#negative acute phase proteins
Text

#dietetics#positive acute phase proteins#negative acute phase proteins#acute phase proteins#ferritin#transferrin#haptoglobin#CRP#C reactive protein#albumin#prealbumin
1 note
·
View note
Text
Just a "mild" neuron infection you got from brunch with the girlies :)
Highlights
"Our study shows that the increase in serum biomarkers of neuronal and glial damage, sNfL and sGFAP, was present one week after resolution of asymptomatic SARS-CoV-2 infection or mild COVID-19 and was more pronounced in patients with cognitive impairment. Furthermore, 10 months after resolution of the infection, levels of these biomarkers were still significantly higher than in healthy controls, although reduced from those observed at baseline. At the same time, self-reported cognitive impairment appeared to worsen in the same subjects, suggesting that early neuronal and glial damage may have resolved by 10 months post-infection, although subjective cognitive impairment may persist or become more pronounced."
"The second relevant finding of our study is represented by the higher sNfL and sGFAP levels in the eleven COVID-19 patients complaining of cognitive failures at T0. Cognitive deficits are common after COVID-19 and can impair executive functions, attention, and episodic memory. Studies on the neuropsychological alterations during acute COVID-19 and in the post-COVID-19 phase show inhomogeneous results, particularly for the variable time of the evaluation, ranging from two to five weeks after the onset, up to one year after the recovery. Most of these studies, however, mainly focus on hospitalized patients, being non-hospitalised patients somehow overlooked."
"A recent study showed that more than one-third of hospitalized and non-hospitalized patients after COVID-19 experienced a perceived cognitive deficit after 30 days after hospitalization or outpatient infection. It should be noticed that, differently from our population, this patient cohort included mainly hospitalized patients with remarkable comorbidities. Our study shows cognitive failure immediately following the recovery in a not negligible percentage (7.5%) of COVID-19 patients, suggesting a clinical impact of SARS-CoV-2 even in individuals with the mildest forms of the disease."
"The previous literature on mild or non-severe COVID-19 cases clearly indicates their significant impact on cognitive function, particularly in domains such as working memory and processing speed, with a good potential for recovery over time though some impairments may persist. Cognitive failures, therefore, may interfere with highly complex working activities, particularly those that require attending to and remembering large amounts of information, like academic or administrative jobs."
"Our patients with CFQ scores higher than 43 could experience high difficulties when returning to their work. The negative impact on daily functioning and quality of life of post-COVID cognitive dysfunction has been highlighted by Quan et al. emphasizing the economic, health, and social burden associated with. In fact, Beck and Flow demonstrate that individuals who had contracted SARS-CoV-2 infection reported cognitive failures at work and difficulty performing their tasks, highly detrimental to their performance, and may leave a job looking for other sources of employment."
"This evidence provides support for the need to perform careful neuropsychological evaluations for all the workers following SARS-CoV-2 infection, to allow both an adequate resumption of work activities and to monitor the onset of any cognitive impairment even in workers with a previous mild COVID-19 or asymptomatic infection."
#mask up#covid#covid 19#covid isn't over#pandemic#covid conscious#long covid#covid is airborne#wear a mask#coronavirus
13 notes
·
View notes
Text
Cirrhosis causes increased INR because the liver makes clotting factors 2, 7, 9, and 10. If the liver is cirrhotic, you can’t make those clotting factors. Risk of bleeding.
So you monitor the INR. Also monitor albumin. The liver lakes albumin, so if it's cirrhotic, albumin is low.
The liver detoxifies things. If the liver doesn't work, you get build up of ammonia-> hepatic encephalopathy. Ammonium builds up in brain-> asterixis (flapping tremor).
Hepatic encephalopathy is diagnosed clinically with confusion and asterixis. Tx: lactulose (eliminates nitrogen through the gut). Rifaximin and zinc can also be used to eliminate excess nitrogen.
The liver metabolizes estrogen. Without liver function, estrogen builds up-> gynecomastia, palmar erythema, spider angiomata.
Portal hypertension-> thrombocytopenia, ascites, varices (porto-caval shunts). Caput medusa, hemorrhoids, esophageal varices result.
Do EGD to evaluate for varices. Tx of bleeding varices is banding and beta blockers (nadolol or propranolol). In the pts we have, octreotide is given for bleeding. Propranolol is to prevent bleeding when the pt is no longer bleeding. Must be a non-selective beta blocker.
If pt has bleeding varices, give octreotide and ceftriaxone. Octreotide reduces portal pressures acutely. If that doesn't work and pt is bleeding, TIPS can be done. TIPS bypasses the liver; connects portal vein to hepatic vein. It saves the pt from bleeding but also increases ammonia because now blood isn't going through the liver, which detoxifies the blood, increasing risk of hepatic encephalopathy.
Serum Ascites Albumin Gradient (SAAG) helps you determine the cause of the ascites. It tells you whether the ascites is due to portal HTN or not. Get paracentesis and determine the difference between the pt's serum albumin and the ascitic fluid albumin. A score greater than 1.1 means the ascites is due to portal HTN. It means there's mostly fluid in the abdomen. A SAAG less than 1.1 means there are cells in the ascitic fluid, so ascites is due to something like TB or cancer.
Ascites presentation: bulging flanks, shifting dullness, fluid wave.
Tx ascites with furosemide and spironolactone; restrict sodium and water intake, therapeutic paracentesis.
SBP = streptococcus and/or gram negative rods. Dx SBP with paracentesis showing polymorphonuclear cells greater than 250. If greater than 250 neutrophils, tx with IV ceftriaxone. If total protein of ascitic fluid is less than 1, give fluoroquinolone for SBP prophylaxis.
Secondary bacterial peritonitis occurs if the ascitic fluid culture shows lots of different bugs, meaning there's a bowel perforation and pt will require exploratory surgery.
Don't wait for the culture to return--if neutrophils are greater than 250, treat SBP with antibiotics. Even if the culture comes back negative, keep treating SBP.
Chronic liver inflammation (cirrhosis or hep B)-> hepatocellular carcinoma. Screen for hepatocellular carcinoma with RUQ US and AFP. Confirm the diagnosis with a triple phase CT (this is the one cancer you don't need a biopsy to diagnose). During the arterial phase of the triple phase CT, cancer lights up.
Hepatocellular carcinoma that's small is treated with resection. If it's big, pt needs liver transplant, if it's really big or multiple sites in liver are affected, tx with radio-frequency ablation or chemo embolization.
2 notes
·
View notes
Text
C-Reactive Protein in Veterinary Practice
Abstract
Animal body reacts to all kinds of injuries and stress to keep up the homeostasis mechanism of the body. This homeostasis achieved either by or nonspecific mechanism. The nonspecific innate resistance of the body like cytological and cytokine reactions including fever, leukocytosis etc. is known as acute phase response. In this response, there will be increase or decrease of serum concentration of proteins. These proteins are known as acute phase proteins. Measurements of serum concentration of these acute phase proteins are found to be useful in assessment of health status and prediction of diseases of the man and animals. The serum concentration of these acute phase proteins returns to base levels when the triggering factor is no longer present. The acute phase response is now considered to be a dynamic process involving systemic and metabolic changes providing an early nonspecific defence mechanism against insult before specific immunity is achieved. Use of one of the acute phase proteins, C-reactive protein as biomarkers for animal disease diagnosis and health status assessment has got high potential in modern veterinary practice is discussed in this review
Keywords: Acute injury; C - reactive protein; Acute phase proteins; Veterinary practice
Abbrevations: CRP: C Reactive Protein; Hp: Haptoglobin; AGP: Acid Glycoprotein; SAA: Serum Amyloid A
Introduction
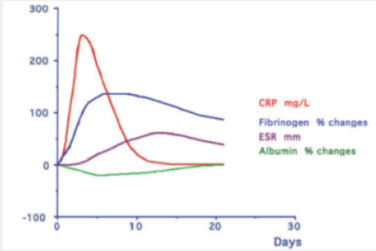
The acute phase reaction encompasses all the phenomena which take place in animals following tissue damage and is particularly associated with inflammation from whatever cause. During the acute phase reaction, the body mounts a multifactorial response to remove and replace damaged tissue and one of the mechanisms involved is the production and secretion by the liver of a number of ‘acute phase proteins’ [1]. The concentrations of these proteins increase during the reaction are called as Positive acute phase proteins (APPs) such as C reactive protein (CRP), Serum Amyloid A (SAA), Haptoglobin (Hp), Ceruloplasmin, α2- Macroglobulin, α1 Acid Glycoprotein(AGP), Fibrinogen and Complement (C3,C4) while those of others, including albumin, Transferrin, Transthyretin and Retinol-binding protein decrease as the liver switches production of protein towards the synthesis of the proteins required to deal with the damage; is called as negative APPs [2] (Figure 1).
Biological functions of C-reactive Protein
The protein was named the C-reactive protein because of its ability to bind pneumococcal C-polysaccharide. The presence of CRP has also been described in human patients during acute infections caused by acute lobar pneumonia, active rheumatic fever and bacteraemia caused by “colon bacillus”. Among the biological functions described in the literature are Complement activation and opsonisation [3,4] Modulation of monocytes and macrophages, cytokine production [5] Binding of chromatin [6] Prevention of tissue migration of neutrophils
CRP in Bovines
During the early stages of infection, the serum concentration of CRP increases [3]. This increase has been described to be evident before an elevated rectal temperature is observed. Even though increased concentrations of bovine CRP during naturally occurring infections and a correlation with herd health status have been reported, CRP is generally not considered an acute phase protein in cattle. As stress increases to a critical point, the liver rapidly synthesizes large amounts of CRP and releases it into the blood to provide immediate protection against stress [7]. Diseases in a dairy herd elevated the serum CRP level. The serum CRP level was also correlated with milk production. The greater the milk production, the higher the level of serum CRP. Diseases, especially acute infections, induced much higher levels of CRP production than stress or lactation. Also showing that plasma C-reactive protein concentration is related to different kind of stress (poor health, high lactation, blood collection). Strong correlation was observed in cows after delivery (0-1 month) between fibrinogen and CRP values [8]. Obtained results suggest that not only inflammations but also physiological factors such as pregnancy, delivery and/or state of lactation may have a significant impact on APPs values in the blood plasma of dairy cows. It would be worth in the future to check whether there is a relationship assessing the animal health status obtained using acute phase proteins method relatively to other indicators, such as milk yield, length of lactation or others. Morimatsu [9] also discovered Elevation of bovine serum C-reactive protein by lactation when compared to other Acute Phase protein such as serum amyloid P component levels (Figure 2).
CRP in Swine
In the pigs, as in the dogs and humans, C-reactive protein (CRP) is the prototypical acute phase protein with major diagnostic value. CRP concentrations are useful for evaluating the health status of a swine herd, but not for the health status of an individual animal or the differentiation of diseases. Serum haptoglobin (HP) concentration is better than serum CRP concentration as an indicator of inflammatory reactions in pigs, and HP is an important marker for swine health status [10]. On the other side, pigs undergone experimental study had CRP serum concentration below 22μg/ml (mean 18.64 ± 2.59). Twenty-four hour after coinfection with swine influenza virus (H1N1) and Pasteurella multocida, the mean concentration of CRP reached 62.85 ± 35.55μg/ml. Significant difference were noticed as compared to control animals [11]. The presence of elevated serum Hp and CRP concentrations in apparently healthy pigs at slaughter could provide important information to a veterinary inspector about the presence of sub-clinical lesions that could lead to condemnations or a decrease in the quality of carcasses [12].
CRP in Canines
In canines CRP is the major APP used as marker for systemic inflammation / infection. Normally the level of CRP is less than 1.5 mg/ dL or even lower than 0.5 mg/dl. The normal range may be 0.08 to 2.26 mg/dl [13]. The level rises within 4 to 6 hrs after onset of inflammation / infection. Serum CRP level above 3.5 mg/dl, indicates presence of systemic inflammation. Level above 5 mg/dl is a strong evidence of systemic inflammation. Strong correlation was observed between CRP and animal’s temperature and Total Leukocyte counts of canine patients naturally infected with Leptosporosis [14]. CRP levels could be used to monitor early responses to antibiotic treatment and might alert veterinarians to the need for further evaluation or additional treatment. Serum CRP concentrations provide useful information about the severity of inflammation inside the Urinary Bladder. These correlations suggest that CRP concentrations can represent a safe, convenient, and alternative method for evaluating the status of bacterial cystitis [15]. Significantly high CRP values were observed in cases like Lympoma, pyometra, panniculitis, acute pancreatitis, polyarthritis, leptospirosis, babesiosis, parvo viral enteritis, glomerulonephritis, immune mediated disease and malignant neoplasia [16]. Rise in CRP may not be observed in local tumours like leiomyosarcoma, upper respiratory tract infection, diabetes, neurological problems involving intracranial disorders. Since the CRP concentration did not increase in patients with intervertebral disk protrusion, it might be useful in distinguishing arthritis from spinal / brain diseases in patients with lameness. Thus, CRP is a nonspecific inflammatory marker, it could facilitate the diagnosis by indicating the presence and the extent of inflammation
CRP in Elephants
The reference interval for CRP reported herein for Asian elephants (1.3–12.8 mg/l) is like CRP intervals reported in harbor seals (Phoca vitulina) and bottlenose dolphins (Tursiops truncatus). When compare to the CRP, SAA is demonstrated to be the most responsive major APP in elephants [17]. This agrees with previous reports where SAA elevations were noted consistently in elephants with Elephant endotheliotropic herpesvirus (EEHV) and in 2 captive elephants with inflammatory lesions. Further studies are needed to address the reactivity of the CRP reagents with elephant proteins and to consider the use of either elephantspecific reagents or non–antibody-based assays
CRP in Chicken
The birds positive for E.Coli, Pasturella multocida and Staphylococcus aureus infections as well as histomoniasis and adjuvant injection found to be positive for CRP. CRP also positive in clinically normal population. These birds on post-mortem, had lesions consistent with chronic respiratory disease, which is highlighting the use of CRP as a potential biomarker for nonclinical disease [18]. CRP did not rise in chickens as quickly as it does in humans, whereby CRP was detectable 36-48 hours post infection in chickens, compared to 16-18 hours in humans. A more recent study investigated CRP serum concentrations using a human CRP kit and found CRP concentrations to increase
CRP in Equines
A high serum concentration was also found in horses with pneumonia, enteritis, arthritis and after castration. Increased plasma concentration has been observed in carbohydrate induced laminitis. Increased serum concentration of CRP has been found in horses suffering from aseptic inflammation induced by intramuscular turpentine injections [3].
To Know More About Journal of Dairy & Veterinary sciences
Please click on: https://juniperpublishers.com/jdvs/index.php
For more Open Access Journals in Juniper Publishers
please click on: https://juniperpublishers.com/index.php
#wild life rehabilitation#Veterinary sonography#Veterinary Therapeutics#Veterinary Virology#Juniper Publishers#open access journals
0 notes
Text
Kidney transplant in Pune

A kidney transplant is a surgical procedure where a healthy kidney from a donor is transplanted into a recipient who has a damaged or failed kidney. The procedure is performed when the patient's kidneys are no longer able to function properly due to chronic kidney disease, acute kidney injury, or other medical conditions.
Before the transplant, the patient undergoes a series of medical tests to determine their overall health, the type of kidney they need, and whether they are a suitable candidate for the procedure. The donor can be a living donor, usually a family member or a friend, or a deceased donor whose kidney has been donated after their death.
Blood filtration, blood pressure control, and haemoglobin levels are just a few of the vital functions carried out by our kidneys. Chronic Kidney Disease (CKD), another name for kidney failure, denotes chronic and irreversible kidney damage that is permanent. All of the kidneys' functions are compromised by this illness. This worsens blood pressure, anaemia, and bone disease while also causing more kidney damage.
Which factors contribute most to kidney failure?
There are various explanations for why renal failure happens. These danger variables are:
1. Diabetes: Diabetes is the main risk factor for CKD. In this situation, diabetes is discovered in its later stages, by which time other organs like the kidneys would have been impacted, due to a lack of awareness and a proactive approach regarding routine health checks.
2. Hypertension: When left untreated, hypertension poses a very significant risk of renal failure. On the other hand, hypertension is not a significant risk factor when it is under control.
3.Family History: Having chronic kidney disease raises the likelihood of contracting renal failure from a family member.
4.Infections: Repeated kidney or urine infections are further warning signs of this condition.
5. OTC drugs: Taking tablets without the guidance of a trained medical professional can have disastrous consequences on the kidneys as well as numerous other negative side effects.
6.Glomerular disease: The presence of proteins in the urine is an early warning indication of kidney damage and, if left untreated and undiscovered, kidney failure.
What are the indications that your kidneys may be in trouble?
The typical warning signs and symptoms are:
1. Undiagnosed anaemia
2.Weakness
3.Tiredness
4. Issues with sleeping
5. Chest ache
6. Breathing difficulty
7. Appetite loss
alterations in urine
9. Facial and foot swelling
10. Constant nausea
11. Reflux
12. Unaccounted-for weight loss
By the time the patient experiences symptoms and seeks medical attention, the kidney has typically already suffered serious damage. This is the rationale behind not waiting for symptoms to show before having your kidneys examined.
How can renal failure be identified early?
To stop this disease from progressing further, it is essential to have a diagnosis early on before it aggravates. The diagnostic methods comprise:
1. Blood tests: to determine the quantity and concentration of chemicals like urea and creatinine.
2. Urine tests are done to assess the amounts of albumin, creatinine, and blood proteins in the urine to see how effectively the kidneys are working.
3. Imaging tests: CT, MRI, and ultrasound scans can help provide an image of the kidneys and aid in the search for any blockages or anomalies.
4.Biopsy: A little kidney sample is taken, and it is examine
7 Absurdly Efficient Ways to Maintain Healthy Kidneys
What options are there for treating kidney failure?
The stage of the disease determines the course of treatment for CKD.
1. The first three phases of kidney failure are those of early onset, during which the underlying cause must be addressed but no special medications for renal failure are given. For instance, blood sugar levels need to be controlled if a person has diabetes. The same holds true with high blood pressure.
2. Giving up smoking is a crucial first step. The earliest possible investigation must be made into any kidney or urine infections.
3. Kidney function may be impaired by up to 60–70% in the latter stages. In these situations, blood pressure regulation and avoiding kidney-harming substances should be prioritised.
4.Some drugs have been shown to stop further advancement, including angiostein-converting enzyme (ACE) inhibitors and angiostein receptor blockers.
5.Medications are ineffective in stage 5, where kidney loss has reached 80–90%, and the only options are dialysis or, if the patient is healthy enough, a kidney transplant.
6. Exercise can indirectly benefit CKD patients since it helps maintain healthy blood pressure, sugar levels, and weight, all of which slow the disease's progression. moderate workouts, such as
7. As kidney disease progresses past stage 4, the possibility of renal failure increases, and it must be managed with particular drugs and dietary modifications like reducing salt and fluid intake as well as looking for any indicators of cardiac problems. Dialysis and kidney transplantation are the only available treatments for kidney failure.
0 notes
Text
Viruses, Vol. 14, Pages 2825: Development of Fluorescence-Tagged SARS-CoV-2 Virus-like Particles by a Tri-Cistronic Vector Expression System for Investigating the Cellular Entry of SARS-CoV-2
Severe acute respiratory syndrome-related coronavirus-2 (SARS-CoV-2) has caused the pandemic that began late December 2019. The co-expression of SARS-CoV-2 structural proteins in cells could assemble into several types of virus-like particles (VLPs) without a viral #RNA genome. VLPs containing S proteins with the structural and functional properties of authentic virions are safe materials to exploit for virus-cell entry and vaccine development. In this study, to generate SARS-CoV-2 VLPs (SCoV2-SEM VLPs) composed of three structural proteins including spike (S), envelop (E) protein and membrane (M) protein, a tri-cistronic vector expression system was established in a cell line co-expressing SARS-CoV-2 S, E and M proteins. The SCoV2-SEM VLPs were harvested from the cultured medium, and three structure proteins were confirmed by Western blot assay. A negative-stain TEM assay demonstrated the size of the SCoV2-SEM VLPs with a diameter of about 90 nm. To further characterize the infectious properties of SCoV2-SEM VLPs, the VLPs (atto647N-SCoV2-SEM VLPs) were fluorescence-labeled by conjugation with atto-647N and visualized under confocal microscopy at a single-particle resolution. The results of the infection assay revealed that atto647N-SCoV2-SEM VLPs attached to the surface of the HEK293T cells at the pre-binding phase in a ACE2-dependent manner. At the post-infection phase, atto647N-SCoV2-SEM VLPs either fused with the cellular membrane or internalized into the cytoplasm with mCherry-rab5-positive early endosomes. Moreover, fusion with the cellular membrane and the internalization with early endosomes could be inhibited by the treatment of camostat (a pharmacological inhibitor of TMPRSS2) and chlorpromazine (an endocytosis inhibitor), respectively. These results elucidated that SCoV2-SEM VLPs behave similarly to the authentic live SARS-CoV-2 virus, suggesting that the development of SCoV2-SEM VLPs provide a realistic and safe experimental model for studying the infectious mechanism of SARS-CoV-2. https://www.mdpi.com/1999-4915/14/12/2825?utm_source=dlvr.it&utm_medium=tumblr
0 notes
Text
Planning Past "Bio-markers,Inch Believe "Life-markers".
Your analytes were divided with a Kromasil C18 line with Thirty certifications D using a mobile cycle regarding methanol as well as Zero.2% acetic acidity within h2o (Eighty three:18, v/v) and discovered in 238 nm. Under the optimum problems, the most amount of enrichment elements either way analytes was 28. The linear ranges ended up 20.08-1004 as well as 20.00-1000 mu g/L with all the link coefficients including 3.9990 to be able to 3.9994 for lovastatin and simvastatin, correspondingly. The total number of organic and natural favourable taken in extraction had been smaller as compared to 0.Several milliliters, and also the extraction time was 10 min. The particular newly designed environment-friendly sample pretreatment technique would have been a good option to standard tactics, like solid-phase removal, liquid-liquid elimination as well as proteins precipitation, to the HPLC determination of lovastatin as well as simvastatin in neurological samples. Copyright (c) This year Steve Wiley & Son's, Ltd.Advances throughout immunosuppressive drug treatments possess increased the actual short-term emergency involving lean meats hair loss transplant. Nevertheless, drug toxicities are already a life threatening condition in sufferers following long-term management. As a result, it is vital to produce a novel immunosuppressant with low-toxicity. We all researched your immunosuppressive outcomes of Emodin on acute graft being rejected right after hard working liver hair transplant throughout test subjects. The individual test subjects of orthotopic liver transplantation have been separated into organizations as follows: isograft+NS team, allograft+NS party, along with allograft+emodin group. The tactical time of the recipients in each team had been recorded. Histopathological alterations in the liver, along with solution concentrations associated with IL-2, TNF-alpha, and Gö 6983 IL-10 along with their expressions within hard working liver cells had been determined. Our results showed that Emodin treatment prolonged liver allograft success serious amounts of limited histopathologic modifications of severe graft being rejected. The negativity activity directory in groups isograft+NS, allograft+NS, and allograft+emodin had been 1.Fifty-two +/- 0.Thirty seven, Some.89 +/- 0.Seventy-five, as well as Some.12 +/- 0.51, correspondingly (R < 0.02, isograft+NS group versus. allograft+emodin party along with allograft+NS group versus. allograft+emodin team). The actual solution levels of IL-2 along with TNF-alpha had been down-regulated but that involving IL-10 was up-regulated by Emodin. Solution amounts of IL-2 as well as TNF-alpha were higher throughout allograft+NS team compared to allograft+emodin team, but that associated with IL-10 revealed complete opposite effects (S < 3.05 or perhaps 0.09). Adjustments to your appearance of those cytokines inside replanted liver organ tissues ended up consistent with alterations in solution amounts. These final results demonstrate that Emodin offers beneficial possibilities with regard to improving acute negativity right after liver organ hair loss transplant throughout subjects and also extending lean meats allograft survival. The particular components root this specific impact could be related to polarizing the particular Th1/Th2 model for you to Th2. Anat Rec, 294:445-452, The new year. (C) The new year Wiley-Liss, Corporation.The actual synthesis along with structure-activity relationships of a compilation of fresh interferon inducers are usually defined.
#Natural Product Library#Ferroptosis inhibitor#Duvelisib#Capecitabine#Almorexant#Elacridar#Lumacaftor#Bosutinib#LY411575#SB-3CT#UK 5099#CBL0137#Remodelin#Topotecan#Entrectinib#Disulfiram#Pracinostat#Go 6983#MS023#Sotagliflozin#Emapalumab#Pamrevlumab#Evolocumab#Omalizumab#Vedolizumab#Epigallocatechin#Bardoxolone#G150#Enzastaurin#Itacitinib
0 notes
Text
First- as well as second-degree family history regarding ovarian as well as breast cancers in terms of likelihood of obtrusive ovarian cancer malignancy within Dark and white women.
It can be getting increasingly clear which a different range of cell phone and molecular components converge to modify valvular calcium mineral load; that is proved installing histopathologic heterogeneity involving CAVD, and also in the multiplicity regarding mobile or portable kinds that can engage in valve biomineralization. Within this assessment, all of us emphasize our own existing understanding of CAVD condition chemistry, focusing molecular as well as mobile elements of it's legislation. We conclusion by simply pointing to important natural and also medical queries that must be clarified to enable sophisticated condition hosting and also the progression of brand-new ways to treat CAVD clinically.Biologics such as monoclonal antibodies less difficult more technical compared to small-molecule medicines, which usually raises demanding inquiries for the improvement as well as regulation evaluation of follow-on variants of such biopharmaceutical goods (also known as biosimilars) along with their specialized medical make use of as soon as obvious defense for that landmark biologic features ended. With all the the latest introduction regarding regulating walkways pertaining to follow-on versions regarding sophisticated biologics, the role involving analytical systems in looking at biosimilars using the related reference point strategy is appealing to significant desire for creating the development needs with regard to biosimilars. Right here, we all discuss the present advanced within systematic technology to assess about three traits regarding proteins biopharmaceuticals in which regulating authorities get defined as becoming essential in growth approaches for biosimilars: post-translational improvements, three-dimensional structures as well as protein location.Gram-negative sepsis has high deaths along with fatality rate, particularly when challenging by simply acute elimination damage (AKI). Your mechanisms involving AKI inside sepsis continue being inadequately understood. Here we utilised intravital two-photon fluorescence microscopy to analyze the potential for one on one connections involving strained endotoxin along with tubular cells just as one procedure regarding AKI throughout sepsis. Making use of wild-type (WT), TLR4-knockout, as well as bone fragments marrow chimeric rats, many of us learned that endotoxin is readily blocked along with internalized simply by Supposrr que proximal tubules via community TLR4 receptors and thru fluid-phase endocytosis. Simply receptor-mediated friendships between endotoxin as well as Cuando induced oxidative strain within border S2 tubules. Regardless of substantial endotoxin customer base, Suppos que portions demonstrated no oxidative anxiety, probably due to your upregulation involving cytoprotective heme oxygenase-1 and also sirtuin-1 (SIRT1). On the other hand, S2 sections did not upregulate SIRT1 as well as exhibited significant constitutionnel along with functional peroxisomal harm. Used jointly, these kind of information suggest that the particular Suppos que portion behaves as a indicator involving blocked endotoxin, that this uses up. Of course this may restrict the amount of endotoxin from the systemic circulation and also the elimination, it leads to significant supplementary harm to the nearby S2 sections.Qualifications: Though bronchi hair loss transplant from donation soon after heart failure demise (DCD), particularly uncontrolled DCD, is fixed through cozy ischemic intervals, your molecular device regarding comfortable ischemia-reperfusion-injury (IRI) is not effectively elucidated. The intention of this research was to make clear the actual longitudinal components regarding molecular aspects involved in comfortable IRI. Methods: Frosty ischemic-time (CIT)-group lungs were restored and also afflicted by 3-h involving cold availability, although hot ischemic-time (Intelligence)-group bronchi were retrieved NP031112 right after 3-h involving comfortable ischemia. Orthotopic rat respiratory hair transplant has been performed as well as the grafts ended up reperfused pertaining to 1 or even 4-h. The particular graft features, gene expression, and initial regarding -inflammatory compounds from the grafts had been assessed.
#GPCR Compound Library#Androgen Receptor Antagonist#Vinorelbine#Hydrocortisone#Melatonin#Fluoxetine#Favipiravir#Dabigatran#Apixaban#Nitazoxanide#PMA#Pexidartinib#MG132#Rapamycin#Navitoclax#Telaglenastat#Mirdametinib#PEG300#Entinostat#Galunisertib#CL 59806#TKI-258#SHR-1258#NMS-P937#PLB-1001#NP031112#ABL001#IMI 28#SC 58635#NSC 113928
1 note
·
View note
Text
Any computational strategy to realize structure-activity relationship of a single,3-disubstituted imidazole 1,5-α pyrazine types identified as Dupracetam aggressive inhibitors with the IGF-1 receptor in connection with Ewing sarcoma
The objective populace of the review can be a hypothetical cohort associated with Sixty years previous ladies in the past helped by breast-conserving surgical procedure with regard to node-negative, estrogen receptor-positive cancer of the breast with growths < 1 cm. Enough time horizon is actually#keep##links# 15 years, as well as the viewpoint is interpersonal. Your interventions tend to be total breast RT, 3-D CRT, along with brachytherapy breasts irradiation. The end result steps are usually expenses (08 US$), quality-adjusted living years (QALYs), and slow cost-effectiveness rates. The base-case outcome was: 3-D CRT was the preferred strategy, pricing typically $10,800 along with producing 11.21 years old QALYs. On-time complete breasts RT charges $368,000/QALY compared to 3-D CRT, higher than the $100,000/QALY WTP patience. 3-D Cathode ray tube was also preferred around delayed whole breast RT. Brachytherapy was not ever chosen. Awareness analysis established that the final results were responsive to the rate involving repeat outside of the initial tumor quadrant ("elsewhere failure") in one-way evaluation. Probabilistic awareness evaluation revealed that results were responsive to parameter uncertainness, knowning that the particular elsewhere-failure charge along with remedy choices may possibly travel results. The limitation with this examine is effectiveness estimations derive from studies that may not totally represent the population patterned. Like a bottom line, 3-D CRT was chosen over whole breasts RT and then for girls more likely to postpone RT, implying that will 3-D Cathode ray tube could possibly be specific better ahead of randomized test proof.Many of us yet others recently revealed that psychological and also physical activation in form involving environmental enrichment minimizes cerebral beta-amyloid (A new experiment with) deposition in transgenic mouse styles of Alzheimer's disease. This specific influence ended up being unbiased via amyloid forerunner health proteins (APP#keep##links#) term or running as well as fairly because of increased wholesale of your try out. However, the comprehensive mechanisms remain cloudy. In today's review, many of us show ecological enrichment inside TgCRND8 these animals (carrying man Software(Swedish+Indiana)) impact the neurovascular product by greater angiogenesis as well as differential unsafe effects of The experiment with receptor/transporter compounds, specifically up-regulation involving LRP1, ApoE and A2M in addition to down-regulation associated with RAGE to ensure brain to body A new 'beta' clearance is actually facilitated. These kind of outcomes advise a previously unidentified effect of environment enrichment counteracting the general disorder within Alzheimer infected mental faculties.Infection shortly after propagation inhibits establishment of being pregnant. Shot regarding peptidoglycan-polysaccharide (PG-PS), a part of gram-positive bacterias, into lambs about evening 5 after multiplying reduces being pregnant rate. Findings specified to gauge the particular acute-phase result (Interest rates) throughout ewes for you to shot involving PG-PS about morning A few#keep##links# right after propagation (day time 3). Catheters had been placed in to the jugular and posterior vena cava upon morning Four. Upon morning Your five, ewes were challenged along with saline or perhaps 30 mu g/kg weight (BW) PG-PS (Exp A single) or 60 mu g/kg BW PG-PS (Exp A couple of). Blood samples had been gathered each and every 20 min for 6 h (Exp One particular) and every 16 min for just two l, by the hour for 14 h, at 24, Thirty five, as well as Forty-eight l (Exp A couple of). Body temperature and medical signs of contamination had been watched in Exp 2.
0 notes
Text
Measuring CRP and prealbumin (negative acute phase protein), as CRP declines, prealbumin should go up. There's currently nothing in the literature about this being a useful way to determine nutritional status.
You can use prealbumin to reflect intake over 2-3 days. When you see C reactive protein go down, that could be your opportunity to do an intervention that you weren't able to do before because they were too stressed.
#dietetics#prealbumin#CRP#inflammation#acute phase protein#negative acute phase protein#Dr P likes this#stress
0 notes
Text
100 days of productivity
day 15
RS/CVS
hypersensitivity pneumonitis is a a type III reaction characterised by circulating IgG precipitins
valve replacement: biprosthetics for older/limited life expectancy, mechanical for younger
statins: expect a 40% reduction in non-HDL cholesterol after 3 months
arrhythmogenic right ventricular cardiomyopathy = AD inherited cause of SCD, especially in young patients after heavy exercise... but due to RV fibrofatty infiltration (which sets it apart from HOCM)
CNS/Ophthal
Froin syndrome = xanthocromia, ↑protein and coagulation of CSF below the level of blockage of CSF flow d/t activation of coagulation factors in thecal stagnated fluid
although wet age-related macular degeneration can mimic proliferative diabetic retinopathy, diabetic eye disease consists of multiple ocular stigmata (glaucoma, cataracts, preproliferative signs, even diabetic macular degeneration), whereas ARMD exclusively affects the retina; the most important risk factor for ARMD is smoking
Endocrine
MCC of primary hyperparathyroidism is a solitary adenoma, but MCC of primary hyperaldosteronism is bilateral adrenal hyperplasia
in 1° hyperPTHism, the parathyroids actually retain some feedback control from Ca levels: so, although Ca might be grossly elevated, PTH may be in reference range. HOWEVER, in the normal homeostatic body, when Ca is elevated, PTH should 'normally' be *below* reference range, and therefore any PTH that is *within* reference range when Ca is elevated is inappropriately elevated—this is the clue to hyperPTH
however in 3° hyperPTH, parathyroids *lose* feedback control from Ca and PTH levels are *above* reference range even if Ca is above reference range
hypocalcaemia predisposes to cataract formation
Onc/Haem
for breakthrough pain, calculate 10% of total daily morphine dosage and give every 2-4 hours; once pain stabilises, convert to sustained-release morphine (or fent patches)
steroids help alleviate symptoms of radiation pneumonitis in the acute phase, but they neither prevent fibrosis nor relieve chronic symptoms, which should be managed symptomatically (eg, dextromethorphan + oxygen); also if steroids do not produce symptomatic relief within 3-4 days, they will not produce symptomatic relief at all
Renal/Biochem
most common cause of calcified bladder worldwide → Schistosoma haematobium
mechanism for hyperuricaemia in von Gierke's disease: ↑G6P acts as a substrate for G6P dehydrogenase, and get shunted into the pentose-phosphate pathway (aka hexose-monophosphate shunt) and ramps ip production of pentose sugars → ↑pentoses stimulate and act as a substrate for phosphoribosyl pyrophosphate (PRPP) synthetase → ↑purine salvaging → ↑purine degradation → ↑uric acid
Rheum/Derm
rugger-jersey spine is seen in all causes of hyperparathyroidism (including CKD)
after a night of PASHion (leading to preggs), an RA sufferer can use these DMARDs safely: Prednisolone, Azathioprine, Sulfasalazine*, Hydroxychloroquine (*yes, even though it is a sulfa drug—does NOT have a strong risk of causing NTDs)
Immuno/Genetics/Misc
MCC of Prader-Willi is actually microdeletion of 15q11-13; maternal disomy is the second most common cause
vaccines contraindicated in immunosuppressed: You Musn't Prescribe BCG In case They RIP Stat = Yellow fever, MMR, Polio, BCG, Intranasal flu, Typhoid, Rotavirus, Shingles
anti-MuSK = anti muscle-specific kinase, found in myasthenia sufferers negative for anti-Nm antibodies with no evidence of thymoma
+ve LR = Sn/(1-Sp); -ve LR = (1-Sn)/Sp
10 notes
·
View notes
Text
Diseases of the thyroid gland
----------------------------------
Chapter 1 : Hyperthyroidism.
-----------------
We're going to discuss:
What is Hyperthyroidism?
Causes of hyperthyroidism?
Clinical manifestation.
Lab works
Other investigations
Treatment
What is a thyroid storm?
----------------------------------------
What is hyperthyroidism?
It is a state where there is ⏫ synthesis of the thyroid hormones : T4 & T3 ➡ ⏫ levels of these hormones in the blood.
-------------------------------
Causes:
Graves' disease (diffuse toxic goiter)
Plummer disease (multinodular toxic goiter)
Toxic thyroid adenoma (single nodule)
Subacute thyroiditis & Hashimoto thyroiditis. (Transient hyperthyroidism)
Fetal thyrotoxicosis
Other rare causes:
- postpartum thyroiditis (transiet)
- Iodine-induced hyperthyroidism.
- Excessive dose of levothyroxine.
------------------
1. Graves' disease:
Autoimmune disorder.
Thyroid-stimulating immunoglobulin TSI (IgG) binds to the TSH receptors on the thyroid cells ➡ triggers the synthesis of excess thyroid hormones.
Younger women >
Goiter : every thyroid cell is hyperfunctioning so it affects ALL parts of the gland >> diffuse. Non tender
2. Plummer disease:
Starts with chronic lack of dietary Iodine ➡ low levels of T4 ➡ triggers high levels of TSH ➡ Thyroid hypertrophy & hyperplasia.
The growth is uneven >> nodules.
These nodules become toxic when a genetic mutation happens and causes TSH recepters to be constantly ON. >> ⏫⏫⏫ T4/T3.
That elevation acts as a negative feed back to the pituitary gland to secrete less TSH >> the rest of the thyroid is not functioning >> atrophy .
3. Adenoma : 2% of all cases.
4. Thyroiditis:
Inflammation of the thyroid gland >> releasing the previously synthesized thyroid hormones ➡ temporary ⏫⏫ in circulating T4/T3.
A hypothyoid phase may follow.
5. Fetal thyrotoxicosis:
Classically in an infant born to a mother with Graves disease. TSI are IgG and can cross the placenta.
--------------------------------------------
Clinical manifestations : Symptoms
Nervousness.
Irritability
Insomnia.
Fine tremor
Hyperactivity
Heat intolerance & excessive sweating.
Weight loss despite increased appetite.
Proximal muscle weakness.
Palpitations.
Signs:
On the thyroid glad:
Graves' : diffusely enlarged. symmetric . Nontender gland. Bruit may be present.
Subacute thyroiditis: exquisitely tender. Diffusely enlarged (viral illness)
Plummer: bump. Irregular . Asymmetric gland.
Toxic adenoma: single nodule with atrophic gland.
Extrathyroidal:
Eyes: - Edema of the extraocular muscles ➡ proptosis (hallmark of Graves') - lid lag - lid retraction
- corneal exposure ➡ excessive tearing.
Cardiovascular effects: ⏫ Blood pressure.
- Arrhythmias : Sinus tachycardia - Atrial fibrillation
Skin: Warm & moist - pretibial myxedema (specific to Graves')
Neurologic: Hyperreflexia - fine tremor.
-----------------------------------
Lab works:
⏬⏬ TSH
⏫⏫ free T4 & FT3
Other investigations:
1. RAIU:
Radioactive iodine uptake scan.
Useful to differentiate the causes of hyperthyroidisim.
If the uptake is ⏫look for the findings (forms):
Diffuse ( homogeneous) ➡ Graves'
Heterogeneous (multiple nodules of ⏫uptake) ➡ plummer
Focal (one area of ⏫ uptake w/suppression of rest of the gland) ➡ adenoma (hot nodule)
No RAIU findings (⏬⏬uptake) we look at serum thyroglobulin:
⏫ ➡ Thyroiditis /iodine exposure / extraglandular production
⏬ ➡ Exogenous thyroid hormone.
2. Radioactive T3 uptake:
Gives information about the status of TBG
We give resin to the patient + radioactive T3.
Radioactive T3 will bind to resin only when there is no space left on TBG.
SO WHEN THERE IS ⏫T4 ➡ no available seats on TBG ➡ more radioactive T3 will bind to resin ➡ ⏫ radioactive uptake.
The importance of this is to know if there is true hyperthyroidism or increased TBG
High TBG production ➡ low radioactive T3 uptake.
3. Free thyroxine index (FTI) :
Proportional for FREE T4 concentration.
Calculated to correct for the changes in the thyroid binding proteins.
FTI : ( Radioactive T3 uptake × serum total T4) /100
FTI : (patient's radioactive T3 uptake / normal radioactive T3 uptake) × total T4
Normal : 4-11
--------------------------------------------
Treatment :
1. Pharmacologic:
🎐Immediate control of adrenergic symptoms:
B-blockers (propanolol)
🎐 Anti-thyroid drugs: Thionamides
Methimazole:
1- Inhibits thyroid peroxidase ➡ stops the oxidation of Iodide into Iodine
2- Inhibits the coupling of DIT and MIT to form T3 & T4.
PTU (propylthiouracil) :
Shares the same mechanism with Methimazole except that PTU works on the peripheral tissue by
- Inhibiting the converting of T4 into T3.
⚠ Watch for side effects⚠
⚠Agranulocytosis
⚠Skin rash
⚠Arthralgias
Specific ⚠ for PTU is:
Hepatotoxicity.
During pregnancy:
Both can cross the placenta but it is preferred to give:
PTU at the first trimester
Methimazole at the 2nd and 3rd trimester.
Sodium ipodate or iopanoic:
Lowers serum T3 & T4 levels and causes rapid improvement of hyperthyroidism.
Appropriate for acute management of severe hyperthyroidism that's not responding to conventional therapy.
2. RAI ; Radioactive iodine:
Causes destruction of thyroid follicular cells.
Uses IODINE 131
Most common for: Graves' disease & multi-nodular goiter.
If the first dose doesn't control the hyperthyroidism within 6 to 12 months then administer another dose.
✔ Selected pations ✔
✔ Elderly patients w/Graves disease.
✔ Solitary toxic nodule
✔ Patients w/graves disease in whom therapy w/antithyroid drugs fails.
⚠ Warning ⚠
⚠ Hypothyroidism over time in the majority patients. ⚠
Note :
Ophthalmopathy can worsen after RAI prevent that by prophylactic therapy w/prednisone in high-risk patients.
3. Surgery:
Very effective
Only 1% of patients are treated by it.
Often reserved w/patients that have large goiters ; more common in toxic multinodular goiter.
⚠ Side Effects ⚠
⚠ permanent hypothyroidism 30%
⚠Recurrent laryngeal nerve palsy 1%
⚠Permanent hypoparathyroidism 1%
⚠ watch for hypocalcemia (due to inflammation/removal of the parathyroid glands)
------------------------------------------
Treatment plan :
Immediate control of adrenergic symptoms (of any cause) ➡ (beta-blocker) propanolol
Non-pregnant patients w/Graves' disease: beta blocker + Methimazole Taper B-blocker after 4-8 weeks (once methimazole takes effect) give methimazole for 1-2 years then measure TSI at 12 months : ✔ Absent ➡ discontinue therapy. ✔ Relapse ➡ Resume methimazole for 1 more year or radioactive therapy.
Pregnant patients w/Graves' disease : Endocrinology consult is indicated before starting treatment.
Toxic multinodular goiter or Toxic adenoma: RAI or surgery Methimazole pretherapy for surgery and before RAI in selected patients.
------------------------------------
What is a thyroid storm?
Rare, life-threatening complication of thyrotoxicosis.
Characterized by an acute exacerbation of the manifestations of hyperthyroidism.
There's usually a precipitating factor: infection, DKA, stress (Surgery, illness, childbirth)
High mortality rate
Clinical manifestations:
✔ Marked fever
✔ Tachycardia
✔ agitation
✔ Confusion
✔ GI symptoms (nausea , vomiting , diarrhea)
Treatment:
Provide supportive therapy : IV fluids , cooling blankets and glucose
Give antithyroid agents (PTU preferred due to its peripheral effects) followed w/iodine.
B-blockers
Dexamethazone (steroids) to impair peripheral generation of T3 from T4 and to provide adrenal support.
-------------------------
Wow that was a long one XD
I tried to include all the important stuff :)
Resources:
First-aid
Kaplan lecture notes 2019
Medscape
Pocket medicine
Step-up to medicine.
#studyblr#study motivation#medicine#biology#medicinewithmarie#endocrinewithmarie#hyperthyroidism#notes#usmle#usmle step 2#medical student#medblr#notes 2020#thyroid#education#endocrine notes#nedicine
27 notes
·
View notes
Text
One of my pts has been C/O headache and he was worked up for giant cell arteritis (GCA). He was treated with prednisone. I remember he was also complaining of visual symptoms. I thought it might be a result of a recent stroke he had, but it didn't make sense given the side that he had the stroke on. Now that I'm reviewing and thinking about it, it makes sense. My attending told the pt to stop prednisone because his ESR and CRP came back normal, but these are non-specific tests, so it shouldn't be these that are used to diagnose. If I remember correctly from medical school, a temporal artery biopsy is the gold standard for diagnosis.
From UpToDate:
When to suspect giant cell arteritis – The diagnosis of giant cell arteritis (GCA, also known as Horton disease, cranial arteritis, and temporal arteritis) should be considered in a patient over the age of 50 years who complains of or who is found to have one or more of the following:
•A new headache
•Abrupt onset of visual disturbances, especially transient/permanent monocular visual loss
•Jaw claudication
•Unexplained fever or anemia
•Elevated erythrocyte sedimentation rate (ESR) and/or serum C-reactive protein (CRP)
•Temporal artery abnormalities such as tenderness to palpation, decreased pulsation, presence of nodules
Any of these findings are of special concern in the context of a current or previous diagnosis of polymyalgia rheumatica (PMR) because of the association between GCA and PMR.
●Initial diagnostic evaluation
•Laboratory data – Laboratory data can aid in the evaluation of GCA and its differential diagnosis, but they are not specific and cannot be relied on as definitive evidence for or against a possible diagnosis of GCA. Initial laboratory testing should include the ESR and CRP levels, which are almost always high in GCA. However, normal acute phase reactants do not exclude the diagnosis of GCA.
•Assessment of the temporal artery – A suspected diagnosis of GCA should be confirmed by temporal artery biopsy or temporal artery color Doppler ultrasound (CDUS).
Scheduling the temporal artery biopsy or CDUS should not delay initiation of treatment with the appropriate dose of glucocorticoids in a patient with a high likelihood of GCA, since delay can put the patient at risk for complications, particularly sight loss.
Evaluation for large vessel GCA in patients with a nondiagnostic initial workup – When the diagnosis of GCA is still suspected in a patient who has had a negative temporal artery biopsy and/or CDUS, the possibility of large vessel involvement can be considered. The diagnostic procedure of choice for suspected large vessel GCA is an advanced imaging study of the aorta and/or its branches. Computed tomography (CT) or CT with angiography (CTA), magnetic resonance imaging (MRI) or MR angiography (MRA), and positron emission tomography (PET) or PET with CT are useful for the identification of large vessel GCA. CDUS of the epiaortic vessels (eg, carotid, subclavian, and axillary arteries) can also be used to diagnose large vessel vasculitis.
Diagnosis – The diagnosis of GCA should not be based on clinical presentation alone but should be premised on histopathologic proof or evidence from imaging exams. Occasionally clinicians are faced with the diagnostic challenge of a negative workup, which should include negative temporal artery biopsy or biopsies and, if indicated, imaging of the large vessels. In this situation, the clinician can choose to either:
-Conclude that the patient does not have GCA and pursue alternative diagnoses, or
-Make a clinical diagnosis of GCA and treat accordingly
Differential diagnosis – The differential diagnosis of GCA includes other vasculitides (eg, Takayasu arteritis, small- and medium-sized vessel vasculitides, primary angiitis of the central nervous system), nonarteritic anterior ischemic optic neuropathy (NAAION), and infection.
Postdiagnostic imaging evaluation in patients with cranial arteritis – We routinely screen for large vessel involvement in all patients with newly diagnosed cranial GCA by performing CDUS of the epiaortic vessels (eg, carotid, subclavian, and axillary arteries).
2 notes
·
View notes
Link
by Rossella Talotta
To the Editor,
I read with great interest the article by Vojdani et al. [1], concerning the hypothesis of a molecular mimicry mechanism between the nucleoprotein/spike protein of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and self-antigens. Viruses are notoriously involved in the pathogenesis of autoimmune diseases [2], and the authors reasonably conclude that such a cross-reactivity might lead to the development of immune-mediated disorders in COronaVirus Disease-19 (COVID-19) patients in the long term. The authors also suggest that a similar scenario might take place following COVID-19 vaccination.
Vaccine-associated autoimmunity is a well-known phenomenon attributed to either the cross-reactivity between antigens or the effect of adjuvant [3]. When coming to COVID-19 vaccine, this matter is further complicated by the nucleic acid formulation and the accelerated development process imposed by the emergency pandemic situation [4]. Currently, lipid nanoparticle-formulated mRNA vaccines coding for the SARS-CoV-2 full-length spike protein have shown the highest level of evidence according to the efficacy and safety profile in clinical trials, being therefore authorized and recommended for use in the United States and Europe. Although the results from phase I and II/III studies have not raised serious safety concerns [5], the time of observation was extremely short and the target population not defined. Reported local and systemic adverse events seemed to be dose-dependent and more common in participants aged under 55 years. These results presumably depend on the higher reactogenicity occurring in younger people that may confer greater protection towards viral antigens but also predispose to a higher burden of immunological side effects.
The reactogenicity of COVID-19 mRNA vaccine in individuals suffering from immune-mediated diseases and having therefore a pre-existent dysregulation of the immune response has not been investigated. It may be hypothesized that immunosuppressive agents prescribed to these patients mitigate or even prevent side effects related to vaccine immunogenicity.
Besides the mechanism of molecular mimicry, mRNA vaccines may give rise to a cascade of immunological events eventually leading to the aberrant activation of the innate and acquired immune system.
RNA vaccines have been principally designed for cancer and infectious diseases. This innovative therapeutic approach is based on the synthesis of RNA chains coding for desired antigenic proteins and exploits the intrinsic immunogenicity of nucleic acids. In order to avoid degradation by RNases, RNA can be encapsulated in nanoparticles or liposomes, which deliver the cargo inside target cells following a process of endocytosis. mRNA is then translated into immunogenic proteins by cell ribosomal machinery [6].
However, prior to the translation, mRNA may bind pattern recognition receptors (PRRs) in endosomes or cytosol. Toll-like receptor (TLR)3, TLR7 and TLR8 are able to recognize chains of double-stranded (ds)RNA or single-stranded (ss)RNA in endosomes, while retinoic acid-inducible gene-I (RIG-I) and melanoma differentiation-associated protein 5 (MDA5) may detect short and long filaments of dsRNA in the cytosol. The final result is the activation of several pro-inflammatory cascades, including the assembly of inflammasome platforms, the type I interferon (IFN) response and the nuclear translocation of the transcription factor nuclear factor (NF)-kB [7].
Importantly, the up-regulation of these immunological pathways is widely considered to be at the basis of several immune-mediated diseases, especially in genetically predisposed subjects who have an impaired clearance of nucleic acids [8]. This could particularly hold true in young female individuals, due to the over-expression of X-linked genes presiding over the antiviral response and the stimulatory effect played by estrogens on the immune system. The X chromosome hosts several genes involved in the immune response, including TLR7 and TLR8 genes, and about 10% of microRNAs indirectly controlling the activation of the immune system [9].
Therefore, young and female patients who are already affected or predisposed (e.g. immunological and serological abnormalities in absence of clinical symptoms, familiarity for immune-mediated diseases) to autoimmune or autoinflammatory disorders should be carefully evaluated for the benefits and risks of COVID-19 mRNA vaccination. According to epidemiological data, these subjects may develop the infection asymptomatically or pauci-symptomatically and it is worth noting that, in line with the article of Vojdani et al. [1], the presence of autoreactive cells and autoantibodies cross-reacting against SARS-CoV-2 epitopes may even turn naturally protective towards the infection. Until proven otherwise, the administration of a nucleic acid vaccine may instead put these individuals at risk of unwanted immunological side effects by either sensitizing the PRRs or generating cross-reactive cell clones and antibodies. Moreover, COVID-19 mRNA vaccine might differently stimulate myeloid or plasmacytoid dendritic cells (DCs), generating an unbalance in the downstream cytokine pathways that play a crucial role in autoimmunity and autoinflammation [3].
Modifications in nucleoside and nanoparticle composition through a proper manufacturing may help to prevent some of these drawbacks. For instance, the substitution of uridine with pseudouridine was shown to reduce immunogenicity and type I IFN production while enhancing the synthesis of viral antigenic proteins [10]. A strong type I IFN response may, in fact, negatively affect the vaccine efficacy by suppressing the process of mRNA translation [10]. However, type I IFNs play a beneficial role in strengthening the antiviral response, as they favor the maturation of DCs, the CD8+ T cell-mediated cytotoxicity and the secretion of several cytokines, like interleukin (IL)-12 and IL-23 [11]. Notably, polymorphisms in the genes encoding these cytokines or their receptors have been associated with the susceptibility to autoimmune diseases [12]. Additionally, an excessive production of type I IFNs may result in the breakdown of the immunological tolerance and, therefore, in autoimmunity [10].
Lipid components may also dictate the type and intensity of the immune response, by enhancing the production of IFN-γ, IL-2 and tumor necrosis factor (TNF)-α with the subsequent activation of both CD4+ and CD8+ T lymphocytes. Although this is not the case of the authorized COVID-19 mRNA vaccines, future formulations containing adjuvant like TLR agonists [13] may exacerbate pre-existing autoimmune or autoinflammatory disorders and should therefore be discouraged in this cohort of patients.
Given the current state of the art, my view is that individuals with a dysfunctional immune response should receive the COVID-19 mRNA vaccine only if the benefits of this approach clearly outweigh any risks and after a careful evaluation case by case.”
References
1. Vojdani A., Kharrazian D. Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases. Clin. Immunol. 2020;217 doi: 10.1016/j.clim.2020.108480. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
2. Talotta R., Robertson E. Autoimmunity as the comet tail of COVID-19 pandemic. World J. Clin. Cases. 2020;8:3621–3644. doi: 10.12998/wjcc.v8.i17.3621. [PMC free article] [PubMed
] [CrossRef] [Google Scholar
3. Goriely S., Goldman M. From tolerance to autoimmunity: is there a risk in early life vaccination? J. Comp. Pathol. 2007;137:S57–S61. doi: 10.1016/j.jcpa.2007.04.013. [PubMed] [CrossRef] [Google Scholar
4. Kostoff R.N., Kanduc D., Porter A.L., Shoenfeld Y., Calina D., Briggs M.B., Spandidos D.A., Tsatsakis A. Vaccine- and natural infection-induced mechanisms that could modulate vaccine safety. Toxicol. Reports. 2020;7:51–64. doi: 10.1016/j.toxrep.2020.10.016. [PMC free articlePubMedCrossRefGoogle Scholar
5. Polack F.P., Thomas S.J., Kitchin N., Absalon J., Gurtman A., Lockhart S., Perez J.L., Pérez Marc G., Moreira E.D., Zerbini C., Bailey R., Swanson K.A., Roychoudhury S., Koury K., Li P., Kalina W.V., Cooper D., Frenck R.W., Hammitt L.L., Türeci Ö., Nell H., Schaefer A., Ünal S., Tresnan D.B., Mather S., Dormitzer P.R., Şahin U., Jansen K.U., Gruber W.C. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020 doi: 10.1056/NEJMoa2034577. [PMC free article
] [PubMed
] [CrossRef
] [Google Scholar
6. Marć M.A., Domínguez-Álvarez E., Gamazo C. Nucleic acid vaccination strategies against infectious diseases. Expert Opin. Drug Deliv. 2015;12 doi: 10.1517/17425247.2015.1077559. [PubMedCrossRefGoogle Scholar
7. Reikine S., Nguyen J.B., Modis Y. Pattern Recognition and Signaling Mechanisms of RIG-I and MDA5. Front. Immunol. 2014;5 doi: 10.3389/fimmu.2014.00342. 342-undefined. [PMC free article PubMed] [CrossRef Google Scholar
8. Pelka K., Shibata T., Miyake K., Latz E. Nucleic acid-sensing TLRs and autoimmunity: novel insights from structural and cell biology. Immunol. Rev. 2016;269:60–75. doi: 10.1111/imr.12375. [PubMed [CrossRefGoogle Scholar
9. Schurz H., Salie M., Tromp G., Hoal E.G., Kinnear C.J., Möller M. The X chromosome and sex-specific effects in infectious disease susceptibility. Hum. Genomics. 2019;13 doi: 10.1186/s40246-018-0185-z. 2-undefined. [PMC free article] [PubMed] [CrossRef] [Google Scholar
10. D’haese S., Lacroix C., Garcia F., Plana M., Ruta S., Vanham G., Verrier B., Aerts J.L. Off the beaten path: novel mRNA-nanoformulations for therapeutic vaccination against HIV. J. Control. Release. 2020 doi: 10.1016/j.jconrel.2020.11.009. [PubMed
] [CrossRef
] [Google Scholar
11. He S., Mao X., Sun H., Shirakawa T., Zhang H., Wang X. Potential therapeutic targets in the process of nucleic acid recognition: opportunities and challenges. Trends Pharmacol. Sci. 2015;36:51–64. doi: 10.1016/j.tips.2014.10.013. [PubMed [CrossRef] [Google Scholar
12. Vandenbroeck K. Cytokine gene polymorphisms and human autoimmune disease in the era of genome-wide association studies. J. Interf. Cytokine Res. 2012;32:139–151. doi: 10.1089/jir.2011.0103.[PMC free article] [PubMed [CrossRef [Google Scholar
13. Liang Z., Zhu H., Wang X., Jing B., Li Z., Xia X., Sun H., Yang Y., Zhang W., Shi L., Zeng H., Sun B. Adjuvants for coronavirus vaccines. Front. Immunol. 2020;11 doi: 10.3389/fimmu.2020.589833.[PMC free article [PubMed CrossRef] [Google Scholar]
2 notes
·
View notes
Text
Are You Experiencing Some of the Common Symptoms of Ascension?
(Long Post)
Some of you may find this helpful, please only take what helps and do not worry or fret if something in this list does not resonate with you. You can take what resonates and leave what doesn’t. That is okay.
Those who need to hear this will be drawn to it, for that is the way of our great Universe.
~ Blessings to All ~
I was just looking at quite a few pages of COVID long haulers support groups...where a COVID-positive was indicated and they have not fully recovered their well being. 85% of the descriptions of their symptoms (which are found as negative health concerns) are labelled as COVID...some are being told it’s Lyme, fibromyalgia and chronic fatigue among other unknown causes. As I reviewed the endless lists and common symptoms I found that they are very similar to ascension symptoms.
However most do not realize that they are going through a physical change in their DNA structure. Those who are aware and have gone through the many waves of change understand and roll with the fatigue and other symptoms in gratitude and not fear, trusting and seeing the positive change in who they are as this occurs. It is a leaving or shedding what has been known... to reveal the true self within.
I felt it would be supportive for you, and for your friends and loved ones to review to find a “positive outlook” on a changing body and world. May this fill you with hope, for all are emerging through this great transformation.
PLEASE NOTE: This article is based on work presented by Samuel Greenberg's original list and is not authored by Dr. Nickerson. Before you read this, realize that you are okay and that what you are experiencing is "The SHIFT". This is a normal process when the universal vibrational energy forces you to rise above your normal 3D level of existence here on Earth. It’s all okay. When in doubt, please see your doctor to confirm to alleviate fear.
Ascension Symptoms:
1. Feeling as though you are in a pressure cooker or in intense energy; feeling stress. Remember, you are adjusting to a higher vibration and you will eventually adjust. Old patterns, behaviors and beliefs are also being pushed to the surface. There is a lot going on inside of you.
2. A feeling of disorientation; not knowing where you are; a loss of a sense of place. You are not in 3D anymore, as you have moved or in the process of moving into the higher realms.
3. Unusual aches and pains throughout different parts of your body. You are purifying and releasing blocked energy vibrating at 3D, while you are vibrating in a higher dimension.
4. Waking at night between 2 and 4 a.m. Much is going on in your dream state. You can’t be there for long lengths of time and need a break. This is also the ‘cleansing and releasing’ hour.
5. Memory loss. A great abundance of short term memory loss and only vague remembrances of your past. You are in more than one dimension at a time, and going back and forth as part of the transition, you are experiencing a ‘disconnect’. Also, your past is part of the Old, and the Old is forever gone. Being in the Now is the way of the New World.
6. ‘Seeing’ and ‘hearing’ things. You are experiencing different dimensions as you transition, all according to how sensitive you are and how you are wired.
7. Loss of identity. You try to access the Old you, but it is no longer there. You may not know who you are looking at in the mirror. You have cleared much of your old patterns and are now embodying much more light and a simpler, more purified divine you. All is in order, You are okay.
8. Feeling ‘out of body’. You may feel as though someone is talking, but it is not you. This is our natural defense mechanism of survival when we are under acute stress or feeling traumatized or out of control. Your body is going through a lot and you may not want to be in it. My ascension guide told me that this was a way of easing the transition process, and that I did not need to experience what my body was going through. This only lasted a short time. It passes.
9. Periods of deep sleeping. You are resting from all the acclimating and are integrating, as well as building up for the next phase.
10. Heightened sensitivities to your surroundings. Crowds, noise, foods, TV, other human voices and various other stimulations are barely tolerable. You also overwhelm very easily and become easily overstimulated. You are tuning up. Know that this will eventually pass.
11. You don’t feel like doing anything. You are in a rest period, ‘rebooting’. Your body knows what it needs. In addition, when you begin reaching the higher realms, ‘doing’ and ‘making things happen’ becomes obsolete as the New energies support the feminine of basking, receiving, creating, self-care and nurturing. Ask the Universe to ‘bring’ you what you want while you are enjoying yourself and having fun.
12. An intolerance for lower vibrational things of the 3D, reflected in conversations, attitudes, societal structures, healing modalities, etc. They literally make you feel ‘sick’ inside. You are in a higher vibration and your energies are no longer in alignment. You are being ‘pushed, to move forward; to ‘be’ and create the New.
13. A loss of desire for food. Your body is adjusting to a new, higher state of being. Also, part of you does not want to be here anymore in the Old.
14. A sudden disappearance of friends, activities, habits, jobs and residences. You are evolving beyond what you used to be, and these people and surroundings no longer match your vibration. The New will soon arrive and feel so-o-o-o much better.
15. You absolutely cannot do certain things anymore. When you try to do your usual routine and activities, it feels downright awful. You are evolving beyond what you used to be, and these people and surroundings no longer match your vibration. The New will soon arrive and feel so-o-o-o much better.
16. Days of extreme fatigue. Your body is losing density and going through intense restructuring.
17. A need to eat often along with what feels like attacks of low blood sugar. Weight gain, especially in the abdominal area. A craving for protein. You are requiring an enormous amount of fuel for this ascension process. Weight gain with an inability to loose it no matter what you do is one of the most typical experiences. Trust that your body knows what it is doing.
18. Experiencing emotional ups and downs; weeping. Our emotions are our outlet for release, and we are releasing a lot.
19. A wanting to go Home, as if everything is over and you don’t belong here anymore. We are returning to Source. Everything is over, but many of us are staying to experience and create the New World. Also, our old plans for coming have been completed.
20. Feeling you are going insane, or must be developing a mental illness of some sort. You are rapidly experiencing several dimensions and greatly opening. Much is available to you now. You are just not used to it. Your awareness has been heightened and your barriers are gone. This will pass and you will eventually feel very at Home like you have never felt before, as Home is now here.
21. Anxiety and panic. Your ego is losing much of itself and is afraid. Your system is also on overload. Things are happening to you that you may not understand. You are also losing behavior patterns of a lower vibration that you developed for survival in 3D. This may make you feel vulnerable and powerless. These patterns and behaviors you are losing are not needed in the higher realms. This will pass and you will eventually feel so much love, safety and unity. Just wait.
22. Depression. The outer world may not be in alignment with the New, higher vibrational you. It doesn’t feel so good out there. You are also releasing lower, darker energies and you are ‘seeing’ through them. Hang in there.
23. Vivid, wild and sometimes violent dreams. You are releasing many, many lifetimes of lower vibrational energy. Many are now reporting that they are experiencing beautiful dreams. Your dream state will eventually improve and you will enjoy it again. Some experience this releasing while awake. My mother commented one day that she believed I was having nightmares in the daytime.
24. Night sweats and hot flashes. Your body is ‘heating’ up as it burns off residue.
25. Your plans suddenly change in mid-stream and go in a completely different direction. Your soul is balancing out your energy. It usually feels great in this new direction, as your soul knows more than you do. It is breaking your ‘rut’ choices and vibration.
26. You have created a situation that seems like your worst nightmare, with many ‘worst nightmare’ aspects to it. Your soul is guiding you into ‘stretching’ into aspects of yourself where you were lacking, or into ‘toning down’ aspects where you had an overabundance. Your energy is just balancing itself.
Remember.....Finding your way to peace through this situation is the test you have set up for yourself. This is your journey, and your soul would not have set it up if you weren’t ready. You are the one who finds your way out and you will.
Looking back, you will have gratitude for the experience and realize that you are a different person.
I hope this helps.
#ascension#awakening#enlightenment#5d#3d#spiritualguidance#spiritual gangster#spiritual development#spirituality#dna#dna activation#covid#covid-19#coronavirus#new age#it's a new world
5 notes
·
View notes
Text
Dexamethasone- The Wonder Drug or The Desperate Hope?
Despite all the desperate efforts to control the spread of the virus SARS-CoV2, wiz getting on nerves of us, humans, as a very, very, social ;sometimes; toxic, species
Hello,
I am Arjun and this picture is not me. Its been like 6 months into this pandemic and I have been eating all this junk you can actually say that this picture is me.Gosh, I was so excited for 2020 because so many exciting things were about to happen.
Elon Musk was actually going to complete that Neuralink trial thingy by the end of this year and I could finally end my never ending struggle to take care of my> oh my god> numerous organ systems? my weight ? and my metabolism? any my eyesight? and my everything? Who the h*ll does that?
But no, its just not happening guys. I am pretty sure now because 2020 is just the worst year! let us just agree to that as a starter!
Can you guys like believe that we cannot go out for window shopping anymore?
I go out to buy milk and I have to wear this Halo master chief armored suit thingy.
Ordering from Starbucks is just a pandemic and one kidney away and I certainly cannot beat the Indian summer heat.
I am desperate, I am so desperate that Baba Ramdev doing Yoga at 4:30 in the morning actually makes sense somehow.
I am so desperate that my lockdown 3 AM anthem is :
Taoism talks about how you should go with the flow so thats what I am actually doing, I am finally going with the flow,
But it feels like this flow is actually going towards a falling waterfall and we all are almost on the edge now.
The International airlines are shut down
You cannot travel to Ladakh or Goa with your friends and Emiway just featured Macklemore in his song? Like seriously? He went from worshiping M&M to MM?
Half a million people have died due to the Coronavirus alone
Yemen is going through a civil war and one of the worst famines in modern history.
And for some reason Delhi is getting its ego drop by a series of Earthquakes.
Well, Thank You 2020, UNESCO just declared you to be the most confused year in the history of mankind. Like seriously, please decide what you want man.
Now, lets talk medicine.
Lets talk about the scope Dexamethasone potentially has, against Covid-19,
There has been numerous claims in the recent past to have successfully found a potential cure for Covid-19, But I was like meh; BUT I am pretty excited for this one which Oxford just released a statement for I think last night maybe.
The World Health Organisation also applauded the initial results of the study.
It is really interesting, the excerpt said that they are trying to publish the data as soon as possible which basically makes it a more trustworthy of a claim.
The study was an attempt to potentially use Dexamethosone (A long acting corticosteroid which can remain in the systemic circulation for as long as 3 days) as a DOC for the Covid19.
What are Steroids?
Steroids is a group of chemical compounds with extensive properties often used as a drug of choice for many life threatening diseases.
Some steroids ( Androgenic Steroids) are activated due to stress and leads to many anabolic processes inside your body for example "Muscle building", When you are like trying to get those gains so badly in the gym, what basically happens is you are stressing your muscular cells (also injuring) as a result of resistance training and then steroids are produced as a physiological response so that more and more protein is available for the muscle to repair (btw this is the reason why some bodybuilders using anabolic steroids, end up gaining exceptional gains over years of steroid use)
Some steroids (Glucocorticoids) can strongly suppress the immune system by either suppressing certain genes in various immune cells or by blocking the important enzyme activities. These steroids can act as Anti Inflammatory too which basically means these steroids counter any inflammatory response which can be physiological or pathological. This is the reason that if a steroid taken in the early phase of the Covid-19 disease (The mild symptomatic or Asymptomatic phase) can actually suppress the immunity to a certain point that the drug itself becomes counterproductive.
Some Steroids (Mineralocorticoids) maintain the mineral balance by salt retention, etc. Lets just skip this one.
Adrenal Gland produces Steroid. Them tiny glands you can see above the kidneys.
Now the immunity suppressing nature of Dexamethasone is also the reason why it cannot be taken as a mass prophylaxis drug, unless the patient is in a state of severe immune response to the infection and requires ventilation or ICU.
The exudate formed in the lungs become an overwhelming immune response to fighting the virus and becomes fatal by causing the patient to stay in respiratory distress and finally succumbing to death.
The Trials done by the Oxford University aka RECOVERY trials, said that :
"1 death would be prevented by treatment of around 8 ventilated patients"
or
"around 25 patients requiring oxygen alone as of now"
*The prognosis may potentially increase as with other combinations in the future*
The study is really interesting because the study population was relatively large ( around 11,500) ; The Cohort population was around 2100 and Control was 4300 which is really exciting.
How does Dexamethasone work against SARS - CoV2?
Dexamethasone is a long acting Corticosteroid and mostly suppress the genes of immune expression
This is the Mechanism of Action of the drug if you are interested:
Dexamethosone vs The Immune System :
The goal of this drug is to just deactivate the immune system which has gone kinda crazy over this virus.
The immune system (IS) basically starts acting like its IS and terrorizes the whole body like its Iraq or Syria.
Jokes aside, This drug can really do some great damage to the hyper super- immune response which is kind of self destructive as the disease progress. Let's try to understand HOW
Only Within 6 hours of single dose of Dexamethasone:
There is a decreased availabilty of lymphocytes, eosinophils, basophils, monocytes,
These cells start redistributing and becomes less available and inactive for almost a day or two.
Also there is a decreased adhesion of these cells to blood vessel walls due to Dexamethasone, Actually the drug is not letting these immune cells to cross the wall of the vessel and go to the infection site (which is kinda cool cuz' no immune response no problem right? seriously why didnt evolution think of this?)
SECONDLY < there is a > decreased phagocytotic capacity of the immune cells so that they do not eat up the virus and form further exudates.
Finally leading to the decrease in respiratory burst (It is the area inside a phagocyte where we burn the pathogen inside the phagolysosome usually, in the case of Covid19, later explodes and kills us, Dont worry the jokes' on evolution not us )
Now the first most remarkable thing Dexamethasone does is, that, it suppresses Macrophage activity.
Which is basically blocking the Arachidonic Acid Pathway, Prostaglandins, Leukotrienes, Interleukin 1, Interleukin 6 and TNF
Explaination :
IL-1 goes to the brain and causes fever and normally increases the production of steroids by stimulating the hypothalamus, but since we are giving Dexamethasone (which is a steroid) there's something called as a negative feedback and it decreases the natural physiological production of steroid, causing the person to be severely dependent on steroids; and if the person stops taking this steroid, he can eventually die due to acute adrenal insufficiency, thats the reason why we should always taper the dose when withdrawing a steroid.
Now,
The Interleukin 6 usually activates almost all other immune system actions (Remember that respiratory burst is also decreased and hence theres no signal from the MHC I and II to activate the immune system either) but when it is suppressed by Dexamethoasone, it cannot activate the immune response like it normally would.
The second most important thing is that Dexamethasone down stimulates the cooperation between naive T cells and Interleukins
In Covid 19, Macrophage connects with the Naive T cells and there is a co-stimulation and can be two pathways. (depending on which interleukin is available for the naive T cell)
The first pathway:
In presence of Interleukin 4, these Naive T cells convert into T helper -1 cells which further increases Interleukin 4 and Interleukin 5 by positive feedback mechanism.
Finally causing the other cells of cell- mediated immunity, the "B-cells" to become active and produce antibodies which bind with the virus antigen and try to repeatedly neutralise it. (and kills us).
The Dexamethasone can potentially end all this suffering by attacking a gene known as GATA3 on the T helper 1 cell, (Remember Steroids suppress some immune genes it is just one of them) and hence GATA3 is suppressed, and therefore the chain is broken and there is no immune response ( yay, we alive now)
The second pathway :
If the naive t cell has Interleukin 12 available instead of Interleukin 4, it becomes T helper 2 cell, which produces Interleukin 2, which activates Cytotoxic T cells which produces some naughty proteins called perforins and granzymes.
These Perforin causes perforations in the infected cell and granzymes are then injected to that infected cell which makes the cell kind of commit suicide I guess ?. (and it kills us)
Dexamethasone acts on the T-bet gene on the T helper 2 cell which suppresses the further activation of immune response ( and hey we back to life again)
Now, ALL this information which just went over all of our heads is just the immune suppression of steroids, Lets not go in details with the EXTENSIVE collection of what Dexamethasone can actually achieve.
Please note the trials were done with Dexamethasone and not other corticosteroids mainly because of its wide availability, inexpensive nature, and most importantly because it is along acting Corticosteroid despite being the most potent among them
Dexamethasone also decreases inflammation
Explaination :
Our Cell membranes have a phospholipid bilayer, which is converted by PLA2( Phospholipase A2 ) enzyme to Arachidonic Acid. a) Arachidonic Acid is acted on By COXs ( Cyclooxygenases) to release PGE2F2, PGI2, Thromboxin A2 b) Arachidonic acid can be converted to Leukotrienes by LOXs (Lipooxygenase)
Dexamethasone can block the PLA2 enzyme and COX2 and COX1, by producing Lipocortin 1, and therefore there's no formation of Arachidonic Acid in the first place, and the whole inflammatory system goes down. (Kudos to the structure of Dexamethasone)
Please, keep in mind that we do need the immune and inflammatory response in the early part of the disease but as their actions overwhelm the healthy effects of the process, steroids can be used. Not too early, because it can actually worsen the disease if steroids are administered too early.
Some Side Effects which are to be kept in mind :
1. Withdrawl :
- Underlying disease which we were treating may rebound even stronger than before - Acute Adrenal Insufficiency - Pseudotumor Cerebri - Myalgias - Arthralgias - Malaise
2. Hyper use of steroid for long period :
- Fluid and electrolyte abnormalities - HTN ( more sodium retention) - Hyperglycemia ( gluconeogenesis) - Increased infection susceptibility (suppressed immune system) - Behavioral disturbances - Striae (fat redistribution)
While this is a serious concern for us as Indians, people are already stocking up Dexamethasone, price is most likely to spike up and things actually somehow do not work perfectly in India. Let's hope we learn from our mistakes in the past and just get this done and over with. PS - I will try to post more articles like this if I find something interesting regarding the pandemic. Thank you for the time. :) Feel free to contact.
Source: Dexamethasone statement by WHO
https://www.who.int/news-room/detail/16-06-2020-who-welcomes-preliminary-results-about-dexamethasone-use-in-treating-critically-ill-covid-19-patients
Oxford Recovery Trial Statement
https://www.recoverytrial.net/files/recovery_dexamethasone_statement_160620_v2final.pdf
2 notes
·
View notes
Last Seen Blogs

itz-kumori
𝙆 𝙐 𝙈 𝙊 𝙍 𝙄

anbloo
manga

sparkskornum09-blog
Untitled

likurg-ever
Andrei Osipov

alwaysmelloweagle
Married💍. ♓️💞♍️