#schizophrenia spectrum and other psychotic disorders
Text
Even after I stopped being delusional, reality didn't feel real at first and I was confused for some time.
1 note
·
View note
Text
Shoutout to the mad, disabled, mentally ill, disordered, etc. whose only safe spaces are obscure online tags where ableists don’t care to know about and thus, cannot reach you
#pdnos#psychosis nos#neurospicy#actually psychotic#madpunk#mad pride#any other personality disorders out there#schizophrenic spectrum#schizophrenic pride#actually schizospec#schizospec#schizophrenia spectrum#mental health positivity#mental heath support#disability pride#seriouslyschizophrenia#schizoaffective#pwpd#actually did#actually osdd#actually dissociative#personality disorder not otherwise specified#npd safe#npd positivity#actually szpd#persodivergent
256 notes
·
View notes
Text
Solidarity between plurals and ANY person with schizophrenia & other schizospec disorders, psychotic disorders, delusional & hallucinatory experiences or disorders, etc. The recent hate is NOT representative of the wider plural community; WE STAND WITH YOU. Neurodiversity is a spectrum and nobody should be written off or used as degrading insults. We both don't deserve that. To the sanism of the world, we're all the same and they're keen to dismiss us based on their assumptions of us. We are in this together. WE WON'T BACK DOWN TO THIS!
Extra shoutout to the people above that are ALSO plural. The intertwining of how things work is something that only the person experiencing it will understand the most, and it's okay to be separately plural or for your neurodiversities to interact with each other.
We're ALLOWED to exist. We are NOT your punchline. We are NOT your insult. We are REAL and deserve to be treated that way. Let's make sure they don't forget it.
If anyone on the spectrums above see this, please feel free to reblog and add to this, since we're only coming at it from a plural side of things and we don't know much. We want to stand with you but your voices are most important.
#pluralgang#plural community#plurality#plural pride#neurodivergent#solidarity#mad pride#schizospec#delusional disorder#schizophrenia#psychosis#i dont know how to tag the other half of this#let us know if any good pride tags we missed exist#hallucinations#ask to tag
388 notes
·
View notes
Text
PSA
-OCD is not a synonym for neat or preoccupied with tidiness. Obsessive-Compulsive Disorder is all about distressing intrusive thoughts and rituals (compulsions) used to combat those thoughts.
-Intrusive thoughts are not synonymous with silly things I want to do. They're deeply upsetting, often taboo mental apparitions. Letting them win is the last thing anyone wants, and nobody is immoral for having them. (See 'impulsive thoughts' if you need a term.)
-Anorexic is not a synonym for thin or emaciated. The majority of anorexic people have OSFED atypical anorexia – that is, their BMI is above 18.5. You cannot judge the severity of someone's illness by their appearance. (If you're worried about someone, look out more for rapid weight loss than thinness, even when it's occurring in someone in a larger body. 10kg in 10 weeks is never a good thing.)
-Eating disorders are not synonymous with just anorexia and bulimia. Anorexia is an ED, but it's nowhere near the most common. Bulimia is an ED, but again, not the most common. Together, they do not constitute the most common. The most common ED is binge-eating disorder, and the second most common is atypical anorexia, which is one of many, many OSFED categories. Those living with ARFID, pica, night-eating syndrome, rumination disorder, subthreshold BN, subthreshold BED, and orthorexia all deserve dignity, compassion, and acknowledgement. Remember: EDs are not necessarily thin, and never glamorous.
-Schizophrenic is not a synonym of all over the place, abnormal, unpredictable, dangerous, or crazy. Nor is schizoid or schizotypal. Folks with schizophrenia spectrum disorders live with hallucinations, delusions, disorganised thoughts/behaviour, and/or catatonia. They are far more likely to be victims of violence than perpetrators, and go to huge lengths to act okay even when distressed by symptoms.
-Schizophrenic is also not a synonym of multiple personalities/volatile. For the disorder involving having different facets of personality that are generally unaware of each other, see Dissociative Identity Disorder, and even then, don't assume it's a) dramatic as it is in the movies; b) evil; or c) trivial. DID is a trauma disorder.
-Delusional is not a synonym of wrong. Nor is it the same as this politician/friend is saying something I do not like/that is potentially dangerous. Delusions are false, fixed beliefs held despite evidence. And generally, folks with delusions don't tend to proselytise them. I know that certain politicians have beliefs that seem to persist in the face of evidence, but nevertheless, we don't need to stigmatise mental illness further to call out poor political/social behaviour. If you need a word for the pundit spewing potentially dangerous content, use 'dangerous' or 'wrong', but don't call them delusional.
-Bipolar is not a synonym of all over the place or fluctuating results. Bipolar disorder involves mood states that, even in the rapid cycling form, tend to last at least 3-4 days (mania) and weeks (depression). If you need a word for the weather, use 'British' instead.
-Psychotic is not a synonym of evil. Psychosis is losing touch with reality, whether it be through hallucinations or delusions. It doesn't make a person bad or violent. It's just a neurological phenomenon that may be distressing. It's also relatively common: 6-15% of people will hallucinate in their lifetime.
-ADHD is not a synonym of just quirky/scattered/forgetful/unfocussed/lazy/careless. ADHD is fundamentally a disorder of being able to choose where to direct attention, rather than of just I can't focus. If someone can't tune out the noise of the crowd, but can't prevent themself focussing on something trivial because their brain is wired that way, it's not laziness or just being quirky/scattered.
-Autistic meltdown is not a synonym of temper tantrum.
-Borderline is not a synonym of harridan.
-Narcissist is not a synonym of abuser.
-Mentally ill is not a synonym of volatile or bad person. This doesn't mean we have to make something artificially positive out of mental disorders. If there is good to be found in certain disorders, great; if there is nothing positive about living with certain others, that doesn't make you any less real or resilient than anyone else. It's okay to have complex feelings about your own disorders. It's okay to feel exhausted or frustrated by a disorder. But never should anyone have to face stigma.
#vent post but also important#ocd#intrusive thoughts#eating disorders#eds#schziophrenia#delusions#bipolar disorder#bipolar#psychosis#adhd#bpd#npd#cluster b#mental illness discourse#i want to make this for a couple of reasons:#a) i have intrusive thoughts (and possibly inserted thoughts) and they're awful#b) i've had OSFED and seeing the AN = thin stereotype is... frustrating#c) so so many people live with the other disorders on this list and don't get help and support because of stereotypes#d) so long as stereotype persists the medical system will not acknowledge the needs of its patients#e) while i don't have the right to speak over anyone with any of these disorders i can at least try to start a conversation#those of you with the above disorders: feel free to correct me if i stuffed up a detail#nt people you may interact with this post#everyone: feel free to add more to the list
638 notes
·
View notes
Note
are there any bb!cats with schizophrenia or that regularly experience psychosis? people absolutely suck about mental illness so like. seeing characters like me going thru life and being treated like people and not monsters for something out of their control never fails to put a smile on my face! thank you for all the research and effort you put into making sure your disabled cats are not only believable but human. pd: cinderheart with bpd is an extremely based headcanon
Not yet but it's on my radar, plus NPD. The reason why I feel so unflappably confident with BPD is because I know and love people who have it, and I hate that I don't see any characters who are like them! So I feel like I'm really good at handling it, and knowing what's wanted in portrayals of it. It feels very personally important to me.
Pair that with the fact I write BB!Clans as canonically struggling with ableism and all these being so heavily stigmatized irl, I've gotta be REALLY careful with NPD and psychosis. I'm less connected to them so personally and I don't want to accidentally strike a nerve, you get me?
That said... I got an ask a while back that I'd been thinking about a lot, basically asking me about how Clan Culture would see psychosis in the first place. I've actually always been fascinated by how deeply schizophrenia is affected by the culture of the afflicted, so I've been idly thinking about that for a while without sharing those thoughts.
OH WAIT hangon let me explain some stuff about Schizophrenia and psychosis for people in the audience!!
Schizophrenia used to be diagnosed in subtypes before 2013.
This is no longer accurate! A lot like Autism, it's a spectrum of symptoms that affect people differently. It's a cognitive disorder that messes with rational and organized thinking, and that can express in all sorts of ways.
One of the symptoms is hallucinations.
It's The Famous symptom of it, but it's not actually something you NEED to have to be Schizophrenic. Not all people who are having hallucinations or delusions are Schizophrenic, either! I want to include an OCD character of some kind who experiences some mild auditory hallucinations, actually. The type where it's just random mumbling.
Delusions and hallucinations aren't the same thing
Delusions are false beliefs and hallucinations are false experiences. An example of a delusion is, "If I don't click my pen three times, my family will die." An example of a hallucination is hearing voices.
PEOPLE WITH PSYCHOSIS ARE FAR MORE LIKELY TO BE THE VICTIMS OF VIOLENCE THAN TO COMMIT IT
Feel like this is common knowledge in this space, and especially within my own following since I make a lot of art about mental illness and awareness, but it's always worth repeating.
So anyway
If you compare psychosis between cultures, you actually end up seeing VERY different expressions of the hallucinations. For example, in some cultures, voice hallucinations tend to say things that are negative or abusive, while other cultures hear significantly more positive, playful voices.
This doesn't mean that they're always less distressing. For example, the study above points out that Nigerian students (reported to hear lots of playful hallucinations) experience as much distress as Dutch students (tend to experience negative, abusive voices) during their psychotic episodes.
Still, there does seem to be a correlation with "less distress" and cultures that encourage psychotic people to see their hallucinations as positive, personal things. Even more interestingly, distress seems to be correlated with income and individualism in a culture.
But it doesn't stop there, the findings are fascinating.
Delusions of grandeur are rare in societies that discourage that sort of social mobility, reflecting social values.
Cultures that believe religious experiences are specific experiences-- like certain smells, temperatures, or sounds, will see those reflected in psychotic episodes
Yet, "voices" seem to be something seen across ALL cultures studied. Though some have more prevalence of random sounds and mumbling than others, they all share some expression of "voices that say stuff."
SO all that to say-- if I include psychosis it's definitely going to be trying to take the culture of each Clan into account, and I need to do a lot more research into what sorts of things people with schizophrenia and various types of psychosis want to see more often.
128 notes
·
View notes
Text
me: wow, tiktok, a platform that has millions of creators and has prided itself on its #EduTok educational video campaign. i wonder what i can find about psychology on here!
video 1: i did one unit of psychology in college, 8 years ago, so let me give you an expert’s opinion on this therapeutic technique. follow for more!
video 2: this is why having a personality disorder makes someone a terrible irredeemable person :) (PS armchair diagnosing is VALID)
video 3: omgg guys, TIL that liking vanilla milkshakes?!…. means you have adhd, autism, bpd, depression, anxiety & maladaptive daydreaming?? woww!!
video 4: adhd is for himbo boys, autism is for quiet girls <3
video 5: how to spot (and exorcise) evil psychotic people with schizophrenia and those other psychotic spectrum disorders idk the name of
video 6: [hypnotic spiral in background] your mom is a narcissist your mom is a narcissist your mom is a narcissist your m
video 7: hi everyone, today i’m dividing all the mental illnesses into the categories of "uwu quirky child" disorder, "evil scary abusive" disorder, and "idk what that is" disorder. these categories should be added to the DSM btw
video 8: i’m an actual psychologist and i just openly hate people with cluster b PDs
video 9: i’m an actual psychologist and im fucking begging you, leave this place while you can, yes i’m talking to you aardvaark, RUN RUN RUN RUN RUN RUN RUN RUN RUN R-
video 10: i made a new youtube tutorial on how to purposely develop this complex, chronic, debhilitating disorder :3 check out my acc!!
#pop psychology#mental health#misinformation#tiktok psychology#anti intellectualism#wren speaks#(to be clear i’m exaggerating but these are all based on very real videos and trends ive seen)#and yes videos like the 10th example do very much exist. i can’t imagine that they work lol but they do exist#tw ableism#tw sanism
57 notes
·
View notes
Text
Mods
[large text: Mods]
Sasza
[Large Text: Sasza]
Hi! My name is Sasza and I use he/him pronouns. I am a disabled artist who loves to write and draw characters like me! I am autistic, (mildly) intellectually disabled and have several physical conditions including-but-not-limited-to dyspraxia, severe hyperkyphosis, cranial nerve diseases (causing double vision, chronic pain and a facial difference among other things), and hypermobile joints. Sometimes I use a cane. I'm very passionate about accessibility and disability representation in all kinds of media - books, comics, video games, and any other kind of art that's out there!
Bert
[Large Text: Bert]
Hello! I'm Bert (previously Mason), and I use he/they pronouns. I am a writer who loves to write plays and fiction with characters like me and my friends. I am autistic and have ADHD, I have psychotic PTSD and a DID system. Physical health-wise I have migraines, fibromyalgia, and a lateral lisp. I love talking about representation and ways we can make a kinder and more inclusive space everywhere we go.
Sparrow
[large text: Sparrow]
Hi, I’m sparrow, they/he for me. I’m a disabled artist who makes a lot of disabled characters like myself and probably like a quarter of the world. I have autism and ADHD, among other brain things, as well as chronic pain in both my jaw and my knee and ankle. I also have POTS and some sort of sleep disorder. I am a sometimes cane user as well. I really enjoy research and thoughtful art that makes people feel seen. Aside from that, I am a huge fan of historical fiction and really enjoy fantasy as well.
Rot
[Large text: Rot]
My name is Rot, I use all pronouns including neo pronouns as well as any rot and insect themed nounself pronouns. I’m an artist who loves putting disability in my stories. I’m mostly undiagnosed due to medical neglect and have chronic fatigue, hypersomnia & chronic pain that ranges from mild to debilitating. My known disabilities are pots, ganglion cysts, nerve damage, tics, autism (level unknown), asthma, GERD, anxiety and psychosis. I have a metal implant, use a cane and am mostly verbal and use aac infrequently. I have experience with temporary palsy, needing carers (family members who stepped up, not hired carers) and being in a wheelchair, though I currently don't have any of those.
Patch
[Large text: Patch]
Hey! We’re The Patchwork Quilt but please call me Patch! I use sof/soft/softs, red/red/reds, they/them/their, and ae/aem/aeir pronouns. I’m autistic (level 1, the very high end of low support needs, unreliably/semi-speaking, AAC user), and I’m a system with highly complex dissociative identity disorder (we use we/us and I/me language interchangeably. Please don’t ask who’s fronting). I also have hypermobile Ehlers-Danlos syndrome, attention-deficit/hyperactivity disorder, specific learning disorder with impairment in mathematics (AKA dyscalculia), developmental coordination disorder (AKA dysgraphia/dyspraxia), chronic fatigue syndrome, essential (kinetic) tremor, avoidant restrictive food intake disorder, dependent personality disorder, severe auditory processing disorder, psychosis (likely somewhere on the schizophrenia spectrum), and Tourette’s syndrome. I use a rollater that can turn into a powerchair. I love drawing, writing, and playing D&D and coming up with creative ways to incorporate disability into those three things. I will be attending college for a degree in disability studies this fall.
Virus
[Large Text: Virus]
Hello! I go by Virus and I use She/Her but anyone can use any pronouns for me, have fun with it. I'm a writer—mostly fanfiction—who has been in fandom very long and used to be a classical musician. I have Hypermobile Ehler Danlos Syndrome along with it's fun co-morbidities (MCAS, POTS, Gastroparesis, Fibromyalgia, and Von Willebrandes). I also have Pan-Hypopituitarism which is the following: Adrenal Insufficiency, Hypothyroidism, Diabetes Insipidus, Precocious Puberty, Growth Hormone Deficiency, Hyperprolactinemia/galactorrhea, as well as High Estrogen and Testosterone issues. I have Pituitary Dwarfism/Proportional Dwarfism, Myoclonic Epilepsy, and a Speech Disorder. I used to have a Port-a-cath, Picc-Lines, and a feeding tube, amongst many other things. Phew, now that that's over. I love every art form with a favour towards music, writing and the fiber arts. I love seeing representation no matter how big or small especially in medias that rep is often glossed over!
Rock
[Large Text: Rock]
Hi! I am Rock; any pronouns are okay. I am a writer, mainly of sci-fi and fantasy, and I love adding all sorts of disabled characters. I am hard of hearing (mild-moderate bilateral hearing loss) and have profound auditory processing disorder. I have scoliosis, POTS, and lower-body muscle weakness so I am a full-time mobility aid user. I am also intersex; I have several hormone deficiencies among other conditions as a result of my intersex variation. I am excited to join the mod team!
Aaron
[Large Text: Aaron]
Hey, I'm Aaron, he/him. I'm a writer of fantasy, science fiction, dystopia, utopia, and historical, and I like writing incorporating casts of disabled characters into all of them and reworking magic, technology, and science to accommodate them. I have a TBI, a lot wrong with my speech, cognitive issues, slight developmental disability, myofascial pain syndrome, medium support needs autistic but fully verbal, OCD, multiple types of anxiety, PTSD, depression, severe ADHD, dyslexia, dysgraphia, articulatory initiation anomia, medically significant migraines, a chronic headache, chronic pain, and chronic fatigue. I'm also visibly disabled (one of those people who looks autistic) and transmasc. And I can't wait to see what amazing things you guys come u with.
#mod sasza#mod intros#cripplecharacters about#mod bert#mod sparrow#mod rot#mod patch#mod virus#mod golem#mod rock#long post#not writing advice#mod aaron
46 notes
·
View notes
Text
Well, since tumblr randomly ate my pinned... -_-
About us:
We're the Stars system, a massively polymultiple and polyfragmented mixed origin DID system. We consider ourselves an infinite system.
Our pronouns are fae/it unless specified otherwise. When referring to multiple of us, you are welcome to use fae&/it& or you& for clarity. If you are up for it, we would also appreciate second person neopronouns being tried out (substituting neos for 'you'), and sometimes we use first person neopronouns (substituting neos for 'I/we')
Some of our labels include (we use general/umbrella labels in places to indicate that we use many of those kind of labels):
(disability)
POTS
MCAS
likely ME/CFS
chronic pain (likely fibromyalgia)
other unspecified chronic illness symptoms
physically disabled with mobility disabilities
anxiety
PTSD and C-PTSD
DID w/strong dp/dr symptoms
schizophrenia/psychotic
cluster B spectrum disorder, comprehensive subtype (we meet the diagnostic criteria for all four cluster B disorders and our symptoms are heavily interrelated)
OCD
autism
ADHD
MADD
OLD (a medically unrecognized disorder)
neurodivergent and neurodisabled
cognitive disabilities
cripple
mad
often housebound, sometimes bedbound (less so now that we have a wheelchair)
low to mid masking
low to mid functioning
mid to high support needs
(system)
traumaendo mixed origin
infinite system
aside from traumagen and endo, spirigenic, schizogenic, bordergenic, paragenic, tulpagenic, and more
(queer)
Abro (and use lesbian, gay, queerhet, bi, pan, omni, and mspec and straight lesbian/gay labels)
transneufemmasc, transfluid
intersex
altersex/salmacian
pangenderfluid, kingender, xenogender, agender, maverique, intergender, multigender, androgyne, and others
faegender
butch and femboy
queer
demigrey aroace and grey apl among others
lesboy/turigirl
radinclus
(other)
alterhuman
otherkin (especially fae/changeling, but pankin across the whole system)
otherhearted
copinglink and linktypes
hearthome
choicekin
constelic
demihuman and nonhuman both
endel
humankin
flickers
hivemind
multiversal
reality shifters
nonperson
We are pro-endo and pro-tulpa, anti-psych and anti-phys, pro-mad-liberation and cripplepunk inclusionists and coined unitypunk. We are kff safe and do not believe ANY identity that someone genuinely identifies as, that is not specifically based on intentional harm to others, can be inherently or ontologically harmful. We are proship/profic and ourselves are survivors of a specific kind of SA that cannot be directly spoken about here. We are also anti-forced-recovery and don't believe in consensus reality.
We also do not believe it is okay to make fun of reality shifters just because it's the current acceptable target, and find it especially hypocritical coming from otherkin. Even if it was always harmful, the appropriate response would be genuine, non-patronizing concern, offering resources, and then backing the fuck off if people can't or won't "recover". That being said, most "anti" sentiment in this context is heavily sanist and centered around the idea of a "correct" consensus reality. Not trusting people to be right about their own subjective experiences is both sanist and just generally an asshole move.
We believe transandrophobia exists, that everyone can be affected by transmisogyny and that TMA/TME labels are reductive and often bioessentialist and intersexist in usage, and that exorsexism and the above are all serious issues both within the trans community and in society as a whole. We support transunity. We also are pro-complicated and conflicting labels, such as mspec lesbian/gay, straight lesbian/gay, transmasc lesbians, and lesgay/lesboy/turigirl labels.
We are transhumanist and support bodily autonomy and good faith identity with NO. EXCLUSIONS. If you think this doesn't apply to you, I promise it still probably actually does. We do our best to judge people on their actions, not their thoughts, feelings, or anything else that occurs internally. We also don't believe any body modifications or exercise of personal bodily autonomy is wrong.
We also believe it's not wrong to be unhealthy, to refuse or be unable to recover, and that healthism is ableism. Disabled people (including neurodivergent people) are the most reliable authority on their own experiences. Also, if someone says they were called a slur, you should believe them, and they have a right to reclaim it regardless of if you think they have the "right" identity (outside of perhaps racial/ethnic slurs, which I feel is not our place to comment on). Slur, label, and flag discourse is all bullshit cop behavior and y'all need to stop it.
There's probably more that we'll come back and add later, but for now, here's a new pinned.
65 notes
·
View notes
Text
The Psychology of Qi Rong (TW for cannibalism and mental health)

This is a review of Qi Rong's behaviour and symptoms in relation to this authors note. According to MXTX, if put into a modern day context, Qi Rong would be said to have bipolar disorder. In order to verify this statement, this post is dedicated to comparing actual symptoms of bipolar disorder and Qi Rong's behaviour from the novel in order to prove this statement true.
I would like to put out a disclaimer that I am not a licensed psychology practitioner, but a student who hasn't finished his degree yet. I am simply writing this because this authors note wouldn't leave my brain. Please don't expect total accuracy from this post, though I will try my best to ensure that there is no error on my part
I would also like everyone to note that the term bipolar itself, is used to describe a spectrum of disorders, and that simply regulating it to one term would be incorrect, and that treatment can vary depending on the disorder
Bipolar Disorder: History, Symptoms and Probable Causes
Bipolar disorder is characterized by chronically occurring episodes of mania or hypomania alternating with depression and is often misdiagnosed initially. Treatment involves pharmacotherapy and psychosocial interventions, but mood relapse and incomplete response occur, particularly with depression.
(I want everyone to m
The first recorded case of Bipolar Disorder as an illness was by Pierre Farlet in the mid-19th Century (1851-1854), who called it “folie circulaire” (circular madness). It was defined by manic and melancholic episodes separated by symptom-free intervals.
In
1854 Baillarger used the term "folie à double forme" to
describe cyclic (manic–melancholic) episodes (Pichot
1995; Ritti 1879).
There also seems to be a mention of bipolar disorder (Unsure of this, take with a bit of salt) in the book Eight Treatesies on the Nurturing of Life by Gao Lian (Different character from the Lian in Xie Lian); dating back to the Ming Dynasty (1591 {first publication()} [requires fact checking])
(Note: Records of treatment of mental disorders in Ancient China go all the way back to the Tang Dynasty. If you check wikipedia, there is the claim that it goes back to 1100 BCE, which I can't confirm [requires fact checking])
Criteria to be met before diagnosing someone with Bipolar I Disorder according to the DSM-5 are at least one manic episode. This may be preceded by and may be followed by hypomanic or major depressive episodes and the occurrence of the manic and major depressive episode(s) is not better explained by schizoaffective disorder, schizophreniform disorder, delusional disorder, or other specified or unspecified schizophrenia spectrum and other psychotic disorder
Manic episodes are characterised increased talkativeness, rapid speech, a decreased need for sleep, racing thoughts, distractibility, increase in goal-directed activity, and psychomotor agitation. Some other hallmarks of mania are an elevated or expansive mood, mood lability, impulsivity, irritability, and grandiosity (Can be remembered using the DIGFAST mnemonic)
Rapid cycling in bipolar disorder is defined as having at least 4 or more mood episodes in a 12-month period. These mood episodes may be manic, hypomanic, or depressive but must meet their full diagnostic and duration criteria. These episodes must be separated by periods of partial or full remission of at least 2 months or be separated by a switch to an episode of opposite polarities, such as mania or hypomania to major depressive episodes (Note: Switching from mania to hypomania or vice-versa would not qualify because they are not opposite polarity). Rapid cycling bipolar disorder patients have been found to be more resistant to pharmacotherapy.
Hypomania and mania can be distinguished by a certain feature- hypomania does not cause major deficits in social and occupational functioning. The duration of a manic episode is at least a week, while a hypomanic episode is about four days
Symptoms of a depressive episode include feeling very down/sad/anxious, slowed down or restless, trouble falling asleep, waking up too early, or sleeping too much, talking very slowly, feeling unable to find anything to say, or forgetting a lot, trouble concentrating or making decisions, unable to do even simple things, lack of interest in almost all activities, and feeling hopeless/worthless, or thinking about death or suicide
(Note: According to the DSM-5, major depressive and hypomanic episodes are common in bipolar I disorder but are not required for the diagnosis)
Bipolar II Disorder is defined by a pattern of depressive episodes and hypomanic episodes. The hypomanic episodes are less severe than the manic episodes in bipolar I disorder
And finally, cyclothymic disorder/cyclothymia is defined by recurring hypomanic and depressive symptoms that are not intense enough or do not last long enough to qualify as hypomanic or depressive episodes
Like in the case of most mental disorders, there is no known cause for disorders on the bipolar spectrum, however the most widelt agreed upon risk factors are brain structure and functioning (some studies show that the brains of people with bipolar disorder differ in certain ways from the brains of people who do not have bipolar disorder or any other mental disorder), and genetics (some research suggests that people with certain genes are more likely to develop bipolar disorder. Research also shows that people who have a parent or sibling with bipolar disorder have an increased chance of having the disorder themselves).
In relation to genetics, many genes are involved, and no one gene causes the disorder (Which, if the authors note is true, we can assume that one of his parents carried the genes for it, most probably his father).
青鬼戚容
Qi Rong needs no introduction or abstract (Because I don't have to submit this to a prof hehehe) to start with. He is iconic, and rightfully so. In order to try and analyse Qi Rong's behaviour, let us take a glance at his introductory (In this case, first physical) appearance.
In his first (physical) appearance Qi Rong talks shit about others, which isn't really notable in regards to this topic. Its like my Mother after the guests leave and she's finished playing social politics. Its nothing interesting, just the typical criteria for the average aunty.
But you know what is interesting? His lair.
He has a throne, a banquet hall style dining set up. The only things he needs is the cauldron to cook (human) meat. I don't remember any of his subordinates needing to eat, and considering all of the salted carrion he has hanging around; not to mention the fresh meat stores he keeps (Three hundred humans...three hundred), he doesn’t eat a good chunk of the humans brought to him immediately. Its all unnecessarily grandiose for a single person, (We know that he doesn’t invite any dinner guests over. If he did, they'd be the main course)
If you notice Qi Rongs behaviour a majority of the time fits the criteria for a manic episode. Its also probably why his schemes seem to fail most of the time. Note that there has to be a remission period of two months in the case of rapid cycling (Which I belive occurs in Qi Rongs case), so MXTX is right, in a way. Qi Rong would be diagnosed with a disorder on the bipolar spectrum, more specifically Bipolar I Disorder
(One may also assume that he had cyclothymia during his days as a prince, but I believe that its just a showcase of certain symptoms of Bipolar I Disorder from a young age. He always had it, but it didnt manifest much more visibly until later on in his life)
Now Lets Talk About Kuru
Kuru is an infectious, acquired, non-immunogenic, fatal neurodegenerative prion disease. It progresses rapidly with cerebellar and extrapyramidal signs and symptoms, with death occurring within one to two years of onset of symptoms. What causes Kuru? Cannibalism, or more specifically the consumption of the brain tissue.
The diesease originated and was confined to the Fore Tribe in the Eastern Highlands of Paupa New Guinea, where ritualistic cannibalism was practiced. Kuru is now extinct due to the outlawing of ritualistic cannibalism in the region.
(Note: There is a theory that cannibalism occurred due to famine, and that it was ratonalised by the Europeans who arrived their as a ritualistic practice. Colonisers have also used the excuse of cannibalism to colonise and kill indigenous populations)
What causes cannibalism? Usually, the two most predominantly ascribed motivations are hunger and hatred, and the occasional belief that eating human flesh is medicinal.
(This is a bit of a personal note from me, but from what I've heard, human flesh is not good for any living creatures health. In my hometown there are plenty of stories about animals going mad or dying after eating human flesh)
A point I want to make is that we do not know how Qi Rong died. Did he die from being eaten alive? Or did he pass from a neurodegenerative disease caused by consuming human flesh in order to survive? If its the latter, it could explain his behaviour.
Kuru is also known as the laughing disease, as patients exhibited sporadic uncontrollable laughter, due to being emotionally labile. Perhaps Qi Rong passed before the disease could reach the sedentary phase? Maybe he was killed before that. Symptoms of Kuru can take time to manifest completely, so I feel that this theory should not be discounted.
Reference(s)
https://www.ncbi.nlm.nih.gov/books/NBK559103/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3188776/
https://www.nimh.nih.gov/health/topics/bipolar-disorder
https://www.ncbi.nlm.nih.gov/books/NBK493168/
https://www.ncbi.nlm.nih.gov/books/NBK519712/table/ch3.t8/
https://web.archive.org/web/20070928103521/http://www.nmh.gov.tw/nmh_web/english_version/exhibition/exhibition_s0703.cfm
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2813703/
A note of gratitude for @toowolfdelusion for posting that authors note, otherwise this brainfart of mine would not exist
#qi rong#tw: cannibalism#tw: mental health#leafs lilting#or metaing in this case#now to move on to fun stuff that doesnt need me to think#like my qr gets reincarnated as wwx#because i thinks its hilarious#this is what im using my not yet achieved degree for#not complaining#its kindafun when its not for class#tgcf#tian guan ci fu#heaven official's blessing
20 notes
·
View notes
Text
Musings on Psychosis
I realize now that my vampire 'type was a product of a psychotic episode that lasted throughout 2023. That episode has ended and it's been strange having certain perspectives of myself wrenched away from me. For around a year I was, perhaps, an endel in the immediate sense, but I wouldn't venture to call myself that now. It's hard for me to define now what vampires are to me. My general fascination with them is still there, and I remember the identity, shifts, and species dysphoria I experienced acutely, but that sense of self is distant now. I'm torn on whether I consider "vampire" to be a part of myself now - I know I certainly don't with the same intensity that I felt in psychosis. For a year I identified myself with monsters, werewolves, villains, and various morbid topics, and coming out of that was a harsh experience. In some ways I am no longer the person I was prior to the episode, or the person (monster/beast) I was during. All the changes psychosis has put me through have been unsettling - having it warp and change my identity on a confusingly temporary basis has been chaotic and deeply overwhelming.
I see a lot of endels and other psychotic folk on here with presumably permanent identities and sometimes I wonder whether anyone else has had experiences like mine. Especially those with episodic conditions like my schizophrenia/schizoaffective, where severity of psychosis changes over time and there may be periods of remission. I'm medicated, now, but I don't know for sure that this will never happen again. That I will never "become" a vampire again, or become some other species my psychotic brain decides to latch on to. My identity is fluid, and only after years of confusion have I realized that this fluidity is the product of a schizo-spectrum disorder. Maybe next time my identity has a total overhaul I'll recognize it as a psychotic episode - or maybe I'll be in too deep to realize, again.
#endelity#endel#i dont know why im posting this#it feels scattered at best#guess i figured it would be nice to update about like...the biggest thing to happen in my life in the past year#this is SUPPOSED to be my designated alterhuman blog but i so rarely post content on here these days#too little spoons...#using the endel tag in hopes of finding community i guess#i do feel very alone in this#blue speaks#blue's psychotic episodeTM
22 notes
·
View notes
Text
Hey cynical and disabled folks, how can I support my fellow community members without shoving positivity in your face?
I want to support you without pushing my beliefs and my worldview onto you.
I know that what helps me may not help others, so I want to ask: how can I better support my fellow disabled folk?
#actually psychotic#mental health positivity#mental heath support#actually schizospec#disability pride#schizophrenic spectrum#schizospec#seriouslyschizophrenia#mad pride#pwpd#schizoaffective#actually ocpd#any other personality disorders out there#not positivity#neurospicy#pdnos#schizo spectrum#ptsdwarrior#schizophrenia spectrum#schizophrenic pride#ocdawareness#autism acceptance#actually disordered#actually disabled#questions and feedback#q&f
11 notes
·
View notes
Text
Diagnostic Criteria Examples Masterpost
This is a series of posts that I'm hoping eventually covers all the disorders in the DSM-5-TR.
**This will be periodically updated as more posts are made. Please come back to the original post to see these updates**
NEURODEVELOPMENTAL DISORDERS
Intellectual Developmental Disorder (Intellectual Disability)
Global Develolmental Delay
Unspecified Intellectual Developmental Disorder (Intellectual Disability)
Language Disorder
Speech Sound Disorder
Childhood-Onset Fluency Disorder (Stuttering)
Social (Pragmatic) Communication Disorder
Unspecified Communication Disorder
Autism Spectrum Disorder (Levels System)
Attention-Deficit/Hyperactivity Disorder
Other Specified Attention-Deficit/Hyperactivity Disorder
Unspecified Attention-Deficit/Hyperactivity Disorder
Specific Learning Disorder
Developmental Coordination Disorder
Stereotypic Movement Disorder
Tourette's Disorder [Tourette Syndrome]
Persistent (Chronic) Motor or Vocal Tic Disorder
Provisional Tic Disorder
Other Specified Tic Disorder
Unspecified Tic Disorder
Other Specified Neurodevelopmental Disorder
Unspecified Neurodevelopmental Disorder
SCHIZOPHRENIA SPECTRUM AND OTHER PSYCHOTIC DISORDERS
Delusional Disorder
Brief Psychotic Disorder
Schizophreniform Disorder
Schizophrenia
Schizoaffective Disorder
Substance/Medication-Induced Psychotic Disorder
Psychotic Disorder Due to Another Medical Condition
Catatonia Associated With Another Mental Disorder (Catatonia Specifier)
Catatonic Disorder Due to Another Medical Condition
Unspecified Catatonia
Other Specified Schizophrenia Spectrum and Other Psychotic Disorder
Unspecified Schizophrenia Spectrum and Other Psychotic Disorder
BIPOLAR AND RELATED DISORDERS
Bipolar I Disorder [Includes criteria for manic episodes and major depressive episodes]
Bipolar II Disorder [Includes criteria for hypomanic episodes and major depressive episodes]
Cyclothymic Disorder
Substance/Medication-Induced Bipolar and Related Disorder
Bipolar and Related Disorder Due to Another Medical Condition
Other Specified Bipolar and Related Disorder
Unspecified Bipolar and Related Disorder
Unspecified Mood Disorder
Specifiers for Bipolar and Related Disorders
DEPRESSIVE DISORDERS
Disruptive Mood Dysregulation Disorder
Major Depressive Disorder
Persistent Depressive Disorder
Premenstrual Dysphoric Disorder
Substance/Medication-Induced Depressive Disorder
Depressive Disorder Due to Another Medical Condition
Other Specified Depressive Disorder
Unspecified Depressive Disorder
Specifiers for Depressive Disorders
ANXIETY DISORDERS
Separation Anxiety Disorder
Selective Mutism
Specific Phobia
Social Anxiety Disorder
Panic Disorder
Panic Attack Specifier
Agoraphobia
Generalized Anxiety Disorder
Substance/Medication-Induced Anxiety Disorder
Anxiety Disorder Due to Another Medical Condition
Other Specified Anxiety Disorder
Unspecified Anxiety Disorder
OBSESSIVE-COMPULSIVE AND RELATED DISORDERS
Obsessive-Compulsive Disorder
Body Dysmorphic Disorder
Hoarding Disorder
Trichotillomania (Hair-Pulling Disorder)
Excoriation (Skin-Picking) Disorder [Also called Dermatillomania]
Substance/Medication-Induced Obsessive-Compulsive and Related Disorder
Obsessive-Compulsive and Related Disorder Due to Another Medical Condition
Other Specified Obsessive-Compulsive and Related Disorder
Unspecified Obsessive-Compulsive and Related Disorder
TRAUMA- AND STRESSOR-RELATED DISORDERS
Reactive Attachment Disorder
Disinhibited Social Engagement Disorder
Posttraumatic Stress Disorder
Acute Stress Disorder
Adjustment Disorders
Prolonged Grief Disorder
Other Specified Trauma- and Stressor-Related Disorder
Unspecified Trauma- and Stressor-Related Disorder
DISSOCIATIVE DISORDERS
Dissociative Identity Disorder
Dissociative Amnesia
Depersonalization/Derealization Disorder
Other Specified Dissociative Disorder
Unspecified Dissociative Disorder
SOMATIC SYMPTOM AND RELATED DISORDERS
Somatic Symptom Disorder
Illness Anxiety Disorder [Hypochondria]
Functional Neurological Symptom Disorder (Conversion Disorder)
Psychological Factors Affecting Other Medical Conditions
Factitious Disorder Imposed on Self
Factitious Disorder Imposed on Another
Other Specified Somatic Symptom and Related Disorder
Unspecified Somatic Symptom and Related Disorder
FEEDING AND EATING DISORDERS
Pica
Rumination Disorder
Avoidant/Restrictive Food Intake Disorder
Anorexia Nervosa
Bulimia Nervosa
Binge-Eating Disorder
Other Specified Feeding or Eating Disorder
Unspecified Feeding or Eating Disorder
ELIMINATION DISORDERS
Enuresis
Encopresis
Other Specified Elimination Disorder
Unspecified Elimination Disorder
SLEEP-WAKE DISORDERS
Insomnia Disorder
Hypersomnolence Disorder
Narcolepsy
Obstructive Sleep Apnea Hypopnea
Central Sleep Apnea
Sleep-Related Hypoventilation
Circadian Rhythm Sleep-Wake Disorders
Non-Rapid Eye Movement Sleep Arousal Disorders [Sleepwalking and Sleep/Night Terrors]
Nightmare Disorder
Rapid Eye Movement Sleep Behavior Disorder
Restless Legs Syndrome
Substance/Medication-Induced Sleep Disorder
Other Specified Insomnia Disorder
Unspecified Insomnia Disorder
Other Specified Hypersomnolence Disorder
Unspecified Hypersomnolence Disorder
Other Specified Sleep-Wake Disorder
Unspecified Sleep-Wake Disorder
SEXUAL DYSFUNCTIONS
Delayed Ejaculation
Erectile Disorder [Erectile Dysfunction]
Female Orgasmic Disorder
Female Sexual Interest/Arousal Disorder
Genito-Pelvic Pain/Penetration Disorder
Male Hypoactive Sexual Desire Disorder
Premature (Early) Ejaculation
Substance/Medication-Induced Sexual Dysfunction
Other Specified Sexual Dysfunction
Unspecified Sexual Dysfunction
GENDER DYSPHORIA
Gender Dysphoria
Other Specified Gender Dysphoria
Unspecified Gender Dysphoria
DISRUPTIVE, IMPULSE-CONTROL, AND CONDUCT DISORDERS
Oppositional Defiant Disorder
Intermittent Explosive Disorder
Conduct Disorder
Pyromania
Kleptomania
Other Specified Disruptive, Impulse-Control, and Conduct Disorder
Unspecified Disruptive, Impulse-Control, and Conduct Disorder
SUBSTANCE-RELATED AND ADDICTIVE DISORDERS
Alcohol Use Disorder
Alcohol Intoxication
Alcohol Withdrawal
Unspecified Alcohol-Related Disorder
Caffeine Intoxication
Caffeine Withdrawal
Unspecified Caffeine-Related Disorder
Cannabis Use Disorder
Cannabis Intoxication
Cannabis Withdrawal
Unspecified Cannabis-Related Disorder
Phencyclidine Use Disorder
Other Hallucinogen Use Disorder
Phencyclidine Intoxication
Other Hallucination Intoxication
Hallucinogen Persisting Perception Disorder
Unspecified Phencyclidine-Related Disorder
Unspecified Hallucinogen-Related Disorder
Inhalant Use Disorder
Inhalant Intoxication
Unspecified Inhalant-Related Disorder
Opioid Use Disorder
Opioid Intoxication
Opioid Withdrawal
Unspecified Opioid-Related Disorder
Sedative, Hypnotic, or Anxiolytic Use Disorder
Sedative, Hypnotic, or Anxiolytic Intoxication
Sedative, Hypnotic, or Anxiolytic Withdrawal
Unspecified Sedative-, Hypnotic-, or Anxiolytic-Related Disorder
Stimulant Use Disorder
Stimulant Intoxication
Stimulant Withdrawal
Unspecified Stimulant-Related Disorder
Tobacco Use Disorder
Tobacco Withdrawal
Unspecified Tobacco-Related Disorder
Other (or Unknown) Substance Use Disorder
Other (or Unknown) Substance Intoxication
Other (or Unknown) Substance Withdrawal
Unspecified Other (or Unknown) Substance-Related Disorder
Gambling Disorder
NEUROCOGNITIVE DISORDERS
Delirium
Other Specified Delirium
Unspecified Delirium
Major Neurocognitive Disorder
Minor Neurocognitive Disorder
Major or Mild Neurocognitive Disorder Due to Alzheimer's Disease
Mild or Major Frontotemporal Neurocognitive Disorder
Mild or Major Neurocognitive Disorder With Lewy Bodies
Major or Mild Vascular Neurocognitive Disorder
Major or Mild Neurocognitive Disorder Due to Traumatic Brain Injury
Substance/Medication-Induced Major or Mild Neurocognitive Disorder
Major or Mild Neurocognitive Disorder Due to HIV Infection
Major or Mild Neurocognitive Disorder Due to Prion Disease
Major or Mild Neurocognitive Disorder Due to Parkinson's Disease
Major or Mild Neurocognitive Disorder Due to Huntington's Disease
Major or Mild Neurocognitive Disorder Due to Another Medical Condition
Major or Mild Neurocognitive Disorder Due to Multiple Etiologies
Unspecified Neurocognitive Disorder
PERSONALITY DISORDERS
General Personality Disorder
Paranoid Personality Disorder
Schizoid Personality Disorder
Schizotypal Personality Disorder
Antisocial Personality Disorder
Borderline Personality Disorder
Histrionic Personality Disorder
Narcissistic Personality Disorder
Avoidant Personality Disorder
Dependent Personality Disorder
Obsessive-Compulsive Personality Disorder [Anankastic Personality Disorder]
Personality Change Due to Another Medical Condition
Other Specified Personality Disorder
Unspecified Personality Disorder
PARAPHILIC DISORDERS
Voyeuristic Disorder
Exhibitionistic Disorder
Frotteuristic Disorder
Sexual Masochism Disorder
Sexual Sadism Disorder
Pedophilic Disorder
Fetishistic Disorder
Transvestic Disorder
Other Specified Paraphilic Disorder
Unspecified Paraphilic Disorder
OTHER MENTAL DISORDERS AND ADDITIONAL CODES
Other Specified Mental Disorder Due to Another Medical Condition
Unspecified Mental Disorder Due to Another Medical Condition
Other Specified Mental Disorder
Unspecified Mental Disorder
MEDICATION-INDUCED MOVEMENT DISORDERS AND OTHER ADVERSE EFFECTS OF MEDICATION
Medication-Induced Parkinsonism
Neuroleptic Malignant Syndrome
Medication-Induced Acute Dystonia
Medication-Induced Acute Akathisia
Tardive Dyskinesia
Tardive Dystonia [and] Tardive Akathisia
Medication-Induced Postural Tremor
Other Medication-Induced Movement Disorder
Antidepressant Discontinuation Syndrome
Other Adverse Effect of Medication
64 notes
·
View notes
Text
throwback to my AP psych class in highschool where my teacher always said "im a little bit ocd" and our first assignment was to "study" a student from another class and then make assumptions about their life based on their behavoir, then he taught us The Four Types of Schizophrenia and he said "no one knows why catatonic schizophrenics are like that no one knows whats going on in their brain" and then we watched a video of someone publically having a psychotic episode, and then we watched the movies Stand By Me and The Breakfast Club and had to write a paper where we diagnosed each character with a different mental illness
now lemme tell you why all of that was complete bullshit:
you cant be "a little bit ocd" (he said cause he liked things organized was why) because its a mental disorder characterized by obsessions and compulsions, simply being tidy doesnt make you a little ocd, either you have the disorder or you dont
i felt so creepy having to watch and write about a student i didnt know in another class, this is just such a weird thing to do, and not anything a psych profesional would actually do so i have no idea why we did it, and then for the rest of my time at school i was paranoid that someone was studying me which as an undiagnosed schizophrenic was horrible for me
the four types of schizophrenia is outdated, it was when i was in the class, its now known to be a spectrum where people can have mulitple or even all of the symptoms of the four types
yes you can easily find out whats going through a catatonic persons brain if you just ask (once they are no longer catatonic), ive been catatonic multiple times and ill tell you any day
do not watch videos of people publically having a psychotic episode, they didnt consent to filming or uploading the video, they probably didnt want one of their most terrifying and emberassing moments posted publically so a room full of teenagers could gauk at it, it is extremley disrespectful to the person in the video and their humanity is more important than any education you could bring on by the video
you cant diagnose people you dont know, even with the proper training, an hour worth of content is not enough to make a diagnosis from, i seriously dont know why we were encouraged to diagnose anyone, especially characters in a movie, i dont know what we learned from this other than thinking we had the power to diagnose people we didnt know
this was an AP psych class so that means it was college level, i hope this isnt what theyre teaching in college and i just had a particularly uneducated teacher
#schizophrenia#ocd#catatonia#catatonic#psych#ap psych#psych class#neurodivergent#mental illness#actuallyschizophrenic#mental health awareness
189 notes
·
View notes
Text
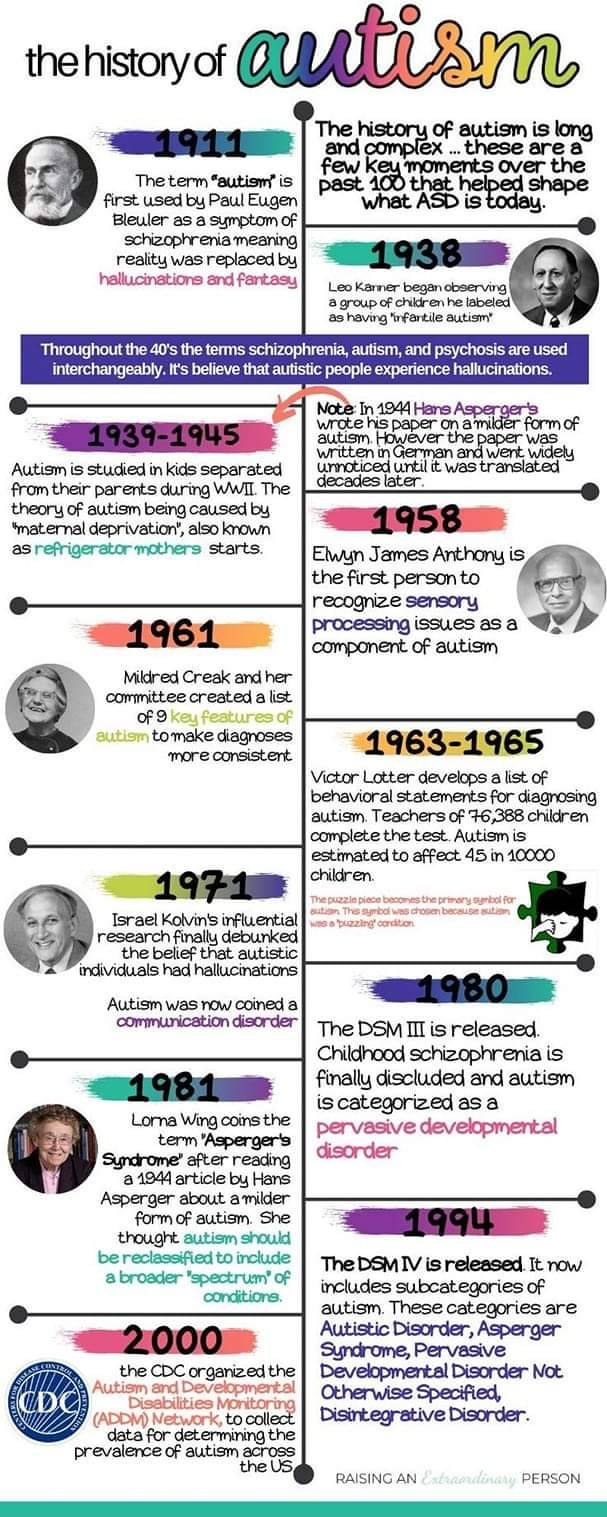
History of Autism
The term autism first was used by psychiatrist Eugen Bleuler in 1908. He used it to describe a schizophrenic patient who had withdrawn into his own world.
Eugen Bleuler coined the word "autism" in 1908 among severely withdrawn schizophrenic patients.
In 1943 Leo Kanner studied 11 children. The children had difficulties in social situations, adapting to changes in routines, good memory, sensitivity to sound, allergies to food, good intellectual potential, echolalia, and difficulties in spontaneous activity.
In 1944 Hans Asperger, who was a German Nazi, sorted autistic individuals into two categories. He studied one group and had the other group killed. The children he studied were considered "high functioning" and spoke like grownups. He also said that many of the children were clumsy.
In 1952 autism is added to the DSM as a psychiatric disorders diagnosed by a profound emotional disturbance that does not affect cognition and many people with schizophrenia were misdiagnosed.
Bruno Bettelheim studied the effect of three therapy sessions with children who he called autistic. He claimed that the problem in the children was due to coldness of their mothers. He separated the children from their parents. Kanner and Bettelheim both worked towards making hypothesis that showed autistic children had frigid mothers. This is where the term refrigerator mother came from.
Bernard Rimland was a psychologist and parent of a child with autism. He disagreed with Bettelheim. He did not agree that the cause of his son’s autism was due to either his or his wife’s parenting skills.
Autism came to be better known in the 1970’s. The Erica Foundation started education and therapy for psychotic children in the beginning of the 80s. Many parents still confused autism with mental retardation and psychosis.
In 1980 autism was changed in the DSM to be a pervasive developmental disorder seperate from childhood schizophrenia. It defined autism: a lack of interest in people, severe impairments in communication and bizarre responses to the environment, all developing in the first 30 months of life.
It was in 1980’s that Asperger’s work was translated to English and published and came into knowledge. Lorna Wing read it and coinsd the term Asperger's.
In the 1980’s that research on autism gained more traction and it was believed that parenting had no role in someone being Autistic and that there were neurological disturbances and other genetic ailments as the cause.
In 1987 the DSM divided autism into categories based on functioning labels. PPD NOS was used to describe those considered high functioning and autism for those considered low functioning.
Lorna Wing, along with Christopher Gillberg at BNK in Sweden in the 1980’s found the Wing’s triad of disturbed mutual contact, disturbed mutual communication and limited imagination.
In the 1994 the DSM is changed to include Asperger's. With PPD NOS as high functioning, Asperger's in the middle, and Autism for low functioning.
Them Ivar Lovaas studied and furthered behavioural analysis and treatment of children with autism. He developed it to target younger children (less than 5 years of age) and implemented treatment at home and increased the intensity to about 40 hours weekly. This therapy was ABA. This therapy was also modified and used as conversation therapy.
In 2013 the DSM removes Asperger's and PPD NOS and autism is now classified a social communication disorder.
In 2018 the DSM classified Autism as autism spectrum disorder and makes a distinction between autism with and without intellectual disability, and highlights the fact that older individuals and women sometimes mask their autism traits.


#autistic#autistic pride#autism acceptance#autism#audhd#actually audhd#autism acceptence month#asd#autistic adult
13 notes
·
View notes
Text
I’m gonna say it: internet pop psychology can’t tell the difference between neurotypical woo woo pseudoscience dumdums going “but what if psychosis is ACTUALLY seeing another dimension??” and stable, informed individuals with schizophrenia spectrum disorders or other psychotic conditions who are safely managing their symptoms discussing the religious and spiritual aspects of psychosis, which had traditionally been an accepted cultural concept (it was understood that psychotic and/or neurodivergent people couldn’t do traditional jobs but often had relevant insights and knowledge) until the Age of Enlightenment when it was decided that “madness” and “reason” were opposing forces
it’s already a thing in the mental health world that otherwise lucid psychotic people can benefit from discussing their experiences of reality in an open and non-judgemental setting, and organizations like the Hearing Voices Network aim to help people do that
suppressing discussion of unreality and altered reality in an effort to contain some kind of memetic contagion only silences marginalized voices and isolates already alienated people
#just make sure to tag religiously and you’re good imho#psychosis#actually schizophrenic#schizo spectrum#mad pride#cw delusions#cw psychosis
8 notes
·
View notes
Text
Non-schizos talk about the schizophrenia & other psychotic spectrum disorders like they’re on r/creepypasta
39 notes
·
View notes
Last Seen Blogs

channydraws
Marcillecore

rebalaccess
Rebalaccess

mothzilla-aka-mozzy
Princess Of The Monsters

pax34
fanfic 100

anna99blog
Eyes of the Dragon