#psychiatry with did
Text
One thing (among many) that people need to keep in mind when they say things like "oh if you think you have a mental disorder, consult a professional" is that a lot of professionals will not consider evaluating and/or diagnosing you with something you bring up yourself. Especially the more uncommon/complex the disorder is. For things like MDD or GAD you likely won't have that problem, for things like OCD or ADHD they'll likely be suspicious but still comply somewhat, but for things like personality disorders or DID most professionals will completely brush you off and refuse to evaluate you. Because they think you're attention seeking and diagnosis shopping, and that you couldn't possibly have it, even if you haven't done anything to earn that suspicion.
For disorders like that, unless the professional themselves suspects you have it and comes up with that idea themselves, good luck getting evaluated at all. Especially when it comes to disorders most professionals don't even think they'll encounter, like SzPD or DID.
It'd be nice if we lived in a world where you could go see a psych, say "hey I think I have this", and they'd do a proper and fair evaluation for you the way a physical doctor would (moreso should but that's another can of worms).
It just isn't as simple as "ask a professional".
#mental health#mental illness#neurodivergent#mental disorder#psych#psychiatry#disabled problems#ocd#adhd#asd#did system#osdd 1b#osdd 1a#personality disorder#cluster a#cluster b#cluster c#szpd#avpd
3K notes
·
View notes
Text
I could totally do surgery on myself and even give myself anesthesia and then stitch myself up i could totally do that. I think I can figure out how to put it back
#is this just poetic or srs.....we'll never know#just know that i am high af rn#i dont have steady enough hands or good enough vision to ever be a surgeon i dont think. not in that sterile room. lol#sigh guess i'll pursue psychiatry#gonna fuck myself up irreversibly someday wdyt#trust meee#essentially surgeons ask that we trust them like thanks for not leaving any tools behind in my body i appreciate it man#that one nurse who did my 55+ stitches we had a moment#i was like no lidocaine pls i don't want my arms to be numb for the next day and a half i will kms more#so he didnt#that was so respectful of him
90 notes
·
View notes
Text
random but it’s annoying to me that ‘narcissist’ is like. colloquially referring to the diagnosis now. like it’s a word outside of psychology too. it’s like if i was like “wow he’s such an asshole” and someone was like “oh, he’s been diagnosed with Asshole Personality Disorder?” or like “he’s stupid” “you mean he’s clinically Unintelligent?” like. girl no. clearly i am using this word in an non-professional manner. i am making an observation and using an adjective. not every adjective requires a doctor’s input and they cannot claim all the useful adjectives
#like. my dad did not have a personality disorder he thought the world should revolve around him#sorry but the word for that still IS narcissistic#in the normal adjective sense.#in the “in love with yourself” sense. in the “resembling narcissus” sense#but i would also get cancelled again if i shared my personal opinions on the field of psychology and psychiatry so 🙊
44 notes
·
View notes
Note
ok so queerautism (it/its) stuff:
Allegations of it sexualizing stuff a minor said and acting predatory? Can’t confirm bc can’t find evidence / haven’t found evidence yet
Block evading
telling its followers to harass anti endos
supports endos
says it’s ok to demedicalize disorders including OCD
started its own religion and some ppl spread rumors it was a cult but from what I read it didn’t sound like a cult and other ppl said it wasn’t a count, just odd
Harmful anti-psychiatry takes
harassing ppl and encouraging others to harass ppl
says disorders and stuff can be spiritual?
encouraged somebody to stop going to therapy I think?
making cult jokes
Said being told to touch grass was ableist?
It’s made some sorta comments about the holocaust and Jewish ppl that upset Jewish ppl? (It’s not jewish to my knowledge)
constantly shits on positivity posts and starts drama for attention
*note I could be wrong about some of this, this was just a quick scroll through stuff abt it- I’ll check again when I have more time and I’ll link sources TvT
(also jokes(?) about making ppl plural. And I saw some posts saying it claimed to be a system. Some saying it was endo and some saying it was traumagenic and some saying it wasn’t a system at all so I have no idea and i don’t wanna fakeclaim-)
also supposedly it claimed it’s system was formed in adulthood but is traumagenic?? Which- that- that doesn’t work TvT
so yeah
(sorry this is so damn long- I tried to keep it short-)
also I think I used they them first ask bc I didn’t know its prns were it/its bc I didn’t check/ so I’m sorry /gen
That's... a lot. Even without the sources, that's still a lot and very disgusting behavior.
If there's another ask citing sources, I'll make sure it gets answered as soon as possible. Allegations are serious and not having sources might make a lot of people question, but everything else is vile behavior.
#did system#endos dni#system#osddid#traumagenic system#actually did#actually traumagenic#endos not for you#anti endo#did plural#did plurality#osdd plural#osdd plurality#tw sexualization#tw sexualization mention#tw predatory behavior#tw harssment mention#tw cult jokes#tw anti psychiatry#tw holocaust mention
35 notes
·
View notes
Text
Fuck it my blog is pro-psych, just pro-reform.
Psych Critical if you will.
I am quite literally fucking exhausted by the amounts of (typically low support needs) NDs who go around talking about how there should be "no more psychiatry" and "no more psychology" and we should "abolish the DSM" and "abolish psychiatric/psychological care". How about actually- fuck you? How about that because you want me to fucking die- you want to kill off NDs with higher support needs who rely on doctors to be able to stay alive and not be in danger.
No I don't want to abolish psychiatry because not only do I need my medications but I am logistically opposed to people just randomly being able to get whatever medication they want because they self diagnosed themselves with something. If you haven't taken a psychiatric med you had a horrible reaction to- you're lucky, If you have the wrong combination or take one your personal body doesn't like you can experience psychosis, suicidal ideation, homicidal ideation, dizziness, drowsiness, nausea, hallucination based psychosis, etc. No the public should not get to dictate what medication they get because people are not educated enough to know if they will cause adverse effects when mixed.
No I don't want to abolish psychology just because one of our past therapists abused us and groomed us as a kid. Sometimes bad people are in places of power. Our good therapists have helped us immensely. Our life has improved drastically since we've been seeing a specific therapist for our DID. We've been able to function better we've been able to feel some happiness in the midst of the horrific memories we have uncovered.
I think all this healthcare should continue. I think however it should be free- and it should be possible and easy for even minors to refuse certain types of treatment if they personally want. However anti-psych seeks not to reform the issues- but to destroy the support networks so many rely on. It is not about people's freedom to choose- it is about forcing others out of a system that may very well be the only thing keeping them going.
#pro psych#psych critical#mad pride#neurodivergent#actually aspd#actually autistic#actually DID#actually OCD#actually disabled#actually ptsd#actually traumatized#actually mentally ill#psychology#psychiatry#pro psychology#psych ciritical
95 notes
·
View notes
Note
wild. came to check out the terf allegations and found the hot systems take. hope you find some psychology research soon because there's plenty about it. not to mention the DSM entries (did/osdd). typically that's the stuff people are exposed to that makes them think systems are a thing.
does the dsm cover how middle schoolers come to believe that the cast of hazbin hotel lives in their brain
#does it cover how did and osdd had a huge spike in popularity after short-form video became the main medium for online posting#do you take everything you see online at face value#i’m published in multiple psychiatry journals lol don’t try it
33 notes
·
View notes
Text
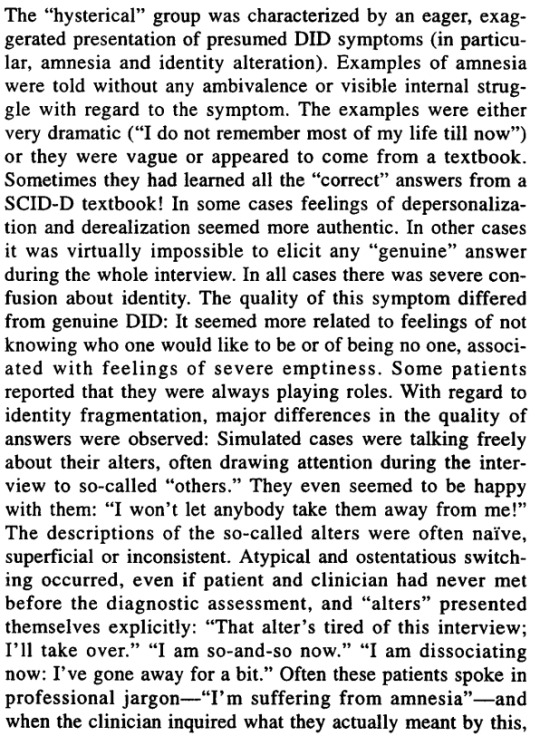
Imitated DID 2 - Hysterical Boogaloo
We're diving back in from where we left off last time. Now with the "hysterical" group.

There is actually a certain level of logic to part of this.
I don't diagnose people with disorders. But when talking about plurality with questioning systems, I find it much more useful to ask about their internal experiences and hear them described in their own words.
Especially because a lot of medical jargon and even plural community terms kind of suck for describing these type of experiences. If someone isn't describing things in their own words, I can understand feeling like they might be faking. But that doesn't mean they are.
Comorbid Mental Illnesses can affect communication: We have ASD. If you've noticed, we tend to use jargon and big words a lot. I often make up my own jargon too because much of what I see from psychiatry is inadequate. (I could go on long rants about how meaningless the word "dissociation" is.)
The issue is that a lot of people with ASD or other disorders might behave like this. We might use clinical words if we've studied them. I'd like to think We would have the presence of mind to not reply to a psychiatrist asking "what do you mean by amnesia" by explaining whether our amnesia is retrograde or anterograde, but I could easily imagine someone else doing that.
Some people also have personality types where they might be seeking respect, and trying to impress a psychiatrist with their knowledge of academic terms.
Perhaps what appears to not be genuine is just another condition that makes people communicate in ways a neurotypical wouldn't be expected to.
This also goes for other behavior that appears non-genuine. Maybe someone presenting more overt presentation just doesn't have a filter or social awareness.
(Also, amnesia isn't even professional jargon. It's used all the time by lay people.)
Again, most people with DID stated they would miss the voices of their alters: Like I said in the last post, 69% of DID voice hearers said they would miss their alters' voices if they were gone.
The feeling of "I won't let anybody take them away from me!" isn't uncommon. They're in the MAJORITY. Maybe expressing these feelings aloud is uncommon. But that just makes me further suspect influence from comorbid disorders that make it difficult to tell what's socially acceptable.
Another possibility is someone mentions their full trauma history and talks about their conditions as a test of sorts. They've learned to expect rejection, and want to be upfront about everything so that if they scare someone away, it will be right at the beginning of the relationship.
It's so important to account for different behaviors in different people, and different illnesses and conditions that can influence those behaviors.
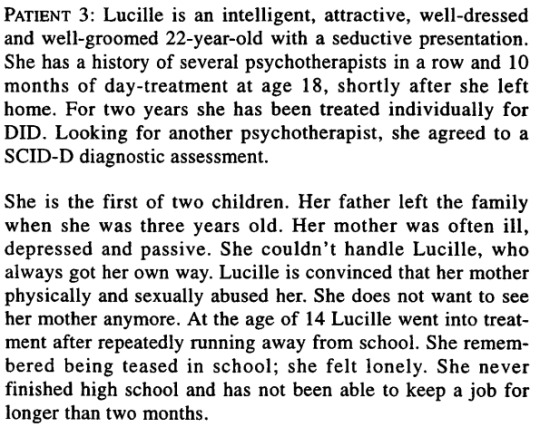
WHAT?!
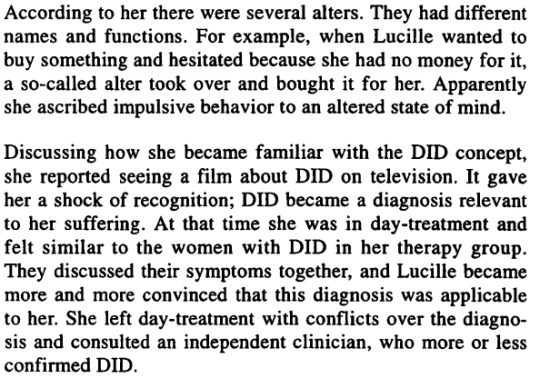
She couldn't handle Lucille, who always got her own way. Lucille is convinced that her mother physically and sexually abused her.
There are many ways to write this that wouldn't involve portraying the mother as a victim of a little girl.
It's stated as an objective fact that Lucille's mother "couldn't handle Lucille," suggesting Lucille was always the problem. Meanwhile, "Lucille is convinced" her mother abused her. It's not even neutral language, like she "reported" or "described" it. She's "convinced."
I'm absolutely appalled.
Also, it feels a little gross for the doctors to describe their patient as "attractive" and with a "seductive presentation." I'm not the only one feeling that, right?
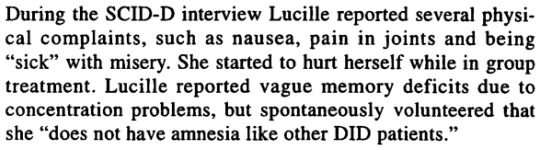
So she essentially did report amnesia. It just sounds like she didn't understand what amnesia was or was in denial, and clinicians should have questioned further.
Surely, if she were trying to manipulate the clinicians, she'd have claimed to amnesia, right? Since amnesia is part of the criteria?
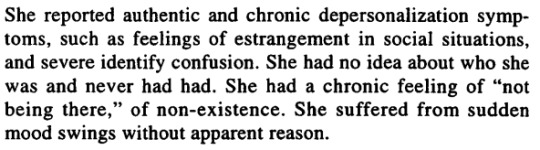
Like with the "borderline" group from before, she had DPDR.
So she recognized similarity in her own experiences with DID systems AND an independent clinician confirmed her DID.
But this is what they're using as evidence against her. That she heard about it first and then identified with it. But that's often how people learn about their disorders. Sure, sometimes it can be wrong. But it shouldn't be treated as evidence against somebody as it is here.

Quick reminder that she started to hurt herself in group treatment.
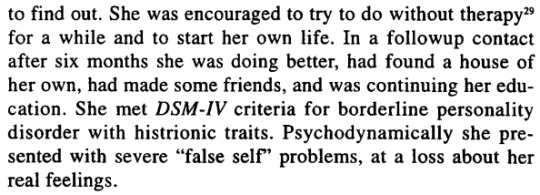
Why would you suggest she go without therapy? Supposedly it worked out if we trust the clinicians' report. But I'm not so certain I do. I doubt they'd say "we told her to take a hike and then she was worse off than when we left her."
Now, the actual section focused on Lucille isn't the last time we'll hear about her, so let's skip ahead a bit.
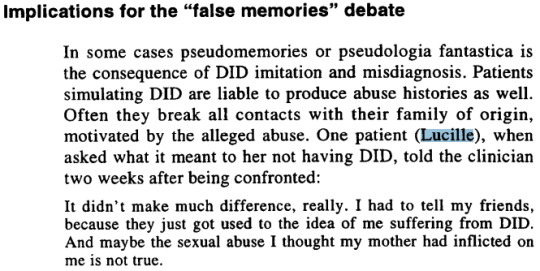
This adds a bit more context to the earlier wording of her being "convinced" her mother abused her.
But the implications are a bit more terrifying to me. What was left out of this case study?
Lucille comes in experiencing chronic symptoms of DP/DR. She believes her mother abused her. The clinicians here seem to take the side of the mother in a peculiar way, describing Lucille's mother as "being unable to handle" the little girl.
After leaving therapy and coming back for a follow up, Lucille is saying, uncertainly, that the abuse she endured might not have happened.
Did the clinicians, as authority figures, also try to convince Lucille that her memories of abuse were false?
This feels extremely gaslighty to me.

This is actually a good practice. And is a huge problem I have with the anti-endo ideology is that it often encourages people to look for trauma to confirm systemhood. If you tell someone who is a system they need trauma to be a system, there is a real concern of them trying to fit themselves into that box.
But is the implication that Lucille fabricated her trauma after seeking treatment for DID, and never believed it prior? If so, that feels like an incredibly relevant detail to omit from your case study.

So their opinion, ultimately, is that these cases of "imitated DID" are fabricating trauma memories.
Essentially, this paper is advocating for False Memory Syndrome.
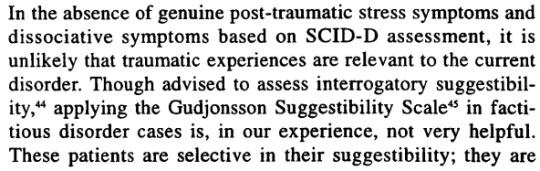
And worse, they admit there's no way to reliably assess suggestibility in these patients, since the authors claim the suggestibility is selective and the scale useless.
It comes down to the individual clinicians with their individual biases to determine who is or isn't an actual trauma survivor.
What is all of this REALLY about?
Now we get to the real point
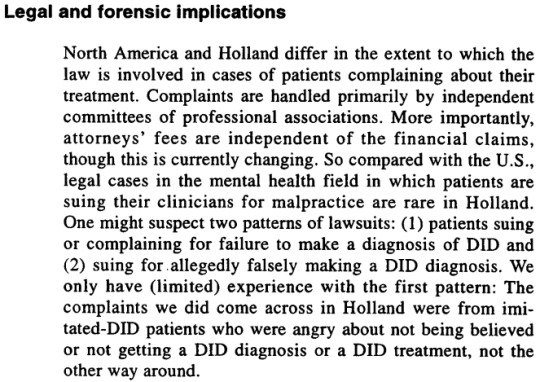
While other parts of the paper pay lip service to helping patients, a large amount of it is focused on addressing malpractice complaints.

Here is some interesting wording. Shouldn't the interests of the patients be the priority of therapy?
I understand the intent behind this. But the wording presents an adversarial relationship between clinicians and hostile patients where clinicians are meant to act as judges and authority figures, and acting in the interests of the patients is "collusion."
Ideally, even if a patient were faking DID, giving them a more correct diagnosis would still be working in the best interests of the patients, right? At no point should acting in the patient's interest be presented as a bad thing as it is here.
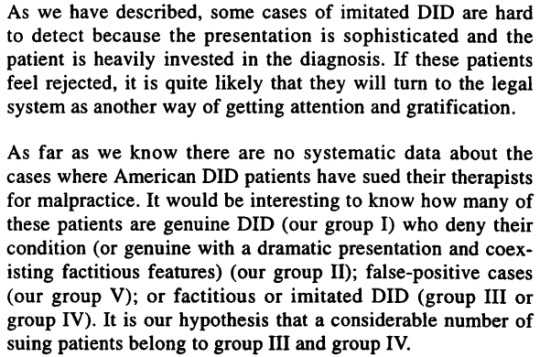
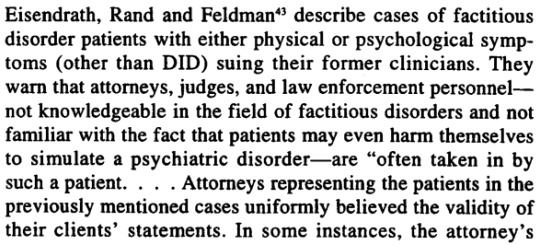
Patients suing therapists over believed-malpractice are presented as seeking "attention and gratification."
I'd agree that it would be interesting to know what groups the suing patients fall into. But there would need to be a better way to make such an assessment.
Because if you're going to have cases like Sandra's, mentioned in the last post, where clinicians are forming biases based on her life history of self-medication with drugs and having an older boyfriend before they even observe her, this method isn't effective.
What would be really interesting to me is, if Sandra or Lucille had gone to another clinic, would the other clinics have judged their DID as being imitated? Or is this solely a result of the biases of these clinicians?
In contrast, would those clinics have judged other patients that this clinic said had "genuine" DID of having imitated DID.
Is there even the slightest bit of credence to this concept? Can it be consistently applied or is this just the opinions of one clinic being treated as gospel?
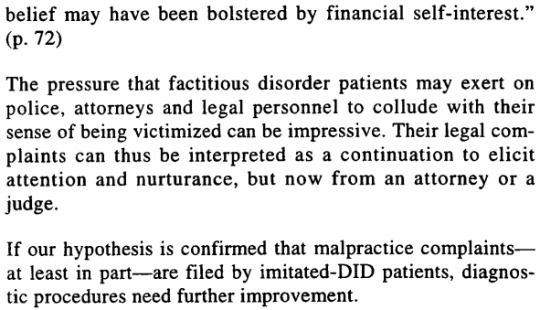
The goal of the whole paper is pushing False Memory Syndrome in a way that pushes responsibility from clinicians onto patients.
Over 20 years later, and this hypothesis is still groundless. Not just the hypothesis that those responsible for lawsuits are imitated DID cases, but even that second opinions could confirm their own case studies as being imitated DID.
This paper that started the "imitated DID" myth, the paper that led to the controversial McLean video, is based on nothing.
It was motivated not with the goal of helping patients with DID nor helping the patients they accuse of imitating DID, but by the self-interest of clinicians trying to protect themselves from malpractice complaints of patients they treat as hostile and adversarial.
#psychiatry#psych critical#false memories#syscourse#mental illness#multiplicity#systems#endogenic#pro endo#pro endogenic#system stuff#science#imitated did#psychology#sysblr#plural#plurality#plural system#actually plural#actually a system#sa tw#abuse tw#child abuse tw#csa tw#tw child abuse
35 notes
·
View notes
Text
Not me having to explain the difference between DID and OSDD to my psychiatrist 🥲
12 notes
·
View notes
Note
HC-DID(/TBMC) culture is feeling so isolated and unseen in psychiatry and having to repeat "I didn't do this thing because I wanted to, I did it because I had to and I hate that I had literally no real control over it" and the explanation just. does not. process with mental health professionals ever and it's like talking to a brick wall
.
#culture is#ramcoa#hc did#hc did culture#hc did culture is#system#system culture#system culture is#ramcoa culture#ramcoa culture is#psychiatry#tbmc
16 notes
·
View notes
Text
there is a certain dehumanization in calling my behaviors "symptoms" when they aren't harming me. i think it's ok to say i have "dissociation" because it's something that fucks me up and gives me directions in how to feel better, but it feels weird to say that being passionate about something is a "hyper fixation" and if it's something that society deems unusual, it's a "special interest". when i feel comfortable enough in my environment and i'm standing up, i start tap dancing in place because it brings me joy. but they will say that i'm "unmasking" and i'm "stimming" because i'm "hyperactive". my body isn't mine now, as my mind. now they're subjects for analysis and i am a lab rat. these symptoms aren't made for me, to help me, but to explain to others why i am the way i am and make them comfortable enough to be around me but not to respect me as a person. i am ok with having my diagnosis because it helps me improve my life according to my limitations, it helped me heal things that were indeed ill, but labels are only useful until people don't see you beyond them.
#very normal post#mini rant#mental healthy#psychiatry#psychology#adhd#bipolar#bpd#autism#depression#anxiety#did#idk now many mental illnesses are there?#the entire dsm-5
10 notes
·
View notes
Text
Since I'm struggling so bad with the dissociative identity disorder lately, I keep wishing I had a therapist to talk it over with. It can't happen, because in the country where I live in, it's not a recognized disorder yet. Still, I get curious about what is known about it, I'll write a bit about that, and it's probably just going to be funny to those who already know what a dissociative identity disorder is.
So by the chance of fate, I happen to work for a psychiatrist, who doesn't know I have any such illnesses, and will not find out (I don't wanna get institutionalized). However, since I do work for them, I sometimes have access to their studying materials, to their diagnostic tools and little workbooks, and if I have a moment, I will secretly grab one of these books and fervently look through to see what they're all about.
I have learned many unsettling things, for example, you can be diagnosed with 'a case of bad nerves' if you come in with symptoms of anxiety and paranoia. You can also be diagnosed with 'hysteric delusions', still. Your spouse can come talk to a psychiatrist and complain about you, and they'll diagnose you with something immediately. PTSD is the end of the line for the psychiatric disorders, and you can only get diagnosed with it if you've partaken in a war. No other way to have ptsd here.
No diagnostic tools or workbooks even mentioned a dissociative disorder.
Then I thought, okay, this is bad, they're definitely not teaching people to recognize or diagnose this, and at this point I suspect people are getting massively misdiagnosed with victim-blaming crap and even the diagnostic tools are telling psychiatrists to diagnose them exactly like that.
But then I also decide to google it in my own language, like there must be some sort of info on it, right? And I find a scientific article about it. And I'm going to translate to you exactly what I read in that article:
"Dissociative identity disorder, or dissociative personality disorders are marked with change of feeling of identity, memory or consciousness. People with this disorder can forget important events from their past, or even temporarily forget who they are, or even take on a new identity. They can even wander off from their usual environment, in a foreign direction."
I don't even know how to react to this. Even if I did get diagnosed, all I would be labeled as is 'has amnesia, wanders off' disorder. And I’m going to be honest, I don’t even wander off anymore. I’m unfit to be diagnosed.
-
I feel bad for putting out all of this misinformation now, so for those who are somehow reading up to this point without knowing what a dissociative identity disorder actually is, here’s a definition from Wikipedia:
“Dissociative identity disorder (DID), previously known as multiple personality disorder (MPD), and colloquially known as split personality disorder, is a mental disorder characterized by the maintenance of at least two distinct and relatively enduring personality states.The disorder is accompanied by memory gaps more severe than could be explained by ordinary forgetfulness. The personality states alternately show in a person's behavior; however, presentations of the disorder vary.“
For people who have it, it can feel like you have different versions of yourself in your head, voices inside of you that are talking to you, or different people in your head who not only talk to you, but can take control over your body, or ‘switch’. They all exist to protect you and hold traumatic memories, hold different aspects of your personality, and they have different needs that need to be fulfilled. Alters can be very different from each other, and have developed different mindsets, priorities and goals, as they are shaped based on different memories and experiences they’ve had. They exist to make it possible for a child to go through severe trauma, and be able to survive it and keep functioning almost as if it didn’t happen.
#dissociative identity disorder#DiD#system#osdd#alters#undiagnosed#psychiatrist diagnostic tools#criticizing the psychiatry#this basically means i can't get therapy via healthcare#i don't have money to find someone abroad#so sadly i will have to keep figuring it out#alone with alters
123 notes
·
View notes
Text
being interested in studying william afton has made me a worse person
#every time i think about him i think about like three things#one. ive read multiple fics where he has the same mental illnesses as i do. sob emoji. assigned child killer at psychiatry#oh btw did i tell you all that my psych wants to evaluate me for autism.#i believe it now#plus my boyfriend gave me a list of autisms i did with them#so. yknow. undeniable at this point.#um what was i gettin at#oh yeah. number two im a massive mike kinnie#we all gotta know this by now#and like i have my own little canon my own little michael and timeline and william and such#and i . yeah i project onto that man. whatre ya gonna do#so three#its really fucked up that i think that william afton is kind of hot#considering these. all the things#all the william afton things#jesus christ im such a caricature#this just in!!!! guy with mommy issues is in love with glados and thinks#the manipulative child killing emotionally abusive william afton in xts head#thinks hes attractive#like. jesus christ#the jokes write themselves#i took my sleep[y meds a half hour ago#i really oughta get into bed#anyways the william afton goes to hell song is really funny and fun#and i cant stop listening
3 notes
·
View notes
Text
who knew that board prep questions would ask me about the common street names for all the drugs?
#where exactly did this fit in the curriculum?#mental health#psychiatry residency#residency#boards#board exams#i bet this isn't on anyone else's boards
7 notes
·
View notes
Text
I am doing unwell ✨psychologically✨
#m rambles#at least I cooked a meal today?#I’ve been surviving off of junk food for like a week I think?#maybe not quite a week#either way#also tmi but I’ve been out of clean underwear for a few days which is so sick#because I have almost a month’s worth of underwear#I have a month’s worth of trash and dishes too#but at least I did half my dishes last night#I’m so tired#all the damn time#I didn’t work today either#I’m so sick of this shit#I have a psychiatry appointment at 6:30am and I have no clue if I’ll manage to wake up for it#but I need to because my meds just aren’t cutting it#I took them for almost a month straight and it hasn’t helped#idk at least my ig is letting me comment and like posts again so that’s nice I guess
3 notes
·
View notes
Text
when the host is just doing whatever and then you accidentally front and you're like "oh fuck i wasn't supposed to do this oh shit oh fuck oh god let me back inside before anyone here notices the mask slip"
#idk man art workshop does things to us#luckily it is with the psychiatry so ppl are understanding ig#but we still dont want to be overt#system things#actually did#actually osdd#actually pdid#actually osddid#cdd system#dissociative system#alters#we still need to learn what tags we're gonna use idk#levi here#yo its sof#ours
20 notes
·
View notes
Text
I read the 90s paper about imitated DID.
All of it is terrible, nothing remotely scientific, the choices to label people as imitated DID was often arbitrary and subject to extreme bias, and toward the end they talk about the legal applications for this in a way that make it clear that the motivation for their hypothesis was protecting therapists from lawsuits rather than helping patients.
#syscourse#psychology#psych critical#psychiatry#sysblr#multiplicity#plural#plurality#sanism#plural system#system#systems#anti psych#pro endo#pro endogenic#system stuff#actually plural#actually a system#mental health#imitated did
30 notes
·
View notes
Last Seen Blogs

you-can-always-come-home
Funny how love is every song in every key

sckmed
babe

shreekrishnajewellers
Shree Krishna Jewellers

sylfadias
Untitled

top-blondie
TØP-Blondie / NOW WITH SPOILERS