#hc-did
Text
The Basics of DID/OSDD
DID, or Dissociative Identity Disorder, is a trauma-caused disorder that forms in early childhood, anywhere before the age of 9 (cutoff age is debated but the typical range is before age 6-9, but some people extend it to 10 because that's the typical age where your identity starts forming independant of your primary caregivers)
Most of the established and spread facts about DID come from the Theory of Structural Dissociation (TOSD)
Here's a good resource explaining The TOSD:
To sum things up, there are levels of dissociation that can occur, and disorders that fall into each level. The lowest end of this spectrum is PTSD, and the highest is DID. Here's a graphic of those levels, and I'll go into each disorder briefly:
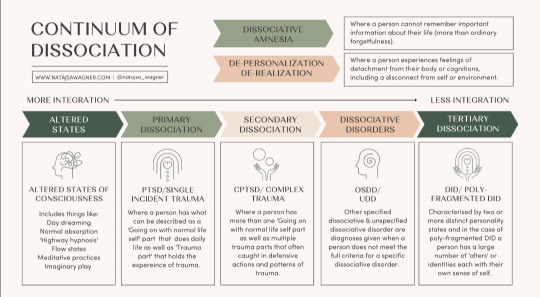
Altered States
Altered states are normal, and likely to occur in everyone at some point. No trauma is required to cause these states. Altered states include normal daydreaming (not including MaDD which is disordered)
Primary Dissociation
Primary Dissociation occurs in people with PTSD. This presents as having one ANP (Apparantly Normal Part, aka you) and one EP (Emotional Part, which occurs when having PTSD flashbacks)
This level is specifically for single-event PTSD, as C-PTSD falls under the next level:
Secondary Dissociation
Complex-PTSD falls under this level because of the occurance of multiple EPs, but still one ANP. These EPs are for a myriad of traumas a person with C-PTSD has experienced.
Dissociative Disorders
This is where we start touching on systems. This level includes OSDD and UDD.
OSDD (Otherwise Specified Dissociative Disorder) is a bit of an umbrella disorder, and it encapsulates multiple different types of OSDD. The one you've most likely heard of is OSDD1b, but I'll go into all of them.
OSDD1a is a disorder in which a person has multiple identity states but they lack distinction. They have intense enough amnesia to qualify for DID, but their identity states aren't differentiated enough to fully qualify for DID. This can sometimes (not always, of course) present as multiple identity states that are all one person, just at different ages when trauma happened.
OSDD1b is a disorder in which a person has multiple identity states that qualify for DID, but have no amnesia. A common misconception is that to be diagnosed with DID, you have to have blackout amnesia (will explain amnesia types later in the post), but any type of amnesia can qualify. OSDD1b is for systems who have absolutely no amnesia.
OSDD2 is a disorder in which there are identity disturbances and dissociation caused by brainwashing, torture, cults, and things of that sort. From what I understand, OSDD2 occurs after the cutoff age of DID or OSDD1, hence why this disorder does not cause a system.
OSDD3 seems to be a temporary diagnosis for symptoms of dissociation, derealization, depersonalization, amnesia, sudden loss of motor skills, ect for less than one month, occuring directly after a traumatic event. If the symptoms persist after this one month period, another diagnosis may be looked at.
OSDD-4 is a disorder in which people experience dissociative trances that do not have any known cause. People slip in and out of these trance states, often unaware of their environment while in them, and may "come to" confused and with amnesia from their time in the trance state.
And lastly, UDD. UDD, or Unspecified Dissociative Disorder, is exactly as it sounds. It's a catchall diagnosis for when a dissociative disorder is present, but it's unknown exactly which one. This can include systems, or it can include other dissociative disorders.
Tertiary Dissociation
Teritary Dissociation is what includes DID, C-DID, and HC-DID.
DID is the disorder we are all reading this post for. It is a disorder that causes multiple identity states that are distinctly different, called alters (or other terms depending on the system's comfort, such as headmates or sysmates), and amnesia between these identity states.
C-DID is a community term which stands for Complex DID. It is synonymous with Polyfragmented DID; they both mean the same thing. C-DID is characterized by a more complex system structure and the presence of many fragments, occuring because of more complex and longterm trauma that starts before the age of 5 (so earlier than the DID cutoff), and typically continues long after the system forms. There are many signs of polyfragmentation in a system, but the most siginifigant are the earlier onset of trauma, presence of many fragments, and more complex internal structure.
HC-DID is another community term which stands for Highly Complex DID. This term is synonymous with programmed systems/RAMCOA systems. These systems formed because of childhood trauma involving Mind Control (the MC of RAMCOA), aka programming. I won't go too in-depth on HC-DID systems, because I'm not confident in my knowledge at this time. However a great blog I can recommend for anyone wanting to learn more is @cultishhellvent
Misc.
You might have noticed at the top of the graphic I included earlier a little blurb about DPDR, or Depersonalization Derealization Disorder. This is a dissociative disorder characterized by, well, persistant depersonalization and derealization. This disorder cannot co-occur alongside DID, but DID can cause depersonalization and derealization. The DPDR diagnosis is for those who don't have another dissociative disorder like DID, but do experience those specific symptoms of depersonalization and derealization.
P-DID, or Partial DID, is a version of DID in which one alter is almost always fronting. Other alters are present, and may front in specific situations, but typically the one alter will stay at front and other alters will come and go from co-con or co-front.
Things To Know About Systems
So here is a bunch of catagories of info about systems that I feel are necessary to know if you're looking to know the basics.
Amnesia Types
Blackout Amnesia is amnesia that is full and total. Periods of blackout amnesia will be fully gone from the person's memory. However, contrary to popular belief, blackout amnesia does not entail literally 'blacking out' and 'waking up' at a later time. It simply means the memories from a time period are totally and utterly gone and inaccessable to you.
Greyout Amnesia has two typical definitions. The first is amnesia that slowly occurs as time goes on, like slowly forgetting the days as you pass them, at a faster rate than would be considered typical for those without a dissociative disorder. The second definition is similar to blackout amnesia, except some memories can be retained. So you may not fully remember an event you went to last week, but you might be able to recall a few blips of major things that took place. Most detail is usually lost.
Emotional Amnesia is when you remember the actual event or time frame, but none of the emotions attached to it. This usually presents as being able to remember a traumatic event, but feeling numb or disconnected to it, or like it happened to someone else.
And something important to keep in mind is that these amnesia types are not hard rules, and amnesia is often somewhere between these three labels.
Innerworlds
Innerworlds, or headspaces, are internal worlds in which alters can go when they aren't fronting (fronting meaning to be in control of the body)
Not all systems have innerworlds, and many systems with Aphantasia (when you can't visualize) simply don't have the ability to create them.
Innerworlds are often created unintentionally as the system grows up, but they can be intentionally created and that can be a beneficial process to the system.
Alter Roles
Alter roles are labels systems can assign to their alters to describe what role they play in the system's life. Some common ones include Host (primary fronter), Protector (self-explanitory), Persecutor (causes the system harm for whatever reason), Traumaholder (alters who hold trauma), and Littles (child alters)
These roles are not hard set, they are simply labels to help explain and put words to what certain alters' jobs in the system may be. And, not all alters have a discernable role.
Introjects
Introjects are alters who form based on an existing identity. This is common in fragments, since they aren't as fully formed, but can of course also happen in fully formed alters.
There are two main catagories of introjects, however many people like to get specific with the terms they use.
Fictives are introjects of fictional characters. This can be from visual media, books, OCs, ect.
Factives are introjects of real people. This can be from friends, abusers, family, celebrities, ect.
Introjects are NOT the same as the thing they are sourced in. They are their own separate people, and should be treated as such.
One of the specific terms I mentioned could be songtives (introjects from songs). I wanted to briefly mention that as an example of the specific terms systems may use.
Co-Con/Co-Front
Co-con, or co-conciousness, is when two or more alters are present at the front. This is usually used to describe one alter fronting, with one or more other alters hanging out nearby and talking occasionally.
Co-front, or co-fronting, is when two or more alters are sharing the front together fully. Think of two people trying to drive the same car at once.
I think I've covered everything I wanted to cover. If I missed anything, said anything incorrect, or you'd like something added please feel free to send an ask or comment/reblog.
#did#osdd#udd#pdid#anti endo#anti tulpa#polyfrag system#c-did#hc-did#ramcoa#actually traumagenic#endos dni#did community#traumagenic did#system#osdd system#actually osdd
578 notes
·
View notes
Text
If your trauma caused you to split, then you were traumatized 'enough' to be traumagenic/have DID, OSDD or what have you. Trauma isn't always from a parent: it can be peer bullying/shunning, sibling abuse, near death experiences, experiencing death of a loved one or even a stranger, medical trauma, etc.
I will go one step further and say that if your system experience isn't purely traumagenic, and you're pushed out of supposed safe spaces because of it, don't feel pressured to change the labels that feel right for y'all. I have half a heart to not post this in traumagenic tags, because SO MANY traumagenic systems are anti endo it seems. But mixed origin systems exist, endo systems exist, non-disordered traumagenic systems exist, etc and plurality is such a large umbrella of different experiences (even yours!).
You're doing nothing wrong by existing.
#plural positivity#system positivity#osdd#did#traumagenic#endo safe#mixed origin safe#sysblr#disordered system#nondisordered system#p-did#c-did#hc-did
168 notes
·
View notes
Text
Friendly reminder that if you lock up alters to protect the system from being discovered because you're still in an abuse setting, or because you're an HC-DID system and have programmed alters who could kill the body or hurt others, you are not a bad person and I get it. And it's okay. We're all on our own journeys and I'm not here to put moral value on anything your system does in regards to itself.
"Locking up alters is ALWAYS bad" except it isn't, and there are plenty of valid reasons to lock up certain alters for the safety of the body and system as a whole. Do what you need to, heal when you're safe to do so. Don't let tumblr force you to put yourself in a dangerous situation.
167 notes
·
View notes
Text



DID, OSDDID, OSDD



HC-DID, UDD, P-DID



System flags, middle one is Plural Peafowl(link)

More Plural stuff!
DNI is listed within my pinned post. Please go read it before interacting with any part of my content. Ask to tag!
#🎨 post#liom#mogai#liomogai#DID#OSDDID#OSDD#HC-DID#HC DID#UDD#USDD#P-DID#P DID#System#Plural#Plural system#Plural Peafowl#pride emote#pride emoji#pride pixels#pride pixel#plural pixels#plural prixel#plural emoji#system emoji#HCDID#PDID
48 notes
·
View notes
Note
polyfrag (HC) culture is haha I'm not really polyfragmented... I don't even have DID... oH SHIT A SIDESYSTEM MADE UP ENTIRELY OF FRAGMENTS??? THOUSANDS OF FRAGMENTS???
.
#polyfrag culture is#hc did culture is#c did#cdd#cdid#complex dissociative disorder#did#dissociative identity disorder#polyfrag#polyfrag system#polyfragmented#polyfragmented did#polyfragmented system#complex did#hc did#hc-did#highly complex did
56 notes
·
View notes
Text
The urge to make a ***NOT FOR MAKING FIRENDS OR TALKING*** discord server that's just any and all ramcoa resources and ways to figure it out cuz while we were doing research it would have help SO MUCH
and just, yea, wanna just have a server full of resources
Thoughts?
and just to reiterate, not for conversation (except maybe questions that only mods would be able to reply to), we recognize how dangerous it is to put a bunch of traumatized people who could be easily triggered in a room together, the server would be strictly for resources
(I am high-key hyperficiating on ramcoa cuz that's my job)
#north.txt#hc did#hc-did#hc-did system#ramcoa system#tw ramcoa#ramcoa victim#ramcoa#tw tbmc#tbmc#dbmc#tw dbmc#plural#actually plural#plural community#plural system#plurality#traumagenic did
85 notes
·
View notes
Text
I know I just reblogged a post about it, but oh my Fucking God
It's almost impossible to have more than one script and still have somewhat functional programming, let alone 3 or more. Implementing one script is extremely time-consuming, and difficult, and has so many risks of failing and compromising current and further programming.
Scripts are based on things that have been around for years(like, 30. not just 10), have prominent themes that would genuinely benefit the abusers, and are something easy for children to understand(one of the best examples being the bible) The implementation of specific scripts is information passed down from abuser to abuser, and won't include things that have come out recently(warrior cats, harry potter etc)
Forced splitting of alters from media isn't the same as scripts. This is something more widely done, easier to do, and doesn't face the same complications that scripts do.
It is literally unheard of to have multiple scripts and functioning programming. It is extremely unheard of for programmers to Try and implement multiple scripts in the first place, because abusers Know That Shit Will Fail
can we please get real for like. once. every week theres a new kind of stupid in the tags that could be fixed by a basic understanding of the topics we're discussing
27 notes
·
View notes
Note
NPD + (h)cDID Culture Is
Not being able to fathom other people are systems and internally accidentally fake claiming them because how can anyone else be a system? I’m the one whos been through hell. What do you mean? You must be lying.
.
#npd culture is#npd system culture is#npd + hc-did culture is#npd + cdd culture is#npd#actually narcissistic#actually npd#narcissistic personality disorder#cluster b#hc-did#hc did#highly complex did#hc did system#hc-did system#cdd#complex dissociative disorder#cdd system#fakeclaiming tw
32 notes
·
View notes
Text
SHOWERING AS A PART WITH BATHTIME TRAUMA
I am a part that has serious trauma with showers and baths. Water is scary for me, and I hate being wet, but showers are also necessary. Since I've been fronting more often, I need to learn to be okay with showers. Here's some things I think helped me.
CO-FRONT WITH AN ANP/PART WITHOUT WATER TRAUMA
I found that when I was cofronting with our host, who does not have trauma around water, showering was easier. He could offer me reassurance when I started to get scared or uneasy. He also showed me that showers are gentle and wont cause me harm. Co-fronting definitely helps a lot, especially since I didn't need to do the work, I just watched.
PLAY WITH THE WATER
I tried biting at the water, batting it around with my hands, and just generally playing with it. This helped ease the fear because it showed me that water wasn't harmful. It was just a bit warm. It can also make the experience fun rather than scary.
BE OKAY WITH YOUR FEAR
It's okay to be scared of showers, especially if you have trauma with them. I realized that my fear was okay and it wasn't something to be ashamed of. Since I could acknowledge my fear, I could then address it. You need to accept your fear before you can work on it. Denying the fear will only make things worse.
Showers are hard, but they're getting easier.
(PS I don't have a name besides my number yet, so I'll just be going by KM for now.
~ KM
26 notes
·
View notes
Text
it’s so interesting how programming just absolutely FUCKS the order and presentation of a system. like i was so certain we had osdd and there was no possible way we had did because of the immensely frequent co-conciousness that we experience, that caused us to think we don’t experience any dissociative amnesia, because “everyone always knew everything”… like yeah bitch all of the 10 alters you THOUGHT you had knew everything because they were always present to see it. going from that to knowing there are 400+ of us and that we have an insanely large headspace with a town in the mountains that literally has a fucking c/lt operating there… bruh. it’s so fucking wild.
#tw tbmc#tbmc#programmed system#hc-did#complex trauma#complex did#ramcoa#ramcoa vent#complex dissociative disorder#dissociative identity disorder
115 notes
·
View notes
Text
In spite of the endo hatred on certain sys tags, I will continue to post endo positivity in them. We are a disordered traumagenic system, and we're unaffected by endos existing. Endos don't harm 'real systems' or 'mock trauma' or whatever antis whine about. In case any nondisordered endos needed to hear that from a sys like us, there you are.
Edit: I say 'traumagenic' but our origins are more complicated than that lmao (not to mention I'm trying to let go of origin labels). It's sort of like a heavy simplified idea of things per se.
14 notes
·
View notes
Text
At the risk of creating another wave in already unsteady waters, I just want to get some clarification about a term I have seen used recently.
Hyper-Complex Dissociative Identity Disorder.
I have not been able to find any medical literature on the topic. From what I know, it is supposed to be a label describing a specific type of complex dissociative structure in systems who have undergone RAMOCA. However, I am very confused by it.
The first point of confusion is what it actually is. A lot of the structures it references, such as high fragment counts, multiple innerworlds, subsystems, ect are seemingly the same as complex-DID.
The only point that I know of that differs is that sometimes it can involve programmed alters. Which, first of all, does not inherently involve complex internal structures. Second, it seems as though it is not an inherent part of HC-DID, just a common one.
But if HC-DID involves C-DID structures + programmed alters, I fail to see how that would only be possible through RAMCOA? Now, do not misunderstand me, I know programmed alters can only happen intentionally, but I am under the impression RAMCOA refers to a very specific type of trauma. I know of someone with programmed alters from an ex of its who realised it had DID, does that mean that it underwent RAMCOA because the person intentionally programmed it? I will admit that is a grey area in my understanding, and if progamming itself inherently counts as RAMCOA I do apologise for implying otherwise.
But I also saw that it does not inherently have programmed alters and that the defining factor is that it is caused by RAMCOA. So, is it just complex-DID caused by RAMCOA? I fail to see what the unique aspect of internal structure that differentiates it from C-DID is in that case.
I even saw the definition that it was DID caused by RAMCOA in general, but RAMCOA does not inherently create complex internal structures.
I am just.
Quite lost.
54 notes
·
View notes
Text
Ok i am usually against harrasment but harrasing mfs that wanna have my trauma so bad is my fav activity :3
13 notes
·
View notes
Text







Benjamin Lawman from BEN Drowned is a gay nonbinary boy with CPTSD, HC-DID, and severe aquaphobia!
Behavioral Event Network/BEN is an aroace subsystem within Benjamin that is made up of fragments!
Link from Majora's Mask is an introject in Benjamin's system!
dni link
#benjamin lawman#ben drowned#gay#gay man#nonbinary boy#cptsd#hc-did#aquaphobia#behavioral event network#ben#aroace#subsystem#link#majora's mask#introject#creepypasta#scopophobia
13 notes
·
View notes
Note
polyfrag culture is
“If you put my system an a HC/RAMCOA system side-by-side, the only thing that would separate is is our trauma!”
a few months later
“OH SHIT-“
.
#polyfrag culture is#c did#cdd#cdid#complex dissociative disorder#complex dissociative identity disorder#did#dissociative identity disorder#polyfrag#polyfrag system#polyfragmented#polyfragmented system#polyfragmented did#hc-did#hcdid#hc did#highly complex did#highly complex dissociative identity disorder#osdd did#osddid#did osdd#ramcoa#ramcoa tw#❓
51 notes
·
View notes
Note
System culture is having HC-did and osdd1b
(one's a subsys)
.
#system culture is#anon#plurality#actually plural#actuallyplural#plural system#pluralgang#hc-did#osdd 1b
9 notes
·
View notes
Last Seen Blogs

amen-madonna
The QUEEN

hisakura-genso
HISAKURA ZBROJOVKA

oaknart
Oak n' Art

claudehenrysmootuniverse
Smooterific

clairepatroclus
take me home