my disphoria is acting up more often but also before that just to function semi normally i need to get meds from psychiatrist and it helps to see my psychologist every 3 months and hey while writing this one handed they awnsered and did it and it was quick and effective yay <3 i wont lose acess to mental health stuff for another few months yay yipee <3 the lady was super nice im happy i love nhs im just sad its going badly and it will get worse anyway the ammount of stuff i was working up on this hold and then the relief i felt once she said she asked for the new date omg how did i ever need someone else to tell me i have ocd and not know it myself the spiral was spiraling anyway yay <3 back to trying to do work i should have delivered weeks ago yipee
0 notes
Text
Time for a personal rant and reminder about why, as good as private healthcare looks right now (compared to the state the NHS is in at the moment), we need good quality healthcare (less than good is insufficient) to be free for all.
The emergency doctor I saw yesterday at my local GP (who was a dr I'd never met before) prescribed antibiotics for my ear, but my ear was blocked so he couldn’t tell if the problem was just the wax, or also an infection, or something else.
But I don't have any other symptoms or signs of ear infection like I normally get and I'm not gonna use antibiotics unnecessarily because 1. antibiotic resistance and 2. I often get a stupid fungal infection afterwards (cos it kills the good bacteria that help keep your immune system in shape as well as the bad bacteria… I really hope big pharma is at least working on ways to develop antibiotics that can be more targeted?!)
privileged enough to have a sister who gets work perks like free private gp appointments, I had a TWENTY MINUTE phone call with one of them today and it was so much more thorough and useful than the 5 minute appointment I had yesterday (the only useful thing about that was getting my ear looked at).
After explaining everything from how my symptoms have developed since last week, what I think triggered it, my ear health history, etc - we came to a very different conclusion (where he basically agreed with me that I don't think this is likely to be an infection). He thinks that as well as the earwax I may have a blocked eustachian tube, which could definitely have been triggered by the sore throat I had for a couple of days last week (which I think wasn’t due to any infection but from temperature fluctuations i experienced the day before).
So one doctor’s quick conclusion was antibiotics. The other doctor’s conclusion was: use the steroid nasal spray i already have leftover from when covid gave me post-nasal drip and take some antihistamines. and he explained WHY (reduce inflammation to help unblock the eustachian tube), and he went into the detail of HOW to use them all - which included some nasal spray tips i’d never been made aware of previously even though i’ve been prescribed nasal sprays before.
I’m so glad I’m knowledgeable enough to be able to suspect some things in the right direction, but also grateful that I'm privileged enough to get a second opinion that corroborated this and taught me even more. But healthcare is a human right, so everyone should be able to get healthcare (not being diagnosed/treated sufficiently is not healthcare - that’s negligence) without having to pay or have any privileges.
If I took those antibiotics when I had no bacterial infection to treat, it would’ve not only been a waste of medicine, it would create complications for my immune system that would take even longer and more effort to treat - and the original problem with my ears would still need treating as well.
I’m old enough to remember when NHS GP appointments were long enough to explain yourself in full detail, heck even back when I was 5 years old they did home visits if you requested it!
Problems are often complex when you have health conditions and when you are aware about certain kinds of things pertaining to your health, so you want to give your doctor as much relevant information as possible so they can make the most informed choices about what will be the best treatment for you. Short appointments are insufficient and can therefore be damaging. The NHS needs FUNDING, RESOURCING, and much more effective forms of MANAGEMENT than it currently does. The last thing the NHS needs is cuts and privatisation, both of which have led to mismanagement, inefficiencies, consequences for patients, and therefore worse health overall for the population.
I need everyone in government and corporate who is working on sabotaging and privatising the NHS to be stopped. Speaking of which, these guys are trying to do just that: https://everydoctor.org.uk/
1 note
·
View note
Text

University of Aberdeen scientists fight back against global public health emergency
Following the declaration by the World Health Organisation (WHO) that antimicrobial resistance is one of the top global public health threats facing humanity, a 5-year long project is now underway to find the best and most effective forms of defence against this growing problem.
The UK Antimicrobial Registry (UKAR) study, led by Professor Gary Macfarlane from the University of Aberdeen, will incorporate information from hospitals across the UK to achieve a multi-stakeholder registry of antimicrobial agents.
Funded by the British Society for Antimicrobial Chemotherapy, the study will determine which antibiotics are the most effective and best able to control the threat of antimicrobial resistance.
Antimicrobial resistance occurs when bacteria, fungi and viruses mutate over time and no longer respond to medicines. This can make infections harder to treat and increases the spread of disease. One common example, MRSA, often labelled a ‘superbug’ is an example of a bacteria that has become resistant to commonly used antibiotics and as such proves difficult to treat and can lead to serious illness and even death.
The UKAR study will look at how effective eleven new-to-market antibiotics are; how well they work, how good they are at treating different infections and how they are currently being used in UK hospitals on infections that cannot currently be treated. The resulting registry will help doctors and scientists navigate the ever-changing microbial environment and keep the threat of antimicrobial resistance at bay.
Professor Macfarlane who is leading the project said: “Antimicrobial resistance is a real threat to our ability to treat common infections and is one that demands urgent attention.
"Currently available antibiotics are becoming less effective against some infections, so it is vital that we use them appropriately.
“The UK Antimicrobial Registry study will look at the effectiveness and safety of new antimicrobial medications which are used to stop the growth of micro-organisms that can cause disease.
“These medications are a vital part of modern medicine and include antibiotics (which target bacteria), antivirals (targeting viruses), and antifungals (targeting fungal infections).
“This work will help us find out how widely these medicines are used across the UK, why they are being prescribed, and how effective they are.”
Dr Noha El-Sakka, Consultant, Medical Microbiology and Virology at Aberdeen Royal Infirmary who is leading the NHS Grampian arm of the study added: “Antimicrobial resistance represents a global challenge and the need for new antimicrobial agents is becoming more and more essential.
“The UKAR study is an exciting project that will help address and shed light on the available new antimicrobial agents, and the clinical value of their use particularly in the context of limited available other option. This is much needed information, and data from the study is going to be an extremely valuable resource to help shape the strategy for management of infection in the future.”
To learn more about the UKAR Study and other research led by the University of Aberdeen Epidemiology group, visit the website.
0 notes
Text
New Post has been published on All about business online
New Post has been published on http://yaroreviews.info/2023/04/britains-economy-is-back-says-chancellor
Britain's economy is back, says chancellor
By Faisal Islam & Lucy Hooker
BBC News
Chancellor Jeremy Hunt says Britain’s economy is “back”, and that his strategy for growth has been welcomed at the International Monetary Fund meeting in Washington.
His predecessor, Kwasi Kwarteng, left the previous IMF meeting in October early, amid a barrage of criticism.
Mr Hunt said the international lending body saw he was “putting the British economy back on the right track”.
However, the latest figures show the UK economy failed to grow in February.
On Wednesday, the IMF said it expected the UK economy to shrink by 0.3% in 2023, which would make it one of the worst performing of the world’s major economies.
When challenged over whether the UK’s current performance undermined his positive message, Mr Hunt said: “It’s other finance ministers who are telling me Britain is back”.
Britain’s economy has only just recovered to the size it was prior to the pandemic, following months of industrial action, rapidly rising prices and labour shortages.
On Friday nurses in the RCN union rejected the offer of a 5% pay rise and said they planned to strike again at the start of May. Meanwhile, NHS junior doctors in England are currently staging a four-day walkout over pay, ending at 07:00 on Saturday.
The wave of industrial action affecting the UK in recent months has contributed to its lack of growth, the Office of National Statistics said this week.
However, Mr Hunt said it was important to avoid fuelling further inflation through pay rises. He said Britain had avoided recession this year “so far”, and that he hoped to see faster growth and falling inflation in the months ahead.
Measures in his March Budget to help businesses recruit more staff and to increase investment, including an increase in childcare funding, should stimulate growth, he added.
Investor confidence in the UK was shaken last year during the short-lived government of prime minister Liz Truss, which saw Mr Kwarteng present an economic strategy that included major tax cuts without an explanation of how they would be funded.
Nurses strike on bank holiday as pay deal rejected
Pay rises above inflation would be a mistake – Hunt
Strike action sees UK economy flatline in February
The outlook for the UK, which relies heavily on financial services, could be clouded by current uncertainty in the banking sector, following the collapse of three US banks and UBS’s emergency takeover of Credit Suisse.
However, Mr Hunt said the UK had “a very robust, resilient banking system”, which was now in a much better position than it was before the 2008 financial crisis.
“Am I confident in the resilience of our banking system, the second largest financial services centre in the world?’ Yes, I am,” he said.
While the government is considering reforming some of the rules governing financial services, put in place after 2008, Mr Hunt said the plan was “absolutely not to unlearn the lessons of the financial crisis”.
“We are looking at all of these things, but we’re not going to do it in a way that rows back on any of the very important protections that we have in place,” he said.
But he said the growth of the UK’s tech and life sciences industries meant regulations needed to adapt.
“We have a lot of high growth companies in the UK, and they need to have banking services that suit their needs. And that’s a difference from a decade ago,” he said.
Related Topics
International Monetary Fund (IMF)
UK economy
Jeremy Hunt
More on this story
Nurses to strike on bank holiday as pay deal rejected
2 hours ago
Pay rises above inflation would be a mistake – Hunt
1 day ago
Strike action sees UK economy flatline in February
1 day ago
0 notes
Text
How to Slow Down Time
Think of a clock. Not a digital one. One with a second hand. Not a second hand as in the second of two hands. A second hand to delineate the passing of seconds. Maybe known by some as a third hand?
Let me restart. Think of a clock but without the minute or hour hands. Just the second (as in the denoting of time) hand. Now you have your clock. Adorn it with pretty ideograms for numbers. Now, can you count to sixty and imagine for every second that you count, the second hand moves approximately one-sixtieth degrees around your clock.
You probably didn’t do this. If you did, you probably would have noticed that it felt like longer than a minute.
I’ll set this out another way. If you were anything like me, during your school days you must remember taking furtive glances at the clock on the wall. Do you remember thinking half an hour must have gone and then feeling dismayed when you see only ten minutes had gone?
Conversely, doing your exams. You think you have ages left and then, much to your chi grin, see that you have only five minutes left, and you still haven’t even started the long-form question inAlbert Camus’ L’Etranger in your French A-level exam. While that may not have been your exact situation , I shall assume you get my drift. And that is that time passes slowly when you wish that it passed quickly. And time passes quickly when you want it to pass slowly. Except it doesn’t. Of course it doesn’t. We all know it is entirely psychological.
Back to my clock analogy. Imagine counting those sixty seconds. Do it again sixty times. Then again 1040 times. Then imagine you had to do those sixty seconds 189,280 times. Seems like an awful lot of seconds.
That was an ineloquent way of expressing how time passes for me. Slowly. Like a snail with no foot. A big fat bulbus slug making its way up a hot, oily pipe.
Well, I have now mastered the power to slow down time on a perennial basis. I spend much of the day lying on my bed staring at nothing and thinking about nothing you want to hear about. Wishing for time to pass. Any stimulation just pisses me off and most of the time I don’t even mind the wallow.
It has been sixteen days since I had my surgery and it has felt I have been this way for months. I would pay good (all of my) money to be knocked unconscious for two months and be fed through tubes and have one of those machines that turn you over so you don’t get clots. How that sound like the life for me. I have enquired, but perhaps unsurprisingly it is not something offered by the NHS, or any private healthcare institution.
On the note of private healthcare, I’d like to make a shout out to my private healthcare insurance provider, AXA PPP. Thanks for refusing to pay for any CBT sessions and thanks for refusing to pay for anything related to my pain, because they don’t fund “chronic conditions”. If this is litigious, do you really think I care? AXA: you’re shit. And NHS? Still waiting! Our poor NHS. So little money and so many sick people. It’s doomed to becoming an emergency-only service in the coming decade or so. I am on the urgent list and still have to wait months for treatment. Imagine if you were having to wait for elective treatment. Well actually five million people don’t have to imagine as they have been waiting over a year for treatment. The saddest part is that if you can afford it, you can get treatment for, let’s say a hip replacement, the following week. For the same treatment under the NHS, you’d be looking at waiting two or three years. Isn’t it great to see how fair society is becoming?! Gone are the days that Etonians stroll the halls of power! Gone are the days that contracts are given out to the chums of ministers! Gone are the days that white classically educate men (hello) dominate the highest paid positions of the always egality-driven financial services industry. While there may be more ethnicities and regional representations in both financial and political spheres, it’s still the same.
Turns out I didn’t apprise you on how to slow down time. I suppose I can summarise it to you in three simple steps:
Think about things In the future that you want now
Think about how what you are doing right now is what you really don’t want to be doing
Think about the past and all the good memories and sour them with the knowledge that they will never happen again
Based on my experience, doing these as concurrently as possible will ensure you psychologically a long and unhappy life. Which is what we all crave, in the end.
You’re welcome.
0 notes
Last Seen Blogs



