#medicaid health plan
Text
Me: There are no dentists near me that take medicaid. I wonder if I can just get a dental plan.
The answer is apparently not because, when you then try to use medicaid to get a therapy appointment, your dental plan comes up as a third-party insurance.
#i can't afford either one separately#but i guess i gotta choose#because fuck me i guess#the lady i spoke to about the medicaid plan was very sweet#because even she was like wtf does dental have to do with behavioral health#but i am so fucking tired
2 notes
·
View notes
Text
CW: sexual violence and medical trauma
yknow, I wanted so badly to be able to entirely blame myself for bolting from the gyny yesterday. If it was just a problem with me, I can have total control of it.
but I dont think the way they handled it was ok. I had a crying panic attack about a vaginal exam and said "well it seems like I dont have a choice". They also knew I hadnt been to a gyny in 20 years. I barely looked at them. I hugged my body. It was really obvious I was very uncomfortable and scared and upset.
I think it would have helped a lot if they had done things to help me trust them - like say it was my choice, I could take breaks if I needed, and talked more about the procedure. Talked to me more about making me comfortable.
Also, I dont know that this procedure even WAS necessary when they were just "seeing for themselves" what the ER had already found.
Instead they just kinda said, we need to do this, and not much else- and then with two complete strangers staring at me, ordered me to undress from the waist down. Just like that, right there in front of them. They couldnt offer me a gown, to undress in private, or something? My last gyny was that long ago but I swear that's what she did then.
I panicked and bolted. And yes, I could have acted differently. Im not saying I dont have ANY responsibility or way to make the situation better. Im just saying, I think gynys ought to change how they deal with people who may be severely uncomfortable.
After talking to two female friends, BOTH of them mentioned feeling panic of the gyny. I bet this is really common, especially with young people.
When I was in the ER, and at Planned Parenthood, they did a lot more to make me comfortable and feel safe. I refused a pelvic at PP, and the lady did just kinda assume I was having a pelvic instead of asking, but they didnt push me to do it.
In the ER they presented it as my choice, they talked about taking breaks, they talked me through it, they offered breaks, they offered aftercare when I was crying and working on my breathing to prevent a panic attack. I felt safe, understood, and respected.
I was supposed to get my surgery from that hospital, where I had built trust, that week, and then insurance got declined. And that made me have to start all over. And this is hard.
It hurt to have to feel like I am not allowed access to a great care team because Im too poor, and being poor in part because of medical disabilities that include mental and physical chronic illness. What a sick joke. American healthcare.
I didnt even really go through any major sexual trauma, nothing that happened to me in terms of actual sex was even entirely non-consensual, just kinda not having my full consent fully respected the whole time and stuff like that. And stuff like getting groped at parties or whatever, frankly really normal stuff. I also do have some history of being mistreated by medical people in the past, mostly due to being queer and mentally ill. but nothing really major. I cant imagine what this would be like for someone who had survived something much more extreme. 
The last person I trusted with my body I knew for a year, and he scared me very badly (trigger warning for this, but - he expressed a fantasy of killing me, during sex, out of nowhere. /TW). So why should I trust a woman I JUST met?
I want to survive, I dont want to suffer, I dont wanna get more disabled, I dont wanna lose my job. I am worried and scared, sad, exhausted, ashamed, lots of big feelings, I need help and support, and it falls on me to do this. I have therapy in a few hours, and I will come up with a plan. but I would like to not be the only one who learns from my experience. I would like some doctor somewhere to hear my story some day and learn.
#medical#ob-gyn#Planned Parenthood#patient care#TW SA#PTSD#chronic illness#healthcare is a right#medicaid#TW medical trauma#mental health#mental illness#obstetrics and gynecology#gynecology#DV#IPV
2 notes
·
View notes
Text
I made $200 in tips last yesterday ❤️❤️ maybe I will be okay 😎
#this is a lie. I am not ok and I still don’t have health insurance and I suspect I may have diabetes cuz it runs in the family and I’m#showing symptoms. but I can’t afford to go to the doctor. and health insurance is expensive#and I keep getting denied for Medicaid#not to mention I’m due for another depo shot next month. thank god planned parenthood has the funding to let me pay what I can and they#cover the rest but fuck man it’s $130-160 per shot :/
2 notes
·
View notes
Text
sometimes my mom will to try to kick us off the phone plan or try to get us to pay for our own health insurance despite the fact that we're in school fulltime and some of us have literally no savings but I ALWAYS know when my dad swoops in to pay for it himself because she'll text us immediately after like "don't worry about it" whew dodged a bullet today
#it's because she wants to save money but is also planning multiple cruises 🙄#yeah I guess health insurance for your children with medical conditions and/or mental illnesses aren't as important#as you getting to play music with *squints* alan doyle on the rhine#anyway shoutout to my dad for not cutting us off#I'd probably be okay even so since I'm getting a job in a few months but my sister has literally no money and couldn't find a job#anyway. I don't have to change apply for or even worry about health insurance thank GOD#she REALLY wanted me to be paying for it though. ma'am its like 500 a month#I was in the process of applying for medicaid when she texted me but thanks goodness I did not want to deal with that#I could probably still get food stamps though#cor.txt
2 notes
·
View notes
Text
Yesterday at Work
New Boss: *mostly talking to me, but standing where My Boss could see and hear her* I'm going to have to leave at 4:30 for a while so I can pick up my son; sorry.
My Boss: You get to pick him up everyday. It's great!
New Boss: I don't know if- I might not be able to be in much tomorrow.
Me: Well, during the summer, I don't usually work on Fridays, so...
My Boss: Neither do I!
New Boss: *looking back and forth between us* Not working on Fridays? I could probably figure that out. *deep breath* Give me a few weeks. *small laugh* Or months.
Me: *grinning* I also take Wednesdays off most of the time. Even in Tax Season.
New Boss: *grinning back* I think I might really like it here.
#i love my job#i love my boss#my boss basically asked me if she could let her friend crash in the guest room while she got out of an abusive relationship#new boss acknowledges that she has a lot of professional trauma to figure out#i need to find that @copperbadge post about the trauma box#i'm leaving the legalities and final decisions up to the two of them#but it currently looks like new boss might actually become a fully named partner in the firm#i have also offered to give up my medicaid benefits if needed so we can get a group plan#it's complicated and i probably shouldn't be getting full benefits anymore but i am and because of my dad i know why and.....#and sometimes living with and being an editor/sounding board for a actual Expert on Universal Health Care means i know WAY than i should#WE'RE WORKING ON IT! okay?#it's not as easy as you want to make it#but more people are for it than you'd think#my dad's an Old White Male Republican (but mostly okay) and HE has been working for 15 years to make Universal Health Care happen#i could go on for days#maybe later i will#but i think it won't take long for me to love my new boss#her partner/baby daddy/if needed for legal reasons husband within 48 hours is basically my brother pat#we get each other so hard it's almost funny
6 notes
·
View notes
Text
.
#dont read this it’s just boring shit about my work lmao#was doing an assessment w a client today to get her updated in our system so she could get financial assistance#she used to be on my caseload when i had a caseload and i’ve been working w her for almost 3 years#she had sent a mortgage statement but we ran out of our mortgage assistance after a month and a half when it’s supposed to last us a year#so no mortgage assistance again until january#we were talking and the assessment is like personal questions about health and stuff and she started crying bc#she only has 7 of her antiretroviral left#and medicaid is telling her they’re gonna stop covering her bc her income is too high so she had cut back to working 2 days a week#and then couldn’t afford her bills#made me so sad 😭 i wish she had told me she was having issues we have a whole insurance department she’s never utilized#our org will pay her entire premium for a marketplace/employer plan#and she’s already enrolled in a program that will pay for her meds regardless of her insurance#mad me so sad she has been so deeply stressed about this i hope she lets me connect her to the insurance people bc they can fully solve her#made*#problem and she would be able to work full time again
0 notes
Text
Opinion Here’s how to get free Paxlovid as many times as you need it
When the public health emergency around covid-19 ended, vaccines and treatments became commercial products, meaning companies could charge for them as they do other pharmaceuticals. Paxlovid, the highly effective antiviral pill that can prevent covid from becoming severe, now has a list price of nearly $1,400 for a five-day treatment course.
Thanks to an innovative agreement between the Biden administration and the drug’s manufacturer, Pfizer, Americans can still access the medication free or at very low cost through a program called Paxcess. The problem is that too few people — including pharmacists — are aware of it.
I learned of Paxcess only after readers wrote that pharmacies were charging them hundreds of dollars — or even the full list price — to fill their Paxlovid prescription. This shouldn’t be happening. A representative from Pfizer, which runs the program, explained to me that patients on Medicare and Medicaid or who are uninsured should get free Paxlovid. They need to sign up by going to paxlovid.iassist.com or by calling 877-219-7225. “We wanted to make enrollment as easy and as quick as possible,” the representative said.
Indeed, the process is straightforward. I clicked through the web form myself, and there are only three sets of information required. Patients first enter their name, date of birth and address. They then input their prescriber’s name and address and select their insurance type.
All this should take less than five minutes and can be done at home or at the pharmacy. A physician or pharmacist can fill it out on behalf of the patient, too. Importantly, this form does not ask for medical history, proof of a positive coronavirus test, income verification, citizenship status or other potentially sensitive and time-consuming information.
But there is one key requirement people need to be aware of: Patients must have a prescription for Paxlovid to start the enrollment process. It is not possible to pre-enroll. (Though, in a sense, people on Medicare or Medicaid are already pre-enrolled.)
Once the questionnaire is complete, the website generates a voucher within seconds. People can print it or email it themselves, and then they can exchange it for a free course of Paxlovid at most pharmacies.
Pfizer’s representative tells me that more than 57,000 pharmacies are contracted to participate in this program, including major chain drugstores such as CVS and Walgreens and large retail chains such as Walmart, Kroger and Costco. For those unable to go in person, a mail-order option is available, too.
The program works a little differently for patients with commercial insurance. Some insurance plans already cover Paxlovid without a co-pay. Anyone who is told there will be a charge should sign up for Paxcess, which would further bring down their co-pay and might even cover the entire cost.
Several readers have attested that Paxcess’s process was fast and seamless. I was also glad to learn that there is basically no limit to the number of times someone could use it. A person who contracts the coronavirus three times in a year could access Paxlovid free or at low cost each time.
Unfortunately, readers informed me of one major glitch: Though the Paxcess voucher is honored when presented, some pharmacies are not offering the program proactively. As a result, many patients are still being charged high co-pays even if they could have gotten the medication at no cost.
This is incredibly frustrating. However, after interviewing multiple people involved in the process, including representatives of major pharmacy chains and Biden administration officials, I believe everyone is sincere in trying to make things right. As we saw in the early days of the coronavirus vaccine rollout, it’s hard to get a new program off the ground. Policies that look good on paper run into multiple barriers during implementation.
Those involved are actively identifying and addressing these problems. For instance, a Walgreens representative explained to me that in addition to educating pharmacists and pharmacy techs about the program, the company learned it also had to make system changes to account for a different workflow. Normally, when pharmacists process a prescription, they inform patients of the co-pay and dispense the medication. But with Paxlovid, the system needs to stop them if there is a co-pay, so they can prompt patients to sign up for Paxcess.
Here is where patients and consumers must take a proactive role. That might not feel fair; after all, if someone is ill, people expect that the system will work to help them. But that’s not our reality. While pharmacies work to fix their system glitches, patients need to be their own best advocates. That means signing up for Paxcess as soon as they receive a Paxlovid prescription and helping spread the word so that others can get the antiviral at little or no cost, too.
{source}
6K notes
·
View notes
Text
i dont wanna come off like im bragging but i make too much money now djdjsje im almost done paying off my car loan, I've been able to save up a lot, and i am able to get takeout regularly and buy cool shit. i bought a projector yesterday!
ive always been on the other end of stuff so this is weird. especially after dropping 10k on my cats surgery and not really having to stress much about it. if that happened a year ago id be fucked and he would quite possibly be dead.
ive been trying to give back when i can so i always tip really well and ive been contributing to donation posts and i sometimes buy my partner's groceries lol. disclaimer guys im a good person
im putting a hold on trying to move out bc theres a housing crisis and im sure fucking tired of paying an application fee only to not hear back from them what the fuck. and i happen to not be in a rush. so i don't have many bills. and i have pretty much everything i need so i dont really have much to buy. i wish i at least wanted more but i wouldnt have anywhere to put it in my tiny room lol
literally feel like a fucking dragon or elon musk maybe
#never not been poor and i did nothing for it#the only thing is i dont qualify for medicaid anymore and starbucks health insurance plans are fucking dumb
1 note
·
View note
Text
Steps to Creating an Estate Plan
In the eyes of the law, your estate is defined as all of your belongings and accounts, including credits and debts, that are left behind after you die. Upon your passing, the executor of your estate will need to process your will to ensure that your estate is settled. This means transferring assets and accounts to the entities you’ve chosen and paying debts and collecting credits as needed.
Before your passing, you can engage in estate planning to help those left behind. Estate planning is the process of laying out how you want your assets and accounts to be distributed after death. The goal of estate planning is to make the execution of your will easy and efficient so that you can rest assured that your wishes will be carried out.
Below are the steps needed to create an estate plan:
1. Take an Inventory
The first step in estate planning is to take an inventory of all your assets and accounts. These can include real properties, bank accounts and investments.
2. Decide How You Wish to Distribute Assets
You can then decide how you wish to have your assets and accounts distributed after you pass. You will need to create official documentation for your wishes to be recognized by the legal system in your state. You may also want to establish trusts for certain assets since trusts can provide unique advantages when it comes to transferring ownership of assets.
3. Work With an Attorney
Although you can draft estate planning documents yourself, most legal experts agree that it’s best to work with a local estate planning attorney instead. The reason you want to look for a local attorney is that laws regarding estate settlement differ from state to state.
If, for example, you live in Albany, you would want to look at a New York estate planning law firm for guidance. A New York estate planning law firm will be able to help you navigate the laws about estates and wills in New York, whereas an attorney in another state may not be able to provide the same level of service.
Read a similar article about New York City estate administration attorney here at this page.
0 notes
Text
Medicare Advantage plans are often advertised as being a "better" option than traditional Medicare. However, there are a number of ways in which these plans can be misleading. One way is that they often tout their low premiums, but they don't always mention that these premiums may increase over time. Additionally, these plans may have higher copays and deductibles than traditional Medicare. Another way that Medicare Advantage plans can be misleading is that they may not cover all of the same benefits as traditional Medicare. For example, some plans may not cover prescription drugs or vision care. Finally, Medicare Advantage plans may also be misleading about their network of doctors. Some plans have very limited networks of doctors, which can make it difficult for patients to find a doctor who is in their plan. It's important to do your research before enrolling in a Medicare Advantage plan. Make sure you understand all of the terms and conditions of the plan, and that it will meet your needs. If you're not sure whether a Medicare Advantage plan is right for you, you can always talk to a licensed insurance agent.
Your physician's fees are just one part of the overall cost of healthcare. However, your physician can play a role in helping you to control your healthcare costs. By following your physician's advice and taking care of your health, you can reduce your risk of developing costly health problems. You can also talk to your physician about ways to reduce your healthcare costs. For example, your physician may be able to help you to get a prescription for a generic drug instead of a brand-name drug. Your physician may also be able to help you to find a hospital or clinic that offers lower prices for services. It is important to remember that your physician is there to help you. Physicians have no say when it comes to the cost of a medication. They prescribe medications that have clinically proven to help patients that are experiencing similar symptoms or have the same disease. At the end of the day, your health insurance decides what they will and will not cover, how much they will pay leaving the remaining coinsurance for the patient to pay. They also create barriers to avoid having to pay for high cost treatments. Here are some of the ways health insurance is creating barriers for physicians to treat their patients:
Low reimbursement rates: Health insurance companies reimburse physicians at rates that are often below the cost of providing care. This can make it difficult for physicians to make a living, and can force them to reduce the number of patients they see or the services they provide.
Burdensome paperwork: Health insurance companies require physicians to fill out a lot of paperwork, which can be time-consuming and take away from the time they spend with patients.
Administrative complexity: Health insurance companies have complex rules and regulations that can be difficult for physicians to understand. This can lead to errors and delays in the processing of claims.
Preauthorization requirements: Some health insurance plans require physicians to obtain preauthorization before providing certain services. This can delay care and make it difficult for patients to get the care they need when they need it.
Network restrictions: Some health insurance plans only allow patients to see physicians who are in their network. This can limit patients' choices of physicians and make it difficult for them to get the care they need.
These barriers can make it difficult for physicians to provide quality care to their patients. They can also make it difficult for patients to access the care they need.
There are many factors that contribute to the high cost of prescription drugs, including:
The high cost of research and development
The high cost of manufacturing
The high cost of marketing
The high cost of insurance
The high cost of government regulation
Your doctor is not responsible for any of these factors. They are simply trying to provide you with the best possible care. Meanwhile, insurance companies' profits are increasing and patients are paying more for their insurance coverage but often realize they are paying more money for less coverage. They are able to do this:
Raising premiums. Insurance companies have been raising premiums for years, and this trend is likely to continue. This means that patients are paying more for their health insurance, even though the quality of their coverage is not always improving.
Reducing benefits. Insurance companies are also reducing the benefits that they cover. This means that patients are paying more for their health insurance, but they are getting less coverage in return.
Increased deductibles and copays. Insurance companies are also increasing the deductibles and copays that patients have to pay. This means that patients are paying more out of pocket for their health care, even though they are paying more for their health insurance.
Denying claims. Insurance companies are also denying more claims than ever before. This means that patients are paying for their health insurance, but they are not getting the care that they need when they need it.
Using loopholes to avoid paying out on claims. Insurance companies are also using loopholes in their contracts to avoid paying out on claims. This means that patients are paying for their health insurance, but they are not getting the benefits that they are paying for.
It is important to be aware of these practices so that you can make informed decisions about your health insurance. The Medicare Advantage program is a federal program, but it is administered by private insurance companies. These companies are not subject to the same regulations as traditional health insurance companies, and they are not required to disclose the same information about their plans. Medicare Advantage companies often advertise their plans with catchy slogans and promises of low premiums and comprehensive coverage. However, they often do not explain the difference between their plans and traditional Medicare. This can be confusing for consumers, who may not understand the implications of the different plans.
#Accountable Care#ACO#CAPG#Health Policy#healthcare reform#Medicare Advantage#Value Based Healthcare#ACA#Affordable Care Act#Capitation#obamacare#Patient Protection and Affordable Care Act#Triple Aim#wellness#managed care#Medicaid#Medicare#Medicare Advantage Plan#Medicare Plan#Medicare Ratings#Medicare Stars#medicaredisadvantage#regulatemedicareadvantage#profitovercare
0 notes
Text
What is Limited Medical Insurance?
A limited medical plan is a form of supplemental health insurance that can be used with or without a major medical plan. Limited medical plans have a set amount of money for treatment that they give to you to pay for common medical expenses. They recognize that common services like wellness visits can sometimes turn into a financial strain for people. Since this type of insurance does not cover…

View On WordPress
#getcoveredNJ#healthinsurance#healthinsurancebroker#healthinsuranceinPA#healthinsurancenearby#HealthInsuranceNearMe#healthinsuranceNJ#limitedmedical#medical medicare medicalplans Medicaid healplans totalbenefitsolutions employee benefits healthinsurance#minimumessential#OBAMACARE#pennie#smallgrouphealthinsurance#TotalBenefits#marketplace health plans obamacare#The Marketplace
0 notes
Text
Hi, local long-time tumblr resident here. Please take a moment to spread this message if you can.
In South Carolina, my home state, bill H. 4624 is swiftly being approved and passed through legislation with virtually no media coverage or conversation happening around it.
It is a dangerous and aggressively transphobic bill that will outlaw treatment for any trans person under 18, would require school teachers, counselors, and medical practictioners to disclose a student's status as trans to parents (which can lead to abuse or worse) and will also make it illegal to use any public funds to cover transition-related medical services for anyone of ANY age.
For transgender adults on medicaid or the state health plan, this is absolutely terrifying.
For anyone in SC who believes trans people should be allowed to live dignified and peaceful lives, I urge you to read up on the bill and to send emails to the governor and (if they are on the medical affairs committee) your local senator.
Links below.
Bill H. 4624
An explanation of the bill
Find your local senator
Message the Governor
2K notes
·
View notes
Text
I feel like people often don’t talk about the experiences of disabled people who have caretakers because so much of the conversation is about us—not including us.
I receive in home care for 30 hours a week (+ 4 hours/week for respite). This is paid for by Medicaid (state insurance). Outside of paid hours, my primary caretakers care for me unpaid and assist me most of the time. I’m very rarely left alone due to my high support needs. Often, when I am left alone, I am completely bedridden or at minimum housebound. I have frequent emergency life threatening health problems, falls, and serious injuries even with support in place, and these things significantly increase when I’m on my own.
I’m extremely lucky that my paid caretakers are my partner, my sister (the only family member I have regular contact with, I’m estranged from the rest of my immediate family and most of my extended family) and my best friend.
I used to have agency staffing which was horrible for me and borderline traumatic. At several points, before doing the self directed care option (which allows me to choose my own staff, hire and train them myself and dictate hours for them), I opted to not have any staffing. I was regularly in the emergency room. I can’t drive, so I was having to walk and if I was lucky enough to be able to take the bus on occasion or get a ride from a Facebook acquaintance, they were few and far in between. I don’t have family support, and even my sister who is supportive wasn’t living in the state at the time and doesn’t have a car most of the time.
And before I could even choose which staffing option, even though medically it had been deemed essential for me to have in home care, even though my insurance covered it, I had to wait several years (I was 18 when I was approved) until I was 21 to qualify to start. The reason why: I was legally an “adult disabled child” because of my high support needs (which is funny because I STILL don’t have SSI at age 24) and thus legally unable to consent to my own care plan. I needed a blood relative to consent, and that same blood relative (who had to have proof of such!) couldn’t care for me. At the time, my sister was the only person who could’ve been my caregiver and also she is the only verifiable blood relative I have contact with for safety reasons, and my only relative on this side of the USA.
The first business day after my 21st birthday I immediately got things set up to get in home care.
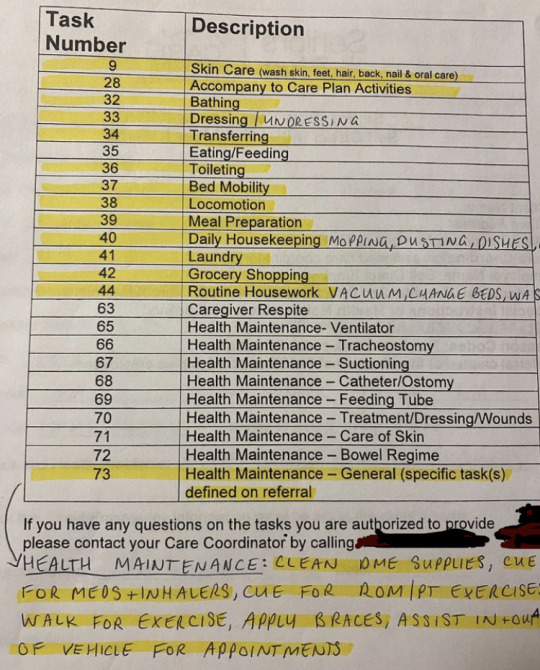
This is out of date, I get assistance with more than just these highlighted ADL (activities of daily living) tasks now.
In short: my day-to-day life is entirely dependent on others.
And there’s power imbalances that exist between me and my caregivers, even with my current caregivers being amazing and anti-ableist. They will always exist. We talk about the power dynamics of me being dependent on them for my survival, and how heavy that weight can be for each of us.
Having caregivers often means that accessibility is extra difficult— I’ve been told straight up multiple times that I can’t have assistance from my caregivers to help me change in a changing room when we’re out shopping. That they can’t go into the bathroom with me, that they can’t help me get un/dressed during appointments, that they can’t come into spaces with me.
I’ve been denied access to psychiatric care because I can’t do my daily living tasks (ADLs- the highlighted items) independently. And when I’m in a hospital or emergency room, I can’t have my in home workers be paid to care for me, there’s an expectation that the nursing staff at the hospital will do it. Even though my caregivers were specifically trained to learn my body and needs for weeks and have been working with me for years. I have severe cPTSD and showering in front of a stranger is something I cannot do. I would rather fall or faint or get injured or just not shower than deal with that. But I’m expected to just let anyone have access to my body just because I’m physically disabled and need support.
When I faint/fall/get injured/have life threatening health issues arise while I’m not clothed, or when I’m otherwise vulnerable, I’m supposed to let strangers just touch me however they want to. I have to show them my chest (for my cardiac care) and let them poke and examine me. I can’t object without losing access to vital care.
I have agency. I have rights. I have autonomy. I deserve to be able to exercise these things.
#chronically couchbound#disability#disabled#disabled pride#cripple punk#cripplepunk#disability pride#high support needs#ableism#professional caregiver#activities of daily living#ADL#medicaid#healthcare#in home care#home care#home care aids#nothing about us without us
1K notes
·
View notes
Text
'Free' screening? Know your rights to get free care
‘Free’ screening? Know your rights to get free care
By Julie Appleby, Kaiser Health News
Wednesday, July 6, 2022 (Kaiser News) — An ounce of prevention… well, you know the rest. In medicine, prevention focuses on detecting problems before they worsen, affecting both a patient’s health and finances.
One of the more popular parts of the Affordable Care Act, which allows patients to undergo certain tests or treatments without spending cash to cover…

View On WordPress
#Cost and quality#Healthcare costs#Insurance#Medicaid#Medicare#medicines#Obamacare Plans#Preventive services#the health law#vaccines
0 notes
Text
Feminizing HRT Overview, Guide & Information for All People Seeking It
we also have a version of this post for testosterone/masculinizing HRT as well. we wanted to write a companion piece as many folks have asked about this. it has take a bit of time, but here we are!
The testosterone HRT post is here.
Getting Your Prescription
To start taking estrogen, you will need to find a general practitioner, family doctor, endocrinologist or informed consent clinic where you can discuss gender affirming care with knowledgeable staff. Planned Parenthood is a good option for many trans people in general. Your mental health may also be evaluated, and your heart health and screening for a few other health conditions, as well as having access to your family health history if possible will be required.
Check to see if you have medical insurance, either through your family, your job, or if you are low income, a program like medicaid. Search for low income insurance plans in your area if it is needed, many places offer insurance plans for those who can't afford care on their own.
Here is a map of informed consent HRT clinics in the US.
You will discuss any gender dysphoria, gender presentation needs, if you have a support network, how you are impacted by your gender in your every day life with your provider and so on before being given a prescription. You will only be given a prescription after you discuss the risks of HRT and are screened for possible health problems and diseases or ways your body could react negatively to HRT. If you have needle trauma or phobias and can't inject hormones, it's best to bring it up before you get your prescription to save time and confusion.
The Medications
Treatment typically starts with spironolactone (aldactone), an anti-androgen that blocks androgen receptors ("male" sex hormones) for a few weeks, and then add estrogen, but many folks start with spiro and estrogen at the same time. Spiro will lower the amount of testosterone your body makes. For some people, spiro isn't necessary at all!
Some forms of spironolactone are reported to make folks pee like crazy, others do not have as bad of a time with it. Your mileage will vary depending on manufacturer. Spironolactone is intended to be a blood pressure medication, meaning it is a diuretic and is intended to help your body flush out fluids + salt. You will need to keep yourself hydrated if you notice this effect, as well as increasing electrolyte intake where possible.
Estrogen also lowers how much testosterone your body makes, and triggers changes in the body that occur during puberty in afab & adjacent people. Estrogen can be taken several ways, and is usually taken daily, and several times a day. You can take it in a pill or shot, and several forms of estrogen that can be applied to the skin like creams, gels and patches.
Make sure you thoroughly sanitize the skin of any injection sites or areas you will be applying gel or patches. If you are given topical estrogen, make sure you wash your hands after application and do not have someone else apply it for you. Make sure you do not go swimming or shower within several hours of application to make sure your skin absorbs the hormone.
You may not need to take anti androgens if you are doing estrogen injections, depending on how effective the estrogen injections are for you. Some people may not end up needing anti-androgens at all, and may be able to skip that entirely as spiro has unwanted side effects. Your natural hormone levels will dictate whether or not it's necessary, but it is not necessary for everyone.
You may end up being recommended to switch from one form of estrogen to another as your transition progresses, depending on how your body responds.
It's recommended to not take estrogen as a pill if you have personal/family history of blood clots in a deep vein or in lungs (venous thrombosis).
Some people also end up taking progesterone as well alongside estrogen. Progesterone is typically taken to encourage breast tissue growth, as this is the most prominent effect of the hormone. If sufficient breast tissue growth isn't seen from estrogen alone, progesterone can be added to your regimen, though this is only done later on into treatment, around a year or so in.
If you choose injectable estrogen, make sure to listen to your provider and ask for instructions about how to use needles and syringes, as well as injection angles, how and where you'll be injecting. Do not inject in the exact same spot every time, this can prevent the issue from healing properly and create scar tissue or cause infections or skin tissue necrosis (death). You also need a sharps container to safely dispose of your needle tips. Never re-use a needle, even if it was used previously on yourself. Always ask the pharmacy if you need more needles. A lot of places let you get them in bulk.
If you are going the injection route, make sure you know whether or not you are instructed to do intramuscular or subcutaneous injections. Intramuscular injections usually taper out of the system more quickly and need to be done more frequently, where as many patients find subcutaneous injections less painful and easier as they can be done less frequently.
For more information on safe intramuscular or subcutaneous injection for estrogen, please read here.
Another option for feminizing HRT is to take gonadotropin-releasing hormone (Gn-RH) analogs. They lower the amount of testosterone your body makes and may allow you to take lower doses of estrogen without using Spiro. Gn-RH analogs are usually more expensive, but are an option if for whatever reason the conventional route can't work for you.
DON'T GIVE UP IF YOU DON'T SEE THE EFFECTS YOU WANT TO SEE RIGHT AWAY! Many of them can take a long time to develop, often times patience is the key. If you wait it out and still don't see the results you'd like, you can try another route. Don't give up, a lot of people get deterred in the early stage of transition, you'll get there with patience and communication.
Stay patient, stay positive!
What to Expect from Feminizing HRT
Less facial and body hair growth: typically happens 6 - 12 months after treatment starts. Full effects within ~3 years on average.
Slower scalp hair loss: begins 1 - 3 moths after treatment begins. Full effect between 1 - 2 years on average.
Softer, less oily skin, and changes in general skin texture: 3 - 6 months after treatment starts, full effects within 2 - 3 years on average
Rounder, softer features including face and body, and more body fat: 3 - 6 months after treatment starts, full effects in 2 - 5 years.
Breast development: begins 3 - 6 months after treatment starts, full effects within 2 - 5 years on average or more, according to medical studies, but it can vary wildly from person to person, give dosage and hormones taken. If desired effects are not seen, progesterone can be taken alongside estrogen to help after around one year on estrogen. When breast growth begins, it starts with hard lumps under the nipples along with some soreness and itchiness. Some have sore breasts for a long time, and some may get scared and think they have cancer during this stage. Breasts will be swollen and tender for good while, and nipples may be especially sensitive to even light touch.
Reduced muscle mass/density: 3 - 6 months after treatment starts, full effect in 1 - 2 years on average
Potential decrease in libido if on estrogen alone, though not guaranteed: If it happens, it's generally within 1 - 3 months in and can last a while, but may even out over time
Fewer erections, decreased ejaculate volume, and erections that can become painful or uncomfortable if frequent erections are not maintained. This begins 1 - 3 months after treatment starts, and the full effect is within 3 - 6 months. Regularly maintaining erections and frequent ejaculation can ease some of these uncomfortable feelings in some people.
Changes in how orgasms feel, changes in texture and degree of sensation of penis and scrotum skin as well as changes in body odor: typically begins within 3 - 6 months, though it varies from person to person. Often times the way one's body responds to orgasms completely changes, many people find themselves experiencing full-body orgasms and more intense erogenous zones elsewhere in the body other than the genitals.
Smaller testicles, or testicular atrophy happens within 3 - 6 months and the full effects are usually seen within 2 - 3 years.
Increase in size of bladder and decrease in size of prostate over time which can lead to making one's gspot harder to find, and make prostate examinations more difficult, though they are still vital, as prostate cancer is still a possible factor.
Potential mood fluctuations while adjusting to the hormones, many report increased crying and sadness during the first 3 - 6 months with this tapering off after a full year at most.
Increased fatigue while adjusting to the hormones, sleepiness and becoming easily exhausted are common reports. This can vary drastically from person to person, ymmv.
If you have testicles and choose to have them removed, you may need to take testosterone as well as estrogen in order to have a healthy endocrine system. You will need to discuss the effects of this with your specialists if you want to go this route. If your androgen levels get too low because your body cannot synthesize enough testosterone after bottom surgery, you may need additional medication.
Potential infertility, though this is not a guarantee, and safe sex should still be practiced at all times. No timeline projected though the longer one is on E the more likely it becomes.
Monthly cycles akin to menstrual cycles: these are not present in everyone, but many people report entering a cycle of extreme fatigue, body aches, abdominal cramping in the approximate area where a uterus would sit, headaches, and more for around the duration of a menstrual cycle (4 - 10 days on average).
Progesterone inversely to estrogen can cause an increase in libido in most who take it, and is the primary hormone used for breast growth. Lactation may also occur while taking prog, if this happens, talk to your doctor right away.
Keep track of your progress when and where you are able, and don't be afraid to bring up any concerns you may have with your professionals or trans friends, or any other trans resource. Your transition is in your hands and you're allowed to modify it as you see fit. If you do not see the effects you want from traditional HRT, you may be able to seek the Gn-RH route, and if you aren't seeing the results you want from just estrogen, progesterone might be of use to you.
You will need to keep an eye on your bone health as high levels of estrogens can increase your chance to develop osteoporosis, and potential new cancers like breast cancer may arise, as well as heart problems. Getting checkups as frequently as possible and communicating with your doctor/s will be of great use when and where possible
Either way, we hope this helps in some way! We will add to it as we find/think of more information. Good luck to everyone seeking feminizing HRT, you deserve to look and feel like yourselves!
#transfem#transfeminine#transgender#trans#lgbt#lgbtq#queer#transfemme#trans girl#trans woman#trans women#trans lady#trans girls#trans gal#nonbinary#enby#genderqueer#genderfluid#drag queen#estrogen#progesterone#spironolactone#feminizing hrt#hrt#hormone replacement therapy#estrogen hrt#e hrt#e#our writing#resources
1K notes
·
View notes
Text
F—k Tex-ass Republicans!
🖕
#republican assholes#Tex-ass Republicans#fuck Greg Abbott#fuck Ted Cruz#traitor trump#Texas republicans are the worst#Medicaid#maga morons#republican values#republican family values#republicans hate poor children
163 notes
·
View notes
Last Seen Blogs

daliacrossing
daliacrossing

brufhruf
Untitled

sxrrymum
Finders Keepers, Losers Weepers

1dbmhs
unicorns
