#metabolism affects
Text
So many skk fanfics have Chuuya be the one that openly shows affection while Dazai is emotionally constipated and while Dazai IS emotionally constipated have you seen them?? Dazai is out there giving Chuuya touching farewell speeches and Chuuya gets so embarrassed he shoots Dazai in the face. They're both so bad at showing care in ways that aren't actions but like Chuuya is EXTRA bad. The most physical affection he's given anyone is like, the fistbump he gave Dazai's shoulder that one time. You're telling me Chuuya is the one openly discussing feelings in this relationship?? Dazai will probably get two words in and Chuuya's already running for the hills. I can't imagine him even hugging people unless someone else initiates.
#dazai avoids and chuuya fights but like. dazai so far has been WAY better at openly showing he cares#look all im saying is we need more fics where chuuya is just. really bad at physical affection#have him give the most awkward comfort pat to someone#bsd#nakahara chuuya#soukoku#dazai osamu#skk#shitpost#this isnt even headcanon this is canonically shown chuuya cannot handle feelings#he metabolizes them into heroic gestures#touch starvation who is she
651 notes
·
View notes
Note
What kind of body types do you think the lanterns/flash fam have??
im rly only confident in my hal and barry rn, but i do plan on doing a lineup for everyone when i get further into my dc dive!
here’s the idea so far:

speedster scars/stretchmark version:
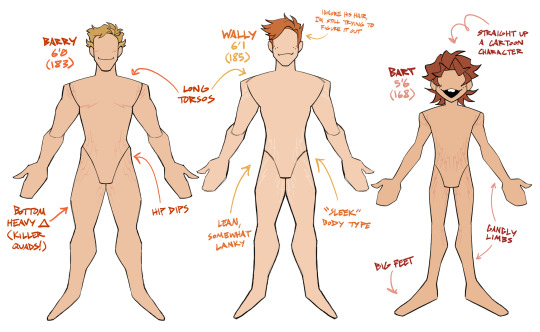
#danswers#green lantern#hal jordan#flashfam#the flash#barry allen#wally west#bart allen#dc#dandoodles#i feel like jay would be kinda stockier so each new gen of flash is getting leaner and leaner#due to the age their powers manifested as well as how their metabolism affects their muscle growth#and hal is hal he has no bearing on how the other lanterns are shaped lol#i’ll just have to see when i get to know them better
231 notes
·
View notes
Text
I like the headcanon that Wolfwood has enhanced senses from the Eye of Michael's experiments, because it puts such a great twist on his "cool guy" sunglasses and smoking. He's happy to let everyone think it's an affectation, and not that his vision is too sensitive without the dark lenses filtering things out, or that the cigarettes help blunt his sense of smell and taste so he isn't constantly picking up on the tang of gunpowder and blood.
#granted it can very much be an affectation too to deal with his insecurities#but one with a practical twist#I also like the headcanon that the cigarettes help with hunger pangs since he has that ultra-speedy metabolism#nicholas d wolfwood#trigun#trigun stampede#trigun meta#lena has thoughts#lena's trigun nonsense
257 notes
·
View notes
Text
mutuals! I must build a portfolio
#ive been thinking about what i want to do after college and i realized that#academia isnt really for me#i dont have the strength of mind really BUT#ive enjoyed tremendously doing figures for my thesis presentation#explaining the infection processes and the metabolic routes affected in a way that isnt mind numbing#and my colleagues say im really good at it too!!#so ive been looking into getting a masters in scientific illustration and its looking really cool!!#i have to work for a few years before i can afford it but in the meantime i can build a pretty sick portfolio... uehehe#idk if you have any tips lmk!
19 notes
·
View notes
Text
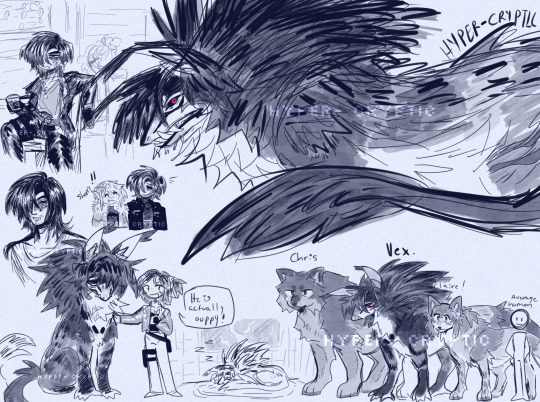
(I DIDN'T FORGET A CAPTION... YOU DID!)
He pop'd in my brain and some demon took over my body to draw him n' other sillies from this au. :3
#one day i will design jill as well because she is actually. very important to the lore of this au LMFAOO#i just don't have any designer juice left in my body#resident evil#las plagas au#he is NOT controlled by las plagas it just had a very bad side effect on him because he couldn't remove it as fast as Ashley.#their plaga had a variation of the g-virus in it on the go basically. so it started to affect his wolf n human form#reminder that zombies in this AU are actually Just vampires!#Ashley also has permanent chompers n pointy ears but she doesn't look dead like Vex does#he looks dead because he was put through 2-3 years of testing and experimenting instead of trying to actually...help his side effects#they thought he was a lost cause since he had became so aggressive in his wolf form and had said he could not remember very well what he#was doing while in his wolf form. he also. mauled someone but yknow. normal ppl things#turns out one of the side effects was and IS just extreme hunger aka his metabolism go faaaaasstt and he needs to eat every like 5 mins#yeah he does have kind of regen as well. not As Fast or good as Sherry's but it's defo noticeable that he has regen.#it also leaves a lot of scars#aka its a vampire thing. in mine it's not really blood they're after but it does make them stronger. they're just eternally hungry#anyways Vex has huge beef with Simmons because under his call for him to get experimented on but they don't know until re5 times?#everyone in this au is out for Simmons LMFAOOOA#uh ... um#haheheooo rambled a bit here :3#leon s kennedy#claire redfield#chris redfield#sherry birkin#and a secret fifth person lets see if yall know who that is#my art
37 notes
·
View notes
Text


i currently do not have the physical or mental energy to correct my mistakes or go all out on this but at least he made it into my gallery
i ignored the fact the choir boys have badges on their caps and not crosses but I combined them lmao.
Yippee
#lord of the flies#lotf#lotf ralph#lotf jack#jack lotf#ralph lotf#jalph lotf#lotf jalph#jalph lord of the flies#lord of the flies jalph#jack merridew#ralph lord of the flies#lord of the flies ralph#lord of the flies jack#jack lord of the flies#i feel drowsy af rn#but hey#it ain't affecting my typing more than it is to my drawing#lol#fanart#my art#sketch#maybe#damn#apath3t1c-pr1nc3#I'm starving#fast metabolism hittin hard#choir ralph#choir ralph lotf#i forgot what else i was gonna put
10 notes
·
View notes
Text
I dont think that anything you do in the second decade of your life should permanently impact your health
#i havent grown a whole bunch since middle school and. yknow i have a theory that it might be because ive had what could be classified as an#eating disorder all four years of hs and my freshman year of college?#like its permanently affected my metabolism but yknow malnutrition can also stunt growth so theres a theory that i fucked myself up a bit w#that one and thats why im shorter than all my immediate family by a significant amount#a bit beyond just natural variation . since all three of them are ~6 ft and im 5’7 on a good day#but also trying alcohol or weed when youre in your late teens shouldnt have a lasting impact i think. you should be allowed to mess around#a bit without it being bad for you#sev rambles
2 notes
·
View notes
Text
Y'know now that I think about it, of the two Arkhe has much bigger horns than Rekrito does
#Rekrito's malnoursihment affected his horn and scale health and Arkhe's affects his metabolism#so their development is much different#I dunno I like little details like that I like stuff affecting Au Ra scales and horns and how they look#it's the little things development-wise
2 notes
·
View notes
Text
I really ought to finish these damn Transferrin Saturation paper notes but I'm struggling with the line-by-line horror stories of how fucked up it is.
Like phew I don't even know what's worse:
• Transferrin Saturation as an indicator of Hepcidin production (oop)
• >50% Transferrin Saturation exposure associated with joint symptoms
• High Transferrin Saturation (>50%) also associated with the appearance of NTBI (Non-transferrin bound iron), which is likely linked to things like *organ damage*
• Therapeutic Phlebotomy treatment linked to an INCREASED iron absorption after procedures because (somehow. I haven't found exactly HOW yet) it decreases Hepcidin production.
It's such a fucking hot mess like what do we even DO with this information??? There's no hepcidin synthetics from a few (admittedly quick) googles (I *did* check the clinical trials website and nothing of interest/help). The paper in question talks about how a Melbourne study suggests that it may be more beneficial to *NOT* treat mild cases of iron overload. Which I find wild because the same paper also points out that a low ferritin does not mean you have a low transferrin saturation, and it's exposure to a high TS% over a long period of time that seems to be associated with worsening symptoms (particularly joint pain, ability to do work, athletic ability, and libido).
From my brief googles, there's no easy lab tests for Hepcidin. There's no easy lab tests for NTBI. These are things that could be doing who-knows-what and we can't even tell.
Add to it the whole Estradiol/Hepcidin link and it just all is an absolutely hot mess and do not like the implications of where this leads nor the fact that it seems very few people in research world have looked at this. (I'm not surprised. I'm not fucking surprised. They love to run with the myth that women with haemochromatosis are protected by their periods. In the words of a specialist I absolutely loathed, "you're self medicating with periods". Yeah. Sure. Tell that to my 18 year old self. Tell that to anyone who either knowingly or unknowingly is taking a Contraceptive Pill that has iron tablets instead of sugar placebos. [Because I only just found out THAT is a thing. I was always so worried about what's in the hormone tablets, but this was a whole new level of 'wot'].)
I'm rambling because I keep stopping every couple of sentences. This paper goes hard. Sure it's not perfect and there's a lot of unanswered questions too but there's plenty of food for thought and ooooh boy I'm sorry Dr Haemotologist Sir, it's gonna be one hell of an introduction session.
#rambles#iron#iron metabolism#haemochromatosis#hemochromatosis#transferrin saturation#ntbi#non-transferrin bound iron#hepcidin#estradiol#venesection#phlebotomy#an Etlu is angy about the state of play with iron metabolism and haemochromatosis research yet again#if I'm not careful I /will/ end up seeking out that biomed degree and doing it myself#(I'm so tired of being told women aren't a concern)#(like literally most of the BBC interviews are young women with the disease)#(can we just actually acknowledge that it affects young women and start looking into HOW it affects us)#(still pretty darn sure that >90 ferritin contributes to my PMDD mood swings)
5 notes
·
View notes
Note
I thought you weren't supposed to eat or drink grapefruit if you took medication because it could like deactivate it or smthin?
its only some medications that are affected by grapefruits i think mostly ssris and anti psychotics? but even then its like you would have to eat an actual grapefruit to have any effect. squirt only has 2% grapefruit juice
#i think u are mixing up stories there was something going around a while ago saying orange juice would deactivate your meds bc of the vit.C#but that was debunked bc it would take So Much of it to actually deactivate your meds.#but grapefruit doesnt deactivate the meds it makes your body not metabolize them so you have a higher concentration of it in ur system#I THINK. i dont care enough to read any more bc im not on anything that it would affect lol#ask#anon
3 notes
·
View notes
Text
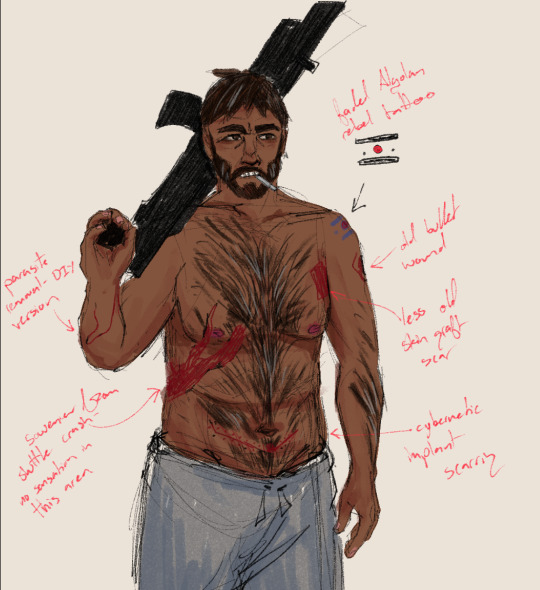
twitter no longer gets my wips bc of the views update.... so now tumblr must see my babygirl drawings <3
i think that compared to how much he's gotten injured, nassim's pretty scar-free since usually he has access to good medical technology... the only scars he has are things he got either before meeting kaveh, or somewhere where there was no medical tools available for a long time
#coriolisposting#i tried to make him a bear but.... that didnt happen#rip#mmm i keep trying to think of ways his botched cybernetics would affect him#but ALSO. coriolis cybernetics make no fucking sense#'weatherproof' halves metabolism and water consumption#which would imply a total overhaul of the entire fucking body#which to ME sounds like bioengineering. but NO! theyre cybernetics!!!#how would that even work#gives me a headache
2 notes
·
View notes
Text

Big Ol Mako Momma Baps. The Biggest, Baddest, Sloshiest Baps around.

And the Gigaton Pancake Presser Buns!

And of course: Ultra-Powerful, Voluminous, Jovian Gut. Noisy, Gurgling Thunderous Tummy.

#muse: makoto#I really wanna do more with Mako’s special capabilities#sweets she drinks/eats affects her milk#her control over her metabolism and powerful behind stomach-
5 notes
·
View notes
Text
I forget why, but I was on the Wikipedia page for polycystic ovarian syndrome, and I started researching hirsutism in women, and I learned the following things in this order:
there's a diagnostic criteria used to evaluate how hairy a woman is
This is important because being too hairy is a diagnostic criteria of most disorders that cause hyperandrogenism
Disorders that cause hyperandrogenism can be diagnosed by...measuring how hairy you are (this is the main and most important diagnostic criterion for PCOS)
Disorders that cause hyperandrogenism are important because they are correlated with obesity, infertility, and...being too hairy?
I think to myself, wait, what is a normal range for testosterone in women? I find this article...which set reference ranges for "normal" testosterone levels in women...EXCLUDING WOMEN WITH PCOS?
Quote: "Polycystic ovary syndrome (PCOS) is another notable condition in genetic (XX) females, which is characterized by excessive ovarian production of androgens. This condition is included for comparison with DSD, as the affected females with PCOS are genetic and phenotypic females. The elevated levels of testosterone in these females can lead to hyperandrogenism, a clinical disorder characterized variably by hirsutism, acne, male-pattern balding, metabolic disturbances, impaired ovulation and infertility. PCOS is a common condition, affecting 7%-10% of premenopausal women."
So: the study claims to demonstrate a clear distinction between the normal range of hormone levels in "Healthy" men and "healthy" women...with "healthy" being defined in the study as...having hormones within the "normal" range.......................
So I researched what the clinically established "normal" range for testosterone in women is
THERE ISN'T ONE????
Quote from the above article: "Several different approaches have been used to define endocrine disorders. The statistical approach establishes the lower and the upper limits of hormone concentrations solely on the basis of the statistical distribution of hormone levels in a healthy reference population. As an illustration, hypo- and hypercalcemia have been defined on the basis of the statistical distribution of serum calcium concentrations. Using this approach, androgen deficiency could be defined as the occurrence of serum testosterone levels that are below the 97.5th percentile of testosterone levels in healthy population of young men. A second approach is to use a threshold hormone concentration below or above which there is high risk of developing adverse health outcomes. This approach has been used to define osteoporosis and hypercholesterolemia. However, we do not know with certainty the thresholds of testosterone levels which are associated with adverse health outcomes."
What the fuck?
What the fuck?
It's batshit crazy to make a diagnostic criteria for medical disorders by placing arbitrary cutoffs within 2-5% of either end of a statistical distribution. What the actual fuck?
"The results came back, you have Statistical Outlier Disease." "What treatments are available?" "Well, first, we recommend dietary change. You should probably stop eating so many spiders."
Another article which attempted to do this
Quote: "Subjects with signs of hirsutism or with a personal history of diabetes or hypertension, or a family history of polycystic ovarian syndrome (PCOS) were excluded."
"We're going to figure out the typical range of testosterone levels that occur in women! First, we're going to exclude all the women that are too hairy from the study. I am very good at science."
Anyway I got off topic but there are apparently race-specific diagnostic tools for "hirsutism." That's kinda weird on its own but when I looked more into this in relation to race I found this article that straight-up uses the term "mongoloid"
19K notes
·
View notes
Text
Once again lookin at myself n askin what the fuck happened
#i used to be so hot#n yea yea i know it's cause i'm now in a human body with human metabolism n also not doin hard drugs#& val's not tryin to actively starve me#but jesus christ#i guess i'm lucky he doesn't say anything bout it anymore (cause he realized it affects doll more than me) but#i still got eyes don't i. don't need him to point out the obvious.#ugggghhhh#spdrvent
0 notes
Text
.
#personal#weight management#tw disordered eating#i know that ive been eating more junk food recently becausd my food police abuser died#but ive gone up 2 pant sizes after being essentially the same size since high school#i was always fat but binge eating didnt do much to affect my weight#and i can feel my ancient metabolism slowing down and im scared ill be fat forever#and i dont know if i can lose weight like mentally#and its made me very upset#and now im eating when not hungry and making myself feel sick#why does it have to be so hard#i wish i didnt hate my body so much
0 notes
Text
Age old question: am I hungry, or am I bored?
#eating#hungry#shitpost#shitposting#i have the metabolism of an elephant soi can eat a lot without it affecting me but ive started wondering if im actually hungry or if ive#accidentally fucked up my brain and now my only two settings are and
0 notes
Last Seen Blogs

seddekarsenal
Seddek-Arsenal

kallyfactory
kallyfactory

sakutori
SakuTori ART

kayipgolge
Lümpen Proletarya

zentechs-blog
Zentech Systems