#in addition to the medical bias it's like
Text
.
#a post rly triggered my internalized fatphobia and i am not feeling great about myself rn#like i genuinely believe i look good but im very much aware that the majority of the world does not hold this opinion or they think im#attractive but with an addition like they're cute but fat they'd be hot if they lost weight#and it's like ik professionally it would be advantageous to be thinner for that#in addition to the medical bias it's like#yeah no there are real tangible reasons to lose weight but fucking christ I SHOULDNT HAVE TO#i'm not unable to do the things i care about bcuz of my weight#i like how i look#weight is not an indicator of anything but weight#so it's like why should i have to do something proven to be unhealthy dangerous and unlikely to work long term without surgery#like it's bullshit#it's garbage#it makes me feel bad#fatphobia tw
6 notes
·
View notes
Text
Disabled POC face a unique combination of racism+ableism in reaction to their disability.
I’m more likely to get the cops called on me for bringing my service dog into a shop than a white person with a service dog.
I’m often labeled aggressive and violent when advocating for myself, while white people are more likely to be dismissed as a frustration or a nuisance.
Disabled people of color are more likely to be viewed as a threat whereas white disabled people are more likely to be viewed as weak and pitiful.
While all disabled people, regardless of race, are going to face medical neglect/mistreatment, disabled POC will face additional neglect due to racial bias in healthcare.
In fact, POC are more likely to *become* disabled due to medical negligence than a white person.
My experiences with ableism are largely impacted by race in a way that white disabled people don’t face when experiencing ableism.

[Image ID: White text in a Galaxy background reads If you: Derail my posts; are an “aspie”; run a sh/ed blog; are under 16; are a TERF; think cripplepunk is for mental disabilities; think that autism isn’t a disorder; are pro-transabled, trace, transage, etc; are pro-map or pro-zoo; are a transmed; want to completely demedicalize autism, I will probably block or mock you. End ID]
#disabled#disability#chronic illness#chronic pain#hypermobility spectrum disorder#chronically ill#hypermobility#mobility aid#cripple punk#cane user#cpunk#POC#disabled poc
3K notes
·
View notes
Note
do you feel like SSRIs are mostly pseudoscience? I'm not sure if I should be open to trying them or avoid them at all costs since I'm not sure if they even work or if they will mess me up permanently
a preliminary note that i don't find the category 'pseudoscience' to be useful & would classify SSRI research more as 'methodologically shoddy science' or 'ideologically slanted' or 'part of a centuries-long effort on the part of psychiatrists to secure themselves professional prestige by claiming neurobiological etiologies where none are shown to exist' &c &c. imo the notion of 'pseudoscience' is itself pretty positivistic, ahistorical, and ideologically noxious (particularly apparent in any analysis of epistemological imperialism).
that aside: you raise two major issues with SSRIs, namely whether they work and whether they will cause you harm.
efficacy of SSRIs is contested. a 2010 meta-analysis found that in patients with mild or moderate depressive symptoms, the efficacy of SSRIs "may be minimal or nonexistent", whilst "for patients with very severe depression, the benefit of medications over placebo is substantial". a 2008 meta-analysis found a similar distinction between mildly vs severely depressed patients, but noted that even in the latter population, drug–placebo differences were "relatively small" and argued that the differences between drug and placebo in severely depressed patients "seems to result from a poorer response to placebo amongst more depressed patients" rather than from a greater efficacy of SSRIs. a 2012 meta-analysis found some SSRIs consistently effective over placebo treatments, but several authors disclosed major relationships with pharmaceutical companies. a 2017 meta-analysis concluded that "SSRIs might have statistically significant effects on depressive symptoms, but all trials were at high risk of bias and the clinical significance seems questionable" (emphasis added) and that "potential small beneficial effects seem to be outweighed by harmful effects".
when evaluating any of this evidence, it is crucial to keep in mind that studies on antidepressant trials are selectively published—that is, they are less likely to be published if they show negative results!
A total of 37 studies viewed by the FDA as having positive results were published; 1 study viewed as positive was not published. Studies viewed by the FDA as having negative or questionable results were, with 3 exceptions, either not published (22 studies) or published in a way that, in our opinion, conveyed a positive outcome (11 studies). According to the published literature, it appeared that 94% of the trials conducted were positive. By contrast, the FDA analysis showed that 51% were positive.
meta-analyses are not immune to this issue, either. in addition to the problem that a meta-analysis of a bunch of bad studies cannot magically 'cancel out' the effects of poor study design, the authors of meta-analyses can and do also have financial interests and ties to pharmaceutical companies, and this affects their results just as it does the results of the studies they are studying. according to a 2016 analysis of antidepressant meta-analyses,
Fifty-four meta-analyses (29%) had authors who were employees of the assessed drug manufacturer, and 147 (79%) had some industry link (sponsorship or authors who were industry employees and/or had conflicts of interest). Only 58 meta-analyses (31%) had negative statements in the concluding statement of the abstract. Meta-analyses including an author who were employees of the manufacturer of the assessed drug were 22-fold less likely to have negative statements about the drug than other meta-analyses [1/54 (2%) vs. 57/131 (44%); P < 0.001].
[...]
There is a massive production of meta-analyses of antidepressants for depression authored by or linked to the industry, and they almost never report any caveats about antidepressants in their abstracts. Our findings add a note of caution for meta-analyses with ties to the manufacturers of the assessed products.
so, do SSRIs work? they are certainly psychoactive substances, which is to say, they do something. whether that something reduces depressive symptoms is simply not known at this point, though it is always worth keeping in mind that the 'chemical imbalance' narrative of SSRIs (the idea that they work by 'curing' a 'serotonin deficiency' in the brain) has always been a profitable myth. look, any medical treatment throughout history has been vouched for by SOME patients who report that it helped them—no matter how wacky it sounds or how little evidence there was to support it. this can be for a lot of reasons: placebo effect, the remedy accidentally treating a different problem than it was intended for, the symptoms coincidentally resolving on their own. sometimes the human body is just weird and unpredictable. sometimes remedies work. i'm sorry i can't give you a more definitive answer about whether SSRIs would help you.
as to potential risks: these are significant. SSRIs can precipitate suicidal ideation, a risk that has been consistently downplayed by pharmaceutical companies and studies. SSRIs are also known to contribute to sexual dysfunction and dissatisfaction, again a risk that is minimised and downplayed in much of the literature and in physician communication with patients. further (known) side effects range through emotional blunting, glaucoma, QT interval prolongation, abnormal bleeding & interaction with anti-coagulents, platelet dysfunction, decreases in bone mineral density leading to increased risk of osteopenia and osteoporosis, jaw clenching / TMJ pain, risk of serotonin syndrome when used in conjunction with other serotonergic substances, dizziness, insomnia, headaches, the list goes on.
i don't mean to sound alarmist; all drugs have side effects, some of the ones above occur rarely, and you may very well decide the risk is acceptable to you to take on. i would, though, always encourage you to do thorough research into potential side effects before starting any drug, including an SSRI. more on SSRI side effects in david healy's books 'pharmageddon', 'let them eat prozac', 'the antidepressant era', and 'the creation of psychopharmacology'; 'pillaged' by ronald w maris; and 'the myth of the chemical cure' by joanna moncrieff.
in addition to the above, SSRIs are known to come with a risk of 'discontinuation syndrome'—that is, chemical withdrawal when stopping the drug. this, too, is often downplayed by physicians; many still deny that it can even happen. some patients don't experience it at all, though i can tell you purely anecdotally that SSRI withdrawal was so miserable for me i simply gave up on quitting for over a year, despite the fact that at that point i was already thoroughly experienced with chemical withdrawals from other, 'harder' drugs. again, i am not telling you not to go on SSRIs if you decide these risks are worth it to you! i simply think this is a decision that should always be made with full knowledge (indeed, this is a core, though routinely violated, principle of medical 'informed consent').
ultimately this is not a decision anyone should make for you; it's your body and mind that are at stake here. as always i think that anyone considering any kind of medical treatment should have full knowledge about it and should be making all decisions freely and autonomously. i am genuinely not pushing any agenda 'for' or 'against' SSRIs, only against prescription of them that is done carelessly, coercively, or without fully informing patients of what risks they're taking on and what benefits they can hope to see.
439 notes
·
View notes
Text
so many words about historical men's corsetry
(This got way too long to send via Discord -- Dangimace in the Renegade Bindery server asked about men's corset sewing/resource recs so here is my half-assed and non-exhaustive rundown. Most of my historical sewing is focused on fashions of the UK, US, and Europe for the second half of the 18th century and first half of the 19th century, so that bias is reflected here; also disclaimer overall that "menswear"/"womenswear" are socially constructed categories and real people's bodies have always looked a wider variety of ways than fashion and other social forces would dictate. I sew historical garments with enthusiastic disregard for the historical gender binary and I'm barrel-chested, thick-waisted, and narrow-hipped no matter what I'm wearing.)
Onward, lads!
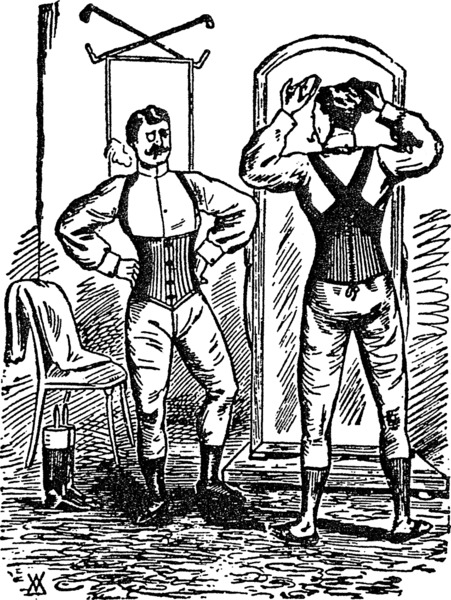
Ok wrt men's corsetry: there's a whole lot of fogginess around how historical men's corsets were constructed for a bunch of annoying reasons but that means there's lots of possibilities to explore in pattern drafting and project planning. Stays and other stiffened body-shaping garments have a whole complex conceptual relationship to the body basically as soon as they start appearing. 16th and 17th century garments do a whole lot of shaping (both compressing and building up) for men and women alike, but things really kick off in the 18th century in terms of the symbolic weight placed on stays and (later) corsets. Whole lot of stuff about gender, social class, race, fatness, morality, etc. getting projected onto these garments. So I'm a little leery about people taking obviously satirical illustrations of fashion-victim dandies or Gross Corpulent Libertines getting laced into corsets as truthful and indicative of the way men were really dressing -- scurrilous gossip and exaggeration are both a pain to sift through if we want to know which men wore corsets, what kind, and why.
In the very late 18th/early 19th century corsets were part of the repertoire for achieving highly fashionable shapes in menswear. (Along with a whole lot of padding.) They weren't mandatory for all dudes, but for fashion-forward dandies and equally fashion-forward military men, male corsets/stays were definitely a thing. The whole Romantic-era pigeon-breasted, narrow-waisted silhouette can be emulated by shapewear worn beneath the clothes, pads in the garments themselves, or both; in addition to waist reduction it helped to maintain smooth visual lines underneath close-fitting garments.

(look at these minxy 1830s dudes and their tiny waists)
As the century goes on the desired menswear silhouette becomes boxier and less fitted, and male corsetry recedes into the background; we start to see patents and advertisements for men's corsetry, so they still seem to have been worn, but there's a lot more language around vigorous manly athleticism and supporting the structures of the body. It can be hard to tell whether a particular piece is intended to be worn primarily for some medical purpose or for its perceived aesthetic benefits. This is giving me such flashbacks to trying to find post-surgical compression garments.
(Side note: there's also a vigorous tradition of fetishist writing about corsetry all through the 19th century, in fairly mainstream channels, which is fascinating. Due to the relatively private and deeply horny nature of fetish tightlacing we don't necessarily know as much about what those same letter-writers may have "really" worn at home, but I hope they were having fun.)
I've seen very few specifically men's corsetry patterns from historical pattern-makers-- not even really big names like Redthreaded. I sewed my 19thc menswear corsets from the men's underbust pattern in Laughing Moon Mercantile #113 which afaik is speculative rather than reproducing a specific historical garment, but it's not too different from the women's late-19th-century underbust patterns in the same pattern pack.

(image credit: LMM)
However, a lot of underbust and waist-cincher patterns from more general historical patternmakers could be made suitable with some minor alterations. Here I'd also rec books like Jill Salen's Corsets: Historical Patterns And Techniques and Norah Waugh's Corsets & Crinolines, though their focus is definitely on womenswear and you need to be relatively comfortable scaling up or drafting from pattern diagrams.
The structural features and desired results for a man's corset are pretty much the same as any other corset (back support, compression in some areas, etc.) even when the desired silhouette is different; commercially-created patterns are drafted with the expectation of certain bodily proportions so like with all corset-sewing it's important to make a mockup for fitting purposes. (I ended up liking one of my mockups so much I finished the process and made it a whole separate corset.) I don't know much about this area but I seem to see a lot more belt-and-buckle closures and criss-crossing straps in corsets designated as being for men -- this might be a byproduct of gendered differences in how people got dressed, but it might be nothing.
There's some weird and wonderful historical examples, both extant and in images -- I appreciated this post at Matsuzake Sewing, "A Brief Discussion Of Men's Stays", and its accompanying roundup of images on Pinterest though the tone wrt historical fetishwear corsets in the blog post is a little snippy. I really want to make a replica of Thomas Chew's 1810s corset (which you can read more about here at the USS Constitution Museum) but it incorporates stretch panels made with a shitload of metal springs and I'm not ready for all the trial and error trying to replicate that.

(image credit: USS Constitution Museum Collections)
There's a pretty rich vein of modern men's corset patterns which seem like they could be easily pattern-hacked for historical costuming purposes, like these with shoulder straps from Corsets By Caroline or DrobeStoreUpcycling's waist cincher which also looks like it could be altered pretty easily to cinch with straps and buckles like some 19thc men's corsetry does. This pattern for a boned chest binder in vest form by KennaSewLastCentury is also really cool but I didn't get a chance to sew it pre-top-surgery. (I think I've also seen someone who made a chest-compressing variation on Regency short stays, but I can't find it now.)
In general a lot of underbust and waist-cincher patterns should work just fine for silhouette-shaping without much bust/hip emphasis -- my usual resource for free corset patterns (Aranea Black) recently took down all her free patterns but they're definitely still circulating out there. For general fashion purposes the sky is the limit and there are a lot of enthusiastic dudes in corsets out there. This Lucy Corsetry round-up shows a variety of modern corsetiers' styles designated as being for men or more masculine silhouettes (including a SUPER aspirational brocaded corset with matching waistcoat made by Heavenly Corsets that I'd love to sew a historical spin on) and you can see some commonalities and possibilities for body-shaping.
I can also give some more general corset-sewing resources but I'm very much in the learning process here and I'd love any recs or input from people more experienced in pattern-drafting and corset-sewing.
95 notes
·
View notes
Text
I can't believe that this is a debate that we seriously have to humour at this point but since this is clearly the level of (trans-)misogyny we're at: The reason that men outperform women in chess is mathematics. It is not some "biological" advantage. It is a collective advantage, not an individual one. Not even an advantage of averages or median:
There simply are more men who play chess than women, especially at a professional level.
And if we assume that the necessary skills to succeed as a professional chess player are arranged on a bell curve across the population, that means the people at the very top end of that bell curve are going to be a very small number - and the simple mathematical odds dictate, that you are most likely to find this small group of people or at least the majority of that group within in the bigger group.
Let's say you have a group of 5000 AMAB people and a group of 500 AFAB people. Statistics dictate, that 1-2% of either has red hair. This accounts for 50-100 AMAB people and 5-10 AFAB people
Stupid conclusion: There is a correlation between gender and hair colour because there are more red-haired men
Logical conclusion: We have differently sized sample groups returning misleading data. When corrected for sample size, the results are about the same. This implies a lack of correlation between sex and hair colour
And this becomes even more evident if instead of a close-ended question (red hair: yes or no?) you have a Likert scale (e.g. performance): If we look for people with an Elo rating of say....2500 or up, it is very likely that we find more of them in the largest sample-size and fewer of them in smaller sample size. We are also likely going to find more horrible chess players in the larger sample-size. Except we are not testing for bad chess players or holding competitions for Worst Chess Player, preventing the reading that men are actually worse at chess than women.
The idea of excluding trans women from women's chess is actively cementing misogyny (the idea that being AMAB gives you some superior brain power and logical-strategical reasoning) and feeds the narrative that there is a biological reason for the distinction that is being made - when there isn't. It is, in fact, the oldest story in the book: Having a misogynistic expectation already planted in your head and using whatever data you can find (more male Grandmasters) while allowing only for one possible answer: If data shows that women are at a disadvantage, it is because women are inferior. If data shows that women have an advantage, the study has an agenda.
It is straightforwardly anti-scientific and rooted in misogynistic bias. It erases the studies that show us that there is no indication of a significant biological aspect to an individual's chess performance. It's erasing the data we have in favour of the deeply misogynistic narrative that women are less intelligent or strategically minded than men. The solution here is not to ban trans women - it is to teach your afab kids chess and to motivate them and have them play in atmospheres that are welcoming to them. So that one day, chess is no longer socially viewed as a male-sphere and a male interest and that maybe we have comparable sample sizes.
Trans women make up 0.6% of the human population, as far as we can document - that is 1.2% of women. They have no mathematical advantage over cis women, cis women are outnumbering them significantly. Banning trans women from women's chess is on the same level as banning the aforementioned red-haired women - WITH an additional helping of sexism and discrimination, anti-scientific sentiment and medical misogyny reasoning.

#I'm not sure this is worded in the best way but this whole thing is so stupid#misogyny#transmisogyny
124 notes
·
View notes
Note
I feel like it's more common for gods to be associated *with* things rather than *of* things. not that there are never gods of things it just doesn't seem like it's as common that gods were boxed up so tightly in antiquity as people seem to do with them now, and maybe that's a result of thousands of years of cultural separation, I don't know ¯\_(ツ)_/¯
okay so let's deconstruct this shall we?
I never said there was a god 'of' beekeeping. Someone asked me about it, but I said that while there are gods/goddesses in Ancient Egypt who are associated with bees in some way (i.e. there's at least one mention in their mythology) they're not directly related to it.
So, lets talk about cultural separation, and the direct implication of modern bias, and re-centre it within the Egyptian cultural background. When we talk about 'associations' or 'gods of X' what we mean by that is that the Egyptians themselves very clearly reference a certain aspect or association again and again. They make it very clear in their writings that a certain plant/animal/natural phenomenon/emotion is tied intrinsically with this deity's behaviour and mythos.
Take Seth, for instance. One of his main aspects is chaos, and that's often associated with storms, thus he is often noted as a storm god. So, how do we know this? Well the Ancient Egyptians frequently talk about storms in relation to Seth. Several words for 'storm' in Middle Egyptian use the Seth-animal determinative when writing them, or they use the medjed fish determinative, and the medjed fish is also associated with Seth. In Egyptian medical papyri, certain afflictions we reverse-diagnose as a headache were referred to as “a storm in the head”. In addition, in the story of Seth, Anat, and the seed of P’Re, Seth tries to take the goddess Anat against her will, but the Seed flies against his forehead and he is taken ill, presumably with a terrible migraine. Now, the earliest example of that story we have it from the Ramesside Period, but it’s indicative of a certain connection storms and Seth himself had to headaches.
See how there's a lot of repeated symbolism, and how the Egyptians weave this into their everyday lives? That's how we can say that Seth is both associated with and the deity of Storms in Ancient Egypt.
In the case of bees/beekeeping, none of the gods mentioned in the original post have this sort of continual weaving of bees throughout their mythos that spills into the everyday consciousness. I've tried to look up the 'Ra cried Bees into existence' myth, to see what the original text it is that comes from so I could understand it in a better context. Do you know what I found? Endless references to people saying it, but no one actually mentioning where this information was from. When that happens in academia, it's what's known as a 'circular citation', where someone said it once and then everyone has repeated it but...it might actually not exist at all. If Ra was associated with bees to the point that it escaped the religious sphere (where usually only priests and the king cared and none of the regular populace would have been aware of it) and entered popular consciousness then we'd expect to see references to Ra in scenes where they make honey, or metaphorical references to it within texts that talk about bees and/or honey. But you don't. The Egyptians don't mention him, or any other god for that matter, when discussing it.
Thus, from looking at how the Egyptians themselves associated bees and their surroundings, we can determine that there wasn't (as far as I can find out) any specific deity they associated with, or thought bees to be an aspect of, bees and beekeeping. I mean, we know Min is associated with lettuce, because when lettuce is mentioned the Egyptians make reference to Min in one way or another. If the same were true for bees, we'd see that reflected in the corpus and we don't.
So, no one is boxing anything up tightly. Based on the current evidence we have, and knowledge of how the Egyptians interacted with their gods, we can pretty much say 'ehh while they may have mentioned it once, it didn't really form any aspect of their worship'.
But ¯\_(ツ)_/¯
60 notes
·
View notes
Text
Reed the Flame Shadow has allowed for a lot of creative plays, she’s truly fun to use. I also appreciate that she’s very versatile and that her skill selection is very case to case basis, like Cantabile for example. Both S2 and S3 have a lot of different roles and applications besides their main apparent slotted duties. S2 is her most damaging skill, though also her most resource-intensive skill if the aim is to use it for single target shredding (three deployment slots! Congruent with Kal’tsit, who needs two to do her huge damage — I like this idea of Medics that can theoretically deal a lot of damage but are expensive to use in the terms of slots), but even if you don’t want to use it like that, it’s still an immensely useful skill to lane, sustain and dps.
Likewise, S3 is famous for its big explosions and crowd thinning, but it’s not bad at all when you need a mix of mob control and boss/elite killing power. In IS3 Waves 12, for instance, the ATK debuff in Cinders has actually been very useful to survive some hits that my units otherwise would’ve buckled under, and the fact that it’s multitarget with a decent ATK buff means that Reed will be doling out insane healing in addition to good damage. I keep seeing this aspect of the skill glossed over, it’s an incredibly powerful sustain tool in addition to a damage tool, Cinders also inflict Arts Fragile, which stacks multiplicatively (to my knowledge) with Fragile, so a combo with Suzuran, Shamare, Pramanix and Gnosis can set up some truly delirious Arts haymakers on enemies.
Flame Shadow does so much for a single slot, with varied selection! She’s become core in my teams now. Part of that is my bias since she’s a favorite, but the other part is raw utilitarian pragmatism since she is honestly that good. Funnily enough, her S2 suffers from a similar issue as Laurentina’s S3: It’s description is not quite effective at explaining exactly how strong the skill really is.
104 notes
·
View notes
Text

Pain and Prejudice: A Call to Arms for Women and Their Bodies by Gabrielle Jackson is an excellent addition to my health feminism and bias in medicine shelves.
She does an excellent job of laying out why there are no incentives for treating or researching chronic pain, and how the healthcare system must adjust; she also makes a good case for why this change should come from the government and their funding. She breaks down well how the system is not set up for something like chronic pain, and highlights the issues of 'heartsink' patients, the pressure on doctors to cure and have all the answers rather than mitigate or investigate, and how a higher life expectancy does not necessarily mean a better life quality.
I've reviewed many of these books and so I want to highlight specifics that Jackson brings to the table that I did not find in other books. These include a breakdown of Chronic Overlapping Pain Conditions (COPCs), descriptions of each of the primary ones and how they intersect, and a focus on chronic pain conditions overall throughout the book. She has a especially excellent breakdown of how the lack of knowledge of female biology overall results in hysteria narratives, an enforced need for women to go to the doctor more often for basic prescriptions due to an inherent distrust or policing, and how overall misogyny and sexism ties in with our inability to believe women about their pain. I appreciated how Jackson paired her discussion of a lack of education in female biology and chronic pain with an in-depth education about those things for women who might need it.
I also appreciated her quoting and acknowledging Maya Dusenbery. I've found that many books recently quietly use her research or issues she brought to the forefront but bypass her specifically, and so I really appreciated how much she was highlighted for her analysis of this issue.
Overall, Jackson's book is a tremendous success and call-to-action about the bias in medicine against women, the failures of the health-care system to treat or consider chronic pain conditions, and what can be changed. Her own endometriosis story influences much of her writing, and it adds a particular indignation throughout that is tremendously satisfying and convincing.
Content warnings for sexual assault, compulsory sexuality, misogyny, medical trauma.
#pain and prejudice#gabrielle jackson#health feminism#chronic illness#bias in medicine#sexism in healthcare#healthcare#chronically ill#fibromyalgia#endometriosis#my book reviews
45 notes
·
View notes
Text

12th January 1932 saw the death in India of Isabel Kerr, a doctor and missionary who pioneered the treatment of leprosy in India.
Isabella Kerr was born in Gollachy, Enzie in Banffshire on 30 May 1875. Her parents were Mary Garden and John Bain Gunn, a farmer. Kerr studied medicine at the University of Aberdeen, graduating in 1903.
Kerr met and married the Reverend George McGlashan Kerr, a former joiner who had returned from being a missionary in Africa. . They married in 1903, and worked together in England until they were sent out to India by the Wesleyan Methodist Missionary Society in 1907
Upon undertaking missionary work, not related to their field of interest, they realized the medical treatment given to the leprosy patients was inadequate and warranted serious attention. Considering the incidence of leprosy in this area and the urgent need for proper treatment of the patients at the right time in 1911 Kerr opened a leprosy centre at the mission in Nizamabad, Telangana.
In those days many of the people were not aware of an important fact about leprosy because of misinformation and ignorance. It is one of the least infectious diseases as nearly everyone has some kind of immunity to resist it.
The unfortunate patients had to suffer unbearable Stigma and ostracism on account of disfigurement suffered by them. So, they were isolated and shunned, removed far away from the community. Fear of discrimination, poor treatment of them in the society impacted every aspect of their life-style. In its wake affected are their participation in the social activities, marital life, livelihood, economic security, and mental health. Leprosy is also the leading cause of permanent disability in the world and is primarily a disease of the poor.
The news of her mission and dedicated work and medical treatment without any bias spread far and wide like summer bush fire. Consequently, the response was just overwhelming and she needed additional space and beds to accommodate them.
By the early 1920s, the hospital gained better name and had more than 120 buildings dedicated to leprosy related problems. Many buildings were built by the Nizam family members. The complex comprised 360 acres of land.
She worked closely with Ernest Muir who had experimented with the use of hydrocarbons to treat leprosy. Their centre at Dichpali became a leading center for leprosy treatment and cure and people in thousands were benefited at this center. In view of their dedicated services to the cause this dreaded disease and their establishment of a leading hospital to treat leprosy. patients, the British India government awarded Kaisar-i-Hind Medals to the couple in 1923. As ill-luck would have it, Kerr died in January 1932 (at the age of 56) and her husband George Kerr continued her mission until 1938 after which he got back to Scotland to lead a retired life. In the 1960s, the hospital founded by Isabella Kerr could take care of 400 patients. The incidence of leprosy in India has come way down. Isabella Kerr's name is permanently etched in the medical history of India related to leprosy.
The following is quoted from an obituary on Isabel Kerr;
'Dr. Isabel Kerr, a medical missionary who was one of the foremost authorities on the treatment of leprosy in India, has died at Dishpali, the Methodist Leper Home and Hospital near Nizamabad, of which for the past 12 years she had been the medical superintendent. Struck with the great need for a leper home in the area, she and her husband chose a beautiful site six miles from Nizamabd and, with money given for the purpose by a devout Hindu, began to build. When Sir Leonard Rogers made great discovery of the remedial value of the injection of the essential principle from chaulmoogra oil, the home developed into a hospital.
In 1923 Dr. Kerr was awarded the Kaisar-i-Hind Gold Medal in recognition of her services. Her medical skill and her devotion to the cause of the leper, together with her modest reserve and womanly charm, won her innumerable friends both in India and at home.'
The photograph is of Kerr vaccinating a child
11 notes
·
View notes
Text
A Study In White:
The first wave of cocaine use occurred in the second half of the 19th century, between 1860 and 1905. This stimulant, which has the characteristic of causing a pleasant effect, evidenced by a feeling of well-being, euphoria and lack of shame, was greatly welcomed in the medical community as a miraculous panacea that could be used to solve various diseases and ailments, from toothache to labor contractions, as well as mental disorders such as “hysteria” or “melancholy”. One of the greatest enthusiasts of the therapeutic use of this substance was the Austrian physician Sigmund Freud who often prescribed this drug during consultations with his patients to resolve the most varied emotional or physical pathologies.
In this sense, when considering the close patient-physician relationship that was probably established between the latter and Mr. Sherlock Holmes during treatment for the absence seizures that he reported to be having due to malicious hypnosis techniques, it is possible to assume that cocaine was indicated by Dr. Freud to Mr. Holmes. Furthermore, if Sir Arthur Conan Doyle's transcripts are taken at face value, it is noteworthy that in the first book, which would give rise to the series of the detective's adventures, “A Study In Scarlet (1887)”, Mr. Holmes mentions taking regularly, 3x a day more specifically, the stimulant at 7% dilution intravenously. A high dosage, but not particularly shocking as the occasional use of the drug was common practice in Victorian England.
Reaffirming this fact, in “The Sign Of Four (1890)”, cocaine is referred to as a mind stimulant and nerve tonic during idle moments, being extremely useful for strengthening logical reasoning. It is thus clear why the use of the stimulant is so appealing to Holmes, since there are few other things he values in equal esteem as the power of his brain and the importance of keeping his wits sharp. In addition, if Freud had indeed prescribed the drug there would be even more reason for Holmes to use it religiously in order to avoid the relapse into the absence seizures that made him seek help from the Phoenix Brotherhood in the first place.
It is also noteworthy that Holmes did not consider himself an addict in the most common sense of the word, but maintained his chemical dependency as something to be managed. This sense of control over one's addiction, whether justified or not, will be a relevant point as this discussion moves towards its conclusion.
Now that the foundations of this essay have been laid on the character of one of those involved, it remains to discuss the other. Unfortunately, due to the specific quality of the fraternity of which it is said and I quote, "Amelia is all about secrets", there has been a difficulty in obtaining reliable data about the past life and believable personality of Arthur, the Interviewer and many of the claims that will be made here are based on speculation and empirical analysis. In order to avoid unnecessary bias when dealing with an individual who is already sufficiently obscure, two main sources were used: "The Amelia Project Wiki: The Interviewer" and "The Amelia Project Personality Database: The Interviewer".
Based on these, the following information was extracted:
“The Interviewer is a very jolly fellow. He is often enthusiastic and can be quite intense, especially when engaged in something of his liking. However, he is also very easily bored, and doesn't like to partake in things that's not interesting to him. While often friendly, he can come across as a bit arrogant, rude and self centered. He does care a lot about the people closest to him though, and often seems genuinely interested in helping other people, and of course to hear their stories.”
Furthermore, he fits as a 7w8 ENTP by the Myers-Brigg method, associated with the sanguine temperament described by Galen of Pergamum.
Although the ENTP 7w8 personality is seen as a particularly cheerful, outgoing, intellectual and quick-witted type who value creativity, freedom and self-expression above all else, these have as their main characteristics the impulsiveness that leads them to take unnecessary risks and accomplish poor planning in medium and long term consequence analysis. These individuals tend to be irresponsible, often putting themselves in dangerous situations, since the journey for “freedom and stimulation” can lead them to destinations that are sometimes easily avoidable.
In addition, the sanguine temperament only reinforces these traits. While they are generally communicative, expressive and cordial, they are also prone to emotional instability and indiscipline, often being exaggerated and unproductive in their decisions.
It is emphasized, of course, that the use of stimulating substances is related to several intrinsic and extrinsic factors to the individual, but several researchers such as the Institute of Addiction Medicine, in Philadelphia, USA, point out personality traits that are common in people with greater chance of developing chemical dependency, namely: Impulsivity, non-conformity, low stress tolerance, sensation seeking, etc.
It is possible to observe that Arthur, the Interviewer has most of these traits, having a personality that almost presents itself as a risk factor.
That, coupled with a close friend, Mr. Holmes, who makes prescribed use of the drug while denying the addictive quality of the substance, plus the fact that at the time there was no knowledge about the negative effects associated with its use, such as neural destruction, liver and kidney damage, mental illnesses, among other problems, corroborate the speculation that Arthur could have been exposed and even introduced to the stimulant during the period referring to the cohabitation between him and Mr. Holmes.
Furthermore, it is chronologically possible with what was exposed during the year 1929.
BIBLIOGRAPHIC REFERENCE:
Available at: <https://www.google.com/url?sa=t&source=web&rct=j&url=https://www.victorianweb.org/authors/ doyle/addiction.html&ved=2ahUKEwiHlLXfzL3_AhUurpUCHZ-FCNUQFnoECBEQAQ&usg=AOvVaw3P5rR8LLkdUh3gx32ln5Vj>. Accessed on: 13 June. 2023.
Available at: <https://www.google.com/url?sa=t&source=web&rct=j&url=https://www.gruporecanto.com.br/ blog/what-leads-a-person-to-use-drugs-understand-the-reasons/&ved=2ahUKEwiL16iGzb3_AhUSrJUCHZdIDR0QFnoECBAQAQ&usg=AOvVaw06pjH1omH5FVLgpi3PAlX8>. Accessed on: 13 June. 2023.
Available at: <https://www.personality-database.com/profile/602939/the-interviewer-the-amelia-project-mbti-personality-type> . Accessed on: 13 June. 2023.
The ENTP 7w8 : Characteristics, Weaknesses and Famous Characters - Introverted Growth. Available from: <https://introvertedgrowth.com/entp-7w8/>. Accessed on: 13 June. 2023.
@ameliapodcast though you would like the essay
22 notes
·
View notes
Text

Abstract
The study’s purpose was to describe a population of individuals who experienced gender dysphoria, chose to undergo medical and/or surgical transition and then detransitioned by discontinuing medications, having surgery to reverse the effects of transition, or both. Recruitment information with a link to an anonymous survey was shared on social media, professional listservs, and via snowball sampling. Sixty-nine percent of the 100 participants were natal female and 31.0% were natal male. Reasons for detransitioning were varied and included: experiencing discrimination (23.0%); becoming more comfortable identifying as their natal sex (60.0%); having concerns about potential medical complications from transitioning (49.0%); and coming to the view that their gender dysphoria was caused by something specific such as trauma, abuse, or a mental health condition (38.0%). Homophobia or difficulty accepting themselves as lesbian, gay, or bisexual was expressed by 23.0% as a reason for transition and subsequent detransition. The majority (55.0%) felt that they did not receive an adequate evaluation from a doctor or mental health professional before starting transition and only 24.0% of respondents informed their clinicians that they had detransitioned. There are many different reasons and experiences leading to detransition. More research is needed to understand this population, determine the prevalence of detransition as an outcome of transition, meet the medical and psychological needs of this population, and better inform the process of evaluation and counseling prior to transition.
Sir,
Bustos et al1 aimed to measure the prevalence of regret following gender-affirmation surgery. Given the significant rise in young people seeking medical intervention for gender dysphoria, which can include surgery, outcome studies that accurately assess regret are of increasing importance. In this letter, we argue that the conclusions of their systematic review and meta-analysis are questionable due to limitations in their methods and shortcomings of the studies selected.
Starting with methods, the authors overlooked numerous relevant studies, including one of the best-known,2 raising questions about the adequacy of their search strategy. One study3 was inappropriately included as it only investigated regret regarding choice of surgical procedure, not of surgery itself. In addition, there are significant data extraction errors, leading to erroneous conclusions. For instance, the sample for surgical regret in their largest included study4 was inflated from 2627 to 4863, likely due to a miscalculation from a table reporting the treatment patterns of that paper’s total study population.
Besides these methodological inaccuracies, data in this field are often of low quality because of “lack of controlled studies, incomplete follow-up, and lack of valid assessment measures,”5 as well as the long amount of time regret can take to manifest (the average and median are estimated at 8–8.5 years2,4). Many of the included studies had participants with follow-up periods of only 1 or 2 years postsurgical transition. None appear to have a long enough follow-up period to reliably identify regret. The study contributing almost half of the participants4 explicitly noted their inclusion of participants with short follow-up time, relative to time to regret, and their large 36% loss to follow-up as limitations. These shorter studies only provide an estimated lower limit, as the large numbers of patients lost to follow-up add correspondingly large uncertainties to any quoted number.
Bustos et al1 acknowledge “moderate-to-high risk of bias in some studies.” Actually, this affects 23 of the 27 studies. The majority of included studies ranged between “poor” and “fair” quality: only five studies—representing just 3% (174) of total participants—received higher quality ratings. However, even these had loss to follow-up rates ranging from 28% to more than 40%, including loss through death from complications or suicide, negative outcomes potentially associated with regret.
A last and major concern involves sample selection. The cohort presenting with gender dysphoria today is substantially different from the cohort presenting during the research periods of the included studies. Further, there has been a significant liberalization over time of the criteria assessing readiness for surgery. Thus, the outcomes reported may be of limited relevance for estimating current surgery outcomes. Additionally, the generalization to “TGNB” populations seems unreliable, as it is based on an explicit sample size of only one “non-binary” patient. The authors do not address these issues.
In light of these numerous issues affecting study quality and data analysis, their conclusion that “our study has shown a very low percentage of regret in TGNB population after GAS” is, in our opinion, unsupported and potentially inaccurate.
Abstract
Two Dutch studies formed the foundation and the best available evidence for the practice of youth medical gender transition. We demonstrate that this work is methodologically flawed and should have never been used in medical settings as justification to scale this “innovative clinical practice.” Three methodological biases undermine the research: (1) subject selection assured that only the most successful cases were included in the results; (2) the finding that “resolution of gender dysphoria” was due to the reversal of the questionnaire employed; (3) concomitant psychotherapy made it impossible to separate the effects of this intervention from those of hormones and surgery. We discuss the significant risk of harm that the Dutch research exposed, as well as the lack of applicability of the Dutch protocol to the currently escalating incidence of adolescent-onset, non-binary, psychiatrically challenged youth, who are preponderantly natal females. "Spin" problems—the tendency to present weak or negative results as certain and positive—continue to plague reports that originate from clinics that are actively administering hormonal and surgical interventions to youth. It is time for gender medicine to pay attention to the published objective systematic reviews and to the outcome uncertainties and definable potential harms to these vulnerable youth.

Abstract
Introduction
Concerns about future regret and treatment discontinuation have led to restricted access to gender-affirming medical treatment for transgender and gender-diverse (TGD) minors in some jurisdictions. However, these concerns are merely speculative because few studies have examined gender-affirming hormone continuation rates among TGD individuals.
Methods
We performed a secondary analysis of 2009 to 2018 medical and pharmacy records from the US Military Healthcare System. We identified TGD patients who were children and spouses of active-duty, retired, or deceased military members using International Classification of Diseases-9/10 codes. We assessed initiation and continuation of gender-affirming hormones using pharmacy records. Kaplan-Meier and Cox proportional hazard analyses estimated continuation rates.
Results
The study sample included 627 transmasculine and 325 transfeminine individuals with an average age of 19.2 ± 5.3 years. The 4-year gender-affirming hormone continuation rate was 70.2% (95% CI, 63.9-76.5). Transfeminine individuals had a higher continuation rate than transmasculine individuals 81.0% (72.0%-90.0%) vs 64.4% (56.0%-72.8%). People who started hormones as minors had higher continuation rate than people who started as adults 74.4% (66.0%-82.8%) vs 64.4% (56.0%-72.8%). Continuation was not associated with household income or family member type. In Cox regression, both transmasculine gender identity (hazard ratio, 2.40; 95% CI, 1.50-3.86) and starting hormones as an adult (hazard ratio, 1.69; 95% CI, 1.14-2.52) were independently associated with increased discontinuation rates.
Discussion
Our results suggest that >70% of TGD individuals who start gender-affirming hormones will continue use beyond 4 years, with higher continuation rates in transfeminine individuals. Patients who start hormones, with their parents’ assistance, before age 18 years have higher continuation rates than adults.
#Christina Buttons#Leor Sapir#Dr. Phil#Lisa Littman#detrans#detransition#transition regret#medical scandal#medical malpractice#medical corruption#evidence based medicine#gender affirming care#gender affirming healthcare#gender affirmation#religion is a mental illness
4 notes
·
View notes
Text
The Exterminator
So, I’ve been talking with @dnpanimationstudioclone about Danny Phantom for a while, mainly their renditions of the cast. While we were talking, something stuck with me while we talked about Spectra: mainly, the way she died.
https://www.tumblr.com/dnpanimationstudioclone/704033048987140096/the-good-doctor-has-always-been-trapping-people?source=share
Basically, the working idea was that a client finally realized Spectra’s true nature and used a black widow to kill her. The plan worked perfectly as the client was never even suspected. Well, I wanted to expand on this character, hence the creation of The Exterminator.


A ghost who is demented enough to use blood blossoms is too horrendous of an idea, hence why many ghosts believe The Exterminator is a myth. However, those who were aided by them know far too well that such a ghost does exist.
The Exterminator(Ex) is a very reclusive ghost. Even when they remove the scent of blood blossom from their hazmat suit, many ghosts just find it too risky to get too close unless they want to attempt to hire Ex or destroy them for status. Despite being classified as a bounty hunter, Ex is incredibly picky with what jobs they accept and dwells more within the material realm, hence making it more difficult to hire. Despite this, many ghosts desire Ex for their infamous blood blossom gas because of how effective it is. Despite the offered money and status, Ex only accepts jobs that require them to take out what they deem as ‘parasites’.
Character:
Role in the Story- Beyond being a ghostly ally to Danny and the human trio, I would have Ex be a cautionary tale for what Jack and Maddie will become if they ever go too far in their ghostly research(i.e. vivisection/dissection). Though they have good intentions, going past such a threshold would ensure their souls would never truly rest. Ex was right to be furious towards Spectra, but they could have reported and gotten Spectra fired/blacklisted. Instead, Ex went to the ultimate extreme of murder. Ex’s afterlife is one of solitude and they lived a typical life after the murder. What would happen to Jack and Maddie, known ghost hunters, if they become ghosts? Danny can’t imagine a single good outcome if this were to happen.
Also, Ex’s ultimate goal is to destroy Spectra completely, even if it results in their own destruction as well.
Abilities
Entomology- If the style of killing Spectra wasn’t already an indicator, Ex was an entomologist in life: a Taxonomic Entomologist to be exact. As their job focused on looking for insects unknown to science, Ex is very observant of their surroundings. Beyond this, Ex’s knowledge of living/ghostly insects makes them quite knowledgeable about making medicines. Ex usually acts as a medic if taking a collaborative job.
Gardening- Beyond insects, Ex grows their own medicinal herbs and flowers. Obviously, the most cherished flowers are blood blossoms.
Synthesizing- Ex is knowledgeable as to how not to liquefy blood blossom, but to compress it into canisters for portable use. They modified their gas gun to act as a portable synthesizer that can continue altering the blood blossom into different states(like water, ice, and air).
Investigation(conversationalist)- It’s the very reason Ex is so quiet that many humans talk to them: humans tend to hate silence. As Ex has a good memory and is a good listener, many humans like to vent to Ex about earthy and supernatural issues. Despite the Earthy bias, Ex can fill in the blanks of the human victims of the parasitic target, thus Ex only needs humans for additional information. When a ghost does try to talk to Ex normally, the effects are usually the same. Ex is quiet, but that doesn’t make them shy. Despite humans/ghosts not caring they don’t know anything about Ex when their conversations end, these interactions are always one of mutualism as Ex knows when to back off. They will never be in another parasitic relationship again.
Combat
Fighting style: Capoeira
I would classify it as capoeira as Ex always needs to be on move because of their lean stature and to ensure they spread out the blood blossom gas. You’d think this would be difficult having a large canister on their back, but it’s basically an extension of Ex at this point. Ex is always moving, never giving their target time to process what is going on.
Weaponry choice: Gun/ Bludgeoning
Gun- Despite being known for pumping out gas, Ex’s gun has different settings on it that they can choose from (similar to Ember’s guitar). These settings are:
Blood Blossom Gas(This gas is so dense, many onlookers mistake Ex’s gun as a flamethrower)
Blood Bullets(compressed blood blossom petals, look more like paint-balls than bullets)
Blossom Goop(meant as harmful confinement for ghosts, can be used for torturous interrogation. Ex has never done this despite Vlad Plasmius’ insistence)
Because of these different states of blood blossom, Ex’s gun acts as a synthesis tool. Also, Ex’s gun works as Bluetooth, hence why there isn’t a cord connected to the canister. However, this means Ex needs to be a certain distance from the active canister, hence why they strap it on their back. Ex can shrink their canisters for easy transportation(keeps them in their belt pouches), but the canisters can’t be activated in these shrunken states.
Canister- Now, I would have Ex trained with using typical melee weapons(sword, spear, knife, clubs), but I just find the idea of Ex using their canisters as their main bludgeoning weapon to be hilarious. Like, a ghost believes they got Ex to use up all their blood blossom gas so it goes in for an attack. Ex proceeds to bash the ghost into ecto-goop with the empty canister. Ex also uses the exposed canister as bait, many ghosts try to damage their hazmat suit to expose them to their own concoction; an ironic ending to Ex’s existence. However, no ghost has yet to survive such a stunt to spread the word about the truth about Ex.

Ex is a Blood Blossom Ghost.
Pronouns- She/They(unknowingly a demi-girl)
Appearance-
For her hazmat suit and casual look, I used the blood blossoms color scheme. Despite the blood blossom petals being a bright red, I just couldn’t bring myself to use it beyond Ex’s hair lining, pupils, and the blood blossom gas: it’s just too much for me.
So, for her hazmat suit, I chose the stem/leaf colors: black and purple. I made the hazmat suit have a gradient to make the brightness of the purple more gradual(seriously, I didn’t remember OG blood blossoms being so bright) and to draw the viewer's eye to Ex’s gas mask. I also added the crossing straps to add visual interest to Ex’s chest. I couldn't for the life of me figure out what to put there logo-wise, so, the straps took its place. I added the additional color of white to lighten things up and to draw a subtle connection to her casual look. I made the Ex’s hazmat suit tight in the chest while making it baggier everywhere(the arms and legs) as I wanted to show off their abs.
I’m particularly proud of how the canisters turned out despite how simple they are. The spider is to show Ex’s lingering hatred of how Spectra took advantage of them when they were alive. I’m not sure why the canister on Ex’s back is so hazy, but the amount of computer issues I had while drawing Ex makes me not care.
Now Ex’s casual look took a while for me to figure out. First, I wanted a purely sporty look for her, but then I wanted to incorporate overalls into her look. However, once I figured out Ex’s back story, I knew I had to drop both ideas. The overalls would cover Ex’s abs(a huge no-no for Ex), and a hint of sporty fashion with her yarn leg warmers(Even through death, Ex has to keep training to retain her beautiful muscles). Ex’s skin was originally going to be black with purple lining- correlating with the hazmat color scheme, as I found the idea of Ex looking like OG Spectra an interesting parallel. However, I changed it to white as I thought the correlation to Walker was more interesting: Both have good intentions, but their methods have become corrupt over time. For artistic reasoning, I had an easier time adding details over white than black. I made Ex’s pupils X’s as a subtle way to tie her casual look to her hazmat look.
Instead, I went with a more fashionable approach, with Ex wearing a black sheer long-sleeve shirt as a way to show off her abs and feel free. The bra underneath is pure black while the straps and extra detailing are red. The red jean shorts follow the same theme of wanting to feel less constrained and showing off muscles(thighs for days!). Her boots were originally gonna be black, but I just couldn’t get the detailing to pop, so I went with a gray with red stitching.
Again, despite the simplicity, I love how Ex’s hair turned out. I was having difficulty figuring out what bangs to give her, almost dropping them with the aid of a headband, but I found a very easy solution. I just used the leaf shape of the blood blossoms to help me. I’m especially proud of how her rose bun turned out. If my username wasn’t an indication of it already, I like roses. So, I had a lot of fun just drawing the hair.
With the heavy makeup: the long black eyelashes and red lipstick along with the dark circles underneath her eyes, I wanted to show Ex’s age: either mid-30’s-mid 40’s. As Ex lived her life until passing away to natural causes in her 90s, I wanted her ghost form to reflect when she was in her prime. Not only did she finally achieve her muscular body around that time frame, but that was also when she met her husband. From the golden necklace hangs the diamond wedding ring Ex made sure she was buried with as she never wanted to lose this connection with him.
Overall, I’m happy with how each version of Ex turned out. I like the idea of Ex wearing a hazmat suit not for their protection, but to protect innocent ghosts from herself as her mere existence is a threat. Not that their hazmat suit is uncomfortable, Ex just wants to occasionally be fashionable and let her muscles air out every once in a while: an act she can only achieve either in her lair or in the human realm. I also like the idea of her gas mask contorting her voice, making it harder for ghosts to truly know who they are until she reveals it herself, like Lord Dominator from Wander over Yonder.
Myer Briggs Personality- INFJ
Ex is very particular about who they choose as a client let alone a friend. Because of this, Ex is always watching, always picking up on every micro action that even the person doesn’t realize they are doing. The observation makes Ex know if those around them have good intentions or not, her intuition has yet to fail even after death. Because Ex speaks only when necessary, those around always stop to listen.
Don’t mistake Ex’s silence as shyness, for she does like being out in public and is capable of delightful conversation. However, being a ghost does make humans hesitant to approach. Despite this, animals and children don’t seem to find Ex’s presence an issue as the sweet smell of blood blossom makes her quite approachable. Though Ex does enjoy the company, she favors the insects that come and taste the nectar of her petal hair. Even when Ex finds a friend, she tends to spend her personal time alone. While in her hazmat suit, many ghosts/humans can’t seem to pinpoint her gender, thus referring to her as ‘they’. Ex feels no need to correct this as it never hurts to have an alter-ego for protection, but something about being referred to so gender-less comforts Ex for some reason.
Since it takes a while for Ex to make up their mind, when they do make a decision- she tends to take the most extreme approach. Ex offers to make lunch, you’d better expect the number of meal options to rival a buffet. Ex says they’re going to help clean your house, you’ll see she not only dusted every crevice but also alphabetized any books/movies you have and color coordinate your closet. With such an extreme approach, it’s no surprise that Ex has multi-options of blood blossom ammunition. Though Ex is particular about her targets, she views those who protect the targets just as parasitic, thus the ecto-baths are common when Ex strikes. This approach has yet to deem itself negative, with no human nor ghost mourning those who Ex eliminates. Walker has even tried to hire Ex as a guard, but the warden’s need to make those he works with his prisoners have made such a deal impossible. It has taken a lot in Ex not to eliminate Vlad Plasmius for personal beliefs, the old halfa trying to hire Ex and attempting to blackmail her to do so. Alas, the old halfa skewed view of friendship ensures Ex's true companions are safe, so a simple pelting of blood bullets makes the halfa leave her alone for a while. If it weren’t for the fact that Plasmius paid his ghost goons fairly well, Ex would have eliminated the man ages ago.
Because Ex manifested into such a rare ghostly form(blood blossom), she interpreted their predicament as a mission that needs to be completed: To get rid of every parasite they come across. Ex believes if she takes out enough parasites, she can finally ascend and possibly reunite with her family. There are rumors that the parasite Ex had taken out in their life had manifested into a ghost, a rumor Ex takes completely seriously. If Ex were to ever see that damn therapist again, she’d make sure that parasite will completely fade to nothingness even if that means she has to fade too.
How Ex Gains Strength- Since Ex is a type of plant ghost at the end of the day, water and sunlight are her prime requirements to rejuvenate. It's a slow process to gain additional strength this way, but there’s no way Ex would energy feed like some parasite. Perhaps an ecto-charged plant feeder would give Ex a quick power boost, like an energy drink. Alas, Ex wouldn’t want to have such things too often as she does favor water the most.
Weaknesses-
Long-range weapons: Blood Blossom and Capoeira can only take Ex so far as a skilled shot can incapacitate them at the very least.
Ice/Snow: Not only does gas not travel properly in cold climates, but Ex’s gun needs to be at an average temperature to be able to synthesize properly. Can you imagine the embarrassment Ex would feel if she lost not only to a single snowman, but a single snowman that was very capable at snowball fights?
Approachability: It’s hard to get a read on someone who’s always wearing a mask. The fact Ex doesn’t talk much makes it even more difficult for many to approach.
Story Facts in no particular order:
It’s Vlad who informs Ex that Spectra does exist and he can take them to her as proof: A corrupted version of Zuko helping Katara find the man that killed her Mother.
It’s Danny that teaches Ex the gender identity of ‘Demi Girl’, thus helping Ex learn more about themselves.
Ex found out that she wanted muscles after killing Spectra when she went to a bodybuilding competition and saw the women contestants.
She graduated from Cornell University with a master's in entomology. It was during college that she met her husband.
Ex had two boys(twins) and one daughter
Jazz reminds Ex of her daughter
Ex is completely willing to teach any human about blood blossom protection.
As humans don’t have ghostly money, Ex takes water as payment whenever they help with human parasites.
Ex never truly fights Danny, merely dodging his attacks until he and the rest of the phantom team calmed down enough to just talk with Ex.
Ex teaches Valerie how to properly take care of blood blossoms as the ones in her care at the time were struggling.
Ex is completely willing to teach any human about blood blossom protection.
Ex will destroy Spectra when they finally find her. Not only to ensure that no one else will become a victim but to make sure there’s no possible way Ex would feel as weak when she was in Spectra’s “care”.
When the two are face to face, Spectra and Ex instantly recognize each other.
Klemper is the main obstacle that keeps Ex from destroying Spectra. https://www.tumblr.com/dnpanimationstudioclone/690616135717093376/meet-klemper
Both Ex and Spectra are willing to fade to nothing if it means the protection of others, Spectra protects Klemper while Ex protects Jazz and the citizens of Amity Park. However, it’s Klemper and Jazz who protect the two from themselves.
OP notes: That’s it, I can’t keep working on this any more for the sake of my own sanity. If anyone is interested, I will post a legit background for Ex at some point with even more additional information, but I need a break from this character. I didn’t intend on having so much to write about them, but as you can see I ended up with quite a bit. Thank you to those who stuck around.
#Danny Phantom#danny phantom oc#original character#dp spectra#dp klemper#a-sterling-rose art#PhanArt#danny phantom fanart#my art#dp blood blossom#dp blood blossom ghost
10 notes
·
View notes
Video
youtube
saw this and because I literally never stop thinking about Transformers I immediately realised that in Pharma’s med bay on Messatine, Ambulon was absolutely “the resident”, lmao :’(
I know this because it’s hard to even find panels where he’s not actively working, lol, with the fucked up paint job and everything, look at him
you know he was Having Some Kind of Time through the whole rust plague thing because the entire time he’s been at Delphi he’s just been like “when can I transfer, can I get Pharma to give me a reference, does First Aid know anybody who might be hiring, if I go back to Cybertron is it worth the pay cut, if they ask me for my certifications do those databases even exist anymore”
I mean technically he was a Ward Manager, but we don’t know how medical career progression works in the TF universe and I always get a distinct “forever resident” vibe from Ambulon (possibly just because life dunked on him so hard), so I’m just gonna stick with that in my own perception of things lmao
also since Ambulon was working under Pharma/alongside First Aid, and we know he went through his Act of Affiliation relatively recently, I wonder how that might have affected his role in any healthcare provision duties... or how previously being not-an-Autobot might have impacted the way he was treated professionally by others, at least at first.
I also wonder about the process of integrating Decepticon and Autobot medics together into non-factional healthcare services after the conflict ended
because oh my god...
holy shit can you imagine what the Reintegration Act post-war was like from the point of view of the fucking medical teams
“hey we’re going to be introducing a few more staff members, check out the new roster”
“thank Primus, we need more people in... wait...HE’S THE BOT WHO KILLED--”
“yeah I know, he got some of mine too. he’ll be on the Cyberpathology Team.”
can you fucking imagine this process!!!!
like we know medical units were a target during the war, as unfortunately they are also often targeted in real life (my dad was an Army medic, I know this to be true)
and enemy medics may well have been asked to advise on any strategic actions against opposing medical units... it’s grim, but that’s war, and Cybertron has no Geneva Convention.
it would have been so fucking rough trying to form a non-factional healthcare system on Cybertron after the war, hooooly shit
thinking about all the possible safeguarding concerns, like the amount of shit that probably went into figuring out how to manage the Reintegration Act in regards to healthcare services must have been next level
I would imagine healthcare/medical services were probably among the last services to fully actually integrate, even if they did start to attempt integration efforts early (if only for the sake of ensuring all Cybertronians regardless of any prior factional allegiance may then feel able to access and obtain care if needed without fear of bias or lingering factional discrimination)
it’s a hell of a situation to have to figure out
I’d imagine they likely had people working in pairs for at least some time while sorting out how to fully integrate in a safe and agreeable way, lmao fuuuuck
(the reason I say that is because when a healthcare worker is suspected of intentionally harming or murdering patients in a hospital, it is often the case that staff will then be made to work in pairs whenever possible for the sake of surveillance until the investigation is concluded. sadly, this is very much a real thing which has happened on some notable occasions.
paired working can also be mandated when a service’s mortality statistics are notably higher than what is expected, typically also as part of a further investigation; it might be only certain staff etc. that are asked to pair up, or depending on the investigative approach, they might bring in externally affiliated observers either as an alternative or in addition to this type of measure. lots of variables, but it’s something that can and has definitely been done in specific situations.
it’s super grim so I won’t go too much more into this, but if you want to know about this kind of shit, check out the Stafford Hospital Scandal and the Stepping Hill Hospital Incident for a couple examples.)
it was probably not a great time for anyone for a good minute or so!!!
circling back around to my original point here though LOL, I truly feel for Ambulon, dude went through nothing but bullshit lmao
anyway, consider this post part of my never-ending campaign to get a canonical Med Bay mini-series of some kind, please just give me Scrubs but with space robots already, god it would be so good
#mtmte#lost light#ambulon#tf pharma#idw pharma#med bay#maccadam#maccadams#medbay#medbay posting#long post#analysis post#transformers analysis#transformers lore#reintegration act#idw 1#idw transformers
81 notes
·
View notes
Note
I couldn’t remember all the emoji’s but can I get trypanophobic💰+✌🏻(blood draw?)
And can the reader’s relationship be somewhere in between 🤝 and 💖? Like soft and physically contact but without kissing or anything associated with sexual attraction? (Asexual friendly)
Hugging, shoulder touching, back rubs/ pats/ soothing, hand holding is fine <3
Thank you so much for the request! Hope you enjoy! 💜


💛 Anon requested that Ravio has difficulties with his procedure.
💛 Anon requested that Ravio throws up.
💛 Anon requested that Reader calls Ravio заяц which is a Russian term of endearment translating to "bunny rabbit". Pronounced "ziats", rhyming with "bias" with the addition of the "t".
💛 Reblogs appreciated along with likes and comments!
💛 You can request your own scenario here!
💛 Content under the cut!
From the moment you step inside the building, Ravio is a bundle of anxiety and fear. You have to grab his shoulders and manually guide him over to the front desk so you can get him checked in. The poor bunny almost trips on his own locked knees as you walk to the room where the provider will be drawing his blood.
“Give me a few minutes to prepare, then we can get started. Please make yourself comfortable in the meantime,” the provider says from where they are setting out equipment.
You let your hands fall from Ravio’s shoulders and grab his hand. “Doing okay, заяц?” you ask softly, even though you know the answer.
Ravio squeezes your hand back, gripping tighter every time he spots something new. His eyes dart every which way, taking in the boxes of bandages and gloves on the counter, the two chairs lining the opposite wall, the sharps bin full of discarded syringes. His breathing comes out in stutters and gasps, and he squeaks, “No!”
You immediately pull him into a hug so he can stop looking for a moment. “Hey, I’m going to be here the whole time. Remember what we talked about. Take deep breaths, make sure you don’t look, and think about what I told you we’re gonna do after.”
Ravio hiccups then mumbles, “You said we can go to the market and I can get whatever I want?”
“That’s right! Remind me what you want me to buy?” you prompt, leading him to the chair and dragging the other right next to his.
“A new bell for the shop door… a-and some premium treats for Sheerow…” Ravio says, squirming in his seat. “And maybe some-” His words freeze in his throat as he glances at the provider, who has finished setting up.
“Hey, Ravio.”
His ear flicks back, gaze still set on the medical equipment.
“Look at me, please?”
He does, and you reach out and wipe a tear from his cheek. Your fingers spread to cup his face and he leans into your touch as your thumb smooths over already-tearstained skin.
“Focus on me, okay?” you tell him.
“All right, are we ready to begin?” the provider asks, the question making Ravio flinch.
“Ready as we’ll ever be,” you say, smiling at the provider. You try to ignore Ravio’s wide eyes silently begging for more time to delay.
“Very good. Tell me, Ravio, have you ever had problems during a test before?”
“This is his first time,” you answer for him.
“I see. Well then, would you like me to tell you what I’m doing before each step?”
Ravio whimpers and closes his eyes. Still cradling his face with one hand, you grab his dominant hand with your free one.
“I think it would be better if you don’t, please,” you say, watching Ravio’s reaction. When no argument comes, you nod to the provider.
They tie a tourniquet above Ravio’s elbow and clean his inner arm with a sanitizing wipe before feeling for a vein. He startles at the contact and tries to move his head and look, but you hold him in place, making sure he keeps facing you.
“You’ll make it harder on yourself if you look, заяц. Listen to me…” You keep up a steady stream of soft chatter, encouraging Ravio to focus on you and not the current situation. You pause a few times to answer the provider’s questions when they locate an ideal vein and explain the next steps using minimal detail.
“Deep breath, Ravio, like me,” you say, timing your example as you see the provider angle the needle towards the unsuspecting merchant’s arm.
Ravio yelps as the needle enters, thankfully not attempting to yank free of the provider’s grip. He squeezes your hand, face scrunched up in discomfort as the provider fiddles with the placement of the needle. After a few moments of experimenting, they pull the needle out and replace it with a sterile one.
“Don’t worry, it’s normal to take more than one try,” the provider assures you and Ravio.
Tears are flowing freely down Ravio’s face as the provider goes through two more sticks, each time having difficulty in their attempts to pierce the vein. You murmur and hush Ravio’s cries, squeezing his hand back whenever he feels another prick of pain. He grows paler, barely noticeable but still visibly so, and his hiccups turn into desperate gulps for air.
“It’s the vein,” the provider explains, preparing yet another new needle. “You may have some symptoms of dehydration or even malnutrition, Ravio. These problems often cause your veins to weaken, making them harder to keep in place for procedures.”
“That’s important to know. We’ll have to keep an eye on that,” you say. Ravio only lets out a strained whine.
The provider finally manages to insert the needle into the stubborn vein and you see Ravio’s blood begin to drain through the tube.
“You’re doing well, заяц! Now we just have to wait. How are you feeling?” you ask, noticing his overexaggerated steady breathing and eyes shut tight.
“Nnn… I think I’m gonna…” Ravio gasps, “Be sick-”
Before the provider can even move, you jump up and dart over to the counter, grabbing a small bin you noticed earlier. You place it on Ravio’s lap right before he loses the battle with nausea. He vomits into the bin, intermittent sobs breaking your heart as all you can do is rub his back and wait it out.
Thankfully, the spell passes before long. You set the bin aside so neither of you have to see or smell the sick. You’ll have to bring Ravio to the restroom later so he can clean up, but for now, you settle for holding him as closely as you can without jostling his arm. Your fingers reach up to play with his hair, gentle and careful to soothe without pulling at his sensitive scalp.
“I know, I’m sorry for all the pain you had to go through today,” you whisper, looking around him to check how much blood has been drawn. Good, it seems like he is almost done. “You’ve been so brave, my заяц, and you only have a few minutes more.”
True to your word, you barely have to wait before the provider slides the needle from Ravio’s arm and binds it with cotton and gauze. They instruct you to wait in the room until enough time has passed for Ravio to safely stand. Ravio shudders, exhausted from the stress of the procedure, and leans heavily against you.
“You’re all done now,” you assure him, giving him a smile that he is too tired to return. “And once we get out of here, the market awaits!”
#linked universe#linkeduniverse#lu#linked universe x reader#lu x reader#linked universe ravio#lu ravio#lu ravio x reader#trypanophobia#needle phobia#fear of needles#fable's asks#chatting with anon!#fable writes#next in line: 📚🐭💖✌️😮😣💬 requested by anon
29 notes
·
View notes
Note
what do you think of the headcanon that Heavy is fluent in English, and simply fakes being bad at it so people leave him be ? would that explain to you the inconsistent, odd language patterns he has ? would you have additional ideas of purposefully bad English he would use ?
To be honest, I'm not a fan of this idea, mostly because of the way I and a lot of people I know personally experience language-based bias.
I like to think my written English is fluent, and my spoken English is alright enough to qualify me as a language teacher, but I still very much do have an accent. Aside from that, I currently live and study in a place where people are fluent in a language I speak with difficulty, often making grammar mistakes and misusing or mispronouncing words. Kind of how Heavy does.
And the last thing any fluent speaker does when noticing it is leave me alone.
You see, when your language skills aren't that of a native speaker, there are automatically two walls of disadvantage in front of you. One of them is natural, the other one - imposed by society. The first one is easy to explain. You don't process the information you hear as quickly, you can't think of a suitable reply on time, you miss on a lot of conversations. You can't joke properly because jokes require their own, comedic timing, usually faster than your brain can work. You can't discuss a lot of topics you're passionate about because you lack the terminology. All of these things are deeply frustrating and infuriating, and something I personally wish was featured more often in Heavy-centered fanfiction, next to the funny misunderstandings and light-hearted quirks. But that's not what the ask is about, so I digress.
The imposed disadvantage is more nuanced and more unfair. When you speak a little slower than everyone else, use simpler words, and make grammar mistakes even a child wouldn't make, people start thinking you're... well, dumb. And from there on it can go several different ways, none of them - pleasant. Case one - they don't figure you're a foreigner, and just think you're stupider than them, so you get the respective treatment. People start speaking obnoxiously slowly to you, talking over you, poking fun at your language quirks, listening to how you say something over what you're actually saying. Case two - they do figure you're a foreigner, and it's miles worse in my experience, because not only do they base their perception of you on their internally pre-existing stereotypes and notions, they'll also base their perception of your home on your behavior. So you become sort of like a harbinger of all of Russia. Everybody's very excited to talk about that one Russian friend they have who drinks like a sailor and lives in Moscow, and whether or not you know him by any chance. Oh, and you still get the "dumb" treatment, just with other issues on top.
And you're probably reading this thinking "that's bullshit, I don't do that", and it's good if you don't, but there's also something I like to call a White Savior Complex: Extended Cut. It's when a good native-speaking samaritan decides to be your all-time language teacher, and I swear they're sometimes even worse because they think themselves so noble and awesome for helping you that they don't hesitate talking down both to you and about you, like hey, this is my friend Misha, his language skills are terrible so I'll be speaking in his stead 99% of the time, isn't that wonderful!
That's the kind of experience no person would subject themselves to willingly. The only reason I don't try to get rid of my accent is because it's a somewhat rare cultural mash-up that I want to preserve, but I swear most of the time it would make my life so much easier if people treated me the way they treat native speakers.
Now, that, of course, is not a universal experience, and you may have it differently, but that's my opinion. I don't think Heavy would pretend to be non-fluent on purpose, unless it's some kind of ruse, like Medic's "German tourist" gig for organ-harvesting.
Do his mistakes sound artificial to me? Not really. When trying to purposefully make mistakes, as I do when I write Heavy, I mostly think in terms of my native language anyway. Mistakes made on purpose and mistakes made accidentally tend to be the same if the person making them is basing them on their native language.
Hope this answers your question. Let me know if you need any further clarification, and have fun writing!
24 notes
·
View notes
Last Seen Blogs




