#like calling people into work physically who are at risk for COVID complications
Text
#JamesDonaldson On #MentalHealth - Why So Many Long #Covid #Patients Are Reporting #SuicidalThoughts
How Vaccination Affects the Risk of Long #COVID
Photo by Edward Jenner on Pexels.com
BY JAMIE DUCHARME
Last year, Diana Berrent—the founder of Survivor Corps, a Long #COVID support group—asked the group’s members if they’d ever had thoughts of #suicide since developing Long #COVID. About 18% of people who responded said they had, a number much higher than the 4% of the general U.S. #adult population that has experienced recent #suicidalthoughts.
A few weeks ago, Berrent posed the same question to current members of her group. This time, of the nearly 200 people who responded, 45% said they’d contemplated #suicide.
While her poll was small and informal, the results point to a serious problem. “People are suffering in a way that I don’t think the general public understands,” Berrent says. “Not only are people mourning the life that they thought they were going to have, they are in excruciating pain with no answers.”
Long #COVID, a chronic condition that affects millions of #Americans who’ve had #COVID-19, often looks nothing like acute #COVID-19. Sufferers report more than 200 symptoms affecting nearly every part of the body, including the neurologic, cardiovascular, respiratory, and gastrointestinal systems. The condition ranges in severity, but many so-called “long-haulers” are unable to work, go to #school, or leave their homes with any sort of consistency.
The statistics around Long #COVID and #mentalhealth are striking. A report published in eClinical Medicine last year found that about 88% of Long #COVID #patients experienced some form of mood or emotional issue during the first seven months of their illnesses. Another study, published in BMC Psychiatry in April, found that people with post-#COVID conditions were about twice as likely to develop #mentalhealthissues including #depression, #anxiety, or #posttraumaticstressdisorder as people without them. #COVID-19 survivors were also almost 50% more likely to experience #suicidalideation than people who hadn’t had the #virus, according to a study published in February in the BMJ.
Exploring the body-brain connection of Long #COVID
Understanding the link between Long #COVID, #suicide, and #mentalhealthissues is more complicated than it might seem. While some people do develop #depression, #anxiety, or other #mentalhealthissues after their diagnoses, others are suffering from physical symptoms that have psychological side effects or that are mistaken for #mentalhealthproblems, experts say.
The #virus that causes #COVID-19 has well-documented effects on the brain, which can potentially result in psychiatric and neurologic symptoms, says Dr. Wes Ely, who treats Long #COVID #patients at Vanderbilt University Medical Center. “We’ve been collecting brains of some #patients who didn’t survive Long #COVID,” he says. “We’re seeing inflammation and ongoing cellular abnormalities in these brains.”
Those changes to the brain can have profound effects, possibly including #suicidalthinking and #behavior. “There is a high probability that symptoms of psychiatric, neurological and physical illnesses, as well as inflammatory damage to the brain in individuals with post-#COVID syndrome, increase #suicidalideation and #behavior in this #patient population,” reads a January 2021 article in QJM: An International Journal of Medicine. Research published as a preprint last year (meaning it had not been peer-reviewed) also found differences between “post-#COVID #depression” and typical #depression, including higher rates of #suicidalbehavior—suggesting “a different disease process at least in a subset of individuals.”
Long #COVID can also be incredibly painful, and research has linked chronic physical pain to an increased risk of #suicide. Nick Güthe has been trying to spread that message since his wife, Heidi Ferrer, died by #suicide in 2021 after living with Long #COVID symptoms for about a year. Among her most disruptive symptoms, Güthe says, were foot pain that prevented her from walking comfortably, tremors, and vibrating sensations in her chest that kept her from sleeping. More than 40% of Long #COVID #patients experience moderate-to-severe sleep disturbances, according to recent research, and insomnia has been linked to suicidal thinking and #behavior.
“My wife didn’t kill herself because she was depressed,” Güthe says. “She killed herself because she was in excruciating physical pain.”
Since speaking out about his wife’s death, Güthe has heard from numerous families with similar experiences. Recently, he says, he’s noticed a grim change. “I used to get contacted by people on #socialmedia who were suicidal,” he says. “Now I’m getting reports of suicides. I had three in the last week.”
During that time, there’s been little tangible progress for long-haulers. #Doctors still don’t understand much about the condition or how to treat it. “You’ve got people now who have been suffering with Long #COVID for almost two years,” Güthe says.
Part of the problem is that in the U.S., illnesses are typically considered either physical or mental, but not both, says Abigail Hardin, an assistant professor of psychiatry and behavioral sciences at Rush University who works with seriously ill #patients, including those with Long #COVID. “In reality, all of these things are actually very bidirectional,” she says. “Everything is integrated.”
In part because the medical system often fails to accommodate that complexity, many chronic-disease #patients are misdiagnosed or assigned labels that don’t capture the full reality of their conditions.
Myalgic encephalomyelitis/chronic fatigue syndrome, a post-viral condition so similar to Long #COVID that many long-haulers meet its diagnostic criteria, is one example. Decades ago, #doctors widely and incorrectly believed that patients’ symptoms—including crushing fatigue, often exacerbated by physical #activity—were all in their heads. Even today, ME/CFS #patients—as well as those with similar conditions, like chronic Lyme disease and fibromyalgia—are often misdiagnosed with #mentalhealthissues because their providers don’t understand their conditions. #Suicide is also disproportionately common among people with ME/CFS, research shows.
Adriane Tillman, who has had ME/CFS for a decade and works with the advocacy group #MEAction, remembers trying to get #doctors to understand the extent of her physical symptoms, which at first kept her bedridden—only to be diagnosed with #depression.
While Tillman was grieving for the life she’d led before she got sick, she says reducing her debilitating condition to #depression was too simplistic. “I just thought, okay, I’m not explaining this enough,” she says. “I brought my husband . I brought my dad. I brought a Powerpoint presentation.” Still, the best she got was an increased dose of antidepressants.
Many Long #COVID #patients report similar experiences. Teia Pearson faced disbelief from #doctors and loved ones after developing Long #COVID following a March 2020 case of #COVID-19. “The doctor’s calling you crazy. Your family and friends are…treating you like you’re crazy. That really messes with your head,” she says.
Jaime Seltzer, director of scientific and medical outreach at #MEAction, says research on #mentalhealth needs to better account for the realities of chronic illness. For example, many #depression screening questionnaires ask if the individual struggles to get out of bed in the morning, but fail to distinguish between feeling unable to get up and being physically unable to get up. “Until we have a #depression scale and an #anxiety scale for people who are physically disabled…people with physical disabilities will continue to be misinterpreted as depressive or anxious even when they are not,” Seltzer says.
#James Donaldson notes:Welcome to the “next chapter” of my life… being a voice and an advocate for #mentalhealthawarenessandsuicideprevention, especially pertaining to our younger generation of students and student-athletes.Getting men to speak up and reach out for help and assistance is one of my passions. Us men need to not suffer in silence or drown our sorrows in alcohol, hang out at bars and strip joints, or get involved with drug use.Having gone through a recent bout of #depression and #suicidalthoughts myself, I realize now, that I can make a huge difference in the lives of so many by sharing my story, and by sharing various resources I come across as I work in this space. #http://bit.ly/JamesMentalHealthArticleOrder your copy of James Donaldson's latest book,#CelebratingYourGiftofLife:From The Verge of Suicide to a Life of Purpose and Joy
www.celebratingyourgiftoflife.com
A need for solutions
Berrent says there’s an immediate need for a #suicidehotline specifically for people with Long #COVID, since operators at other services may not know about or understand the condition. More research into Long #COVID treatments would also go a long way, she says, because it would give people hope as well as eventual relief from their often-devastating symptoms.
Marissa Wardach, whose ex-husband John died by #suicide in March after developing Long #COVID the prior summer, wishes there had been more options available to him. When he spoke with #doctors, she says, “they kind of just shrugged it off and said, ‘Sorry, we don’t really know much about it,’” she remembers. “That shattered any kind of hope he had.”
Wardach wonders how things might have gone if clinicians had referred John to specialty treatment centers or #patient support groups, rather than sending him on his way. But even when #patients are connected to the relatively few Long COVID treatment centers that exist, they often face months-long waits for an appointment. “Long #COVID #patients feel they’ve been abandoned, in many circumstances,” Ely says. “There are too many the country where there’s not a Long #COVID clinic.”
Emerging evidence about what does seem to work for #patients also isn’t always shared widely among #doctors. Güthe, for example, learned from a #physician months after his wife’s death that a drug called trazodone may have helped her sleep despite her chest vibrations—something her own #doctors didn’t mention. “Every general practitioner in the #UnitedStates should be up to date on the basic guidelines for helping #patients with Long #COVID deal with the major symptoms,” he says.
Seltzer says all #doctors and #mentalhealthpractitioners also need a better understanding of what will—or will not—help people with Long #COVID and other similar chronic diseases. Approaches like #cognitivebehavioraltherapy, which focus on changing thought patterns, often aren’t helpful for #patients with very real physical symptoms, she says. “Clinicians need to be aware that this is a thing, and they need to not be dismissive about it,” Seltzer says. They need to “not attribute it to stress, and therefore place the responsibility on the #patient to calm themselves down, and not attribute it to an incorrect manner of thinking.”
These shortcomings point to structural issues in the U.S. medical system, Hardin says. Ideally, physical and psychological care wouldn’t be treated as distinct, and patients could get holistic evaluations from any provider. At the very least, she wishes each person diagnosed with a chronic condition had a #mentalhealthprofessional on their care team from the very beginning. But, she says, that’s less common than it should be.
“So much of what we’re seeing with #COVID and the fallout of it is not related to individual providers,” she says. “A lot of it is very structural. This is an opportunity for the country to grow and fix some of the systemic issues that have been under the surface of U.S. medicine.”
If you or someone you know may be contemplating suicide, call the #NationalSuicidePreventionLifeline at 1-800-273-8255 or text HOME to 741741 to reach the Crisis Text Line. In emergencies, call 911, or seek care from a local hospital or #mentalhealth provider.
Photo by Edward Jenner on Pexels.com
Read the full article
0 notes
Text
COVID LONG-HAULERS FACE HURDLES IN LTD BENEFIT CLAIMS: TIPS FOR APPLICATIONS
Based on information from the World Health Organization which has been repeated to us time and time again through the media, we have come to understand that 80 percent of those infected with COVID-19 will experience only mild symptoms or be entirely asymptomatic and will recover after only two weeks, while the elderly and those with pre-existing medical conditions are more likely to suffer serious complications and possibly, death. However, many of these reported statistics fail to consider the growing number of people who are reporting serious, long-lasting and debilitating effects of the virus, weeks and months after infection. These individuals are now commonly referred to as “long-haulers”.
Unofficially, long-haulers are commonly characterized as those that have been sick with symptoms of COVID-19 for one month or more and continue to experience the impact of the virus in every aspect of their daily functioning. The number of so-called long-haulers is still unknown, however, in the U.S., estimates have been in the tens of thousands. According to what little is still known about long-haulers, it appears that most are previously fit and healthy women with an average age of 44. Often they report having experienced only mild symptoms of the infection initially and may not have been tested for COVID-19 (due to not meeting the early criteria or having the symptoms required for testing) or they may have tested negative for the virus (due to waiting too long to be tested or for some other cause for false-negative test results). (Long-Haulers Are Redefining COVID-19, The Atlantic, August 19, 2020)
Long-haulers report symptoms commonly associated with COVID-19, including fever, cough, and shortness of breath. However, they also report experiencing an ever-growing list of other serious symptoms including gastrointestinal, cardiac and neurological problems (such as hallucinations, delirium, short-term memory loss), as well as vibrating sensations when they touch surfaces and problems with their sympathetic nervous system (which controls unconscious processes like heartbeats and breathing). They may feel out of breath when their oxygen levels are normal and feel their heart racing when their EKG readings are normal. They often describe “brain fog” and intense fatigue and anxiety and depression. Many of their symptoms may come and go and vary in severity over time.
Unfortunately, given the nature of their symptoms, long-haulers may be faced with skepticism from their friends, family, employers, doctors and their LTD insurance companies. How could they have one set of symptoms one day and an entirely different set of symptoms the next? How could some of their symptoms become more severe over time, rather than improve? These are questions that go directly to a long-hauler’s credibility and put them at risk of misdiagnosis by healthcare providers and/or denial of LTD benefits by their LTD insurance companies.
Long-haulers face a myriad of hurdles; physical, emotional and financial. Their issues are complicated and difficult to navigate; particularly given the nature and extent of their physical and cognitive impairment. When they are told that their symptoms are “all in their head” or caused by stress or anxiety, they are left to feel alone and helpless to deal with the issues before them. They may feel frustrated by the lack of recognition that they are suffering and limited in their functioning. Their relationships with family and friends may suffer and their employment relationships may deteriorate if they are not able to work or not able to meet their employers’ expectations.
For long-haulers, this might be the first time they have experienced serious financial, emotional and medical issues. However, these same struggles are not new for a vast number of chronic pain and chronic fatigue sufferers who have been struggling to be seen and heard by the medical community and also by their LTD insurance companies, for decades.
For those unable to work due to conditions such as myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and complex regional pain syndrome, including fibromyalgia, LTD benefit disputes are all too common. There is a long history of insurance companies denying LTD benefit claims on the basis of there being no “objective” evidence of disability or no “objective” evidence to support the severity of a condition. Insurance companies are notorious for denying claims where the only evidence of disability is subjective, meaning there are no tests that confirm the nature or severity of the condition and the only basis for the LTD claim are self-reported symptoms and functional abilities. Long-haulers, particularly those who do not have a positive COVID-19 test result in hand, will undoubtedly struggle in proving disability to their LTD insurance companies.
If it becomes clear that you are not able to work due to COVID-19 related symptoms, even long after you became infected, you may have the option to claim Short-Term (STD) and Long-Term Disability benefits, either pursuant to an individual (or private) insurance policy or under your group insurance policy with your employer.
To be eligible for LTD benefits under most group benefit plans, you must satisfy various terms and conditions in your insurance policy. The terms may vary between policies, however, generally, you must satisfy the insurance company (or benefit plan administrator for STD) that you are “unable to perform the essential duties of your own occupation for the initial period of disability (usually 24 months) and thereafter, you are unable to perform the duties of any (gainful) occupation”. There will be other conditions of payment, such as getting appropriate treatment, attending independent medical assessments, and participating in insurance sponsored rehab programs.
If you are self-employed, you might have your own individual (or private) LTD policy. These policies vary greatly with respect to what benefits are available to you and corresponding eligibility requirements. In addition to benefits for “total disability”, you might also have coverage for “partial disability” and “residual disability”. There might also be various benefits related to business loss, in the event that you become disabled. Generally, you will need to demonstrate that you are disabled for the purpose of the benefit you are applying for. This may mean that you will need to prove that you are not able to work at all or it may mean that your condition prevents you from working full-time or from performing some of your usual duties.
Whether you are claiming disability benefits under a group or individual policy, the insurance company will require you to provide proof or evidence of disability. Long-haulers, just like those suffering from chronic fatigue, chronic pain and mental health-related conditions, will only have subjective evidence of disability; what they report to their doctors and other healthcare providers. Therefore, it is important that the self-reported symptoms, restrictions and limitations that are relied on as the basis of the LTD claim are corroborated and confirmed by other means.
Long-haulers can benefit from the lessons learned by those suffering similar symptoms who have been successful in their LTD claims or in their LTD lawsuits. Since there may be no blood test, x-ray or other objective measures to explain the severity of long-haulers’ conditions, they must rely on other means to persuade the insurance companies to approve their LTD claims.
If you are suffering the ongoing effects of COVID-19 infection and you are not able to work, we encourage you to consider the following tips for applying for LTD benefits:
THE THREE MOST IMPORTANT TIPS FOR APPLYING/APPEALING AN LTD CLAIM FOR LONG-HAULERS
Functionality is key.
Always focus your answers and remind your doctor(s) to focus answers to questions on forms and in telephone calls, on your functioning; that is what you can and can not do, as a result of your symptoms. This is what the insurance company should be most concerned with in assessing your LTD claim.
Many people believe that a diagnosis is necessary to be successful in an LTD claim. Often with long-haulers it takes a long-time to get a diagnosis and sometimes the cause of your symptoms might never be determined or you might even be misdiagnosed. Approval for LTD does not hinge on a specific diagnosis; it’s all about whether you meet the definition of disability under the plan/policy.
In terms of meeting the definition of disability, it will help your LTD claims representative to know what the duties of your “own occupation” are and what specifically prevents you from performing those duties. For example, pain and fatigue may prevent you from standing, walking, sitting, concentrating, remembering, communicating, regulating emotions, etc. These are all functions you might need for your job. Therefore, the insurance company needs to understand that your symptoms prevent you from doing both the physical and cognitive demands of your job on a consistent basis or at all.
Treatment is critical.
While treatment is extremely important for you, medically, it is also important for proving your LTD claim. This holds true for all LTD claims, but especially so for claims for long-haulers. The nature and extent of your treatment tells the insurance company a lot about the severity of your condition, about your self-reported restrictions and limitations, and about your credibility. When all you have to rely on is what you are telling your doctors, you need another means to support your claim. Treatment is one of the best ways to prove to your insurance company that you are not able to do your job and that you are not malingering or exaggerating your condition.
Follow your doctor’s orders; meaning you should be filling prescriptions, attending specialists’ appointments, getting investigations done (such as x-rays, blood tests, MRI’s, medical assessments, etc.), regularly attending recommended or prescribed therapies (such as physical therapy, massage, acupuncture, cognitive behavioural therapy, group therapies, etc.), and following your doctors’ recommendations regarding your functional limitations and restrictions (such as, trying to go on walks, not overdoing it, rest as needed, limiting bending, walking, sitting, etc.). Do not be afraid to advocate for yourself by researching your condition and talking to your doctor about possible referrals or treatments.
Your insurance company is more likely to be convinced of the severity of your post-COVID-19 condition and of your self-reported functional restrictions and limitations if there are medical records that document a history of self-reporting that is consistent with what your doctors observe (and which might be observed in the insurance company’s surveillance).
If your family doctor has referred you for countless tests and investigations and to various specialists, that would suggest that your doctor believes you and believes that your condition is so severe as to warrant these investigations and referrals. Specialist reports will lend additional credibility and validity to your self-reports, as they will also be consistent with what your family doctor and you are reporting. It should be clear to the insurance company, from all the testing and appointments and treatments that you are not choosing to be disabled. Who would opt to spend their days going from doctor to doctor and being poked and prodded and undergoing often painful (emotionally and physically) treatments, if they could work and earn their full salary?
Credibility can make or break a claim.
When completing forms or speaking with the insurance company representative who is assessing your claim, remember to be open and honest. You should also be careful not to be overly optimistic about your return to work or overstate your actual functional abilities. You should include all of your symptoms in your claim and explain the waxing and waning of those symptoms.
Remember, it is not unreasonable to assume that the insurance company wants to pay legitimate claims. Since you are legitimately struggling with your functioning, be clear about what you can not do, but also be clear on what you can do. You do not need to be bedridden everyday or in a hospital to be eligible for LTD benefits. You must only satisfy the insurance company that you are not able to do the essential duties of your “own occupation” or after the initial period (usually 24 months), that you are not able to do the duties of “any occupation”. (Note: the definitions of disability in your policy might be slightly different.)
If the insurance company finds a medical record or conducts surveillance and finds inconsistencies in what you have reported to them versus what you are doing in the “real world” or what you have reported to your doctors, your credibility comes into question and your claim becomes that much more difficult to prove.
Overstating your abilities or optimism for your recovery can be relied on by the insurance company to deny or terminate your claim. It may be difficult to admit to ourselves and others that we are not doing well and that we are not coping as well as we would like. While optimism and positivity may be key to recovery or key to living with a disabling condition, your insurance company could easily misconstrue these sentiments and use them as a basis for denying/terminating your claim or initiating rehabilitation and return to work efforts, well before you are ready.
YOU MAY STILL NEED OUTSIDE HELP TO PROVE YOUR “INVISIBLE CONDITION”
Applying for LTD for a condition stemming from COVID-19 infection is a difficult task, at the best of times, and even more so when you are struggling with the symptoms of your disability. It is important that you get help where you can to ensure that your application is complete, accurate and most of all, persuasive to your insurance company to increase the likelihood that your claim will be approved and to avoid the stress of appealing or litigating a denial.
From decades of experience litigating LTD claims from both sides (as in-house counsel for insurance companies defending LTD claims and as plaintiff’s counsel, representing disabled persons in their complex LTD disputes with all insurance companies in Canada), we know that the type of LTD claims that will be made for long-haulers (such as those for chronic pain, chronic fatigue and mental health conditions) are the most common types of claims that are denied or later, terminated. We understand why these claims were not successful and how to persuade insurance companies of their legitimacy and resolve these disputes for our disabled clients.
Together, our three law partners have over 50 years of LTD litigation experience representing professionals, self-employed individuals and employees with conditions akin to those experienced by long-haulers. Based on that experience, we have put together the above list of the three most important tips for long-haulers applying for or appealing their LTD claims. It is our hope that our suggestions will increase the likelihood of these claims being approved early on, so that you can focus on your recovery without worrying as much about losing your income and other health-related benefits and possibly, your job.
HELP WITH YOUR STD OR LTD APPLICATION, APPEAL AND LITIGATION
We encourage you to contact us if your STD or LTD claim has been denied or terminated by your insurance company. We offer free consultations to help you decide whether to appeal the denial of your claim or whether to proceed straight to litigation. Remember, there is no requirement that you appeal the denial or termination of your STD/LTD claim. (Note: Unionized employees may be required to grieve STD and/or LTD denials/terminations, depending on the wording of their collective agreements. We are able to review collective agreements for jurisdiction over STD/LTD issues.)
As an added support, during this pandemic only, we are offering long-haulers free consultations at the sick leave/LTD application stage. If you are considering sick leave and/or applying for STD or LTD, we encourage you to contact MK Disability Lawyers to schedule a time for us to discuss the details of your disability claim. We will discuss the claims process with you, provide you with direction with respect to what to include in your initial claim and review your claim forms before you submit them. Every claim is different and it is important that you use wording and provide medical evidence that will be most supportive and persuasive to the insurance company and result in the approval of your claim.
We appreciate that there are a number of resources available to help you in your LTD claim application and appeal. Unlike many other resources provided by your employer and insurance company and union, we have the unique perspective that comes only from seeing and litigating countless LTD claims for conditions, such as those of experienced by long-haulers (and all variety of other medical conditions) that have been denied or terminated and we can use that insight and experience to help you avoid those outcomes. One of our partners, Courtney Mulqueen, also has the added insight that only comes from having worked for insurance companies defending LTD claims.
If you have specific questions about LTD, please contact us to schedule a free individual consultation. We also invite you to visit our website www.mkdisabilitylawyers.com, where you will find an extensive collection of blog articles about LTD, including our most recent articles:
“LTD and COVID-19: Applying for Disability Benefits During COVID-19,” “LTD and COVID-19: Mental Health Claims Related to the Pandemic” and “Struggling to Be Seen and Believed: Making an LTD Claim for an “Invisible Condition” and our “Guide to LTD for Union Representatives”, as well as other information related to applying LTD.
0 notes
Text
A workplace that tells you to “take care of you mental health” is a workplace reminding you that any loss of productivity due to stress or trauma will result in your unemployment.
#capitalism#watching my friends experience this in real time#being told to take time for mental health#by the same people giving them increasingly unrealistic demands#like calling people into work physically who are at risk for COVID complications#anticapialism#labour rights#ableism
2K notes
·
View notes
Text
My Universe: BTS & Coldplay’s Sci-Fi Music Video Explained
https://ift.tt/3im7ht2
BTS and Coldplay went fully, gloriously sci-fi in the music video for their collaboration, “My Universe.” In the new music video, released at midnight on September 30th, the two bands exist in a futuristic reality where music is forbidden. In spite of the ban, and with the help of a space DJ, the groups come together for a high-energy, galaxy-spanning performance of their new song.
The “My Universe” music video/short film is directed by Dave Meyers, an American filmmaker best known for his commercials and music videos, which include MVs for artists Drake, Ed Sheeran, Pink, Normani, Ariana Grande, and many, many more. High-concept, genre-driven music videos are par for the course in the visually immersive world of K-pop, but are less common in western music videos, which (save for some outliers, like Janelle Monae’s funky, political sci-fi adventures) have more “grounded,” realistic aesthetics, even when they skew fantastical. A great example of the latter is Harry Styles’ “Adore You” video. Also directed by Meyers—it has a speculative fiction premise in which Styles has a literally blinding smile, falls in love with a fish, and is able to power his sailboat using the winds of his jarred yells, but keeps its visuals down to Earth to tell its fairy tale-like story.
“My Universe,” on the other hand, embraces the science fiction aesthetics of working class space operas like Space Sweepers or Guardians of the Galaxy, with some (and I mean this as a compliment) Zenon: Girl of the 21st Century thrown in for good measure.
Rebellion is a popular theme in the space opera subgenre, and it’s one that “My Universe” embraces. The video is set in an intergalactic future in a place known where all music is banned. Three different bands—BTS, Coldplay, and a fictional alien supergroup called Supernova7—who live on three different plans defy the ban to create music together via hologram. They are hunted by The Silencers, who enforce the no-music status quo.
Most importantly, the music video doesn’t prioritize either Coldplay or BTS’ worlds. While we may visit Coldplay’s dry, graffitied planet first, where we first meet BTS in their holographic forms, we also go to BTS’ industrial-dystopia home, where Coldplay visits as holograms. The music video’s best moment, in fact, comes when we follow a flickering, holographic V from Coldplay’s planet back to his own, where he—and, with him, the six other members—bloom into more tangible form.
Read more
Culture
Squid Game Competitions, As Played By BTS
By Kayti Burt
TV
Did BTS Invent Star Trek?
By Kayti Burt
The design and CGI for the video is impressive and varied, though a little too busy to fully appreciate the stunning outer space visuals, Tron-esque spaceships interiors, and alien planet-scapes. The video includes visual callbacks to the official lyric video for “My Universe,” which is beautifully designed to feature the multi-colored English and Korean-language lyrics zooming through space. The colors and premise are also reminiscent of the video serial that was part of BTS’ Muster Sowoozoo Concert in June. In the story, the seven members of BTS make their way across an alien landscape in a camper van, searching for a safe place to meet ARMY. While the Sowoozoo serial was much cozier and more chill than “My Universe” video, I’d love to hear some good head canon about how these videos exist in the same fictional universe.
What Does the “My Universe” Music Video Mean?
Both the “My Universe” song and music video have a pretty broad, easy-to-get-behind concept. The love song is about a relationship that transcends boundaries. Thematically, the idea of coming together across divisions or differences is particularly poignant when performed by bands from different sides of the planet. This is reinforced by the decision to include Korean-language lyrics in the collaboration. BTS has proven themselves more than capable of singing in English. Three of their latest hits—”Dynamite,” “Butter,” and “Permission to Dance”—are all sung fully in the English language by the Korean band. However, BTS and Coldplay chose to feature Korean-language elements as an integral part of the collaboration, emphasizing the multicultural nature of the song and its message.
The music video doubles down on the theme of people coming together despite distance and differences. In it, BTS and Coldplay (and, OK, alien supergroup Supernova 7) are excited to collaborate. Together, they make something beautiful and special that brings them joy despite the seemingly dismal worlds that surrounds them both. Here, the enemy is not difference, but a mysterious, totalitarian force that has banned all music. Personified by “The Silencers,” this antagonist can be broadly interpreted by the societal prejudices that can sometimes keep up apart, but also by a pandemic that has made the most basic rituals of togetherness more complicated. It doesn’t seem a coincidence that the fictional versions of BTS and Coldplay featured in this video are unable to be together in person. It’s a representation of the forced physical distance that has come to define much of the past few years. It’s why seeing the bands find a way, despite their harsh reality, to share a joyful experience so damn inspiring.
While the visuals of “My Universe” may be intentionally futuristic, the ability to play together across vast swathes of space is not. Just last week, Coldplay and BTS performed as part of the Global Citizen Live event. The bands were in two different countries—Coldplay in NYC, and BTS back home in Seoul—but came “together” on stage. The seven members of BTS were featured as holograms on a backdrop as Chris Martin sang both English and Korean-language parts of the song. (The Korean-language rap sections performed by Suga and J-Hope were pre-recorded.) Coldplay notably traveled to Korea to record “My Universe” during the pandemic.
“My Universe” Music Video Ending Explained
The breakout character from the “My Universe” music video is arguably DJ Lafrique, played by actress Joe Diao. DJ Lafrique is the character who is able to bring Coldplay and BTS together, across the universe. She is the most powerful figure featured in this story, and her rebellion comes at a high risk. At the end of the video, The Silencers find DJ Lafrique’s ship, which is making the intergalactic jam session possible. The Silencers’ power up their Death Star-like weapon in preparation to take out DJ Lafrique. However, BTS and Coldplay are able to buy her time by rocking out even more intensely (as you do); she powers up her hyperdrive and blips away before The Silencers can silence her forever.
The ending works for the video; it would be jarring to watch a music video featuring BTS that doesn’t end with a message of hope. The Korean band’s full name, Bangtan Sonyeondan, can be translated as “Bulletproof Boyscouts,” and the group has always seen it as one of their primary missions to act as a buffer between young people and the harsh stereotypes and pressures they face. While the group has always worked to be a balm in a harsh world, this has especially been the case since the outbreak of COVID, which has brought with it unprecedented mental health challenges. In the wake of the global crisis, BTS has worked to be a comfort to their global fandom, known as ARMY. When they released album “Be” in November 2020, member Jin said during the accompanying press conference: “Our goal with the music on ‘BE’ is that it can be a comfort to a lot of people … If many people can relate to it, I will be really thankful.”
cnx.cmd.push(function() { cnx({ playerId: "106e33c0-3911-473c-b599-b1426db57530", }).render("0270c398a82f44f49c23c16122516796"); });
What did you think of “My Universe”‘s science fiction concept? Let us know in the comments below.
The post My Universe: BTS & Coldplay’s Sci-Fi Music Video Explained appeared first on Den of Geek.
from Den of Geek https://ift.tt/3kRPUSt
4 notes
·
View notes
Link
Zayner, who has a PhD from the University of Chicago, worked for NASA researching the terraforming of Mars, and is the inventor of a musical instrument called the Chromocord that creates sound when light reacts with bacteria, was and is one of the world’s leading “biohackers.” He defines the term to mean “constantly pushing the boundaries of science outside traditional environments,” which he certainly did in this case, taking a radical approach to combating longstanding intestinal troubles. In layman’s terms, his plan was to nuke his natural bacteria with antibiotics, and replace them with bacteria from the feces of others.
“I wanted to see if, by transplanting different bacteria in my body, they would change the way my gastrointestinal system was functioning,” is how he explains it now. “Because, at the time, it wasn't functioning very well.”
On that May, 2016 podcast, neither science reporter Liz Lopatto nor Arielle Duhaime-Ross, who wrote the story for The Verge, had much that was positive to say about either Josiah or his experiment. In fact, in an eerie preview of the anger of self-proclaimed “experts” that would become ubiquitous among pundits after the arrival of Covid-19, they sounded downright furious.
“Extremely dangerous, possibly stupid,” said Lopatto, of Josiah’s gambit.
“In his mind, it made sense to tell people about it, and inspire them to take their health into their own hands,” said Duhaime-Ross. “The risk of copycats is really real with this.”
“This is one of the things that does bug me about biohackers,” agreed a put-out Lopatto. “I don’t want people playing with pathogens in their bedrooms. Like, I’m not interested in that, personally, as a person who lives in this society.”
A less judgmental New York Times later produced a short film about the episode called Gut Hack:
Whether it’s Zayner gulping down a massive antibiotic cocktail in a WU-TANG FOREVER t-shirt, or repeatedly grimacing as he swallows home-crafted feces capsules in a hotel room, the short documentary is a parade of scenes make your eyeballs pop out in shock and amazement, cartoon-style. Zayner, by any measure, is an extraordinarily interesting character. He has a mind almost perfectly engineered against obedience: brilliant, fearless, and not accepting every assumption but checking the validity of each. He alternately bristles at or ignores judgment, seeming to draw inspiration from it in either case. At the end of Gut Hack, we see him standing on a subway platform, shaking his head as he listens to the two Verge journalists denounce him. We hear their audio:
“Not putting your life in danger unnecessarily is pretty basic,” they complain, adding that his experiment was “not even a blip in the scientific radar.”
“There’s a fine line,” Zayner later sighs to the Times, “between being crazy and knowledgeable.” He goes on to talk about growing up poor, and different, in the Midwest. “When you grow up on a farm, you have all this freedom,” he says. “We don’t have any neighbors or anyone to interact with, so we’re used to just doing what we want. And when you get to this environment were people don’t do that, you’re immediately pegged as, you know, a weirdo.”
Some weeks after, he’s shown feeling better, but he wants more than a placebo result. The film ends with him receiving the results of genetic sequencing tests that appear to show his “gut hack” experiment worked. He bursts into tears. The Times reporter asks, “Do you feel vindicated?”
He seems surprised by the question. No, he says, it’s not about that. “It’s one of those things,” he says, “where you’re so moved and impressed by how science works.”
Zayner went on to claim his battle with irritable bowel syndrome had been won, only to be replaced by a new malady. “My physical signs of IBS were gone,” he said recently. “But so was my privacy. This is when the deplatforming began.”
Around the same time Gut Hack was being made, Zayner founded ODIN, which he describes as “a company that sells science and genetic engineering supplies to people so that they can do science experiments in their homes.”
ODIN’s product line, which includes CRISPR gene-editing kits, seems designed to give ordinary people the tools to experience science as Zayner does, almost more as artistic expression than means to any end. He describes his Chromacord, for instance, as “something more purely inspirational, just outside the average notion of what science even is. In a manner of speaking, it was simply magic.” Or, as he said in another interview, “People having access to this technology allows them to do crazy and cool shit.”
Unfortunately, after the notoriety he gained from Gut Hack, bringing the “magic” of genetic engineering to the layperson suddenly proved a little beyond what science-journalism scolds or the faceless executives at tech platforms felt comfortable allowing.
Amazon and Facebook began delisting his products, and Patreon, PayPal, and Square all shut him down in short order. Sometimes he was told why, sometimes he wasn’t. He was forced to move on, and doesn’t want to jinx his relationship with his current payment processor by mentioning their name.
In between, the State of California brought a case against him on the somewhat preposterous charge of practicing medicine without a license. He won, but California state authorities were so peeved that they passed a law appearing to target his company alone, declaring that firms must append their wares with labels announcing “not for self-administration,” if they’re in the business of selling home “gene-therapy kits.”
In a piece called “Don’t Change Your DNA At Home,” the MIT Technology Review noted with amusement that, even if one includes ODIN, “We’re not sure any such kit exists.” The sponsor of the law, Republican State Senator Ling Ling Chang, appeared to think ODIN’s products were a lot more Frankensteinian and terrifying than they are.
“It was really weird,” Josiah says now. “It’d be like, I don’t know, labeling a computer: ‘You shouldn’t eat this computer.’ I mean, obviously.” Regarding ODIN’s home experimentation kits, he adds, “How would you use it on humans? I don’t even understand. I guess somebody crazy enough could just take some of the DNA that we sell and try to inject it into their body, but it wouldn’t even work in humans because it was meant for other organisms.”
Zayner didn’t comply with the law, and instead just moved to Austin, Texas (“Land of the free, home of the brave,” he laughs) and set up shop there. Then Covid-19 arrived, and Zayner’s biohacking got him in trouble again.
In May, 2020, he read a scientific paper that claimed a DNA-based vaccine against Covid-19 had been successfully developed and tested on macaques.
“I was like, ‘Why isn’t anybody working on this or trying this?’ Why don’t I go and order up the same DNA vaccine, have the company produce it for me and actually test it and see if it works on humans?” he said. “It worked on monkeys.”
Zayner followed through on his idea, contracting with a company to make the vaccine described in the paper. Then he and two other scientists/bio-hackers live-streamed the process of injecting themselves with it. He claims they all had antibody responses, but even at the time — his experiment was covered by Bloomberg — he said, “I’m very suspicious of my own data.” Here is how he describes the results, and his thinking, in a recent essay:
I’m hesitant to say it worked because vaccines are complicated and we’d need further testing to confirm our results. But, even if it didn't work, the fact that someone could have designed a vaccine, and contracted a company to manufacture that vaccine in June 2020 for under $5k is fucking profound — and that is what, at the time of releasing our video, I felt people needed to know.
At the time, there was no action taken against him. But just as mRNA vaccines began to be distributed across America and other parts of the world, he abruptly received notice from YouTube that he’d been banned for “severe or repeated violations of our community guidelines.”
1 note
·
View note
Video
youtube
What Will it Take to Create a Vaccine for COVID19?
April 29, 2020, 3:30 p.m. — One of the big challenges in navigating the COVID-19 crisis is the novelty of the virus. Because it’s so new, we don’t have any way to prevent infection — and without a vaccine, there’s no telling how long the pandemic will last. So what will it take to get a COVID-19 vaccine available to the public? And why is it taking so long?
What we know about COVID-19
Viruses operate by attaching themselves to living cells in our body and injecting their genetic material, called RNA. The RNA hijacks the machinery of the cell to replicate itself, producing copy after copy of the virus, which eventually explode out of the cell to go in search of new cells to infect. In the case of SARS-CoV-2, the virus primarily attacks the epithelial cells lining the lungs. In the lungs, the fight between your immune system and the virus can cause inflammation, cell death and excess fluid, a combo that leads to pneumonia. Sometimes, when the infection is really bad, patients end up with acute respiratory distress syndrome, or ARDS, when their lungs are so clogged up that their bodies aren’t able to absorb enough oxygen and they really struggle to breathe.
There’s also evidence that the virus, and/or the inflammation it causes, might be having effects on other organs in the body, causing long term complications including brain, liver, kidney, and heart damage and increased risk of blood clots.
Protection against a viral illness is conferred by antibodies, produced by the immune system in response to exposure to the virus. In most cases, contracting the virus gives the immune system the information it needs to produce those antibodies, which can then activate and fight the virus on the next exposure.
What it takes to develop a vaccine
Vaccines take advantage of our natural immune system response to stimulate antibody production against a disease using killed or weakened versions of the pathogen that don’t make us sick. This makes us immune to the disease without ever having to contract it.
The first step in creating a vaccine is to identify a good antigen to target. These molecules represent portions of the virus’ structure that don’t cause illness by themselves but do activate the immune system to produce the correct antibodies. These antigens are then produced in large quantities by cells in Petri dishes before being purified and, if necessary, the virus is inactivated or killed so it can be safely injected. Finally, the antigen is mixed with adjuvants, to help enhance the immune response to produce stronger immunity, alongside preservatives and stabilizers to give the vaccine a long shelf life and allow for multiple doses from the same vial.
Once a vaccine has been created, it has to be extensively tested: first in animal models, and eventually in human beings. This process goes through three phases, to be sure that the vaccine is safe and effective, and to determine what dose should be administered to patients. It takes a lot of testing to be sure that the vaccine is safe in children, adults, pregnant people, and the elderly. And not every vaccine is recommended for every person. Different governments have to balance cost, risk, efficacy, and public health concerns before deciding whether or not they should add a new vaccine to the standard vaccination list.
Usually, it takes 10 to 15 years to develop a vaccine and get it approved by the FDA for use in patients. The exception are seasonal vaccines, like the flu vaccine. Because the flu virus is tracked year-round by scientists, and because the manufacturing process is kept the same year-to-year, researchers are able to use the same foundation for each year’s vaccine and simply replace the antigen with the new virus.
In the case of SARS-CoV-2, because of the high rates of infection and novelty of the virus, it seems critical that we get a vaccine ready quickly, but it’s not as easy just swapping in a new antigen. Thanks to a lot of technological advancement in recent years, and the large number of industrial and academic researchers working on this problem, we’re moving faster than ever toward a vaccine solution for COVID-19.
What’s already happening on the vaccine front?
The SARS-CoV-2 genetic sequence was published on January 11, 2020, allowing for a global flurry of vaccine development, and the first vaccine entered human clinical trials on March 16. By April 8, 115 vaccines candidates were being tested by academic research institutions and industry companies, with 78 of those candidates being close to formal testing. Several of those have already advanced into clinical testing, with several others hoping to follow within the next several months.
The rapid speed of vaccine development is thanks to a wide diversity of technology platforms, testing a variety of potential sources for stimulating the immune response, including peptides, viral vectors, recombinant proteins, and nucleic acids (DNA and RNA). Researchers are also working to develop adjuvants that will produce the most effective vaccines. Most of these vaccines are being tested in the United States and in China, with some development in Europe, Australia, and other areas in Asia.
What we still need to know and do
We still need to figure out some key details about the SARS-CoV-2 virus. One big question that we haven’t answered yet is whether or not exposure to the virus, or to viral antigens, is enough to generate immunity to the virus. The evidence so far suggests that people who have contracted COVID-19 are protected against reinfection, at least temporarily.
Some cases have indicated that patients who experience a more severe infection of the virus may have more antibodies against it, which may provide better protection against future illness. But it’s still unclear if contracting the virus provides any lasting immunity against it, or how long that immunity might last. At this point, virologists believe that immunity is limited; after 1 to 2 years, patients may be susceptible to a new infection, and require a vaccine to protect against it.
Another question is whether or not COVID-19 is at risk of mutating to become more deadly. At this stage, we just don’t know enough about the virus and its behavior to be certain one way or the other, though some experts doubt that there is a high risk of this happening.
Until some of these vaccines have gone through further clinical testing, we won’t know which ones are actually viable candidates for the public. Part of the challenge is the fact that most vaccines require years of testing in the community, where trial participants receive the vaccine or receive a placebo and then go about their daily lives to see if they end up contracting the virus. Because of the drastic impacts of COVID-19 on our lives and economy, some scientists are suggesting that we consider clinical trials where healthy volunteers are given the vaccine and deliberately exposed to SARS-CoV-2 to see how effective the vaccine might be. This could shave months off the development timeline, but is highly controversial due to the obvious risks for trial participants.
So when will we have a vaccine?
With all of these projects underway, scientists think a vaccine may be approved for emergency use by the FDA as soon as 2021. “Emergency use” means that a vaccine has been tested in humans and found to be effective at preventing infection, but hasn’t been subjected to the full, rigorous scrutiny of a traditional vaccine. It will take more time for all of this extensive testing to be completed — likely several more years.
Despite recent technological advances, this means it will still be at least a year before we have a viable vaccine. With that in mind, the CDC and other public health officials continue to recommend that we follow physical distancing, hand washing and mask-wearing guidelines. It’s important that we continue to work together to protect the health of our friends, family, and community by following stay-at-home recommendations as doctors and scientists work not only on developing a vaccine, but also at better understanding how the virus works and figuring out the most effective ways to treat it.
For more information on what we’re doing at UC San Diego Health, please visit health.ucsd.edu/COVID
— Alison Caldwell, PhD, Bigelow Science Communication Fellow
#covid-19#covid 19#novel coronavirus#coronavirus#sars-cov-2#vaccine#immunology#infectious disease#public health#clinical trials#vaccine protocol#vaccine production#stay at home#flatten the curve#pandemic#hand washing#hand hygiene#shelter in place#self quarantine#quarantine#social distancing#science#medicine#academic medicine#ucsd#uc san diego
59 notes
·
View notes
Link
However, the order does override state orders to suspend operations. And it gives the producers a big fat liability shield. From Mother Jones:
But here’s a theory. Already, 20 meatpacking and food-processing workers have died from COVID-19, and more than 5,000 have contracted the disease, according to the United Food and Commercial Workers International Union. What if workers and their families start suing, claiming that the companies’ practices made them sick? Already, one worker—at a Smithfield plant in Milan, Mo.—filed a lawsuit claiming management was not sufficiently protecting workers from the risk of COID-19, and demanding that it follow Centers for Disease Control and Prevention guidelines.
A president invoking the Defense Production Act to require meatpacking firms to keep their plants running during outbreaks would provide a “solid basis” for shielding the firms from suits like this, said Jennifer Zwagerman, director of Drake University’s Agricultural Law Center. She noted that Walmart was recently sued for wrongful death by the family of a worker who died from COVID-19 complications.
And from Reason:
The big deal in the executive order and interpretations of it may be about meat processing plant liability for employee exposure. From [U.S. Solicitor of Labor Kate S.] O’Scannlain and [OSHA Principal Deputy Assistant Secretary Loren] Sweatt’s statement:
Courts often consider compliance with OSHA standards and guidance as evidence in an employer’s favor in litigation. Where a meat, pork, or poultry processing employer operating pursuant to the President’s invocation of the DPA has demonstrated good faith attempts to comply with the Joint Meat Processing Guidance and is sued for alleged workplace exposures, the Department of Labor will consider a request to participate in that litigation in support of the employer’s compliance program. Likewise, the Department of Labor will consider similar requests by workers if their employer has not taken steps in good faith to follow the Joint Meat Processing Guidance.
Even CBS worked out that the worker safety bits were a headfake; relevant agencies merely issued guidance.
Mike Elk’s PayDay report seems to be the only outlet covering Covid-19 strikes; his map now shows 153. Yesterday, Nebraska meatpackers struck. From Elk’s account:
It’s unclear how Trump intends to use the Defense Production Act to force meat packing processing workers back into the assembly line.
Organized labor immediately denounced the move.
“We only wish that this administration cared as much about the lives of working people as it does about meat, pork, and poultry products. When poultry plants shut down, it’s for deep cleaning and to save workers’ lives,” said Stuart Applebaum, president of Retail, Wholesale, and Department Store Union. “If the administration had developed meaningful safety requirements early on as they should have and still must do, this would not even have become an issue.”…
Shortly after Trump announced his intention to issue his executive order, more than 50 meatpackers walked off the job after 48 co-workers tested positive for COVID-19 at Smithfield’s plant outside of Lincoln, Nebraska…
The Nebraska action follows a wildcat strike Monday night at Pilgrim’s Pride meatpacking plant in Cold Spring, Minn.
Another meatpacker facing coronavirus pushback in JBS. In Green Bay, 189 coronavirus cases have been linked to its facility there. Elk informs us that JBS is playing hardball:
At a JBS meatpacking plant in Greely, Colo., 5 workers have died of COVID-19 [6 as of April 30] and at least 100 workers have tested positive for the virus.
However, now JBS is threatening to sue the UFCW because of the negative media attention that they have received.
From KUSA in Denver:
JBS has sent a cease-and-desist letter to the union that represents its workers, arguing that it “has adopted a strategy of generating negative media attention and public opinion” to gain concessions from the company while it battles an outbreak of the novel coronavirus at its Greeley meatpacking plant.
They provided a copy of that letter to the 9NEWS by United Food and Commercial Workers Local 7 on Tuesday, and a rebuttal from the union’s president, Kim Cordova.
“Unfortunately, your cease and desist letter, threatening to stifle our voice, and those of our members, as well as pursuing claims for unfounded, speculative, and unrecoverable damages is rife with numerous inaccuracies, suppositions, and erroneous conclusions won’t spend time rebutting in their entirety,” Cordova wrote.
Have no doubt that that’s also meant to deter the Green Bay workers from making noise.
Trump has threatened to use the National Guard to replace strikers; Elk reports that Democratic Governor Tom Wolfe has called in the National Guard to replace nurses who walked out of a nursing home to demand better safety protections after 19 residents died. I wonder how much appetite members of the National Guard would have for the backbreaking pace of meat processing plants.
Here’s a well argued take:
Nebraska Governor Pete Ricketts suggested yesterday that workers at meat packing facilities should face loss of unemployment benefits unless they returned to work. This follows on the heels of President Trump’s announcement that he would invoke the Defense Production Act to reopen closed plants in an effort to protect the nation’s food supply-chain. Plants, regardless of safety, will be opened and workers will be coerced with loss of UI benefits so that Americans can get their pork, chicken, and beef in a timely fashion.
Don’t get me wrong. I like meat as much, and probably more, than the next guy and will start getting nervous when these products aren’t in my local grocery store’s refrigerator case. But this one-two policy punch from the White House and Governor Ricketts has a few problems with it. These plants are out of operation not because workers have refused to do their jobs but because of serious COVID-19 outbreaks that forced their closure. There have been hundreds of cases of COVID-19 associated with these facilities and a number of deaths. The counties where the plants are located are becoming their own hot-spots in the unfolding disease crisis. Cramped working conditions and hard physical labor seem to lend themselves to efficient viral transmission.
There’s an even darker side to the situation, though. Somewhere between 30 and 50 percent of the meat-packing workforce is made up of undocumented workers from Mexico, Guatemala, and El Salvador as well as immigrants from East African nations. As Smithfield Foods’ statement on the Sioux Falls outbreak indelicately put it, the living conditions of these immigrants are “different than they are with your traditional American family.” Get it? They are in overcrowded houses with inadequate sanitation. “They” aren’t like “us”. Since many — perhaps a majority — of them lack legal status, they are unable to defend themselves against exploitative or coercive labor practices. As recently as last August, ICE agents were rounding them up by the hundreds for deportation.
We need to make up our minds on a number of issues. On the one hand, we shower praise on “essential workers” in hospitals, grocery stores, sanitation and other occupations. On the other, we engage in acts of economic coercion with vulnerable populations who do some of the dirtiest, most difficult, and most dangerous work around. We build a fence along our southern border to keep out illegal immigrants but then seek to force those who are already here to do jobs American citizens simply will not do.
Why so coy about the source? It’s from Brent Orrell….at the American Enterprise Institute. That American Enterprise Institute. Orrell, at one of the bastions of “free market” ideology, gives a more straightforward statement in support of meatpacking plant workers than I have yet to see from any Democrat.
54 notes
·
View notes
Text
Anonymous asked: I really enjoy your cultured posts and especially about wine. I never knew that Roger Scruton wrote about wine! You tantalisingly talked in bits and pieces in past posts about your chateau vineyard in France. I understand why you protect your privacy but can you say a bit more. I was also hoping as a wine connoisseur you can explain to me what wine sommeliers in restaurants mean about wine having ‘terroir’? Are they just making stuff up to look down on us poor saps or is there something to it?
Your experience with the sommelier reminded me of the classic British television comedy, ‘Fawlty Towers’, where John Cleese’s perpetually hard pressed hotel owner, Basil Fawlty, says with his usual sarcasm, “I can certainly see that you know your wine. Most of the guests who stay here wouldn’t know the difference between Bordeaux and Claret.”

I’m sorry that you had from what I can surmise bad experiences with sniffy sommeliers when it came to appreciating wine. I have had one or two depressing experiences myself but it’s important to call out such rudeness so that others don’t have their dining experience spoiled. In Paris at least I can honestly say the spectre of the rude sommelier is dying out - and I have eaten in many great restaurants where I’ve had very lovely experience chatting with sommeliers versed in their wines.
These days sommeliers are positively jumping for joy if you show any kind of wine literacy. Don’t forget these men (and women) have worked extremely hard to hone a refined sense of their craft and they just want to share that knowledge and wisdom with you - otherwise it goes to waste.
Everyone likes to be appreciated and so I go out of my way to listen and appreciate their recommendations based on what I like or if I am looking to pair something interesting with the food I have ordered. If I don’t know I just ask. Indeed often I do know but I still ask because I’m curious to know if there is a better choice of wine and also because I want to learn. There is no shame in asking. Remember they are there to guide you to have the best dining experience in their restaurant. So engage with them with kind civility and your palate will thank you. And tip generously (if applicable).
I do indeed have a chateau vineyard in southern France - south of Paris anyway. But it’s not just mine. I invested in a dream that belonged to my two cousins who are the real wine connoisseurs. Out of their request for discretion I don’t talk too much about it here on this blog (they follow my blog). I can say that I admire both my cousins hugely (I get brownie points for saying that) for their hard work, risk taking, passion, and their artisanal flair.
Both my cousins gave up lucrative corporate careers to follow their dream to owning and managing a small vineyard. In this case it was bought from the family of my cousin’s French wife; her very old traditional family had the vineyard for generations. They had fought off French revolutionaries who wanted to burn down their chateau because of their old roots but they managed to prevail and survive. They barely survived the Great French Wine Blight (the Phylloxera infestations) that was a severe blight of the mid-19th century that decimated many of the vineyards across France. But times change. It’s not a romantic business but an unforgiving one. So rather than sell up to rapacious Chinese investors and other outsiders they instead sold it to us.

I have my day job and that keeps me extremely busy. My two cousins (and their French wives) manage the whole vineyard with other hired staff. They make all the decisions and I do the drinking (for quality control purposes, naturally). I help out when I can. This could be from business marketing advice or attending a few wine merchant trade shows. I often go to Shanghai and Hong Kong for my corporate work and my Chinese is passable; and so I help out my cousins who might be out there when I am there too. In fact one of my cousins was out in Shanghai just before the Wuham Covid 19 outbreak in China; thankfully he got out fine and didn’t suffer any symptoms after his trip.
More fun for me is actually spending time on the vineyard. Call me weird but I really do look forward to rolling up my sleeves and getting down in the dirt. It’s incredibly back breaking work - pruning or harvesting - but very rewarding because we’re all in it together. The camaraderie is immense.
I love escaping into the countryside and I just enjoy the easy bonhomie and companionship of my cousins and their French partners for whom wine is a passion and a way of life. Besides learning a lot more about wine, I also get to run, cycle, and hike in the surrounding hills, a world away from crazy city life.
Like many vineyards in France (and indeed vineyards around the world) the Coronavirus has made it an even more challenging environment to produce and sell wine. We did a lot of business in China and now, like many others, we’ve taken a hit. But we’re not down for the count. We’re fortunate that we are more robust with what we have in place. But like everyone else uncertainty of the future with an expected recession means we need to dig in deep and weather the oncoming storms. But we’ll be fine.

So what is this odd French word, ‘terroir’?
The French have this expression they use when it is clear they are tasting a true terroir wine - "un goût de terroir" - a taste of the place.
Terroir is a largely misused term, though the general understanding of the term of terroir is correct that it refers to the place of where the wine is made. Terroir is not something you pick up after tasting a few wines from one vineyard. It's more complicated than that, which of course makes it harder to use. Which is no fun, because people really like saying fancy French words when talking about wine.
A classical definition of terroir would be something along the lines of this: terroir is the aggregate factors that affect the physical vineyard site: geography, geology, weather, and any other relatively unique environmental conditions that might affect the process or final quality of the fruit.
Put simply terroir is the combination of micro-climate, soil, sun exposure, weather conditions and other environmental influences on wine. To Europeans in general and to the French and Italians in particular, terroir is a key indicator of quality in wine.

The best way to understand what what terroir means is to think of terroir as a different accent - an English accent sounds different from a Scottish accent which sounds different from a Welsh accent. Although the English language is the same, these accents have their own sense of place. Once you are fluent in the language of wine these different accents start to become a lot more pronounced. These ‘wine accents’ echo the terroir where the grapes were grown and the wines were made.
So what does this mean in practice? Take the Pinot Noir grape. Pinot Noir is a notoriously difficult grape to grow because it is very fussy with climate. With the grape being so fussy it is remarkable that the grape can be grown in many parts of the world. Its home is in Bourgogne (Burgundy), France, and yet the grape is grown successfully in Germany (where it's called Spatburgunder), Italy, United States, New Zealand and Australia, among others. So while Pinot Noir is a very fussy grape, it can grow in different climates. It's just the the way it expresses itself can be vastly different. This starts with fruit, whereby it will express a wide range from red fruits like cranberry (cooler climates) right through to black fruits like plum (warmer climates).
The key is the soil - and the sweat and blood that goes into cultivating it.
Soils contain a huge array of types of rock, decomposed rock, and organic materials, in a seemingly infinite array of mixes of topsoil, subsoil, and bedrock. Grape vines tend to grow vigorously and this causes a tendency toward better wines emerging from counterintuitive places - places with relatively poor soils. Too many nutrients and too much water near the surface and the vines will not push down deeply into the ground, seeking out what it needs to live. The belief is, if it does so it will find a more complex variety of nutrients that lead to better, more nuanced wines.
Soil, however, is not the only facet that gives us a full sense of what terroir means.
It is not enough to have a great mix of soils. Vines grown for grapes have a range on Earth in which they will ripen. Champagne, for example, is near the northern ripening limit for growing grapes — around the 49th parallel. They usually do not achieve anywhere near full ripeness nor do they want it - they need lots of acidity - so a northern location works well for their purposes. Too far south, however, and relentless sun and warmth will yield over ripened, jammy, sometimes stewed tasting fruit, lacking acidity and possessing searing levels of alcohol, at times. So the parallel on which the vines are planted is important.

Next, prevailing weather patterns in the region, such as adequate, but not typically heavy rain is necessary. The further north the vineyard site, the more that frosts and hail will likely be factors in varietal planting decisions, as well as harvesting. Achieving full ripeness before vinification is generally the goal for winemakers, but in certain climates the likelihood of sudden rain and weather changes which would dilute or damage the fruit, all go into the perception of the terroir.
Where the vines are planted, even within a commune in Burgundy, can prove very important for several of the reasons listed above: a southeast facing slope in the Côtes de Nuits, for example, provides a poor soil (meaning a good soil for wine grapes,) making the roots grow down deep into limestone, searching for nutrients. The top of the slope to the vineyard's back creates a microclimate and gives a small rain shadow effect, potentially dropping a major portion of rain on the western slope away from the quickly-harvesting vignerons on the other side, before their crop becomes diluted or destroyed. Not to say it always works out this way, because it does not. The point here is that the position within the mesoclimate and even microclimate is important.
Further, the angle or aspect toward the sun in our example is tremendously important. In our example, facing southeast gives the grapes a higher average number of hours per day to ripen in the sun, without getting the stronger, sometimes-harsher evening sun directly. When there is rain, rot can be a problem which leads to yet another factor - slope. A well-drained soil is very important, and altitude is a factor, which will lead to variation throughout a vineyard on such a slope.

Finally, a very important factor in terroir that is not always mentioned is the hand of man.
In the local customs for wine growing, winemaking, cuisine around those wines, and traditions sometimes dating back thousands of years, there emerges a tendency to understand what works well in the local soil and climate. Based on those ideas, certain decisions are made in the cellars that nudge the wine in the direction of one style or another. Decisions can be made that completely mask - destroy - the sense of terroir. Yet decisions are made, nonetheless. They do influence the final product.
Two producers owning parts of the same few hectares of land produce products of two wildly different qualities. There are decisions to be made of using wild yeasts or cultivated yeasts, steel tanks or oak barrels, the type(s) of oak, where it is from, the amount of toasting.

A poor vineyard manager can plant vines in impeccable terroir, but fail miserably in their ability to farm the grapes appropriately, even assuming they planted the right grapes for that terroir. Equally, you can give an inexperienced winemaker the best grapes from the best terroir and he is still very likely to make a mediocre wine at best.
Now, this isn't to say that a great winemaker can take substandard grapes from a poor region and turn them into great wine. But it takes a knowledgable and experienced winemaker to make the best of the spectacular grapes that world-class terroir and impeccable farming technique provides.
So all in all, I would say that terroir, vineyard manager and winemaker are equally as important and there can be no weak links in that equation if quality wine is to be produced.
The point is that all of these factors affect the wine. The best winemakers are artisans who work hard to let the land and vines speak. Over time, some places on Earth have been identified as having very high potential to produce outstanding, unique wines that sing with a voice like no other. That is terroir.

Music is like wine. We appreciate different composers and their pieces more as we understand more of the context of each piece.
Most wine drinkers, no matter their level of knowledge and sophistication, are on a similar path of evolving understanding. Each mouthful whose flavours and aromas we drink, each bottle label we unconsciously imprint in our memory, each line-item on a wine list that we select for the evening’s meal is another volume in our own library of experience, and determines how we will experience the next. The more wine we drink and the more we learn, the better context we have to evaluate (or enjoy) every future glass. So wine drinking is not a race nor is there a prize. You go at your own pace. It’s your own journey of self-discovery. Ignore the pretentious twattery that so often hinders the enjoyment of good wine.
May I add wine enjoys companionship. It makes love to fine food and good conversation. Yes, wine can be drunk on its own but it is more than just a balm to the soul. It is best appreciated when shared or paired - as one might with a cigar and a whisky - with good food. In the words of the late Paul Bocuse, who was a celebrated Michelin starred chef and father of French Haute Cuisine, “La véritable cuisine sera toujours celle du terroir. En France le beurre, la crème et le vin en constitueront toujours les bases.”
Thanks for your question
#question#ask#wine#personal#vineyard#drinking#sommelier#wine making#terroir#french#france#grape#culture#food#life#family
28 notes
·
View notes
Text
Unfair
In Manitoba, there has been two major lockdowns that affected gyms and fitness centres. The first one was from March 13 to June 1 of 2020, and the second one was from November 12 2020 to February 12 2021. These forced closures shut down facilities, hurt consumer confidence, and has taken away an environment where members become healthy. COVID-19 patients may have a deleterious health outcome. These outcomes include cerebrovascular disease, acute organ damage, permanent lung damage, and chronic fatigue. If a patient is obese, already has a chronic condition such as diabetes, or is in their senior years, these negative health outcomes often lead to death, let alone a higher frequency of poor prognosis.
There is always inherit risk when engaging in purposeful physical activity, exercise, or sport. The benefits of being physically active far and wide outweigh any risk, which is why we encourage the general population to do so. Fitness centres and the like offer their members a wide range of equipment to use without worrying about maintenance, controlled environments, plenty of mirrors, and availability of professional advice. It fosters a sense of community in-itself; people exercise for all kinds of different reasons and everyone tends to be respectful of each other’s goals. Not to mention, those at risk from COVID-19 complications may benefit the greatest by being physically active. A stronger heart, increased blood vessel elasticity, healthier lungs, reduction in blood pressure leading to less stress on your kidneys, all of it.
The closure of gyms has a wide-sweeping effect on society. Trainers and other employed staff face job insecurity. Business owners have hard lines financially that lead them to close shop permanently. Unfortunately, I was not able to get any hard numbers to back these up. If you look at your own community, you may have seen these types of closures, or have heard of trainers who lost their position and are looking for a way to make ends meet. Members deal with the psychological drawbacks of losing the health and fitness that they dedicate their time and invest their money in. Home workouts are definitely a viable option, there are lots of apps and generalized exercise prescriptions out there. But participants may loathe exercising alone, be limited by equipment availability, or foster a mindset that they aren’t able to get an effective workout.
Surveys time and time again find that most of everyone want to head back to get their membership. Before that happens, there are issues with consumer confidence that needs to be addressed. A negative feedback loop is developing from the forced or permanent closure of gyms, leading people to lose their faith in the viability of the industry. This won’t change until certain things happen, such as the Provincial Government not constantly hinting that the lockdown is always on the table. Another point that needs to be called out hard is the myth that training centres are petri dishes for the virus. The numbers indicate that fitness centres are rarely ever the case. There was a sensationalized case from the Province of Quebec, and there were two or three separate events in Winnipeg back last Autumn. Even with these national news stories and government postings, gyms are responsible for a fraction of a fraction of COVID-19 cases. Once again, data is hard to come by, and an internet engine search will lead you to news about events in other countries. EuropeActive have conducted their own study1, so I will cite them in this case. They worked out some numbers, that is, the number of visits to fitness centres in the Continent of Europe and positive cases linked to them. The ratio of visits to infections, rounded up, is A MILLION TO EIGHT. Fitness Centres are as clean as they ever were. Patrons are respectful. We are doing above and beyond what is asked of us, and the powers that be think we do not deserve our place in society. It’s not just here, it’s everywhere.
All that I would like to have happen is no third shut-down of the fitness industry. It simply doesn’t make sense to do so. If you want a chance to ease the public health burden, let us do our job. There is work to be done out there, with no time to waste. Trying to demonize a profession whose only care is keeping their community healthy is as disingenuous as it is unfair.
Thank you for reading this out. Any support goes a long way. Stay awesome, and I’ll see you around.
1. Fernandez, C. (2020). SafeACTiVE Study – Preliminary results showing extremely low levels of Covid-19 risk in fitness clubs. EuropeActive. October 27, 2020. https://tinyurl.com/b43c3tma
1 note
·
View note
Text
BE PREPARED FOR THE FLU SEASON
Older people and those with long term illnesses have increased risk of more serious problems from flu and are also more vulnerable to COVID-19. Both can cause pneumonia, so getting them at the same time could wreak havoc on your lungs. Fortunately, many of the same things that prevent COVID-19 will also help protect against cold or flu (and we should be doing them whenever we get cold or flu symptoms, Coronavirus or otherwise). Here are eight things you can do to stay healthy this cold and flu season (and help keep your loved ones and more vulnerable people in your community safe too):
1. Get the flu jab
Getting the flu vaccine is the best thing you can do to reduce your chance of getting the flu; and if you do get the flu, your symptoms will likely be milder and not last as long compared with people who don’t get the vaccine. The flu vaccine is especially important for people who are at increased risk of health complications, like people 65 and over, pregnant women, people with chronic health issues such as diabetes, heart disease, lung conditions, and neurological diseases. This link from the Department of Health has a more complete list of who the vaccine is recommended for and who can get it for free under the National Immunisation Program. If you’re over 65, there’s a specific flu vaccine recommended for you, but it’s not available from all providers, so call ahead to check.
While the flu vaccine won’t protect against COVID-19, it will reduce the risk of the double whammy of getting both the coronavirus and flu at the same time.
2. Wash and dry your hands
Just like with coronavirus, regularly washing your hands for at least 20 seconds with soap and water is one of the best ways to reduce your risk. If you touch a surface in a public place, try not to touch your eyes, nose or mouth without washing your hands first. If you don’t have access to soap and water you can use an alcohol-based hand sanitizer (look for at least 60% ethanol or 70% isopropanol).
3. Keep your distance
By now you’ve probably heard that you should aim to leave about a metre and a half of space between yourself and other people to reduce the risk of coronavirus. The same advice applies to reducing your chances of catching the flu (or passing it on before you realise you’re contagious).
4. Stay home when you’re unwell
If you have flu-like symptoms, stay home and try to keep space from the people you live with to reduce the chance of passing it on. Wait until you’re well to have visitors over or return to work or school.
5. Clean shared spaces
Clean and disinfect frequently touched surfaces like benches, doorknobs and door handles, tables, fridge doors and toilets regularly. You can use regular household detergent and water to clean, but check the label on disinfectant to make sure it is antiviral and not just antibacterial.
You may want to also wipe down your phone, keyboard and other objects that are touched regularly and could be harbouring viruses.
6. Don’t share germs (or personal items where they like to live)
During cold and flu season it’s worth taking some extra care to avoid spreading viruses. Don’t share drinks, cutlery, glasses, toothbrushes or towels. Cough into your elbow or a tissue (that you immediately toss out) rather than your hand.
7. Support your body’s natural defence system
A strong immune system is the first line of defence against infections such as cold and flu. When you’re healthy and well, your body does a better job at fighting off viruses.
• Make sure you get enough sleep. For most of us that’s about seven to eight hours. For more tips on how to get a good night’s sleep, check out this resource.
• Try to find healthy ways to manage stress. This may mean you need to identify sources of stress in your life and ways to reduce it, such as delegating more, practicing saying no, or coming up with ideas to reduce conflict. Learning relaxation techniques such as controlled breathing, and strategies such as meditation or mindfulness can also help you cope better, as can regular exercise. A mental health professional can also help you learn ways to manage stress better, so reach out if you need more support. It’s much easier to keep up a healthy lifestyle when you’re mentally well. If you’re a Medibank member with hospital cover* you can call 1800 644 325 to speak to a mental health professional for confidential support, advice or information.
• Get your body moving. Physical activity can help reduce stress hormones. Aim for at least 30 minutes of exercise on most days of the week. If you’re not used to it, build up slowly.
• Eat nutritious meals with plenty of vegetables, fruit, whole grains and legumes.
• If you smoke, consider quitting. Smoking, or regularly breathing in smoke at home or work makes you more likely to develop infections and experience more severe illness. Support, whether from a free service like Quitline® or your GP, increases the chance you’ll be successful. Encourage family members who smoke to try to quit as well. Contact Quitline® on 13 78 48 or quitnow.gov.au.
8. Be prepared
Flu can come on suddenly, and the less often you leave your house with symptoms, the less likely you are to pass it on to others. So you may want to have some essentials on hand: tissues, medicines to help relieve symptoms, ingredients for a soothing drink such as hot lemon, honey and ginger, and a few favourite meals in the freezer, such as a nourishing soup or stew you can eat as you start to recover.
1 note
·
View note
Text
#JamesDonaldson On #MentalHealth - Why So Many Long #Covid #Patients Are Reporting #SuicidalThoughts
How Vaccination Affects the Risk of Long #COVID
Photo by Edward Jenner on Pexels.com
BY JAMIE DUCHARME
Last year, Diana Berrent—the founder of Survivor Corps, a Long #COVID support group—asked the group’s members if they’d ever had thoughts of #suicide since developing Long #COVID. About 18% of people who responded said they had, a number much higher than the 4% of the general U.S. #adult population that has experienced recent #suicidalthoughts.
A few weeks ago, Berrent posed the same question to current members of her group. This time, of the nearly 200 people who responded, 45% said they’d contemplated #suicide.
While her poll was small and informal, the results point to a serious problem. “People are suffering in a way that I don’t think the general public understands,” Berrent says. “Not only are people mourning the life that they thought they were going to have, they are in excruciating pain with no answers.”
Long #COVID, a chronic condition that affects millions of #Americans who’ve had #COVID-19, often looks nothing like acute #COVID-19. Sufferers report more than 200 symptoms affecting nearly every part of the body, including the neurologic, cardiovascular, respiratory, and gastrointestinal systems. The condition ranges in severity, but many so-called “long-haulers” are unable to work, go to #school, or leave their homes with any sort of consistency.
The statistics around Long #COVID and #mentalhealth are striking. A report published in eClinical Medicine last year found that about 88% of Long #COVID #patients experienced some form of mood or emotional issue during the first seven months of their illnesses. Another study, published in BMC Psychiatry in April, found that people with post-#COVID conditions were about twice as likely to develop #mentalhealthissues including #depression, #anxiety, or #posttraumaticstressdisorder as people without them. #COVID-19 survivors were also almost 50% more likely to experience #suicidalideation than people who hadn’t had the #virus, according to a study published in February in the BMJ.
Exploring the body-brain connection of Long #COVID
Understanding the link between Long #COVID, #suicide, and #mentalhealthissues is more complicated than it might seem. While some people do develop #depression, #anxiety, or other #mentalhealthissues after their diagnoses, others are suffering from physical symptoms that have psychological side effects or that are mistaken for #mentalhealthproblems, experts say.
The #virus that causes #COVID-19 has well-documented effects on the brain, which can potentially result in psychiatric and neurologic symptoms, says Dr. Wes Ely, who treats Long #COVID #patients at Vanderbilt University Medical Center. “We’ve been collecting brains of some #patients who didn’t survive Long #COVID,” he says. “We’re seeing inflammation and ongoing cellular abnormalities in these brains.”
Those changes to the brain can have profound effects, possibly including #suicidalthinking and #behavior. “There is a high probability that symptoms of psychiatric, neurological and physical illnesses, as well as inflammatory damage to the brain in individuals with post-#COVID syndrome, increase #suicidalideation and #behavior in this #patient population,” reads a January 2021 article in QJM: An International Journal of Medicine. Research published as a preprint last year (meaning it had not been peer-reviewed) also found differences between “post-#COVID #depression” and typical #depression, including higher rates of #suicidalbehavior—suggesting “a different disease process at least in a subset of individuals.”
Long #COVID can also be incredibly painful, and research has linked chronic physical pain to an increased risk of #suicide. Nick Güthe has been trying to spread that message since his wife, Heidi Ferrer, died by #suicide in 2021 after living with Long #COVID symptoms for about a year. Among her most disruptive symptoms, Güthe says, were foot pain that prevented her from walking comfortably, tremors, and vibrating sensations in her chest that kept her from sleeping. More than 40% of Long #COVID #patients experience moderate-to-severe sleep disturbances, according to recent research, and insomnia has been linked to suicidal thinking and #behavior.
“My wife didn’t kill herself because she was depressed,” Güthe says. “She killed herself because she was in excruciating physical pain.”
Since speaking out about his wife’s death, Güthe has heard from numerous families with similar experiences. Recently, he says, he’s noticed a grim change. “I used to get contacted by people on #socialmedia who were suicidal,” he says. “Now I’m getting reports of suicides. I had three in the last week.”
During that time, there’s been little tangible progress for long-haulers. #Doctors still don’t understand much about the condition or how to treat it. “You’ve got people now who have been suffering with Long #COVID for almost two years,” Güthe says.
Part of the problem is that in the U.S., illnesses are typically considered either physical or mental, but not both, says Abigail Hardin, an assistant professor of psychiatry and behavioral sciences at Rush University who works with seriously ill #patients, including those with Long #COVID. “In reality, all of these things are actually very bidirectional,” she says. “Everything is integrated.”
In part because the medical system often fails to accommodate that complexity, many chronic-disease #patients are misdiagnosed or assigned labels that don’t capture the full reality of their conditions.
Myalgic encephalomyelitis/chronic fatigue syndrome, a post-viral condition so similar to Long #COVID that many long-haulers meet its diagnostic criteria, is one example. Decades ago, #doctors widely and incorrectly believed that patients’ symptoms—including crushing fatigue, often exacerbated by physical #activity—were all in their heads. Even today, ME/CFS #patients—as well as those with similar conditions, like chronic Lyme disease and fibromyalgia—are often misdiagnosed with #mentalhealthissues because their providers don’t understand their conditions. #Suicide is also disproportionately common among people with ME/CFS, research shows.
Adriane Tillman, who has had ME/CFS for a decade and works with the advocacy group #MEAction, remembers trying to get #doctors to understand the extent of her physical symptoms, which at first kept her bedridden—only to be diagnosed with #depression.
While Tillman was grieving for the life she’d led before she got sick, she says reducing her debilitating condition to #depression was too simplistic. “I just thought, okay, I’m not explaining this enough,” she says. “I brought my husband . I brought my dad. I brought a Powerpoint presentation.” Still, the best she got was an increased dose of antidepressants.
Many Long #COVID #patients report similar experiences. Teia Pearson faced disbelief from #doctors and loved ones after developing Long #COVID following a March 2020 case of #COVID-19. “The doctor’s calling you crazy. Your family and friends are…treating you like you’re crazy. That really messes with your head,” she says.
Jaime Seltzer, director of scientific and medical outreach at #MEAction, says research on #mentalhealth needs to better account for the realities of chronic illness. For example, many #depression screening questionnaires ask if the individual struggles to get out of bed in the morning, but fail to distinguish between feeling unable to get up and being physically unable to get up. “Until we have a #depression scale and an #anxiety scale for people who are physically disabled…people with physical disabilities will continue to be misinterpreted as depressive or anxious even when they are not,” Seltzer says.
#James Donaldson notes:Welcome to the “next chapter” of my life… being a voice and an advocate for #mentalhealthawarenessandsuicideprevention, especially pertaining to our younger generation of students and student-athletes.Getting men to speak up and reach out for help and assistance is one of my passions. Us men need to not suffer in silence or drown our sorrows in alcohol, hang out at bars and strip joints, or get involved with drug use.Having gone through a recent bout of #depression and #suicidalthoughts myself, I realize now, that I can make a huge difference in the lives of so many by sharing my story, and by sharing various resources I come across as I work in this space. #http://bit.ly/JamesMentalHealthArticleOrder your copy of James Donaldson's latest book,#CelebratingYourGiftofLife:From The Verge of Suicide to a Life of Purpose and Joy
www.celebratingyourgiftoflife.com
A need for solutions
Berrent says there’s an immediate need for a #suicidehotline specifically for people with Long #COVID, since operators at other services may not know about or understand the condition. More research into Long #COVID treatments would also go a long way, she says, because it would give people hope as well as eventual relief from their often-devastating symptoms.
Marissa Wardach, whose ex-husband John died by #suicide in March after developing Long #COVID the prior summer, wishes there had been more options available to him. When he spoke with #doctors, she says, “they kind of just shrugged it off and said, ‘Sorry, we don’t really know much about it,’” she remembers. “That shattered any kind of hope he had.”
Wardach wonders how things might have gone if clinicians had referred John to specialty treatment centers or #patient support groups, rather than sending him on his way. But even when #patients are connected to the relatively few Long COVID treatment centers that exist, they often face months-long waits for an appointment. “Long #COVID #patients feel they’ve been abandoned, in many circumstances,” Ely says. “There are too many the country where there’s not a Long #COVID clinic.”
Emerging evidence about what does seem to work for #patients also isn’t always shared widely among #doctors. Güthe, for example, learned from a #physician months after his wife’s death that a drug called trazodone may have helped her sleep despite her chest vibrations—something her own #doctors didn’t mention. “Every general practitioner in the #UnitedStates should be up to date on the basic guidelines for helping #patients with Long #COVID deal with the major symptoms,” he says.
Seltzer says all #doctors and #mentalhealthpractitioners also need a better understanding of what will—or will not—help people with Long #COVID and other similar chronic diseases. Approaches like #cognitivebehavioraltherapy, which focus on changing thought patterns, often aren’t helpful for #patients with very real physical symptoms, she says. “Clinicians need to be aware that this is a thing, and they need to not be dismissive about it,” Seltzer says. They need to “not attribute it to stress, and therefore place the responsibility on the #patient to calm themselves down, and not attribute it to an incorrect manner of thinking.”
These shortcomings point to structural issues in the U.S. medical system, Hardin says. Ideally, physical and psychological care wouldn’t be treated as distinct, and patients could get holistic evaluations from any provider. At the very least, she wishes each person diagnosed with a chronic condition had a #mentalhealthprofessional on their care team from the very beginning. But, she says, that’s less common than it should be.
“So much of what we’re seeing with #COVID and the fallout of it is not related to individual providers,” she says. “A lot of it is very structural. This is an opportunity for the country to grow and fix some of the systemic issues that have been under the surface of U.S. medicine.”
If you or someone you know may be contemplating suicide, call the #NationalSuicidePreventionLifeline at 1-800-273-8255 or text HOME to 741741 to reach the Crisis Text Line. In emergencies, call 911, or seek care from a local hospital or #mentalhealth provider.
Photo by Edward Jenner on Pexels.com
Read the full article
0 notes
Text
COVID LONG-HAULERS FACE HURDLES IN LTD BENEFIT CLAIMS: TIPS FOR APPLICATIONS
Based on information from the World Health Organization which has been repeated to us time and time again through the media, we have come to understand that 80 percent of those infected with COVID-19 will experience only mild symptoms or be entirely asymptomatic and will recover after only two weeks, while the elderly and those with pre-existing medical conditions are more likely to suffer serious complications and possibly, death. However, many of these reported statistics fail to consider the growing number of people who are reporting serious, long-lasting and debilitating effects of the virus, weeks and months after infection. These individuals are now commonly referred to as “long-haulers”.
Unofficially, long-haulers are commonly characterized as those that have been sick with symptoms of COVID-19 for one month or more and continue to experience the impact of the virus in every aspect of their daily functioning. The number of so-called long-haulers is still unknown, however, in the U.S., estimates have been in the tens of thousands. According to what little is still known about long-haulers, it appears that most are previously fit and healthy women with an average age of 44. Often they report having experienced only mild symptoms of the infection initially and may not have been tested for COVID-19 (due to not meeting the early criteria or having the symptoms required for testing) or they may have tested negative for the virus (due to waiting too long to be tested or for some other cause for false-negative test results). (Long-Haulers Are Redefining COVID-19, The Atlantic, August 19, 2020)
Long-haulers report symptoms commonly associated with COVID-19, including fever, cough, and shortness of breath. However, they also report experiencing an ever-growing list of other serious symptoms including gastrointestinal, cardiac and neurological problems (such as hallucinations, delirium, short-term memory loss), as well as vibrating sensations when they touch surfaces and problems with their sympathetic nervous system (which controls unconscious processes like heartbeats and breathing). They may feel out of breath when their oxygen levels are normal and feel their heart racing when their EKG readings are normal. They often describe “brain fog” and intense fatigue and anxiety and depression. Many of their symptoms may come and go and vary in severity over time.
Unfortunately, given the nature of their symptoms, long-haulers may be faced with skepticism from their friends, family, employers, doctors and their LTD insurance companies. How could they have one set of symptoms one day and an entirely different set of symptoms the next? How could some of their symptoms become more severe over time, rather than improve? These are questions that go directly to a long-hauler’s credibility and put them at risk of misdiagnosis by healthcare providers and/or denial of LTD benefits by their LTD insurance companies.
Long-haulers face a myriad of hurdles; physical, emotional and financial. Their issues are complicated and difficult to navigate; particularly given the nature and extent of their physical and cognitive impairment. When they are told that their symptoms are “all in their head” or caused by stress or anxiety, they are left to feel alone and helpless to deal with the issues before them. They may feel frustrated by the lack of recognition that they are suffering and limited in their functioning. Their relationships with family and friends may suffer and their employment relationships may deteriorate if they are not able to work or not able to meet their employers’ expectations.
For long-haulers, this might be the first time they have experienced serious financial, emotional and medical issues. However, these same struggles are not new for a vast number of chronic pain and chronic fatigue sufferers who have been struggling to be seen and heard by the medical community and also by their LTD insurance companies, for decades.
For those unable to work due to conditions such as myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and complex regional pain syndrome, including fibromyalgia, LTD benefit disputes are all too common. There is a long history of insurance companies denying LTD benefit claims on the basis of there being no “objective” evidence of disability or no “objective” evidence to support the severity of a condition. Insurance companies are notorious for denying claims where the only evidence of disability is subjective, meaning there are no tests that confirm the nature or severity of the condition and the only basis for the LTD claim are self-reported symptoms and functional abilities. Long-haulers, particularly those who do not have a positive COVID-19 test result in hand, will undoubtedly struggle in proving disability to their LTD insurance companies.
If it becomes clear that you are not able to work due to COVID-19 related symptoms, even long after you became infected, you may have the option to claim Short-Term (STD) and Long-Term Disability benefits, either pursuant to an individual (or private) insurance policy or under your group insurance policy with your employer.
To be eligible for LTD benefits under most group benefit plans, you must satisfy various terms and conditions in your insurance policy. The terms may vary between policies, however, generally, you must satisfy the insurance company (or benefit plan administrator for STD) that you are “unable to perform the essential duties of your own occupation for the initial period of disability (usually 24 months) and thereafter, you are unable to perform the duties of any (gainful) occupation”. There will be other conditions of payment, such as getting appropriate treatment, attending independent medical assessments, and participating in insurance sponsored rehab programs.
If you are self-employed, you might have your own individual (or private) LTD policy. These policies vary greatly with respect to what benefits are available to you and corresponding eligibility requirements. In addition to benefits for “total disability”, you might also have coverage for “partial disability” and “residual disability”. There might also be various benefits related to business loss, in the event that you become disabled. Generally, you will need to demonstrate that you are disabled for the purpose of the benefit you are applying for. This may mean that you will need to prove that you are not able to work at all or it may mean that your condition prevents you from working full-time or from performing some of your usual duties.
Whether you are claiming disability benefits under a group or individual policy, the insurance company will require you to provide proof or evidence of disability. Long-haulers, just like those suffering from chronic fatigue, chronic pain and mental health-related conditions, will only have subjective evidence of disability; what they report to their doctors and other healthcare providers. Therefore, it is important that the self-reported symptoms, restrictions and limitations that are relied on as the basis of the LTD claim are corroborated and confirmed by other means.
Long-haulers can benefit from the lessons learned by those suffering similar symptoms who have been successful in their LTD claims or in their LTD lawsuits. Since there may be no blood test, x-ray or other objective measures to explain the severity of long-haulers’ conditions, they must rely on other means to persuade the insurance companies to approve their LTD claims.
If you are suffering the ongoing effects of COVID-19 infection and you are not able to work, we encourage you to consider the following tips for applying for LTD benefits:
THE THREE MOST IMPORTANT TIPS FOR APPLYING/APPEALING AN LTD CLAIM FOR LONG-HAULERS
Functionality is key.
Always focus your answers and remind your doctor(s) to focus answers to questions on forms and in telephone calls, on your functioning; that is what you can and can not do, as a result of your symptoms. This is what the insurance company should be most concerned with in assessing your LTD claim.
Many people believe that a diagnosis is necessary to be successful in an LTD claim. Often with long-haulers it takes a long-time to get a diagnosis and sometimes the cause of your symptoms might never be determined or you might even be misdiagnosed. Approval for LTD does not hinge on a specific diagnosis; it’s all about whether you meet the definition of disability under the plan/policy.
In terms of meeting the definition of disability, it will help your LTD claims representative to know what the duties of your “own occupation” are and what specifically prevents you from performing those duties. For example, pain and fatigue may prevent you from standing, walking, sitting, concentrating, remembering, communicating, regulating emotions, etc. These are all functions you might need for your job. Therefore, the insurance company needs to understand that your symptoms prevent you from doing both the physical and cognitive demands of your job on a consistent basis or at all.
Treatment is critical.
While treatment is extremely important for you, medically, it is also important for proving your LTD claim. This holds true for all LTD claims, but especially so for claims for long-haulers. The nature and extent of your treatment tells the insurance company a lot about the severity of your condition, about your self-reported restrictions and limitations, and about your credibility. When all you have to rely on is what you are telling your doctors, you need another means to support your claim. Treatment is one of the best ways to prove to your insurance company that you are not able to do your job and that you are not malingering or exaggerating your condition.
Follow your doctor’s orders; meaning you should be filling prescriptions, attending specialists’ appointments, getting investigations done (such as x-rays, blood tests, MRI’s, medical assessments, etc.), regularly attending recommended or prescribed therapies (such as physical therapy, massage, acupuncture, cognitive behavioural therapy, group therapies, etc.), and following your doctors’ recommendations regarding your functional limitations and restrictions (such as, trying to go on walks, not overdoing it, rest as needed, limiting bending, walking, sitting, etc.). Do not be afraid to advocate for yourself by researching your condition and talking to your doctor about possible referrals or treatments.
Your insurance company is more likely to be convinced of the severity of your post-COVID-19 condition and of your self-reported functional restrictions and limitations if there are medical records that document a history of self-reporting that is consistent with what your doctors observe (and which might be observed in the insurance company’s surveillance).
If your family doctor has referred you for countless tests and investigations and to various specialists, that would suggest that your doctor believes you and believes that your condition is so severe as to warrant these investigations and referrals. Specialist reports will lend additional credibility and validity to your self-reports, as they will also be consistent with what your family doctor and you are reporting. It should be clear to the insurance company, from all the testing and appointments and treatments that you are not choosing to be disabled. Who would opt to spend their days going from doctor to doctor and being poked and prodded and undergoing often painful (emotionally and physically) treatments, if they could work and earn their full salary?
Credibility can make or break a claim.
When completing forms or speaking with the insurance company representative who is assessing your claim, remember to be open and honest. You should also be careful not to be overly optimistic about your return to work or overstate your actual functional abilities. You should include all of your symptoms in your claim and explain the waxing and waning of those symptoms.
Remember, it is not unreasonable to assume that the insurance company wants to pay legitimate claims. Since you are legitimately struggling with your functioning, be clear about what you can not do, but also be clear on what you can do. You do not need to be bedridden everyday or in a hospital to be eligible for LTD benefits. You must only satisfy the insurance company that you are not able to do the essential duties of your “own occupation” or after the initial period (usually 24 months), that you are not able to do the duties of “any occupation”. (Note: the definitions of disability in your policy might be slightly different.)
If the insurance company finds a medical record or conducts surveillance and finds inconsistencies in what you have reported to them versus what you are doing in the “real world” or what you have reported to your doctors, your credibility comes into question and your claim becomes that much more difficult to prove.
Overstating your abilities or optimism for your recovery can be relied on by the insurance company to deny or terminate your claim. It may be difficult to admit to ourselves and others that we are not doing well and that we are not coping as well as we would like. While optimism and positivity may be key to recovery or key to living with a disabling condition, your insurance company could easily misconstrue these sentiments and use them as a basis for denying/terminating your claim or initiating rehabilitation and return to work efforts, well before you are ready.
YOU MAY STILL NEED OUTSIDE HELP TO PROVE YOUR “INVISIBLE CONDITION”
Applying for LTD for a condition stemming from COVID-19 infection is a difficult task, at the best of times, and even more so when you are struggling with the symptoms of your disability. It is important that you get help where you can to ensure that your application is complete, accurate and most of all, persuasive to your insurance company to increase the likelihood that your claim will be approved and to avoid the stress of appealing or litigating a denial.
From decades of experience litigating LTD claims from both sides (as in-house counsel for insurance companies defending LTD claims and as plaintiff’s counsel, representing disabled persons in their complex LTD disputes with all insurance companies in Canada), we know that the type of LTD claims that will be made for long-haulers (such as those for chronic pain, chronic fatigue and mental health conditions) are the most common types of claims that are denied or later, terminated. We understand why these claims were not successful and how to persuade insurance companies of their legitimacy and resolve these disputes for our disabled clients.
Together, our three law partners have over 50 years of LTD litigation experience representing professionals, self-employed individuals and employees with conditions akin to those experienced by long-haulers. Based on that experience, we have put together the above list of the three most important tips for long-haulers applying for or appealing their LTD claims. It is our hope that our suggestions will increase the likelihood of these claims being approved early on, so that you can focus on your recovery without worrying as much about losing your income and other health-related benefits and possibly, your job.
HELP WITH YOUR STD OR LTD APPLICATION, APPEAL AND LITIGATION
We encourage you to contact us if your STD or LTD claim has been denied or terminated by your insurance company. We offer free consultations to help you decide whether to appeal the denial of your claim or whether to proceed straight to litigation. Remember, there is no requirement that you appeal the denial or termination of your STD/LTD claim. (Note: Unionized employees may be required to grieve STD and/or LTD denials/terminations, depending on the wording of their collective agreements. We are able to review collective agreements for jurisdiction over STD/LTD issues.)
As an added support, during this pandemic only, we are offering long-haulers free consultations at the sick leave/LTD application stage. If you are considering sick leave and/or applying for STD or LTD, we encourage you to contact MK Disability Lawyers to schedule a time for us to discuss the details of your disability claim. We will discuss the claims process with you, provide you with direction with respect to what to include in your initial claim and review your claim forms before you submit them. Every claim is different and it is important that you use wording and provide medical evidence that will be most supportive and persuasive to the insurance company and result in the approval of your claim.
We appreciate that there are a number of resources available to help you in your LTD claim application and appeal. Unlike many other resources provided by your employer and insurance company and union, we have the unique perspective that comes only from seeing and litigating countless LTD claims for conditions, such as those of experienced by long-haulers (and all variety of other medical conditions) that have been denied or terminated and we can use that insight and experience to help you avoid those outcomes. One of our partners, Courtney Mulqueen, also has the added insight that only comes from having worked for insurance companies defending LTD claims.
If you have specific questions about LTD, please contact us to schedule a free individual consultation. We also invite you to visit our website www.mkdisabilitylawyers.com, where you will find an extensive collection of blog articles about LTD, including our most recent articles:
“LTD and COVID-19: Applying for Disability Benefits During COVID-19,” “LTD and COVID-19: Mental Health Claims Related to the Pandemic” and “Struggling to Be Seen and Believed: Making an LTD Claim for an “Invisible Condition” and our “Guide to LTD for Union Representatives”, as well as other information related to applying LTD.
0 notes
Text
@romancedeldiablo just reminded me the entire cybersecurity/information security industry is having the greatest field days ever since this whole Covid-19 triggered a mass work from home exodus.
I have so much to say about it and all the security issues that are occurring. This mostly pertains to the US. This isn’t meant to scare anyone, they’re just food for thought and a bit of explanation about my industry.
PSA: Not all hackers are bad, just a reminder. There are very legitimate reasons for hacking such as compliance and research. When I talk about hackers here, I’m talking about the bad ones who are exploiting without permission and for malicious reasons.
The main thing about this whole working from home thing is that most organizations don’t have the infrastructure to support their entire workforce. Not every company uses Google Drive or OneDrive or DropBox.
This means that companies with on-premise servers, isolated servers or networks are screwed. Imagine trying to connect to your friend’s computer who lives on the other side of the world and controlling their mouse. Can’t do it. Gotta download something on both ends to do it. Now imagine that for 500 people at home who are trying to connect to a single server. You’d need to open that server/network up to the internet. That has its own risks because without controlling WHO can access the server, you’re basically allowing anyone (hackers especially) to go in and take all your data.
But then you ask, “Isn’t that what passwords are for?” BITCH look at your own passwords. Do you really think 500 people will have passwords strong enough to withstand a rainbow table attack or that the server won’t shit itself when receiving 500 connections from unknown locations by means of a not-often used method? Hackers only need to exploit one password (for the most part) while the company needs to ensure ALL 500 are protected. That’s difficult as all hell and if it were that easy, I wouldn’t have a job.
Then there’s shit like Virtual Private Networks (VPNs) and RADIUS servers that’ll secure the network connection so it can’t be hijacked and do authentication respectively. Here’s the problem. VPN solutions need to be downloaded on the client system (your computer). When your organization has very technically illiterate people, that becomes a nightmare. ‘Cause you have to set up their accounts on the VPN system and set the permissions for each of them so they can only access what they’re allowed to access otherwise Bob from sales now has access to the HR system with everyone’s social security numbers. It’s very time consuming and can get very complicated. Even worse is that VPNs often require licenses. When you only have 50 licenses and suddenly 500 people want access, you’re screwed. But you can always purchase more licenses, no problem. Here’s the rub. Suddenly, this VPN tunnel needs to accept connections from 500 people. This tunnel is only strong enough to accept 50 concurrent sessions. When 10x that amount get on, guess what? The tunnel shits itself and basically the company has DoS’d itself. Now no one can get any work done until IT figures out how to get 500 people on a system that’s only capable of supporting 50.
Fuck, almost forgot about RADIUS. There’s DIAMETER, too, but shut up about it. It’s an authentication system but depending on how it’s set up, you’ll have to also set up the users. That’s an extra step and it’s a pain in the ass if RADIUS somehow isn’t connected to AD and the user has different passwords and shit.
Not to mention hackers suddenly gaining access to all this information because they’ve already infected people’s home computers and routers prior to the work from home stuff. There’s very limited way for IT to control what happens on a personal computer, so these personal computers can have no anti-virus or security software. This means all data is in danger because someone decided Windows Defender is annoying. (Windows Defender is pretty great, btw.)
Physical robberies are occurring a little more because there’s no one to protect the stores and such. Physical security is taking a hell of a beating.
There’s been an increase in phishing scams around COVID-19. Unemployment sites are probably being (and probably already have been) hacked and the data is being stolen. I think there were some people who were creating fake unemployment sites to steal PII. There are e-mails going out to people saying stuff like, “Your computer has been infected with the CORONAVIRUS. Click here to clean it up.” And you’re wondering, “What sort of morons…?” Don’t. It’s very easy to give in to your panic. Hackers don’t hack computers solely. They hack into human emotion, into the psyche. Anyone can fall for their shit.
The thing with Zoom? Basically they’re so insecure, people are hacking them without issue. How? Because people are silly and put out links, chat logs are saved onto insecure machines that have already been hacked, there are a bunch of exploits available for Zoom, etc.
Healthcare organizations. Oh boy. So, we all know healthcare organizations are working their damnedest to save people suffering from COVID-19. Every second counts and any delay in that process could mean life or death. They work hard. Here’s the thing. There has always been a delicate balance between security and usability. Too secure and it’ll make it difficult for the end user to do their job. Usable without security just makes it easier for an attacker to do their job. Why am I talking about this?
Healthcare organizations usually hold sensitive information. Health information. Social security numbers. Birth dates. Addresses. Insurance information. Family member information. So much stuff. They are a beautiful target for hackers because all that shit is right there and it’s accessible. Healthcare organizations, by and large, do not put a lot of emphasis on security. That’s changing a bit, but for the most part, the don’t care about security. They do the bare minimum because guess what? Every additional control can add time to a doctor or healthcare worker’s routine. Computer lockscreen every 5 minutes? Now the doctor has to re-logon every 5 minutes. This adds about 15 seconds to their rountine. Multiply that several times over for every patient that comes in assuming a doctor will need to log in at least 3 times during a single visit. That can clock in at at least an hour throughout the day. A hour that they could’ve spent doing something else. So imagine more controls. Password needs to be reset. Need to badge in. Log into this extra program to access this file. Call IT because this thing locked them out. Each one of these normal controls now feel insanely restrictive. The ease of use isn’t there and so organizations might look at reversing these security controls, potentially making things even less secure than before in the name of efficiency.
Don’t @ me about HIPAA. I will start rants about how non-prescriptive and ineffective it is to actually get proper security implemented.
LOL @ internet service providers. Internet speeds are dropping due to the amount of traffic they’re getting. Commercial internet really wasn’t prepared for this. Those poor bastards.
Some organizations outsource their IT teams. Those people (Managed Service Providers aka MSPs) are not prepared for this nonsense. It’s popular now to go after these guys for hacking. An MSP usually works for multiple organizations. So, why try going after 50 organizations individually when you have just one organization with poor security controls managing everything from one place? You’d logically go after the one rather than 50. It’s easier.
MSPs are now overworked because they also have to work from home to connect to systems that can’t support so many people connecting to it on personal computers that the MSP can’t log into like they normally would to fix any issues. This makes them tired. What happens when you’re tired? You make more mistakes. And that’s exactly what hackers go after. Once they’re in the MSP’s system, the hacker can now potentially gain access to the 50 clients’ systems. Easy win.
Shadow IT and alternate solutions. This is another doozy. Imagine all your files and shit are on your company’s network. No one is able to access it because there isn’t any VPN or remote sharing system or FTP server set up for this stuff, but you still need to do your job. So, what do you do? Obviously, you start making stuff on your own computer using whatever you’re comfortable with. Google Drive. Dropbox. Box. Slack. That shitty PDF reader you downloaded three years ago and didn’t update.
Now imagine sharing it through things like your personal e-mail which may or may not have been hacked without your knowledge. Or maybe the recipient’s been hacked without anyone’s knowledge. Maybe your files are normally encrypted if they’re on the company network. Now you’re off of it and nothing’s encrypted. Maybe you forget it delete a file or 80 off of your system which has been infected. Or maybe you pasted shit on pastebin or github and it’s available to the public because that’s just easier. Now anyone searching can find it. This is how database dumps are found sometimes and they’re really entertaining.
Shadow IT putting in alternate solutions without the company’s knowledge is always a fucking nightmare. I get that people need to do their jobs and want to do things a certain way, but can you not be selfish and put everyone at risk because you decided your way or the high way?
That sounds awfully familiar…it feels like a situation that we’re going through right now…hey, wait a minute…
Long story short, this whole working from home thing opens up a lot of security issues. Most companies are ill-equipped to handle IT issues, let alone cybersecurity/information security/IT security issues, but because of that, we’re seeing a lot of interesting things happening. Such as finding out New Jersey’s unemployment system runs on a 60+ year old programming language.
Holy shit I can talk about this all day. I’ve definitely glossed over a lot of stuff and oversimplified it. If anyone wants me to talk about any specific topic related to this or cybersecurity or information security in general, drop an ask. I’m always, always more than happy to talk about it.
26 notes
·
View notes
Text
Online plagues, protein folding and spotting fake news: what games can teach us during the coronavirus pandemic
A lot of us do not take video games as well seriously. But video games are also simulations in which genuine people play, make decisions and connect. This makes video games effective tools for discovering and comprehending complicated scenarios, such as how illness spread out and even just how to treat them.
The 'damaged blood' incident
Among the initial occurrences that showed epidemiologists as well as health researchers that games might provide insight right into the spread of transmittable disease happened in 2005.
It started with a new raid experience in the video game developed to permitted a tiny team of gamers to fight an opponent that might "contaminate" personalities with a curse called "damaged blood". The curse would certainly minimize their health and wellness with time, and also spread from player to gamer near.
But a pest permitted gamers' pet dogs as well as minions to lug the curse into the video game's bigger online globe.
All of a sudden menstruation was spreading throughout nearly 4 million players, and also the people who ran the video game had little control. Is this beginning to seem eerily familiar? What's even more, gamers in the game showed the exact same practices that people carry out in response to a real-life pandemic.
Some gamers followed the suggestions of the publisher of the video game to stay clear of contaminated locations. Others rebelled, some didn't care, as well as some encamped in remote locations far from everybody else.
Amusement video games such as Pandemic extremely directly describe what we are all experiencing today. In this video game, gamers collaborate in order to deal with an infection--- as well as in its simpleness, it can illustrate why social communication is so crucial in our worldwide fight against the illness yet is also extremely hard.
Modelling and simulation-- using official, mathematical and usually computerised computations-- support policy makers and also globe leaders to make the right decisions. These versions work as devices for vital choices such as shutting borders and national lockdowns. It takes substantial quantities of reliable data and also deep proficiency to develop and also analyze such models.
A video game like Pandemic, or Wow, lets gamers take part in simplified versions of such crisis scenarios as well as can provide understanding right into human practices in these conditions. The streamlined yet sensible scenarios permit interaction, as well as discovering by doing, without the risk of real-world effects.
Gamings as research laboratories
Gamings can also aid us to establish brand-new clinical options. In Foldit, gamers can individually interact with protein folding, a crucial procedure in molecular biology. It is difficult to mimic with computer systems, yet it plays a role in drug exploration as well as comprehending specific kinds of conditions. The video game makes use of a multitude of private players as well as the highest scoring options are assessed by scientists as possible brand-new services.
The spin is that each node is-- once again-- a human mind taking into consideration solutions, and this model surpasses computational formulas trying the exact same job.
In one instance, players were able to locate an evasive HIV enzyme in simply 3 weeks. The video game is currently being used directly to looking for services to the coronavirus. Gamings are likewise aiding scientists better comprehend the spread of misinformation regarding COVID-19, in a job of the American College Game Laboratory. (Among the authors of this short article is affiliated with the Video game Laboratory.).
With over a million plays, the recorded dataset supplies essential insights into just how gamers view and also categorise details.
The brand-new pandemic version of the video game is currently educating us of dangerous patterns in rumours as well as misinforming details at this hard time. Discovering the best means ahead.
Games may supply some much-needed getaway as well as social connection in this time of physical distancing, yet they are likewise unbelievable tools for finding out more regarding the real world. In locations such as global health and wellness, they can act as really human simulations that help us prepare for unbelievable circumstances and examination numerous contending concepts to find up with the most effective means onward.
1 note
·
View note
Text
Sunday, March 15 COVID-19 updates: TL;DR this is worse than we thought, people without symptoms can be carriers and infect others, and millions of people’s lives are at risk, but that also means that every act of hygiene + social isolation is both more important and more powerful in flattening the curve and saving lives.
Each source dated; because this situation is changing so quickly, I tried to use sources only from the last few days. (Somewhat, but not entirely, U.S.-centric as I live + am tapped into organizing networks here.)

[id: CNN article headline, March 14: Infected people without symptoms might be driving the spread of coronavirus more than we realized.]
“Several experts interviewed by CNN said while it's unclear exactly what percentage of the transmission in the outbreak is fueled by people who are obviously sick versus those who have no symptoms or very mild symptoms, it's become clear that transmission by people who are asymptomatic or mildly symptomatic is responsible for more transmission than previously thought.
"We now know that asymptomatic transmission likely [plays] an important role in spreading this virus," said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota.
Osterholm added that it's "absolutely clear" that asymptomatic infection "surely can fuel a pandemic like this in a way that's going to make it very difficult to control."
+ “Coronavirus is most contagious before and during the first week of symptoms”
In other words, instead of thinking in terms of avoiding getting sick, we need to think in terms of avoiding getting others sick. There’s a real and ever-increasing chance that, without necessarily knowing it, you could be a carrier.
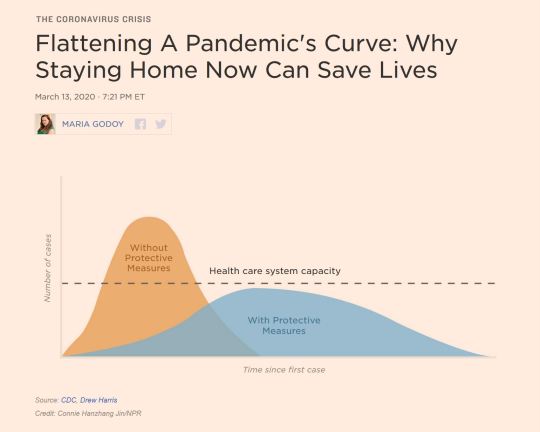
[id: NPR article headline, March 13: Flattening A Pandemic’s Curve: Why Staying Home Now Can Save Lives. Image is of a chart with Number of Cases on the vertical axis and Time Since First Case on the horizontal axis. There’s a straight dotted line labelled Health Care System Capacity running horizontally through the chart. An orange curve labelled Without Protective Measures rises steeply at the beginning of the time axis, showing the number of cases bursting over the Health Care System Capacity line, while a blue curve marked With Protective Measures is spread out over time and and is less steep, staying under the Health Care System Capacity line.]
“As the coronavirus continues to spread in the U.S., more and more businesses are sending employees off to work from home. Public schools are closing, universities are holding classes online, major events are getting canceled, and cultural institutions are shutting their doors. Even Disney World and Disneyland are set to close. The disruption of daily life for many Americans is real and significant — but so are the potential life-saving benefits.
“It's all part of an effort to do what epidemiologists call flattening the curve of the pandemic. The idea is to increase social distancing in order to slow the spread of the virus, so that you don't get a huge spike in the number of people getting sick all at once. If that were to happen, there wouldn't be enough hospital beds or mechanical ventilators for everyone who needs them, and the U.S. hospital system would be overwhelmed. That's already happening in Italy.”
Flattening the curve with hygiene and social distancing isn’t just about the coronavirus. An intensive-care bed is an intensive-care bed, and as people catching a new virus that no one is immune to overwhelm the capacity of the healthcare system, more people are going to die more from all causes--heart attacks, tuberculosis, HIV, the flu, pregnancy complications, injuries from car crashes—because the system won’t have intensive-care capacity for them. Flattening the curve is about keeping coronavirus cases under the dotted line of what the healthcare system--and the rest of our infrastructure--can handle.
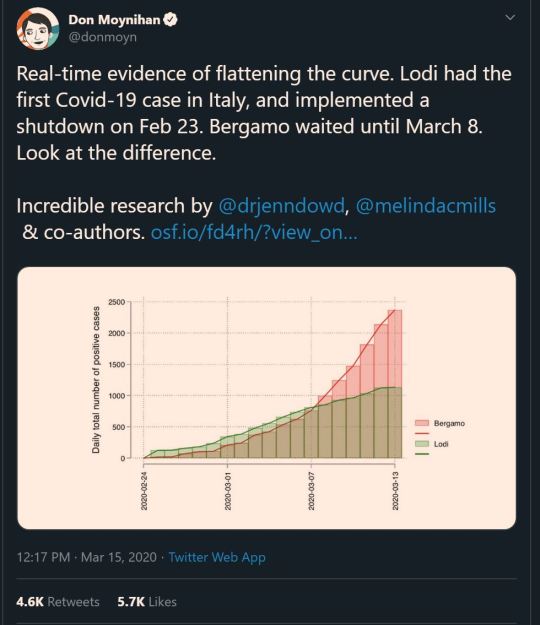
[id: Tweet by Don Moynihan @donmoyn (verified), Mar 15: Real-time evidence of flattening the curve. Lodi had the first Covid-19 case in Italy, and implemented a shutdown on Feb 23. Bergamo waited until March 8. Look at the difference. Incredible research by @drjenndowd, @melindacmills & co-authors. Image is a graph of daily total number of positive cases over time in the two cities, with Bergamo’s rising extremely steeply (approaching 1,000 on March 7 and 2,500 on March 13) and Lodi’s leveling off (approaching 1,000 on March 7 but at barely over 1,000 on March 13). Link in tweet. end id.]
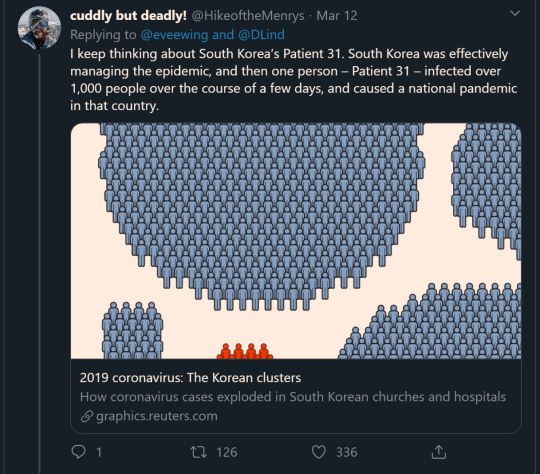
[id: Tweet by cuddly but deadly! @HikeoftheMenrys, Mar 12: I keep thinking about South Korea’s Patient 31. South Korea was effectively managing the epidemic, and then one person – Patient 31 – infected over 1,000 people over the course of a few days, and caused a national pandemic in that country. Link to article in tweet. end id.]
People are currently using #ShutItDown to encourage U.S. event/bar/restaurant closures, and #StayTheFHome to encourage social distancing.
Stay The Fuck Home website (has many languages, and a SFW “Stay The F--- Home” option): staythefuckhome.com

[id: Tweet by Andy Slavitt @ASlavitt (verified), Mar 15: COVID-19 March 15Prep update: Every day brings vital new developments and I talked to leading epidemiologists, public health experts about what is happening & coming & what we should be doing. I learned a bunch. 1/ end id.]
Full Twitter thread here—lots of good info, including on the phenomenon of people taking preparation less seriously in a few weeks if the virus takes longer to hit our communities, and an endorsement of #StayHome/#StayTheFHome
[id: Tweet by Amanda Mull @amandamull (verified), Mar 12: i think the impulse for many people is to look at things closing down or events cancelling right now as a sign of doom, but for the most part i think it's cause for optimism—someone in charge of something is taking this seriously, and doing what they can to limit interactions. end id.]
BONUS ROUND: RESOURCES AND STUFF YOU CAN DO TO HELP OTHERS/RESOURCES TO USE IF YOU NEED ‘EM
- Donate to COVID-19 funds, and to the individual fundraisers of people trying to make it through the pandemic.
- Check in with your friends; offer emotional support if you have the capacity to; offer financial help if you have the capacity to. Can you offer to PayPal/Venmo your friends $5, or $20, or the equivalent of their daily or weekly pay so they can take time off? (If it feels awkward, I’ve found a simple acknowledgement “I hope this doesn’t feel awkward, but” can do wonders to allow awkward-feeling conversations to actually happen! I had the capacity to make one of these offers (hint: not the pricey one) to a friend, and he was not remotely offended.)
(And conversely, don’t be hesitant to ask for or accept others’ support! Text/call your friends if you need to talk to someone! In a time of physical isolation, we’ll get through this by staying emotionally connected.)
- Help others find accurate info. Struggling to talk to the older and/or Fox News-watching folks in your life? Buzzfeed has got ya covered.
- There’s organizing by medical schools and other groups to look out for of elderly, isolated and vulnerable people in many communities; check for (or begin) efforts in your own.
- In the U.S. (and UK and other countries, though again I’m only tapped into things here so this part is U.S.-centric, I’m sorry), there is a large population of people who can’t use hygiene or social distancing: people in immigration detention or incarcerated in jails and prisons.
Many people in ICE detention are already sick from medical neglect and hunger strikes, and many people in prisons and jails (which often overlap with ICE detention--there are county jails and other facilities being used as immigration detention centers in every state in the U.S.--are over the age of 60 and are disabled or have serious mental and physical health issues.
Coronavirus inevitable in prison-like US immigration centers, doctors say
Coronavirus: call to release UK immigration centre detainees
Explainer: Prisons And Jails Are Particularly Vulnerable to COVID-19 Outbreaks
Now is a very good time to donate to bail funds, and to look for and support (or begin) national efforts and grassroots efforts in your community to release people from prisons, jails, and immigration detention. “Iran temporarily released 54,000 people from prison in the wake of this global pandemic. The United States must also consider releasing as many people as possible, among other measures, including decreasing the numbers of people being sent into jails and prisons in the first place.” (Slate)
More asks, actions and links to efforts/mutual aid re: incarceration and the pandemic
The Justice Collaborative has a page and the beginnings of a tracker sheet of efforts to help incarcerated people and other vulnerable populations.
[id: Tweet by Kimberly Corban @Kimberly_Corban (verified), Mar 12: All joking aside, for those who are worried about quarantining during #COVID19 in a home where they do not feel safe, live help is available from the National Domestic Violence Hotline 24/7/365 at @ndvh by chat or by calling their hotline at 1-800-799-7233. end id.]

[id: Tweet by Joanne Starer @JoanneStarer, Mar 9: If you're not plugged into disability twitter, you may not realize that the hoarding of hand sanitizer, wipes, masks is keeping many immunosuppressed people from getting supplies they need. If you have extras, check in with your community to see if anyone could use them. end id.]
[id: Tweet by Clint Smith @ClintSmithIII (verified), Mar 9: A reminder that if public schools shut down, millions of children will lose their access to some of the only meals they receive each day. Food banks will become more important, and I've learned the best way to help is not to donate your spare canned goods, it's to donate money. end id.]
8 notes
·
View notes
Note
i’m so scared my friends could die. they think covid isn’t a big deal anymore, i told them to stop hanging out and showed them how today the cases were at a record high in california and they just told me “only 4000 people have died. that’s less than the flu has killed in a year.” they used to take this seriously but i think they’re just tired of being inside that they’re choosing ignorance. two of my friends have asthma, one of them is working rn and obviously interacts with people regularly
and they just won’t listen to me. the other one that has asthma is also going into other towns to go shopping and going to the beach. i just feel like eventually they’ll get sick and i have tonpreoare to accept that they could die and i’ll never get them back again. they won’t listen to me i seriously don’t know what to do.
I think the first thing is to understand what’s prompting them to leave the house. Is it truly that they’re just not taking this seriously? Understanding what the core of the problem is is the first step in figuring out how to solve it. For example, your friend that’s working probably doesn’t have another option. For your other friend, maybe they need to take more walks in uninhabited areas or drives where they don’t get out of their car. Maybe they need to schedule video calls with friends and family, or they need a schedule/routine, or they need stuff they can do at home. Maybe they feel like if they can keep living their day to day life, if they can maintain a sense of normalcy, they don’t need to be anxious about all the ways the world is going to be fundamentally changed from this. I think for a lot of people, the uncertainty and open-endedness of the situation is more than they’re equipped to handle, and so their brains have gone into “ignore it entirely” mode. Are they the type of person who thinks the media is blowing this out of proportion? That’s a different problem, too.
If they haven’t seen it already, I would show them one of the “flattening the curve” charts. That might help them understand why staying home will save lives.
The Atlantic also has a great article about this problem that I would suggest reading- you can find it here. It has some specific things you can try. In particular, I like the idea of reminding them who they’re protecting in particular (”your parents are at a high risk because they’re older; by social distancing, you can ensure they won’t get sick” or “even though you’re young, because of your asthma and because you’re an essential worker, you’re at a high risk for being able to transmit coronavirus and getting it worse yourself”).
Because you’re in the US, this is also a super complicated issue because we’re getting a ton of mixed messages- “stay inside and socially distance”, but also “everything is opening up again” and “masks are not necessarily” in many places. The lack of leadership from our government on this topic has made a lot of people feel like they have the go-ahead to pretty much go back to their lives, since nobody in charge is really telling them not to. If your friends are in that category, it might be worth sending them some concrete guidelines from experts (read: not our government) to clarify what is and isn’t a good idea for public health at this point.
If you can’t get them to give up social distancing entirely, it may be worth trying to convince them to harm reduce by keeping their physical distance from the people they’re going to see, spending time with people outdoors instead of inside, washing their hands or using hand sanitizer frequently and wearing masks when they leave the house. It’s not a perfect solution, but at least they’ll be at a lower risk of contracting the virus and spreading it to other people.
And- this should go without saying- but while we’re on the subject, everyone wear a face covering! Whether it’s a real mask, a mask you’ve made yourself out of cloth, or a bandana around your face, anything is better than nothing. Please, please, please, everyone who follows this blog, continue to social distance, wash your hands, and please wear masks! I know it may not seem like it, but every person’s actions have an incredible impact, and even small things like wearing a mask or washing your hands do make a big difference.
3 notes
·
View notes
Last Seen Blogs

cockadoodle-doo
The Bees With Teeth are Back

britishbroadwaybooks
remember us to life

cooper-robertson-blog
Every Moment Matters.

alfheimr
the space future

yamakazzii
Yamakazzii