#junior doctor
Text



paeds rotation is nearly coming to an end 🥹 I only hope internal medicine is not too hard on me.
#medicine#medblr#medblog#junior doctor diaries#junior doctors#junior doctor#paediatrics#pediatriccare#neonatology
87 notes
·
View notes
Text
Today in “new low in ridiculous department expectations for doctors”
I fainted on the way to work yesterday because I was strongly suggested to work despite being still sick from covid. This led to me calling in sick yesterday still half collapsed on the platform the moment I stopped vomiting.
Today, get pulled aside by an associate consultant after a seminar for resident doctors and get told off for “calling into work so late and inconveniencing people who have to cover”
I then say to her, verbatim, that “I fainted yesterday on the train on the way to work at 8:40 AM. I usually call in sick early at 7:50 am.”
Her response: to continue insisting I should have called in sooner, despite me repeating that I FAINTED. Something she, as an associate consultant, should know I have no control of.
Does she even know I probably have a case in labour law against her if I wanted to??
I’m done with the way the system uses doctors in general. I’ve done a 28 hour shift overnight on Christmas Eve before when so sick from acute gastritis I was vomiting every five minutes; I’ve worked with chills and coughing so badly even patients were terrified; when my grandfather was suddenly rushed to hospital and I took urgent leave to see him before he died, the department asked if I couldn’t finish a couple more hours of work first. I’ve pushed myself to the point of exhaustion for four years now.
People like this associate consultant don’t deserve their positions.
76 notes
·
View notes
Text
Some more pictures from Whitehall today. It's disappointing that there has been better little coverage in the media, especially little acknowledgement of the turnout and level of support.







57 notes
·
View notes
Text
Something I don’t think is mentioned enough when discussing junior doctors pay is how much we have to fork out ourselves for our training! I just had to make a payment of over £500 for my royal college of physicians training portfolio. This is on top of GMC fees, union fees, medical indemnity fees AND I have an exam to do next year that’ll be >£600 (last year I spent nearly 1k on exams too).
Not to mention the large amount of money most of us spend on commuting, seeing as we move hospitals every year.
Like surely the high costs of literally just going through training and being a doctor should be considered? It’s ridiculous
31 notes
·
View notes
Text
The biggest con of a surgeon partner is that they get stuck in the OR at the worst of times.
#i wanna go to my vacation#family med is 473727 patients a day but when my clock rings i'm free#junior doctor
1 note
·
View note
Text
What I’ve learnt from three years of Psychiatry Training
I’ve now completed three years of core psychiatry training. When I applied to medical school I knew I wanted to become a psychiatrist. When I got into medical school I used my spare time to learn more about psychiatry, using my ‘student-selected components’ and elective to immerse myself in mental health. When I became a foundation doctor I specifically asked for a psychiatry rotation and used that four-month opportunity to pick the brains of my consultant and relish in the fact that this would be my day-to-day job in the not-too-distant future. I used my taster weeks to explore the more niche areas of the speciality and travel the country, seeing how mental health could be treated so differently in the same healthcare system. During the last eight years I have attended mental health conferences, entered psychiatry essay competitions, read books on mental health, followed debates on policy and law on social media and overall fully thrown myself into the world of psychiatry.
Perhaps it is therefore not surprising that core psychiatry training was not what I expected it to be. Perhaps I had an idealistic view of what mental health care actually involved. But then I would have brief glimpses of excellent teams providing fantastic clinical care and realise that what I expected was not beyond the ordinary.
The last three years have left me drained, cynical and hopeless. I am now left with the question: what is the point of Psychiatry? Am I ‘helping’ people or actually harming them? Here are some of the things that I have experienced in my last three years of core psychiatry training that have made me question whether the career I have idealised for so long is in fact one that is slowly degenerating before my eyes.
https://www.angury.co.uk/what-ive-learnt-from-three-years-of-psychiatry-training/
6 notes
·
View notes
Text
How To Survive As An ETD / ED House Officer In The Orthopaedics Department - Housemanship in Malaysia
An article on my experience as a House Officer in the Orthopaedics Posting.
-
#housemanship #malaysia #doctors #medicine #medical #article #blogging #dailyblog #writing
Related Posts:
Pulling Through My First Tagging Experience As An Orthopaedic House Officer – Housemanship Diaries
My Daily Morning Routine As A House Officer In The Orthopaedics Posting – Housemanship Diaries
The Orthopaedics Posting – Housemanship Diaries
My “Coming Morning” Priority – Housemanship Diaries
My Support System During My First Posting In Orthopaedics As A Junior Doctor In…

View On WordPress
#blogger#blogging#blogging as a doctor#dailyblog#doctor#doctor&039;s life#emergency department#house officer#houseman#housemanship#junior doctor#Malaysia#malaysian#medical#medical officer#Medicine#orthopaedic#orthopaedics#writing
0 notes
Text
The best junior white English male doctor on the 12 of Jan 2024 at around 17
There was a junior male doctor at around 20s white English with very pale skill and brown hair mid length a bit big wave very soft with glasses. He is a star and super kind to even very humble people.
There was a white English postman around 30s or people who delivered small parcel and asked one small potato on the main lift (patients and guest area) about where is the medical school as the parcel saying medical school.
The small potato wanted to help but her legs have to go to different places and have done 11,000 steps on daily basis. Therefore, she told him medical school was not on this floor but ground floor. She asked where would he came to the 2nd floor. He replied someone told him from the ground. The small potato replied its on the ground floor but somehow it is how to direct therefore, she said "you can ask this doctor"
There were a doctor passed by and already to tap the card to the ward that next to the stair.
The doctor then turn back his head and the postman went to him then the doctor answered him patiently when the postman showed him the parcel with the address and asked the medical school
The doctor said " I don't know where is it but I can show you the signs" Then he opened the door that next to the stair and they tried to find out where was it.
Then the small potato came forward and said "I think it's UCL's medical school on the ground floor"
The doctor then said "Oh I know where it is now so come with me " to the postman
The doctor ran quickly by using the stairs because the lifts would take forever and never come. The doctor ran from the second floor to the ground to show him where is it and the all the way up to the second floor.
I have never seen people who is so down on earth and kind to humble people.
I hope this doctor will have many good things in returns as being a super kind people.
There is no way to trace who this good doctor is. He is in my mind for being so kind.
Just want to say thank you a big thank you for you. People are very lucky to have you as a doctor
1 note
·
View note
Text
Trauma call.
Content warning: this post discusses suicide.
I stood nervously in the corner of the trauma bay, a giant sticker spelling 'observer' plastered across my chest. Friday night in the emergency department. I'd been in the ED for one week now, and had so far successfully avoided being mistaken for someone who actually knows what they're doing. Can I perform different clinical exams? Sure. Can I interpret the signs and make a diagnosis? Absolutely not. Sprinkle in an emergency and life-threatening situation and you have yourself a one-way ticket to heaven (or hell), my friend. Heaven for the patient, hell for me, that is.
"Trauma call arriving," someone began, "35 year old male 'AJ' jumped off a 15 meter bridge, attempted suicide. Airway patent, he's hypotensive and tachycardic, we've so far administered..." they continued to list off his vitals and the intervention and pain relief he'd had so far. How can anyone possibly take in all of this information and then figure out what to do with it? These scenarios were far more fast-paced than the cruisey, hand-held 'simulations' we undertook in the pretend ward room. There, we had the luxury of time (and knowing we couldn't really kill anyone): we could pause, think, take time to discuss, backtrack if we needed to. Here? Not anymore. This was a real person, with real time constraints, and very real injuries. I found myself taking a small shuffle back. The trauma bay was filling up with people far more qualified than me, and I was becoming very aware that I was taking up valuable space. Here to learn? Yes. But right now, my priority was staying well out of the way.
I mentally snapped myself back into the room as the staff held AJ's head firmly in place in the C-spine collar, discussing his airway and options for resuscitation.
"Don't worry about my airway! Just let me die!" he cried out. I bit my lip. This guy was just a few years older than me. He kept echoing his desperation to die, how he didn't need to be resuscitated, how he just didn't want to exist. "Life is shit, I want to die, life is shit, life is shit," he kept repeating over, and over, and over. The pain in his voice was haunting. I can still hear it to this day.
"We're not going to let you die, mate, we're not going to do that" someone said, gently rubbing his shoulder, "we're here to help you."
From my corner in the trauma bay, I looked at AJ and felt a mixture of confusion and surprise. I guess I thought that someone who jumped off such a height would look... worse? That they'd be deformed or 'obviously' injured in some way. AJ looked distressed, of course, but had no cuts, bruises, or obvious bleeds. But that didn't mean that there wasn't damage to his internal organs.
Once the trauma team had been through their ABCDE (a protocol used in emergencies to help stabilise a patient), AJ was sedated and wheeled off to imaging to work out the extent of his internal injuries. I stood outside the CT room with the surgical team, who were making the value of their time known with constant sighs and ongoing running commentary. I dared not ask any questions about the body parts appearing on the screen.
"Oh my god, why are they so obsessed with the lower limbs?" one surgeon complained as the radiographers moved the images across the legs, "Just show us what's going on in the abdomen already!" Their exasperated comments, unsurprisingly, did precisely nothing to speed up the process. A few more minutes passed, their impatience rising like hot steam (which was almost coming out of his ears at this point). "We just need to know if we need to take him to theatre or not. This is taking f o r e v e r" he growled, rubbing his temples. Eventually, to the satisfaction of the very impatient doctors, they got the all clear that there was no internal bleeding. The surgical team scurried off into the night, just as quickly as they appeared.
Shockingly (and surprisingly), AJ had sustained just two fractures: one in his back, and one in his leg. He'd make a good recovery. But his ankle was dislocated and would need to be popped back into place.
"You're the med student, yeah?" a voice asked. I looked up.
"I, um, yeah I am..." I hesitantly began.
"Want to put that ankle back into place?" he asked. I grinned. I followed the doctor back down to the trauma bay and he showed me how to hold the big toe and lift it up, explaining that he'd help hold other parts of AJ's leg to keep everything in place.
"Alright, on 3" he started counting. One, two... I braced myself and tightened my grip on AJ's toe, "three!". I yanked the two up whilst the registrar held his leg in place. No pop. No crack. Nothing. Was I not strong enough? (I should go to the gym more, I've been saying...)
"Did it work?" I asked.
"Great job," he said, "You got it."
Z, I learned his name, was a kind emergency registrar who took me under his wing that evening, "I figure if you're here at," he glanced at his watch, "midnight on a Friday night, you're probably pretty keen and interested." He was mostly right. It's true, I had been looking forward to my emergency rotation all year; partly because it's where all the 'action' is, and also because I could attend placement at hours that were far more accustomed to my body clock. A midnight shift? You got it. 7am ward rounds for surgery rotations? Torture.
I followed Z around, and he'd send me off to patients to grab a quick history and listen to me as I presented back to him. Any opportunity to teach, he'd take. As a student, when you find doctors like this, you stick to them like toffee in your hair. It was almost 1am and we'd decided to go and see one more patient together before I headed home.
JR was a middle-aged woman who'd come in with abdominal pain and feeling terribly poorly. I watched with curiosity as Z took the reins, crouching down by the patient's chair and listening with a genuine curiosity that I'd not yet seen in the emergency department. He'd ticked off all of the standard questions: when did it start, what does it feel like, how bad is the pain, have you noticed anything else, etc. That's where, so far, most people had stopped. But Z kept chatting with her.
"Who's at home with you?" he asked her.
"Just my son and I," she replied, "My husband is fly-in, fly-out... I only see him every 6 weeks." Z nodded in a way that suggested he genuinely cared about JR's answers. She took a deep breath and paused.
"Plus my son is special needs," she added quietly, taking another deep breath.
"That must be really hard," Z gently responded. JR nodded, twisting a tissue in between her fingers. "How have things been lately?"
JR began sobbing.
She'd had a workplace incident, was suffering psychologically, and was now struggling to care for her son. JR came in with abdominal pain, but clearly had so much else going on. Z's kindness, compassion, and empathy was so terribly moving. Did his consult take a few extra minutes? Of course it did. Was it directly relevant to the abdominal pain? Not necessarily. But both myself and this lady knew that it was because Z deeply cared about his patients. It was clear that he gained a beautiful insight into his patients' lives, even if he might never see them again, and could shape their care in a way that's beyond just the 'presenting complaint'. JR expressed her profound gratitude for Z's time and comfort. I told myself in that moment to never, ever, just see the presenting complaint.
As for AJ and the trauma call? Well, it's been a few months since this night took place. He got the help that he needs and is doing remarkably well, and is so, so grateful to be alive.
In the end, it all comes down to treating the whole patient.
#med school#med student#medicine#medschool#medstudent#gamsat#med school australia#med school aus#student doctor#junior doctor#medical#medical student#medical school
0 notes
Text


FRIDAY—24TH NOVEMBER, 2023
1:36 AM
Currently I'm on call at the hospital, and I'm the only intern/junior doctor posted today. There's two residents as well. And we're looking after 45 beds, almost. It's hectic, af. I also have a case presentation in the morning, my first ever. And I am nervous. I am 24 days in and no consultants know of me yet. My goal is to get at least one LOR by the end of this this three month rotation, God willing. I hope I do well in the presentation. I hope there's some divine help. Amen. Lmao. I am super stressed and just tired and itchy. Under-slept. My eyes are burning. Let's do this. Do it tired, do it sad, do it. Just gonna have faith and go forth with the presentation and hope I make a good impression. There's defo some changes I'm bringing in myself to make the second month of my Medicine rotation more productive. Amen. Upwards and onwards. Godspeed.
#booklr#med studyblr#medical student#studyblr#biscotea tales#hustle#medical school#medical side of tumblr#medical stories#med school#junior doctor
1 note
·
View note
Text
Mario and Bowser's rivalry after 30 years: Exists mostly just to uphold the status quo, instantly dissipates whenever the situation calls for it, Peach's kidnappings probably follow a very specific schedule and after every single one they all go out for coffee together. Luigi is unironically Junior's favorite babysitter.
Sonic and Eggman's rivalry after 30 years: If You So Much As Breathe In My Direction I Am Literally Going to Kill You With My Bare Hands
#Super Mario#Mario#Bowser#King Koopa#Princess Peach#Luigi#Bowser Junior#Sonic the Hedgehog#Sonic#Eggman#Doctor Eggman#Doctor Robotnik#Straight From the Dragon's Mouth#Posts Worth a Thousand Notes
50K notes
·
View notes
Text



26-01-2024
peds rotation goes on
102 notes
·
View notes
Text
New horror stories from the medical world
Went back to work as a fourth-year family medicine resident today after flying back from holiday 48 hours ago
Still horrendous jetlag last night didn't sleep a wink
Saw 32 patients in a 3 hours and 45 minutes AM session (think that over in minutes per patient)
Mentioned to my associate consultant at lunch hour seminar (that I had to stay awake for) that I hadn't slept at all last night and her reply was "Well you woke up properly when you saw patients didn't you? Here I want you to edit this powerpoint tonight for an hour-long presentation tomorrow."
Saw another 24 patients in 2 and a half hours in PM session. Came home. Finished editing the powerpoint at 9 PM.
Sometimes when your doctor looks like she's more tired than you are it's because she is.
#my good ol' workaholic insane associate consultant#have I mentioned I'm also currently doing a diploma in dermatology that needs timed replies for an e conference offset to UK time this week#medicine#family medicine#residency#doctor#junior doctor#my post#personal#medical happenings
18 notes
·
View notes
Text
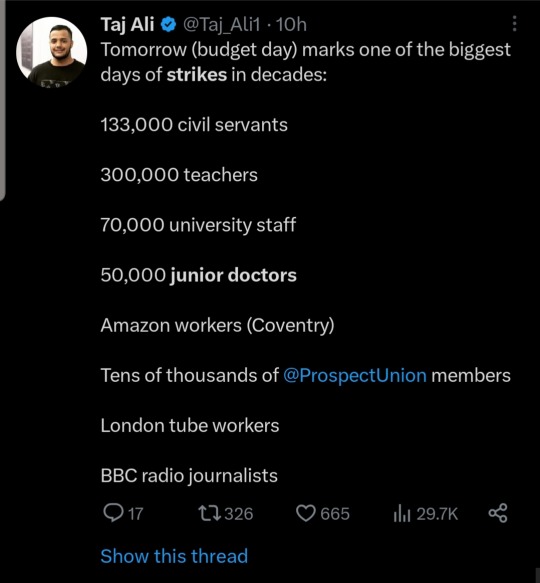
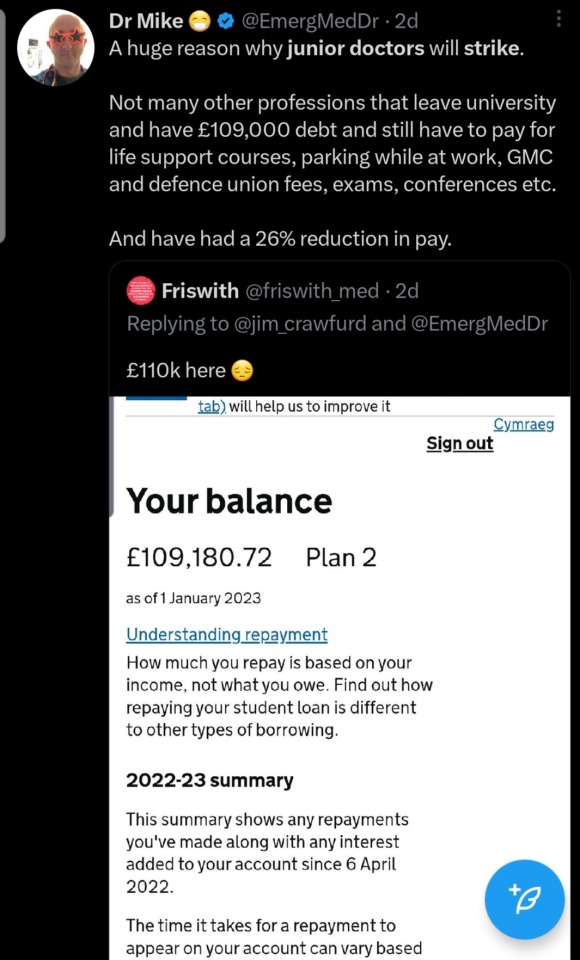
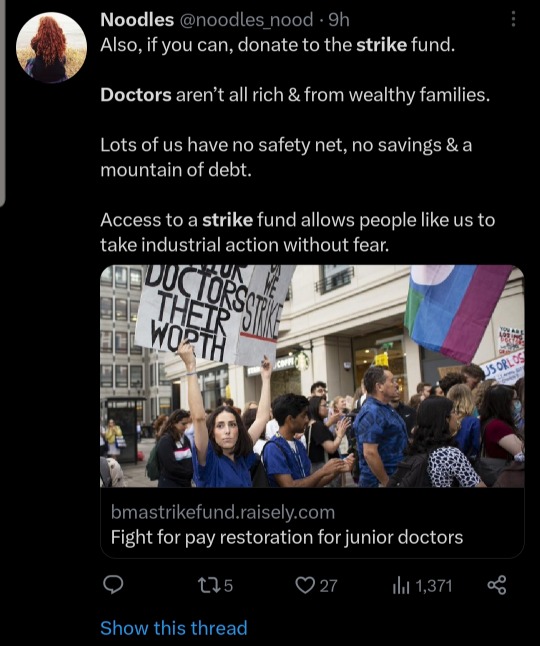
More coverage of the Junior doctor strikes on Twitter.





11 notes
·
View notes
Text
Uhh is it ok for a junior doctor/IMT in england to have bright red hair because I may have accidentally just done that
#i was going for a darker red look but#it turned out super bright?!#which is weird because my natural hair colour is really dark#medblr#junior doctor
3 notes
·
View notes
Text
Slight fever with pain in abdomen and nausea. Shitty breakfast and a can of monster or covid? Let's hope it's the first. If I stayed healthy for two years only to catch covid while on vacation I am going to kill myself. Or quit. Whatever comes first.
#marya personal#buying test in the morning#i am leaning towards the first but this fever is worrying me and I had been in contant with covid patients#i just want my vacation 😭😭😭😭😭#i'm so over this stupid job#i have time off from last year i wasn't able.to use#medblr#junior doctor#er doctor
9 notes
·
View notes
Last Seen Blogs
heartharrow
Living My Best Life.

suchawrathfullamb
such a wrathful little lamb

cyberorganism
upload blog

lesjoursdepluietoujours-blog
Les jours de pluie, toujours.

chocopat
^_^