#history of immunology
Text
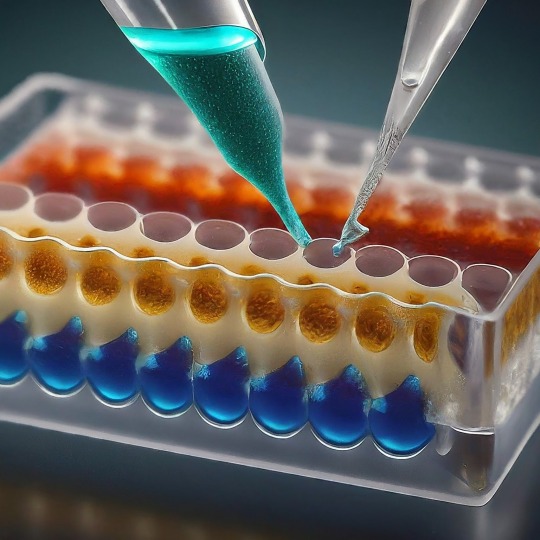
ELISA: A Powerful Tool for Detecting the Invisible
ELISA, or Enzyme-Linked Immunosorbent Assay, has become a cornerstone of medical diagnostics and biological research. This versatile technique allows scientists to detect and quantify minute amounts of target molecules, such as proteins, antibodies, and even viruses, with remarkable accuracy. In this blog, we'll delve into the world of ELISA, exploring its various types, its applications, and the exciting future directions this technology holds.
At its core, ELISA relies on the exquisite specificity of antibodies. Antibodies are highly specialized proteins produced by the immune system in response to foreign invaders. Each antibody can bind to a unique structure, called an antigen, on a specific molecule. In an ELISA, scientists leverage this binding property to create a sensitive detection system.
The 1960s witnessed a surge in interest in immunoassays, techniques that utilize the specificity of antibodies to detect target molecules. One such technique, radioimmunoassay (RIA), developed by Rosalyn Yalow and Solomon Berson, revolutionized medical diagnostics. RIA used radioactively labeled antibodies to detect antigens, offering high sensitivity. However, concerns regarding the safety of radioactive materials fueled the search for a safer alternative. The year 1971 marked a turning point. Independently, Eva Engvall and Peter Perlmann published their work on a novel technique – the enzyme-linked immunosorbent assay (ELISA). ELISA replaced radioactive labels with enzymes, eliminating the safety concerns associated with RIA. Like RIA, ELISA harnessed the specific binding between antibodies and antigens. However, it employed enzymes that could generate a detectable signal, such as a color change, upon interacting with a substrate. This innovation paved the way for a safer and more user-friendly diagnostic tool.
The basic ELISA protocol involves immobilizing the target antigen on a solid surface like a plate well. Then, a sample containing the molecule of interest (e.g., a suspected virus) is introduced. If the target molecule is present, it will bind to the immobilized antigen. Next, an antibody specific to the target molecule, linked to an enzyme, is introduced. This "detection antibody" binds to the target molecule already attached to the antigen. Finally, a substrate specific to the enzyme is added. This antigen-antibody binding is visualized using an enzyme linked to a reporter molecule. When the enzyme encounters its substrate, a detectable signal is produced, such as a color change or luminescence. The intensity of this signal is directly proportional to the amount of antigen present in the sample, allowing for quantification.
The beauty of ELISA lies in its adaptability. Several variations exist, each tailored for specific detection needs.
The Four Main ELISA Formats are:
Direct ELISA: Simplicity at its finest. In this format, the antigen is directly coated onto the ELISA plate. A labeled antibody specific to the antigen is then introduced, binding directly to its target. After washing away unbound molecules, the enzyme linked to the antibody generates a signal upon addition of the substrate. Direct ELISA offers a rapid and straightforward approach, but sensitivity can be lower compared to other formats due to the lack of amplification.
Indirect ELISA: Unveiling the Power of Amplification. Similar to the direct ELISA, the antigen is first coated onto the plate. However, instead of a labeled primary antibody, an unlabeled one specific to the antigen is used. This is followed by the introduction of a labeled secondary antibody that recognizes the species (e.g., mouse, rabbit) of the primary antibody. This two-step approach acts as an amplification strategy, significantly enhancing the signal compared to the direct ELISA. However, the presence of an extra incubation step and the potential for cross-reactivity with the secondary antibody add complexity.
Sandwich ELISA: Capturing the Antigen Between Two Antibodies. Here, the capture antibody, specific for one region of the antigen, is pre-coated onto the ELISA plate. The sample containing the antigen is then introduced, allowing it to be "sandwiched" between the capture antibody and a detection antibody specific for a different region of the same antigen. A labeled secondary antibody or a labeled detection antibody itself can then be used to generate the signal. Sandwich ELISA boasts high sensitivity due to the double-antibody recognition and is often the preferred format for quantifying analytes.
Competitive ELISA: A Race for Binding Sites. In this format, the antigen competes with a labeled antigen (usually a known amount) for binding sites on a capture antibody pre-coated onto the plate. The more antigen present in the sample, the less labeled antigen can bind to the capture antibody. Following a washing step, the amount of bound labeled antigen is measured, providing an inverse relationship between the signal and the concentration of antigen in the sample. Competitive ELISA is particularly useful for studying small molecules that may be difficult to directly conjugate to an enzyme.
ELISA's Reach: From Diagnostics to Research. The applications of ELISA are as vast as they are impressive. Let's delve into some key areas where ELISA plays a vital role:
Unveiling the Mysteries of Disease:
Diagnostics: ELISA is a cornerstone of diagnosing infectious diseases like HIV, Hepatitis, and Lyme disease. It detects antibodies produced by the body in response to the invading pathogen, providing valuable information for early detection and treatment.
Monitoring Autoimmune Diseases: ELISA helps monitor autoimmune diseases like rheumatoid arthritis and lupus by measuring specific antibodies associated with these conditions.
Cancer Screening: Certain cancers can be detected by identifying tumor markers, proteins elevated in the blood of cancer patients. ELISA assays are being developed to detect these markers for early cancer screening.
Safeguarding Food Quality:
Allergen Detection: Food allergies can be life-threatening. ELISA ensures food safety by enabling the detection of allergens like peanuts, gluten, and milk in food products, protecting consumers with allergies.
Monitoring Foodborne Pathogens: ELISA can identify harmful bacteria, viruses, and toxins in food, preventing outbreaks of foodborne illnesses.
Environmental Monitoring:
Pollutant Detection: ELISA can detect pollutants like pesticides and herbicides in water and soil samples, contributing to environmental protection efforts.
Microbial Analysis: This technique can be used to identify and quantify specific microbes in environmental samples, providing insights into ecosystem health.
Research and Development:
ELISA plays a crucial role in various research fields:
Drug Discovery: It helps researchers assess the effectiveness of new drugs by measuring drug-target interactions and monitoring drug levels in the body.
Vaccine Development: ELISA is instrumental in developing vaccines by evaluating immune responses to vaccine candidates.
Basic Research: Scientists use ELISA to study various biological processes by detecting and quantifying specific molecules involved in these processes.
Despite its established role, ELISA is evolving alongside technological advancements. New multiplex platforms allow for the simultaneous detection of various targets in a single sample, boosting efficiency in biomarker discovery and disease analysis. Automation streamlines workflows minimizes errors, and increases throughput, making high-throughput screening feasible in drug development and clinical settings. Miniaturization and portable devices enable rapid on-site diagnostics, providing healthcare professionals with real-time data for quicker interventions. Additionally, ongoing research is improving assay sensitivity, reducing background noise, and expanding detection limits, allowing for the identification of trace analytes and early disease biomarkers with greater accuracy than ever before. Integration of ELISA with emerging technologies such as microfluidics, nanotechnology, and artificial intelligence holds promise for enhancing assay performance, scalability, and data analysis capabilities.
These advancements hold promise for even wider applications of ELISA in the future. ELISA has revolutionized our ability to detect and quantify biological molecules. Its versatility, accuracy, and adaptability make it an invaluable tool across various scientific disciplines. As research continues to refine and innovate ELISA techniques, we can expect even more exciting possibilities to emerge in the years to come. ELISA's future is bright, promising to play a pivotal role in unraveling the mysteries of the biological world and improving human health.
#science sculpt#life science#molecular biology#science#biology#artists on tumblr#ELISA#immunology#immunotherapy#diagnostic management software#diagnosticimaging#history of immunology#scientific advancements#biotechnology#scientific research#scientific equipment#scientific instruments#techniques in biotechnology#scientific illustration#lab equipment#sciencenature#laboratory#lab skills#molecular diagnostics market
11 notes
·
View notes
Text
Snippets—Women and autoimmune disease, the first wine, early Americans, and how cats purr
For Sunday: snippets of science news on some of my favourite things in life (well, the favourite things we can talk about in polite company): cats, wine, and humans in the Americas, plus one of my ongoing personal concerns, autoimmune disease. Some weight
Some of this stuff dates from late last year when I was too busy with Menewood stuff to comment. But as some of my favourite things in life (well, the favourite things we can talk about in polite company) are cats, wine, and history, and as one of my ongoing personal concerns is autoimmune disease, I thought, Eh, let’s combine them. We’ll start with the weighty stuff first then lighten up a…
View On WordPress
2 notes
·
View notes
Text
its actually nuts how missing a single vaccination has shaped my entire fucking life. like not only would I not be deaf if I had gotten it on time but I probs wouldn't have adhd either 🫣
#like yeah I have a family history of adhd but im pretty sure the current model suggests u can be genetically *predisposed* but the actual-#development of adhd is thought to be closely linked to environmental 'triggers' like childhood stress or head injuries lol#or in my case brain trauma. fun fact: a suspected 62% of kids who survive hib meningitis later develop adhd symptoms#vs. 5% incidence in the general population.....#when I first heard that I was still in denial bc i thought of adhd as a 'natural' condition like ur just born that way#so if meningitis survivors displayed symptoms that didnt mean they were ACTUALLY adhd. except literally all adhd is-#is a collection of symptoms its not some tangible 'switch' thats flipped in some ppl and not others. maybe thats a rly obvious statement-#but I found it kinda hard to get my head around. i guess just bc of how a lot of psychology is viewed by the public innit#anyway being deaf + nd kinda fucking sucks yall better be jabbing ur babies with every vaccination possible or im coming for ur knees#its funny bc it sounds like im saying watch out !! vaccination may PREVENT neurodivergence NOT cause it !!#*andrew wakefield voice* u wouldnt want a child with autism#but thats not what i meaaaannn obvs ur kid not getting xyz disease that could kill them is the number 1 most important thing#its so cringe actually bc hib b incidence has been down to abt 2 in every 100 000 babies since the vax was introduced in 1985#so I was one of like. probably less than 10 babies to get it in the fucking country and they misdiagnosed me a bunch of times#bc it was so uncommon + I had some rarer symptoms plus the only way to actually CHECK is to test spinal fluid which is a faff#if theyd realised earlier then i also wouldnt be deaf bc it wouldnt have been as severe. just a series of unfortunate events i guess#anyway. immunology is so fascinating i wish id focused on it more in my degree tbh#over and OUT#.diaries
6 notes
·
View notes
Photo

Camille Guérin was born on December 22, 1872. A French veterinarian, bacteriologist, and immunologist who, together with Albert Calmette, developed the Bacillus Calmette-Guérin (BCG), a vaccine for immunization against tuberculosis. He started as a technician in charge of preparing Calmette’s serum (antivenom against snake bites) and the vaccine against smallpox. After losing his father and wife to tuberculosis, he devoted himself to research on a vaccine. He discovered in 1905 that the bovine tuberculosis bacillum, the Mycobacterium bovis, could immunize the animals without causing the disease.
#camille guerin#tuberculosis#vaccines#immunology#bcg#bacillus calmette-guerin#vaccine#science#science history#science birthdays#on this day#on this day in science history
3 notes
·
View notes
Text
The Black Death working copy
0 notes
Text


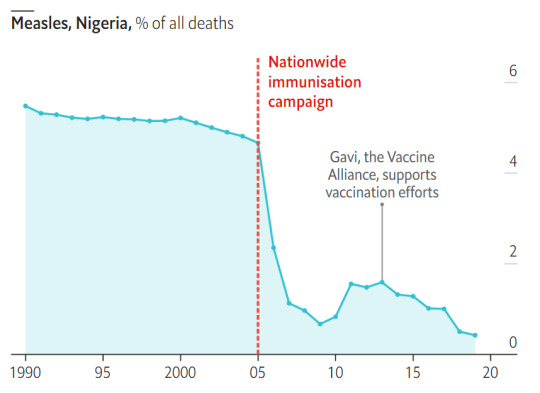
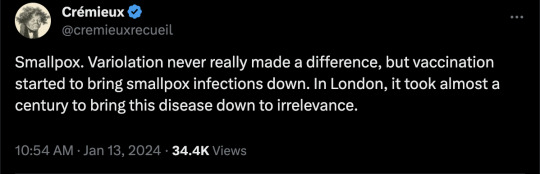
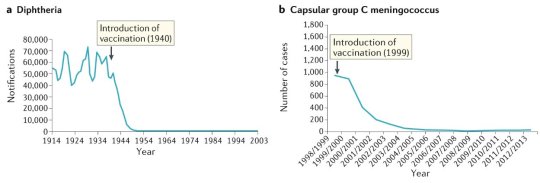




#vaccines#polio#measles#smallpox#diphtheria#meningococcal meningitis#haemophilus influenzae type B#pertussis#vaccine hesitancy#anti vaxxers#anti vax movement#antivaxers#COVID vaccine#anti vaccination#anti vaccine#science#medicine#religion is a mental illness#immunology
250 notes
·
View notes
Note
Hi! Sorry to bother you with this - I checked your FAQ and MCAS tag and if the answers are there already I apologize for missing them! But I was wondering if you have a masterpost or similar with basic info on MCAS (what it is, how to figure out if you have it, what to do...) anyway thank you for posting so much about this, I'm learning a lot ^^
Hello! I don't have a list because if I started typing one out, I'd never stop. The Healthline article about it, however, is fairly comprehensive for the basics.
One thing the article doesn't list is that MCAS can also be a source of deep, deep tissue pain (sometimes I swear it's coming from my bones). Some recent research has linked unstable mast cells to fibromyalgia, which is why you'll often find a lot of anecdotal stories online about the two being co-morbid. MCAS can also be more likely in people with EDS or hypermobility spectrum disorder and can sometimes also be a source of dysautonomia. (Honestly, it's a bit chicken vs egg sometimes.)
They may have updated their criteria since the last time I checked, but the American Academy of Allergy and Asthma & Immunology used to list anaphylaxis as a requirement for diagnosis, but that is not true.
Many people experience MCAS without ever going into full anaphylactic shock.
They also used to stipulate that diagnosis was based on elevated tryptase tests, which is not accurate for MCAS. The tryptase tests are meant for diagnosing mastocytosis, which is like the big cousin disorder of MCAS. Most knowledgeable MCAS doctors now diagnose based on a history of symptoms and response to elevated doses of h1 and h2 antihistamines, as well as other mast cell stabilizers.
TMS for a cure has a lot more info, as well as a patient resource portal that includes a list of physicians, support groups, and ER protocols.
I'd highly rec having a read-through at some point.
Hope that helps!
249 notes
·
View notes
Text


On April 8th 1973 Glasgow University appointed Delphine Parrot as head of the Department of Bacteriology its first female professor in its 522 year history.
Born in London, Parrott graduated in 1949 with an honours BSc degree in Physiology from Bedford College, University of London. She undertook her PhD at King's College Hospital Medical School and graduated in 1952.
From 1952 to 1954 Parrott worked at the MRC Clinical Endocrinology Research Unit in Edinburgh, before returning to London to join the staff of the National Institute for Medical Research in Mill Hill. In 1960, she moved to the Imperial Cancer Research Fund in Mill Hill. She worked on the problems of immune (rejection) reactions to transplants and of the movement of blood cells, especially lymphocytes, involved in inflammation reactions. She also studied the immunology of leukaemia and the effects of the removal of the thymus on immune reactions.
On this day in 1973 Parrott was made Head of Department and later Gardiner Professor of Bacteriology (later known as the Gardiner Chair of Immunology).
Delphine Parrott retired in 1990. She died on 17th January 2016.
7 notes
·
View notes
Text
What Does the Beginning of Monkeypox Look Like?
Recently, there has been concern over monkeypox, an uncommon viral disease. Knowing the initial symptoms is essential for prompt action and management.
Let’s read more into the initial stages and explore what are the first signs of monkeypox.

What Does the Beginning of Monkeypox Look Like?
1. Fever and Headache
The sudden elevation of body temperature is frequently suggestive of the start of monkeypox. A common first sign is a fever, which is frequently followed by a chronic headache. Attention is necessary because these mild symptoms could first be confused for other frequent illnesses.
2. Fatigue and Muscle Aches
As the infection spreads, people may become fatigued and develop widespread muscle aches. It is possible to confuse these symptoms for the flu or other viral diseases. But the confluence of fever, headache, exhaustion, and aches in the muscles ought to cause concern and necessitate more research.
3. Swollen Lymph Nodes
In its early stages, swollen lymph nodes are a hallmark of monkeypox. These tiny, bean-shaped structures are essential to the immunological response of the body. The armpit, groin, and neck areas are where the swelling is most frequently visible.
4. Skin Lesions
The development of skin lesions is one of the unique monkeypox symptoms. Like chickenpox, these lesions usually begin as elevated bumps that develop into blisters. The body's parts may be affected by the lesions, which may be broad.
5. Respiratory Symptoms
In addition to respiratory symptoms like coughing and shortness of breath, it can also cause these. It is important to pay attention to these symptoms as they may indicate how the virus is affecting the respiratory system.
6. Eye Redness and Sensitivity to Light
Some people who have this may get increased light sensitivity and ocular redness. These ocular symptoms may add to the overall clinical picture and might be especially uncomfortable.
7. Gastrointestinal Issues
The early signs of monkeypox can include vomiting, nausea, and stomach pain. When paired with other distinctive indicators, these gastrointestinal symptoms add even more complexity to the diagnosis.
Read: The Advantages of Home Remedies over OTC Medications
Monkeypox Prevention and Seeking Medical Attention
The health of the population depends on stopping this from spreading. Maintain proper hygiene by washing your hands frequently with soap and water. Steer clear of animals that might be viral carriers, particularly in areas where disease is common.
It goes without saying to get medical assistance as soon as possible if you or someone you know has any of the aforementioned symptoms. Make contact with your physician, let them know about your symptoms, and offer any pertinent travel or exposure history.
Early detection lowers the danger of transmission to others by enabling the implementation of suitable isolation measures.
Diagnostic Tests and Monkeypox Treatment
A thorough patient history, laboratory testing, and clinical evaluation are all used in the diagnosis of monkeypox. For confirmation, polymerase chain reaction (PCR) testing, virus cultures, and blood tests are frequently used.
Although there are not many particular antiviral drugs for this disease, supportive care is essential. This could involve taking care of symptoms, avoiding bacterial infections that spread, and drinking enough water. Hospitalization may be required in extreme situations.
Public Health Measures
Coordinated public health measures are needed to stop the spread of the virus during monkeypox epidemics. This entails tracking down contacts, isolating afflicted people, and launching vaccination drives in areas where the illness is endemic.
To increase awareness of preventative actions and early symptom recognition, public health education is also important.
Is Monkeypox Curable?
Yes, although monkeypox is a dangerous sickness, it is usually a self-limiting disease, meaning that it often resolves without the need for special treatment. The majority of this disease victim recovers completely in a few weeks. Yet the disease's severity might vary, and in certain situations, medical attention can be required.
Monkeypox cannot be specifically treated with antivirals; nevertheless, supportive care can be given, such as symptom and consequence management.
Early Detection for Timely Treatment
Understanding the initial indications of monkeypox is essential for prompt detection and suitable medical attention. The key is to identify the combination of fever, headache, exhaustion, muscular aches, swollen lymph nodes, skin lesions, respiratory symptoms, eye redness, and gastrointestinal problems, even if these symptoms may match those of other prevalent illnesses.
For an accurate diagnosis and course of treatment, it is imperative that you or someone you know get medical help as soon as possible if you notice these symptoms. Recall that early identification can have a big impact on how cases of monkeypox turn out. Remain educated and watchful.
(more)
15 notes
·
View notes
Text

A Journey Through Our Defenses: A Dive into the History of Immunology
The human body possesses an extraordinary ability to resist disease, a complex system known as the immune system. Our understanding of this intricate network, however, has evolved significantly over time, shaped by both ancient observations and groundbreaking scientific discoveries. From the ancient Greeks observing immunity after the plague to the cutting-edge research on immunotherapy, the history of immunology is a captivating saga of human curiosity, scientific breakthroughs, and the relentless pursuit of understanding our body's remarkable defense system.
The earliest observations of immunity date back to ancient civilizations. The Chinese practiced variolation, a process where dried smallpox scabs were blown into the nose to induce mild illness and subsequent immunity. Similar practices existed in India and Africa, demonstrating an intuitive understanding of acquired immunity. In 430 BC, Thucydides, a historian of the Athenian plague, noted that recovered individuals could safely care for the sick, suggesting an early recognition of disease resistance. The turning point in immunology arrived in 1796 with Edward Jenner, a British physician. Observing that milkmaids who had contracted cowpox were resistant to smallpox, he conducted a daring experiment, inoculating a young boy with cowpox pus. The boy developed a mild illness but remained protected from the deadly smallpox, marking the birth of vaccination. Jenner's work paved the way for further research into understanding immunity and developing vaccines against other diseases.
The 19th century saw significant progress in understanding the immune system's mechanisms. Louis Pasteur, a French microbiologist, developed vaccines against cholera and rabies, further solidifying the role of vaccination in disease prevention. In 1880, Ilya Mechnikov, a Russian biologist, discovered phagocytes, white blood cells that engulf and destroy pathogens, earning him a Nobel Prize in 1908. Emil von Behring and Shibasaburo Kitasato identified antibodies in the blood of vaccinated individuals, revealing the humoral immune response, where specific molecules target and neutralize pathogens.
The 20th Century: A Golden Age of Immunology:
The 20th century witnessed a revolution in immunology. Karl Landsteiner discovered blood groups, leading to safer blood transfusions. Peter Medawar elucidated the concept of self-tolerance, explaining how the immune system distinguishes self from non-self. The discovery of T cells and B cells by Jean Dausset, Peter Doherty, and Rolf Zinkernagel unraveled the intricacies of the adaptive immune system, where lymphocytes tailor their response to specific pathogens. These breakthroughs paved the way for organ transplantation, autoimmune disease therapies, and the development of new vaccines.
21st Century: Expanding Horizons:
The 21st century continues to push the boundaries of immunology. Monoclonal antibodies, engineered to target specific molecules, revolutionized cancer treatment and immune-based therapies. The Human Genome Project provided invaluable insights into the genetic underpinnings of the immune system, opening doors for personalized medicine. Research on immunotherapies harnessing the body's own immune cells to fight cancer and other diseases is rapidly evolving.
The history of immunology is a testament to human curiosity and ingenuity. From ancient observations to modern marvels, our understanding of this intricate system has transformed healthcare and continues to evolve. As we delve deeper into the mysteries of the immune system, we unlock the potential for even more effective treatments and preventive measures, paving the way for a healthier future for all. The history of immunology is a wild ride, filled with brilliant minds, bizarre experiments, and discoveries that continue to shape our world. And the best part? This story is still being written, with each new chapter promising even more amazing advancements in the fight to keep us healthy.
#science sculpt#life science#science#molecular biology#biotechnology#immunology#artists on tumblr#immunotherapy#scientific illustration#scifiart#curiosity#narrative#create#concepts#history of immunology#medical school#medical science
3 notes
·
View notes
Text
classes i’m taking this coming semester as a senior biology major, specializing in microbiology:
cell & molecular biology
human physiology
immunology
all of these are 3 credits for lecture, 1 credit for lab, giving me 12 credits
plus an online history class (3 credits), studio art (2 credits), and 1 credit for my on-campus job as a microbiology lab tech
total semester credit load: 18
41 notes
·
View notes
Text
Lilith's classes
Odalia used everything in her power to get Amity a place under a Coven Head's training. Though she would've preferred someone else, Lilith was the Emperor's Coven leader. Personal history or not, that was the best for the family. However, her ideas of rigid, ruthless training were a bit off...
Lilith's training was indeed tough, but when Amity got admitted, she was just a five-year-old and way under the age limit. The Head Witch knew she couldn't just use the same methods. So she got in contact with Bump to talk with some of Hexside's teachers and learn a bit from them.
Clawthorne's plan was to follow the school's curriculum, focusing on really reinforcing the basics so the child could build upon it steadily and faster, later. So, while Odalia hoped they were forcing her daughter to sit still and recite the Magic Law, something else was going on... Something like:
Nursery Rhymes! Lilith knew a thousand Nursery Rhymes that taught kids the basics of magic, history, and science. She picked the ones she considered best and would always sing them with Amity at the beginning of class, teaching her the hand gestures and what they meant. It was heartwarming to see the child learning the lyrics and following her excitedly. Lilith was scared she would be too embarrassed to do the dances and that Amity wouldn't join her, but the little girl watched her teacher with her eyes glistening and a big smile.
Drawing and painting! Lilith would bring images of the Isles for them to draw and color. She first focused on the whole Titan, then on specific parts of their body to help Amity get a better understanding of their geography and Titan biology. She also knew, as a future Abomination Coven member, Amity needed to develop geometrical and observation skills to correctly summon and build golems that looked the way she wanted them to look. It was a challenge, and most of the little girl's first drawings were an abstract mess. Lilith toned down the requirements and asked Amity to focus on basic shapes first. This helped the child greatly and soon she memorized the looks of many geographical spaces and demons.
Physical games! Body Awareness and Balance were the only subjects outside of the common school curriculum that Lilith taught, going hard on extra teachings. As someone who never had this type of specialized learning in her youth and had to teach herself later on to survive the Coven's training, she intended to make sure every student of hers would be prepared, and Amity was the first one that would grow up with such nurturing. There were plenty of physical exercises whose intent was to strengthen the witches' bodies and prepare them to endure magical attacks from others and themselves. Specific knowledge ensured that the individual could work smarter with her stamina, reserving as much of it as possible to keep their bile sack from exhausting itself. For most people, it would've seen like senseless training, but every crazy-looking exercise had a point. Amity loved the time they spend doing the exercises and was the only moment she was actually allowed to roll on the grass and be under the sun. Odalia wasn't happy when she found her child dirty and pink from the heat, but Lilith did notice an increase in Ames' immunological system after they began 'playing' outside.
#toh#the owl house#toh headcanon#the owl house headcanon#amity blight#lilith clawthorne#odalia blight#a coven head's apprentice au#my hobby is to imagine their classes#lilith is a great teacher and wonderful mother figure#amity is a dream child#they make me soft#owl house
37 notes
·
View notes
Text
hold the fuckin phone here lads
i had a consult with rheumatology/immunology re: long tall short fat covid, and i went to a PA who was .... let's call it distracted? by the fact that I have prediabetes markers
which, frankly, duh, my mom's entire family are diabetic or prediabetic, my father's (v small) family was Skinny Diabetics -- my genes mean it's a matter of if not when (ETA: "not if BUT when" and/or "when not if". cripes. it took three goes to get this right. see below re: 65% rate of braining good.)
(and like sidebar if everyone in my family got breast cancer nobody would be sitting there like ooooooohhh make sure you're getting enough CARDIO whilst RECOVERING FROM A LIFE ALTERING FATIGUE DISORDER)
anyway there were a couple ..... blood orange flags? things that I wouldn't appreciate from my PCP, but from a specialist? sure whatever, maybe you have really solid evidence that this particular supplement is worth a try. I was coping with Robitussin for a while there.
but!!!!!!
she also gave me some studies to look through, which, hah, thank you, my brain works 65% of the time, but hey, sure, the musculoskeletal effects of diabetes mellitus might be helpful.
Bitch it's chiropractic!!!!!
the principle author is from the TEXAS CHIROPRACTIC COLLEGE
it's published by the JOURNAL OF THE CANADIAN CHIROPRACTIC ASSOCIATION
putting aside the teeny tiny minor issue that I do not at present actually have diabetes mellitus whY are you giving me chiropractic advice
when I took some of what she said back to my pcp (who remains, as ever, the fucking best), she was like "Um. No. No that doesn't track." At the time I was willing to accept that okay, we've taken a rheum/immun tactic off our list, we can go back to Neuro. But now I'm sort of thinking that hi. Hello. Maybe we really didn't spend enough time on the Immediate Family History of Bonkers Rheumatological Issues.
I'm tired. And my hands won't stop being tingly.
#neuro follow up last week was annoying in that I sat in the exam room for 45 minutes reading about shih tzus#and he came in and pretty much went .......... yep. keep going.#I counted and admittedly I take smaller sizes of pills for Not Taking Horse Pill reasons#but I take at least 17 pills a day#More on bad days!#anyway#long tall short fat covid
5 notes
·
View notes
Text
Time Traveling Anthropologists update
In honor of having 2 people on my tag list, meaning it now meets the actual definition of a list, I thought I’d let y’all know where I am on this project.
Part 1: Actual Writing
I am deep into chapter 2. Chapter 1 covered Esther’s first day of work. We learned a bit about how the world works in the 2080’s and met her team. This book takes place almost entirely in the past, but future volumes will explore the future more. So, let’s meet the team!
Esther Dahan: 24 years old. The POV character. Esther is outgoing and a bit awkward. She can be intense and has something of a temper but cares deeply about equity. She is the team linguist, unofficial fighting/weapons expert, and generally ends up being in charge of daily life routines. She speaks 6 languages fluently but is also in charge of collecting linguistic rules for languages that no one knows today. She’s Jewish—there are no borders anymore, but her great-grandparents on her mother’s side were from Russia and her father’s family was from Israel. She’s bisexual. When not in the past, she lives with her parents because renting an apartment only to give it up every year or two would be impractical.
Tony Mourad: 24 years old. He is a bit goofier, fond of lightening the mood, but can also be genuine. Like Esther, he’s pretty loud in general and intense about things he cares about. They will become best friends over the course of this book. He is the expert on fashion, fabric, and and manufacturing history. His hobby is the history of clocks and calendars. He is Muslim and, though he grew up in LA, his family is Iraqi and his mom was born there (when it was still Iraq; the no borders thing is pretty recent). He’s gay and currently rents a small house with his brother, which his wages continue to help with when he’s gone for work.
Valentina Pérez: 25 years old. In this book she’s generally fairly grumpy, distant, and cool. There are reasons for this and they are Spoilers and she’ll be less so in the future. She mostly keeps to herself and is much less interested in the studies they’re doing than her teammates. Her job isn’t even anthropological; she’s the team scientist. This involves multiple jobs actually that they’re just lucky they have a single person qualified for all of them. Her main duties involve sending data home using the circuits in the Time Machine, doing general maintenance on it, and keeping them healthy. She is not a doctor but she has studied immunology and is in charge of vaccines, basic medical care, and the decision when a situation requires returning early for proper care. However, most of those jobs aren’t constant, so she’s always getting drawn into the work of the others and having to observe or write up things for them. She’s a lesbian, has a 2-year-old daughter, and has been married for 7 months to her wife. She’s from Cuba and learned English in college. Their office is based in New York, so their work is mostly in English, but widespread speaking of other languages is more acceptable, so around the office there are plenty of people she chats in Spanish to.
Minerva Myerson: 39 years old. Unlike the others, she isn’t new to the office but joined at its inception 6 years ago. She has been on 3 previous missions and was made a team leader when the religious studies department expanded. She’s generally good humored, charming, and has a fairly loose leadership style. She does get snappy when people break the rules that are there for good reasons, but is otherwise fairly even tempered. Yes this is a little loose and I will develop her character more soon. Her specialization is food history, including how food fits into cultural contexts and the expectations surrounding eating. She’s also formatting and compiling the ethnography, since she has previous experience. She is a black trans woman from New Orleans who lives alone with no kids so she actually does rent apartments temporarily in between time traveling. I think she’s straight, but again am still developing her character.
Chapter 2 has a time skip—16 months in their personal time and 4 months into their time traveling mission. So far we’ve explored the city of Samandar a little, markets and the walls and the way houses work. They have a fairly expositional team meeting and then, a couple days later, Esther is taken by her 3 unofficial “guides” on an expedition to meet warriors returning from the capital of Atil. Her guides are 3 12-year-old girls largely because they have the time and interest to share their lifestyle with a foreign stranger. Also because I thought it would be funny to have 9th century horse girls. So they go to the corral and discuss horse care, which I 100% made up but I think is plausible. Next the men will return and Esther will start talking to Boker largely to fact check the kids’ excited reports on the way warriors work.
Part 2: Outlining
I split the plot into 3 sections: murder, mystery, and [redacted]. I finished the outline for the first part, which actually focuses on anthropology and romance and culminates in the murder, and now I’m working on the second part. As I said before, I haven’t written a mystery before and I think some hints and evidence are going to probably be added in later drafts. I have, though, come up with the first 2 suspects and the actual guilty party. I’m just beginning to figure out who says what and what evidence they discover.
Thank you for listening if you made it to the end of this post! I just realized I haven’t talked much about it yet since I’ve been writing.
Tag list: @amielbjacobs @kingkendrick7
10 notes
·
View notes
Text
🥳🥳
I'm really happy.. feels like an understatement I have been heard And we are investigating my shit immune system!!
🥳🥳
😅For those that want the deets😅
I met with my new Hematologist.
He wanted to go over my ITP history FROM THE BEGINNING! He was shocked how much I had in my head without notes.
I told him what treatments have yielded no platlet responses over the years and how most my drops since 2013 have been immune system triggered or medication triggers (like vaccinations)
He wanted me to take a daily med that stimulates the bone marrow to produce more platlets but these meds have only been out 10 years and were approved as orphan drugs. I have followed these meds the last ten years. I'm not on board with these. MORE SO, I DO NOT have Chronically low numbers. Mine are event drops.
This HOUR long, one on one appointment with him ended with him agreeing that
* I am on top of this
*I manage this condition well
*I can have IVIG infusions when i drop below 20
AND! AND!
since it's tied so to my immune system,
My severe infection history & routine home mitigation, & I respond SO WELL to IVIG w/o roids I am being sent to the immunology department to be checked for IgG Deficiency, CVID & other autoimmune issues. They will follow up with rheumatology should they find anything but both referral sent.
I already have intake appointment with them! I know this isn't likely going to be a fast thing but the possibility of some answers and maybe not end up in the hospital when I get sinus infection or UTI would be really nice.
#itpwarrior#platelets#immune thrombocitopinia purpua#idiopathic thrombocytopenia#autoimmine disease#trachel stenosis#fibromyalgia#CVID#igg deficiency#ivig#iv infusion therapy
4 notes
·
View notes
Text
By: PITT
Published: Sep 30, 2023
Our son recently started graduate school. He began hormone therapy during his final year of undergraduate education. Because he began to identify as a lesbian, transgender woman at 20 and showed no sign of gender dysphoria before that, we never had a chance to reflect – or advise him – on his choices. Going through the published medical research on the effects of estrogen made me aware that psychologically, excess estradiol in the serum causes depression among males, and physiologically, there are potentially much more severe side effects, including some impacting the brain and the immunological system. More of that in a minute.
Fast forwarding to the present day, before our son left for graduate school at a University with one of the country's most renowned medical schools. I decided to write to their student health center and share the studies I had found and, more relevantly, the psychological history of our child. What follows is the text of the letter and, after deleting potentially identifying information, the response from a high-ranking official within the health center. They are, for the lack of a better phrase, quite revealing.
First, my letter (I have not disclosed the name of the university and have changed the name of our child here, with apologies to the real Jonathans of the world; furthermore, apologies for the triggering usage of pronouns – I did not want to be dismissed as the “usual, hateful, bigoted transphobe”; rather, I wanted to be considered as the deadly serious parent who would do anything in their power to prevent their child from coming to harm):
-
Dear Apex University Health Center,
Our child, Jonathan, who is joining the graduate program at Apex University this Fall, identified themself as transgender during their sophomore year in college (2021) and started estrogen therapy in early 2023. Since every one of these interventions is off-label, I have been looking up the peer-reviewed literature on the effect of estrogen and whether there are any risks that our child needs to be aware of as they continue on this path. My findings, which I summarize below (and link to the sources), have been alarming. Several endocrinologists – some who publish extensively – have told me they were unaware of the new literature. I have also been in touch with the Endocrine Society, and their response heightened my alarm.
While we respect our child's identification with their gender identity, we felt that they exhibited several psychological symptoms right before identifying as a lesbian, transgender woman (Jonathan was assigned male at birth and did not show any inclinations to identify as female before April 2021), and these co-occurring symptoms were not considered at all before he started on the prescribed medicines. Most tellingly, just before identifying as transgender, Jonathan's romantic advances were rebuffed by the woman of their affection. Subsequently, Jonathan also lost every friend they had, thereby remaining completely alone in their dorm room for the greater part of their last two years of undergraduate education. However, these psychological symptoms were never explored. Jonathan was recommended to start on estradiol and spironolactone immediately, which they did – and their physical and mental health symptoms have deteriorated since. Jonathan is also quite depressed, spending all their time without emerging from their room.
That is not surprising since, when it comes to the recent research on estrogen in natal males, excess estrogen in the serum in natal males has been associated with depression – studies among adult men and adolescent boys show that. Clinical studies (i.e., studies that recruit actual subjects and follow them clinically rather than rely on anonymous, online, non-probability surveys) that promote gender medicine fail to show any improvement in psychosocial outcomes among natal males. For example, the New England Journal of Medicine study from early 2023 concluded that hormone therapy is psychologically beneficial for transgender youth. However, in the main text, the study finds no improvement in depression, anxiety symptoms, or life satisfaction among natal male youth (the relevant paragraph is at the bottom of page 244 of the journal issue).
Thus, psychologically, there is ample evidence that excess estrogen is associated with depression among natal males. Physiologically, recent research shows that estrogen might have far more deleterious effects. A study showed that 12 months of estrogen treatment among transgender women leads to a decrease in serum BDNF levels. That is significant because a separate study shows that this decrease in serum BDNF level is associated with increased risks of developing MDD (or major depressive disorder). Lower levels of brain BDNF levels have also been associated with neurodegenerative disorders and found in the brains of patients with Alzheimer's, Parkinson’s, MS, and Huntington’s disease.
A high-quality rodent study shows that estrogen therapy among adult male rats leads to changes in their brains that resemble the changes in the brains of trans women. (There have been several other studies (2 links) among trans women that have shown these changes, but the rodent study indicated the mechanism by which these changes occurred in the brain.) Specifically, estrogen seemingly reduced the water content in the astrocytes and thereby disturbed the delicate homeostasis in the brain by increasing the relative concentration of glutamate (the brain's most abundant excitatory neurotransmitter), leading to glutamate excitotoxicity. As the Cleveland Clinic informs us, an increase in glutamate in the brain is associated with higher risks of neurological disorders like Alzheimer's disease, ALS, and many other diseases like multiple sclerosis. The research also showed that estrogen decreased brain cortical thickness and volume (which other studies have linked to patients with schizophrenia and bipolar disorder and lower levels of general intelligence). Furthermore, it was found to reduce cortical white matter integrity (which is related to cognitive instability). There is also empirical evidence of the lowering of cognitive abilities among transgender women that was presented at the EPATH conference in April 2023 (in Killarney, Ireland) - the researchers noted this decline among long-term patients at Amsterdam's famed gender clinic.
Research in the last few years shows that estrogen therapy among trans women has been associated with higher risks of various autoimmune diseases, from multiple sclerosis (recall, too, the association of MS with an increase in glutamate) to rheumatoid arthritis and many others in between. It has been associated with increases in the risks of prostate cancer and breast cancer. It increases risks of cardiovascular diseases (2 links), often by as much as tenfold compared to their cisgender counterparts.
Empirically, we see a much higher incidence of many of these physical and neurological diseases in the transgender population. It is perhaps not a coincidence, therefore, that population cohort studies (2 links) show that trans women, on average, die decades earlier than either cisgender men or women.
When I approached the Endocrine Society with what I had found and pointed out that many of these findings came out after the publication of their guidelines in 2017, I received an email from their Director of Clinical Practice Guidelines that they are currently fast-tracking a revision of those guidelines. She also mentioned that their evidence evaluation criteria have changed since the guidelines were published and that they now use the GRADE criteria for evaluating evidence. This is encouraging, but I have no idea how long it will take for the new guidelines to appear.
I point all of this out because Jonathan has the chance to start afresh and be reevaluated at Apex University's healthcare system. We increasingly see them stumbling with their memory, something that we could not even think of a year earlier – Jonathan used to have a photographic memory ever since they were a child. Having heard so much about Apex's medical school, we have high hopes that Jonathan's evaluation at Apex University's medical system will be more thorough than it has been so far. Let me be clear: We have no doubt about their gender dysphoria or their intense discomfort in their traditional gender role – we worry about that all the time. It is just that we have observed that medicalization has not brought them any balm so far – in fact, just the opposite. While the absence of any upsides (and the possible significant downsides) in the literature – psychological or otherwise – heightens our alarm.
After all, it is not only a lone voice like ours, but even mainstream media like the Economist (their April 5 issue with the cover story “The evidence to support medicalized gender transitions in adolescents is worryingly weak” comes to mind) and storied institutions like the British Medical Association and the systematic reviews of the literature from national medical associations of very transgender-friendly countries like Sweden, Finland, Norway, the UK, and (most recently) Denmark that are raising the alarm on the lack of high-quality evidence of any benefits from hormone therapy. (And these reviews I mention above cover only the evidence of the psychological effects of the hormones – they do not even consider the long-term physiological consequences.)
If all the evidence from the past few years is to be believed, there is now quite a body of evidence of genuine harm from administering estrogen to the natal male body (I have not researched the effects of excess testosterone on the natal female body, and so I cannot comment on that.)
As one of the world's leading lights in healthcare to nudge society toward better outcomes through research, Apex University will be well placed to lead the march for evidence-based care in gender-affirming care.
Thank you very much for reviewing the evidence that I have found and considering our child's health as they start their journey at Apex University. Please let me know if you have any questions. I look forward to hearing back from you.
With warmest regards,
XXX
-
A few days later, I got their response. I have highlighted the relevant portions of their email and annotated them within brackets [all formatting mine]. As I said, it’s quite revealing.
-
Dear XXX:
Thank you very much for sharing your concerns about your child with us.
…Apex U's Student Health Center (Apex SHC) is not directly affiliated with Apex Medical School and we do not provide care under the umbrella of the hospital. [Is the respondent making sure that the medical school is not implicated if something goes wrong with our son?] However, we do collaborate closely with our colleagues at the hospital and medical school, including in the management of our student receiving gender affirming care.
…
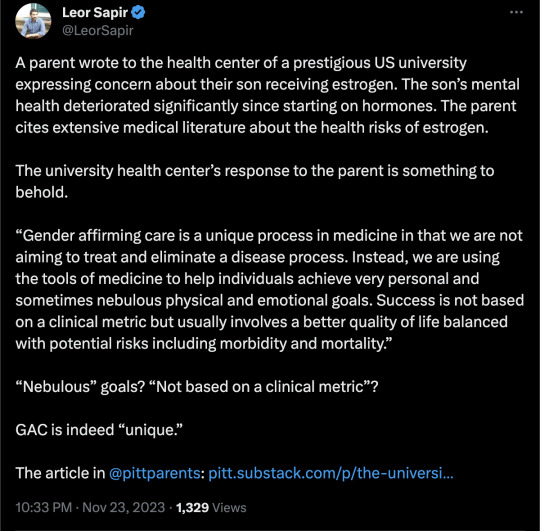
Gender affirming care is a unique process in medicine in that we are not aiming to treat and eliminate a disease process. [Ah, an admission that there is no real goal of treatment through this care. Finally! But read on…it gets better.] Instead, we are using the tools of medicine to help individuals achieve very personal and sometimes nebulous [nebulous? WTF? After all these years of "settled science," all we have is “nebulous?”] physical and emotional goals. Success is not based on a clinical metric but usually involves a better quality of life balanced with potential risks including morbidity and mortality. [So, finally, an explicit admission – success is not based on any clinical metric. That makes complete sense to us inconvenient parents. After all, how can there be? There never have been any metrics, ever. At. All. All we have are some "nebulous" ideas of "better quality of life" – as decided by the patient right now, with no consideration of what might happen in the future as a result of the free dispensation of off-label medication. And oh, by the way, that "better quality of life" includes morbidity factors and dying much faster.] We at the Apex SHC make every effort to ensure that our patients are well-informed [in other words, make sure that they have signed the informed consent forms!] about each decision that they make and have time to consider these impacts without pressure [The irony of the sentence – “have time to consider these impacts without pressure.” Wow! really?]
Should your child decide to engage with us in care, our commitment to them is to prioritize their safety [oh, the irony, once more!], the elements of their well-being that we can support [the rest – whether caring for them for the rest of their lives or paying for their illnesses and hospitalizations, with a big fuck you to your dwindling retirement funds – is up to you, you bigoted parents!], and to help them make a bright future for themselves.
Very best,
AAA
-
As I read and re-read the email, all I could think was – Wow! What an amazing letter! AAA has no qualms admitting that there are no clinical goals of treatment when it comes to gender-affirming care. This is really quite convenient if you think about it—if there are no aims, any outcome is fine! No wonder these physicians get all flustered when we inconvenient parents ask them about clinical goals and outcomes.
All that these caring physicians want to achieve are some nebulous (which the dictionary defines as unclear, vague, or indefinite) goals. Oh, and please remember – once again – that those are personal goals, so please don’t ask about evidence of well-being. (An inconvenient question, though – why should such personal goals be funded by others, whether it is the government or private insurance?)
And what if, as a result of those nebulous goals, the patients go through psychological, emotional, and physical distress for the rest of their lives, as detailed in the medical literature? Really, shame on you, you bigoted parents! Always such a nag! Always the party pooper. Why do you have to ask such inconvenient questions? Haven’t these caring physicians already made it clear that these are personal goals and that it really doesn’t matter that young children who are distressed might have no idea how to make a rational choice about the future? Who cares if they become hyper-fixated about something, as young children are wont to?
But then again, really, there is no pressure. No pressure at all. These kids are otherwise well-adjusted grown adults who know exactly who they are. Probably from the time they were toddlers. (What? You want evidence? This is getting really tiring. Give it a break, will you?) These are kids who are not immersed online, who do not gulp down narratives about “gender euphoria.” They are stable, rational human beings with a very clear idea of what the future holds.
All these well-meaning saints – these gender-affirming physicians – want is to give these kids a bright future: a future so bright that it will probably include that intense bright light these pitiable young men will see when they die decades earlier than their non-medicalized peers. Who are you parents to stand in their way?
==
This is quite a remarkable admission. If there are no metrics and the objectives are "nebulous," then that's the very definition of not-scientific, not-medical. How can this be "necessary," and even "life-saving" if it's also "nebulous"? God is both real and undetectable?
How can it be "settled science"?
You're letting people self-diagnose and self-prescribe in order to chase something nebulous? What the hell?
#Leor Sapir#gender affirming healthcare#gender affirming care#gender affirmation#clinical goals#clinical outcomes#queer theory#gender ideology#medical malpractice#medical scandal#religion is a mental illness
93 notes
·
View notes
Last Seen Blogs

emotional-empowerment
EmotionalEmpowerment

openairplaces
Open Air Places

unitedcab
United Cab 209-888-8888

thinggolf77-blog
Movies Choice

shafy5050
Shafy