#QRS complex
Text
Going through the ACLS online training:
The P wave represents depolarization of the atrial myocardial cells.
The PR interval represents the time from the beginning of atrial depolarization to the beginning of ventricular depolarization. It is measured from the beginning of the P wave to the beginning of the QRS complex. The normal duration of the PR interval is 120 to 200 milliseconds.
The QRS complex represents depolarization of the ventricular myocardial cells. The normal duration of the QRS complex is less than 120 milliseconds.
The J point is the point where the QRS complex ends and the ST segment begins.
The T wave represents repolarization of the ventricular myocardial cells. (Atrial repolarization occurs during ventricular depolarization and is not seen on the ECG; it is overshadowed by the depolarization of the larger ventricles).
The QT interval is measured from the beginning of the QRS complex to the end of the T wave. This encompasses the time from ventricular depolarization to the end of repolarization.
The ST segment represents the time between the end of ventricular depolarization and the beginning of ventricular repolarization. It is measured from the end of the QRS complex to the beginning of the T wave.
Is the amount of time between each P wave the same? What about the amount of time between each QRS complex (i.e., the RR interval)?
To estimate the atrial rate, count the number of P waves over a 6-second period and multiply by 10. To estimate the ventricular rate, do the same with the QRS complexes. Alternatively, if the rhythm is regular, divide 300 by the number of large squares between two P waves (to get the atrial rate) and between two R waves (to get the ventricular rate). If the heart rate is very fast, divide 1500 by the number of small squares between two P waves (to get the atrial rate) and between two R waves (to get the ventricular rate). Are the atrial and ventricular rates the same or different? Are they within normal limits?
Look for the P waves. Are they there? Do all the P waves have the same morphology? Is there one––and only one––P wave associated with each QRS complex? Note that in lead II, the P waves are usually upright but in lead V1, the P waves may be inverted or biphasic.
Measure the QRS complex. Is it within the normal range? (QRS complexes that exceed 120 milliseconds in duration are abnormal.) Do all the QRS complexes have the same morphology?
Look for the T waves. Are they there? If so, do all the T waves have the same morphology? The direction of the T wave should be the same as that of the main vector of the QRS. The T waves should be less than 5 millimeters in amplitude in the limb leads and less than 15 millimeters in amplitude in the precordial leads.
Measure the PR interval. Is it within the normal range? Is it consistent throughout the tracing? If it varies, is the variation predictable?
Measure the QT interval and calculate the corrected QT interval. Because the QT interval varies normally with the heart rate, the corrected QT interval (QTc) is used to give a value that is theoretically independent of rate. The QTc adjusts for heart rate differences by dividing the QT interval by the square root of the RR interval (i.e., one cardiac cycle). In general, a QTc greater than 460 milliseconds is considered to be prolonged. If the heart rate is faster than 120 bpm or slower than 50 bpm, the formula for calculating the QTc is not considered valid and should not be used.
Look at the ST segment. Is it elevated or depressed from the baseline?
Determine the rhythm and its clinical significance. Is the patient showing signs or symptoms? Is the rhythm potentially life-threatening?
In normal sinus rhythm:
Each P wave is linked in a 1:1 fashion to each QRS complex (i.e., atrial depolarization is always linked to ventricular depolarization).
The P waves are uniform in shape, indicating that the SA node is the only pacemaker driving atrial depolarization.
P waves in lead II are normally upright and all the same shape. P waves in lead V1 are normally inverted (or on occasion biphasic) and all the same shape.
The rhythm is regular (but may vary slightly during respirations).
The rate ranges between 60 and 100 bpm.
Causes of sinus bradycardia include:
Vagal stimulation.
Myocardial infarction.
Hypoxia.
Medications (e.g., β-blockers, calcium channel blockers, digoxin).
Coronary artery disease.
Hypothyroidism.
Iatrogenic illness.
Inflammatory conditions.
First-degree AV block is characterized by a prolonged delay in conduction at the AV node or bundle of His. The impulse is conducted normally from the sinus node through the atria, but upon reaching the AV node, it is delayed for longer than the usual 0.2 second. In first-degree AV block, although the impulses are delayed, each atrial impulse is eventually conducted through the AV node to cause ventricular depolarization.
First-degree AV block may be a normal finding in athletes and young patients with high vagal tone. It can also be an early sign of degenerative disease of the conduction system or a transient manifestation of myocarditis or drug toxicity.
In second-degree AV block type I (also called Mobitz type I or Wenckebach block), impulses are delayed and some are not conducted through to the ventricles. After three or four successive impulse delays, the next impulse is blocked. After the blocked impulse, the AV node resets, and the pattern repeats. Second-degree AV block type I usually occurs at the AV node but may be infranodal.
Because the block usually occurs above the bundle of His, conditions or medications that affect the AV node (such as myocarditis, electrolyte abnormalities, inferior wall myocardial infarction or digoxin) can cause second-degree AV block type I. This type of arrhythmia can also be physiologic.
Second-degree AV block type I rarely produces symptoms. Some patients may have signs and symptoms similar to sinus bradycardia.
In second-degree AV block type II (Mobitz type II), the block occurs below the AV node, in the bundle of His. As with second-degree AV block type I, some atrial impulses are conducted through to the ventricles, and others are not. However, there are no progressive delays. The blocked impulses may be chaotic or occur in a pattern (e.g., 2:1, 3:1 or 4:1). In high-grade second-degree AV block type II, the ratio is greater than 2:1 (i.e., 3:1, 4:1, or variable).
Second-degree AV block type II is always pathologic. It is usually caused by fibrotic disease of the conduction system or anterior myocardial infarction.
Patients may present with light-headedness or syncope, or they may be asymptomatic. The clinical presentation varies, depending on the ratio of conducted to blocked impulses.
In third-degree (complete) AV block, no impulses are conducted through to the ventricles. The block can occur at the level of the AV node but is usually infranodal. Pacemaker cells in the AV junction, bundle of His or the ventricles stimulate the ventricles to contract, usually at a rate of 30 to 45 bpm. This means that the atria and ventricles are being driven by independent pacemakers and are contracting at their own intrinsic rates (i.e., 60 to 100 bpm for the atria and 30 to 45 bpm for the ventricles), a situation known as AV dissociation.
Degenerative disease of the conduction system is the leading cause of third-degree AV block. This arrhythmia may also result from damage caused by myocardial infarction, Lyme disease or antiarrhythmic drugs.
If ventricular contraction is stimulated by pacemaker cells above the bifurcation of the bundle of His, the ventricular rate is relatively fast (40 to 60 bpm) and reliable, and symptoms may be mild (such as fatigue, orthostatic hypotension and effort intolerance). However, if ventricular contraction is stimulated by pacemaker cells in the ventricles, the ventricular rate will be slower (20 to 40 bpm) and less reliable, and symptoms of decreased cardiac output may be more severe.
First-Degree AV Block
In first-degree AV block, normal P waves are followed by QRS complexes, but because the impulse is delayed at the AV node or bundle of His, the PR interval is longer than normal (i.e., it exceeds 200 milliseconds). Each P wave is linked in a 1:1 fashion to each QRS complex. QRS complexes of normal duration suggest that the delay is occurring at the level of the AV node, whereas wide QRS complexes suggest that the delay is infranodal.
Regularity: regular
Rate: variable, can occur with normal rate, bradycardia or tachycardia
P wave: upright and uniform, one for every QRS complex
QRS complex: < 0.12 second
PR interval: > 0.20 second
Second-Degree AV Block Type I
Because some impulses are not conducted through to the ventricles, the ratio of P waves to QRS complexes is greater than 1:1. Because each impulse is delayed a little more than the last until eventually one impulse is completely blocked, the ECG shows progressive lengthening of the PR interval with each beat, then a P wave that is not followed by a QRS complex (a “dropped beat”). In most cases, the RR interval decreases before each dropped beat. After the dropped beat, impulse conduction through the AV node resumes and the sequence repeats.
Regularity: irregular in a pattern
Rate: variable, usually < 100 bpm
P wave: upright and uniform; more P waves than QRS complexes
QRS complex: < 0.12 second
PR interval: becomes progressively longer until a P wave is not conducted, then cycle repeats.
Second-Degree AV Block Type II
Second-degree AV block type II is characterized by a constant PR interval. Because impulses are intermittently blocked, there are more P waves than QRS complexes.
Regularity: regular (2:1), unless conduction ratio varies
Rate: usually < 100 bpm (atrial and ventricular), tendency for bradycardia
P wave: upright and uniform; more P waves than QRS complexes (2:1, 3:1, 4:1 or variable)
QRS complex: < 0.12 second
PR interval: < 0.20 second or prolonged; constant for every QRS complex.
Third-Degree AV Block
In third-degree AV block, there is no electrical communication between the atria and ventricles, so there is no relationship between P waves and QRS complexes. The RR interval is constant. The PP interval is constant or slightly irregular. If pacemaker cells in the AV junction stimulate ventricular contraction, the QRS complexes will be narrow (less than 120 milliseconds in duration). Impulses that originate in the ventricles produce wide, bizarre QRS complexes.
Regularity: usually regular RR interval, regular PP interval
Rate: varies depending on escape focus; junctional (40–60 bpm) and ventricular (< 40 bpm)
P wave: upright and uniform, more P waves than QRS complexes
QRS complex: < 0.12 second if junctional escape, ≥ 0.12 second if ventricular escape
PR interval: total dissociation from QRS complexes
Tachyarrhythmias can be categorized as narrow complex or wide complex.
Narrow-complex tachyarrhythmias include sinus tachycardia, atrial flutter, atrial fibrillation and supraventricular tachycardia. These tachyarrhythmias usually originate in the atria or AV node and run normally through the bundle branches, producing a normal QRS complex.
Wide-complex tachyarrhythmias originate in the ventricles and include ventricular tachycardia (monomorphic and polymorphic) and ventricular fibrillation. Supraventricular tachycardia with aberrant conduction can also produce a wide-complex tachyarrhythmia.
Sinus tachycardia is the most common tachyarrhythmia. It is identical to normal sinus rhythm, except the rate is between 100 and 150 bpm.
Atrial flutter is caused by an ectopic focus in the atria that causes the atria to contract at a rate of 250 to 350 bpm. The underlying mechanism of atrial flutter is most often a re-entrant circuit that encircles the tricuspid valve annulus.
Supraventricular tachycardia (SVT) is an arrhythmia originating above the ventricles. In general, the rate is greater than 150 bpm, which helps to differentiate SVT from sinus tachycardia. SVT can be classified as AV nodal re-entrant tachycardia (AVNRT), AV-reciprocating tachycardia (AVRT) and atrial tachycardia.
This rhythm is seen in patients with:
Low potassium and magnesium levels.
Family history of tachycardia.
Structural abnormalities of the heart.
Adverse reactions from certain pharmacologic agents (e.g., antihistamines, theophylline, cough and cold preparations, appetite suppressants).
Certain medical conditions (e.g., cardiovascular disease, long-term respiratory disease, diabetes, anemia, cancer).
Illicit drug use.
Atrial fibrillation is caused by multiple ectopic foci in the atria that cause the atria to contract at a rate of 350 to 600 bpm. Rarely, the atrial rate may be as high as 700 bpm. The AV node only allows some of the impulses to pass through to the ventricles, generating an irregularly irregular rhythm that is completely chaotic and unpredictable.
Atrial fibrillation can occur in young patients with no history of cardiac disease. Acute alcohol toxicity can precipitate an episode of atrial fibrillation in otherwise healthy patients. However, atrial fibrillation commonly occurs in the presence of underlying heart disease, lung disease, hyperthyroidism or myocardial infarction.
Ventricular tachycardia occurs when a ventricular focus below the bundle of His becomes the new pacemaker. The ventricles contract rapidly (usually at a rate faster than 100 bpm) and usually with a regular rhythm. The rapid ventricular rate significantly diminishes cardiac output and can only be sustained for a short period before the patient becomes hemodynamically compromised. Ventricular tachycardia can quickly turn into ventricular fibrillation, leading to cardiac arrest.
In atrial flutter, atrial contraction occurs at such a rapid rate that discrete P waves separated by a flat baseline cannot be seen. Instead, the baseline continually rises and falls, producing the “flutter” waves. In leads II and III, the flutter waves may be quite prominent, creating a “sawtooth” pattern. Because of the volume of atrial impulses, the AV node allows only some of the impulses to pass through to the ventricles. In atrial flutter, a 2:1 ratio is the most common (i.e., for every two flutter waves, only one impulse passes through the AV node to generate a QRS complex). Ratios of 3:1 and 4:1 are also frequently seen.
Regularity: usually regular (could be irregular with variable conduction)
Rate: varies with conduction; < 100 bpm is controlled; > 100 bpm is uncontrolled (rapid ventricular response); usually has ventricular rates of 75 bpm (4:1), 100 bpm (3:1) or 150 bpm (2:1), depending on conduction ratio
P wave: none; flutter (F) waves; characteristic “sawtooth” baseline
QRS complex: < 0.12 second
PR interval: not discernible
Supraventricular Tachycardia
In supraventricular tachycardia (SVT), the P waves may be absent or abnormal. There is minimal to no beat-to-beat variability and the heart rate is usually greater than or equal to 150 bpm.
Regularity: regular; minimal beat-to-beat variability
Rate: > 150 bpm
P wave: absent or not clearly identifiable
QRS complex: < 0.12 second
PR interval: if P waves are visible, PR interval may be shortened or lengthened depending on mechanism
Atrial Fibrillation
The two key features of atrial fibrillation on ECG are the absence of discrete P waves and the presence of irregularly irregular QRS complexes. The baseline appears flat or undulates slightly, producing fibrillatory waves.
Regularity: irregularly irregular
Rate: varies with conduction; < 100 bpm is controlled; > 100 bpm is uncontrolled (rapid ventricular response)
P wave: none; fibrillation (f) waves; chaotic baseline
QRS complex: < 0.12 second
PR interval: not discernible
Monomorphic Ventricular Tachycardia
In ventricular tachycardia, the QRS complexes are wide (lasting longer than 120 milliseconds) and bizarre in shape. When there is only one ectopic focus in the ventricles, monomorphic ventricular tachycardia is seen on the ECG (i.e., the QRS complexes are generally the same bizarre shape). Monomorphic ventricular tachycardia may also be seen with reentrant rhythms.
Regularity: regular
Rate: > 100 bpm
P wave: not discernible
QRS complex: ≥ 0.12 second, uniform in shape
PR interval: not discernible
Polymorphic Ventricular Tachycardia
In polymorphic ventricular tachycardia, which occurs when there are two or more ectopic foci, the QRS complexes vary in shape and rate.
Regularity: irregular (can appear regular due to fast rate)
Rate: > 100 bpm
P wave: not discernible
QRS complex: ≥ 0.12 second, variable in shape
PR interval: not discernible
12 notes
·
View notes
Text
my actual fav thing from the "dan and phil finally tell the truth video" was the dan hates animal crossing part. esp where dan's like "AND I WILL PLAY THE NEXT GAME AND I'LL MAKE TWO FUCKIN TWEETS ABOUT IT AND GET THAT ENGAGEMENT" like. that was more truthful than anything else they said LMAO like as someone who's been playing new horizons daily honestly i kinda hate the decorating aspect it gets way too stressful for me and as opposed to the sims you can't customize your island in like its own menu (except for in the dlc! but not on your own dang island!!!) so it's way more annoying to plan out unless you wanna like keep changing the time on your switch and sure its not actually that complicated to do but it is time consuming and i burn out and basically i get it i have adhd too
#new leaf was so much simpler man you just used a random users cool dirt path qr and then had to do like public projects in order to get like#a fountain installed etc. but that made it feel more special that oh the fountain is in this location! and there was more variety in fruit!#and idk i just feel like even tho new horizons is inarguably the most accessible ac#it misses a little bit of the magic#i played a bit of wild world and i think cuz i didnt grow up w it it was a bit too simple but then theres something great about that too#basically nh is more complex which makes it more annoying and im thinking of destroying my island again#this is in no way about dnp anymore LMAO
11 notes
·
View notes
Text
Another day another piece of common medical paraphernalia drawn in a completely bonkers way in some random fanart across my dash. I'm feeling Nurse Emotions, which are like Shrimp Colors but more pedantic.
one of these days I will make a giant reference post of what some common medical devices are in the hospital and what to google to find reference of them and then I will have fixed it, and all the IVs will stop being inserted upside-down, and the nasal cannulas will be accurate, and the EKG/telemetry strips will stop being in weird arrhythmias.
#I'm not actually mad I'm just performing some anger to go with my amused frustration haha#But also: it was a REAL bad nasal cannula#y'know sometimes someone fully renders a picture of a young otherwise healthy character in a hospital after a trauma#and they have a heart monitor and they have no P or T waves at all and a weird enormous QRS complex#HEY HOSS I YOUR NURSE WOULD BE PRETTY CONCERNED IS ALL I'M SAYING#HEY BUD WHY DO YOU HAVE A HEART BLOCK YOU'RE 25
120 notes
·
View notes
Text

why is there a discernible p wave in my notes
#not my sideblog notes going into atrial flutter!#society if i had a normal qrs complex in my notes#maggie goes to college#btw. when will my grades from the cardiovascular exam return from the war#i need to know if i am correct abt treatment plans for my notes graph.#maggie.txt
8 notes
·
View notes
Text
give me literally any other method of accessing information besides a fucking qr code.
this is not a case of "wah new technology scary". this is another iteration on "you should avoid clicking shortlinks from people you don't trust because you can't see where they will actually take you and could easily direct you through a malware site before you get where the person giving you the link promised it would go, if you even get the promised site at all and not a phishing site made to look like it".
qr codes are just fucking pixels. i can't read that shit. i don't know where it's going or what it will prompt my phone to download. no fucking thank you. give me a god damn url to type in or fuck off.
#at least with a bar code i COULD figure it out given time and references they're not that complex#but a qr code?? nah#stfu blue#okay to reblog
11 notes
·
View notes
Text
QRS Complex Abnormalities
Abnormalities in the QRS complex of an electrocardiogram (ECG) provide significant insights into the heart's electrical activity, shedding light on potential cardiac conditions. The QRS complex represents ventricular depolarization, and variations in its morphology can signify various underlying issues. An abnormally widened QRS complex may indicate conduction delays, often associated with bundle branch blocks or certain cardiac diseases. Conversely, a narrowed QRS complex may suggest pre-excitation syndromes or accelerated conduction pathways. Additionally, fragmented or notched QRS complexes can be indicative of myocardial scar tissue, reflecting previous cardiac events. Identifying and understanding QRS complex abnormalities are crucial for healthcare professionals in diagnosing and addressing potential cardiac concerns. Regular ECG monitoring, coupled with a thorough clinical assessment, remains essential for a comprehensive evaluation and timely intervention in the realm of cardiac health.
#ecg#ecg monitoring#health#health and wellness#medical devices#medical device#heart#heartache#qrs complex abnormalities#abnormal ecg waves
1 note
·
View note
Text
Safe and Sound by Mercury Stardust

Don’t panic—Mercury Stardust, AKA The Trans Handy Ma’am is here to help!
For too many people, the simple act of contacting a plumber or repair person can feel like a game of chance. As a transwoman and a professional maintenance technician, Mercury Stardust has discovered (the hard way) that we live in a world with much to fear. If you've ever felt panicked about opening your home to strangers in order to fix a maintenance issue, this book is for you.
Renting a home can be a complex process—from finding a safe and affordable space, to hiring help for moving in and out, and of course, managing any repairs that come up during your stay.
You deserve to feel empowered to take matters into your own hands—and it’s not as hard as you might think. In this book, Mercury will show you how to tackle the projects that need improvement in your home—from how to properly fix a clog in your bathroom sink and safely hang things on your walls to patching small and medium drywall holes.
Safe and Sound includes:
Guidance for over 50 simple home maintenance projects, such as replacing your showerhead and troubleshooting a faulty garbage disposal.
Chapters covering basic and handy repairs for your plumbing, electrical, carpentry, and safety needs.
Advice tailored to renters to minimize permanent changes.
Helpful illustrations and QR code links to videos to help you on your journey.
Remember—a little bit of knowledge can go a long way toward making you feel more safe and in control of your own life.
#safe and sound#mercury stardust#transfem#trans book of the day#queer books#trans books#bookblr#booklr
2K notes
·
View notes
Text
i see way too many people calling stuff ai when its literally just..... hardcoded pattern recognition......
whoop de doo the thing you made for a specific purpose fufilled that purpose. thats not an ai thats just a program. shut up.
"oh this new ai powered webcam can zoom in on anything with these four squares on it!!" thats not a fucking ai thats image pattern recognition, all it does is scan the visible area for specific patterns, and once recognized, it zooms in. thats it. a fucking qr code scanner is more complex than that. its not ai. shut up.
"this logo maker uses ai to make images" no it doesnt. it randomizes images within the bounds of set fields and assets. its randomization giving a number of results to choose from. thats not fucking ai. shut up.
a real ai is a program that trains itself to respond to inputs "naturally" without instruction using trial and error, for example if an actual ai was to go through a maze,
step one, makes random movements
by making these random movements and bumping into walls, it learns that bumping into walls is an error
step two, explores randomly without touching walls
the ai doesnt know there is an end goal, however it will learn this if moving in a path that isnt directly connected to the exit is an error
step 3, the ai uses what its learned it should not do, and takes the path that is connected to the exit, and the task is complete.
ai is not pattern recognition, its learned pattern adaptation through time. ai is not randomization of assets. it is randomization with consequences that shapes it into a predictable behaviour. shut. up.
#rant#ai#artificial intelligence#programming#coding#tech#technology#please shut up#please shut the fuck up#im so tired#so very tired
280 notes
·
View notes
Text
Days of Love / Nine-Colored Deer Commissions!




Days of Love is here, so it’s time for more commissions! Sadly I did not get my beloved umbrella, but oh well.
All prices are USD, commissions come with coloring and and shading, items I want very much are marked with a ✨
SLOTS:
$4.99 - Classy Cravat (OPEN) - half body
$14.99 - Serendipitous Scepter ✨ (OPEN) - full body with light creature friends
$14.99 - Gift of the Nine-Colored Deer ✨ (OPEN) - full body with light creature friends
$17.99 - Meteor Mantle ✨✨ (OPEN) - actually two slots for this as I want to get one for a friend, full body with simple-moderate complexity background.
$19.99 - Radiance of the Nine-Colored Deer ✨✨ (OPEN) - full body with background or two full bodies
$19.99 - Days of Love Gondola ✨, Swing, or Seesaw (OPEN, OPEN, and OPEN) - full body with background or two full bodies
PROCESS:
You message me letting me know what you want, and I’ll tell you what kinds of reference photos I’ll need to do the art.
Exchange QR codes! This can be skipped if we’re already Sky buddies.
We discuss what kind of pose you’d like your character in, and I’ll sketch out some potential poses to show you.
Since there’s a 3-day waiting period before gifting IAPs is an option, during those days I’ll send you progress shots with the option to change anything you don’t like.
You will receive the final art piece once the IAP has been received. Throughout the waiting period, I may also send you little random doodles of your skykid. Please stop trying to pay me for the random doodles. Please.
As usual, I won’t do anything NSFW, with heavy gore, hateful, or ridiculously complex (sfw furries are okay, so is light gore). DM me if you have any questions or are interested!
✨More Examples of My Art✨


#sky cotl#sky children of the light#sky cotl art#thatskygame#my art#sky fanart#sky: cotl#sky: children of the light#skycotl#sky cotl commission#sky colt#that sky game#sky kid#skyblr#sky game
85 notes
·
View notes
Text
1 minute read
A college has apologised for displaying a sign asking students to report trans exclusionary radical feminist ideology, or Terf, using a QR code.
The Institute of Contemporary Music Performance in north London was criticised for the sign telling staff and students that it had “zero tolerance” of Terf ideology, which it called a specific form of transphobia.
The term is used as an insult to people who have so-called gender-critical beliefs that biological gender cannot change.
Kathleen Stock, the academic forced out of Sussex University for her views on sex and gender, said on social media: “Witch hunts have QR codes now. Find the witch, use the QR code, ‘report and support’. Modern life is wonderful, isn’t it.”
Maya Forstater, who won a case at an employment tribunal after being sacked for gender-critical views, said: “Any staff or students @ICMPLondon who face discrimination or harassment because of your gender-critical views: this is the exhibit to put on page one of your tribunal bundle.”
The sign at the private music college said: “What is a Terf? Trans exclusionary radical feminist ideology is a specific form of transphobia. The primary Terf assertion is that trans women are not women and accordingly have no place in women’s spaces.” It added “Report + Support”, with a link to a QR code.
Paul Kirkham, chief executive of the college, said: “Our intention, following discussions with our student community, had been to communicate the definition of Terf to help clarify what we considered to be growing misconceptions around what the term means. We got it wrong. The signage is clunky and we can see how it can be misinterpreted.” He added that the sign had been removed.
“We’d like to make it clear that our zero-tolerance policy refers to our approach to discrimination of any kind,” he said. “We have a confidential reporting process in place that gives students and staff a direct line of contact with senior trained institute staff if they feel they are in any way being victimised, discriminated against or being made to feel otherwise uncomfortable.
“We recognise that this is a complex and important subject and, like most other organisations, we’re constantly learning. We work closely with our community and welcome debate in order to make sure we’re providing the best environment we can. It is our absolute aim to make all of our students, staff and the wider community feel welcome and included at the institute.”

809 notes
·
View notes
Text
Kiana’s Cardioversion
Kiana was a 25 year old black girl who worked as a personal trainer. She stood at 5’3 with a slim, but fit and toned build. Kiana had dark, medium length, curly, natural hair with a side part. Her eyes were a darker shade of brown, and she had a nose ring and bellybutton ring.
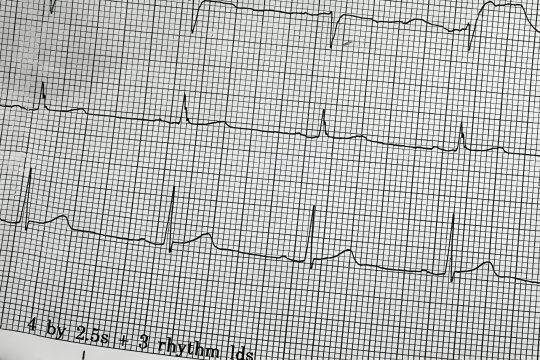
Earlier today, Kiana found herself in our emergency department after developing an array of worrisome symptoms completely out of the blue. She experienced a severe tearing pain in her chest, heart palpitations, and shortness of breath. As a result, she was sitting in the upright position on one of our trauma room tables. She was barefoot, and stripped down to only her sports bra and matching underwear. There were EKG electrodes stuck onto Kiana’s chest, and there were IVs set up in both arms. She was visibly uncomfortable, writhing in pain, squirming around a bit.
The heart monitors were beeping, chirping, and alarming rather loudly, creating a bit of tension and sensory overload in the exam room. The readings on the monitors were a bit concerning as well. Kiana’s heart was racing at 170 beats per minute, and her blood pressure was low at 75/40. The rhythm itself was a tachyarrhythmia of some sort. The EKG showed a narrow QRS complex and possible atrioventricular block. The symptoms and EKG readings pointed Dr Lindsay and in a few very different directions. One possibility was an NSTEMI heart attack, but how likely is that in a 25 year old personal trainer? Next was junctional ectopic tachycardia, which is an uncommon, but potentially deadly arrhythmia that tends to occur in infants or people who recently had open heart surgery. The other possibilities were an electrolyte imbalance, particularly potassium, or her symptoms could be attributed to stimulant use from substances such as cocaine, meth, or molly.
Since the possibilities were all very different, Dr Lindsay had to be thorough and order a whole bunch of tests. First off were blood samples. A CBC, a BMP, a toxicology screening, a cardiac enzyme test, an HCG, and a d-dimer were all drawn and sent off to the lab for stat analysis. Because Kiana was experiencing chest pain, Dr Lindsay decided to order a chest x-ray and an echocardiogram. Unfortunately, both tests didn’t help Lindsay narrow anything down. The chest x-ray came back completely normal, and the echocardiogram showed slight thickening of the ventricular septum, which is a sign of hypertrophic cardiomyopathy. But some of the other symptoms didn’t point in that direction. So what exactly was going on with Kiana? Dr Lindsay was certainly stumped. All she could do was treat Kiana’s symptoms, and hope the lab tests would come back soon and show something noteworthy.
Of course the lab was taking their sweet ass time with Kiana’s stat labs. And of course Kiana started to get worse. Her heart raced faster and faster, and the arrhythmia became more troublesome. Dr Lindsay wasted no time and started chemical cardioversion, urgently trying to calm Kiana’s heart and relieve her symptoms a bit. But as the next little while unfolded, Kiana’s condition didn’t improve, almost as if the antiarrhythmic medications did absolutely nothing. When chemical cardioversion doesn’t work, the next step is electrical cardioversion.
Dr Lindsay explained to Kiana that her heart was in a dangerous rhythm, and they had to give it a quick shock to make it beat normally again. Kiana was a bit nervous and hesitant, but nodded in response to Dr Lindsay, reluctantly agreeing. The defib pads were then stuck onto Kiana’s chest and charged to a lower setting of 125 joules. Lindsay told Kiana the defibs were ready, then pushed the shock button a few seconds later. “MMMM!” Kiana moaned loudly, squeezing her eyes shut, wincing in pain from the quick jolt of electricity. After the shock, Dr Lindsay studied the monitors for a few moments and listened to Kiana’s heart and lungs with a stethoscope. Lindsay discovered there was no change in the rhythm and informed Kiana she had to be shocked again. The defib pads were recharged to 150 joules, and the next shock was sent into Kiana’s racing heart. Her torso shivered, and she clenched her chest with one hand while her face had a distressed look.
Dr Lindsay repeated the same process as before, studying the heart monitors and listening to Kiana’s heart and lungs. Just like before, Dr Lindsay didn’t see any change whatsoever and needed to shock Kiana again at 175 joules. The pads were charged and readied, and Kiana received the next shock. Her chest propelled forwards, and she let out a grunt, reacting to the electricity racing through her while wide awake. This shock failed to correct the arrhythmia, and Lindsay informed Kiana she had to be shocked again. “NO MORE! NO MORE!” She protested, writhing around on the table, on the verge of tears. Despite Kiana’s protests, Lindsay shocked her again at 200 joules. “AHH!” Kiana yelped. After that shock, she started to breathe heavily and tears started to roll down her face. “PLEASE! NO MORE, NO MORE!” she cried, begging Dr Lindsay to stop. But the arrhythmia was still there, so unfortunately Lindsay was unable to stop the cardioversion. The defibs were recharged to 225, and the next shock was delivered. Kiana gasped and cried out reacting to the shock, but just like all the others, the arrhythmia was still there. “PLEASE… JUST STOP! NO MORE! I DON’T WANNA DIE!” Kiana cried out hysterically, squirming and writhing around on the table wanting the nightmare to end.
The defib pads were recharged to 250 joules- twice the strength of the very first shock, and the next shock was administered. Kiana’s body trembled, and she scrunched her toes at the far end of the table trying to fight the pain, showing off the white nail polish on her toes and the thick, soft, wide wrinkles throughout the soles of her size 6 feet. Immediately after that particular shock, Kiana’s breathing slowed a bit. Her head lolled to the side and her eyes rolled back. Kiana’s body went completely limp, and the heart monitors were practically shouting at Dr Lindsay and the rest of our team.
It didn’t take long to realize that Kiana had gone into v-fib, so the team had to change gears and start running a normal code. The bed was lowered, and Kiana’s sports bra was snipped off, allowing her perky, deceptively large breasts to spill out. CPR was immediately started, causing Kiana’s chest to cave in, and her belly to ripple out. At the head of the bed, her airway was the priority. A 7.0 ET tube was carefully but quickly navigated into her airway, being held in place by a blue tube holder once proper placement was confirmed. Post intubation, CPR was halted, and the team decided to try their luck with the defib paddles, rather than the pads. The paddles were gelled, charged to 250 joules, and pressed up against Kiana’s bare chest. KA-THUNK! Her small body was thrown around effortlessly on the table while her eyes remained half open, almost as if she was still watching the events unfold around her. V-fib was still on the monitors, so the paddles were readied once again, and Kiana received a 300 joule shock. Her chest shot up and her back arched. Her big, perky tits jiggled around while she crashed back down onto the table. Kiana remained in v-fib even after this shock, so she was defibbed again after a cycle of CPR and ambu bagging. Her shoulders shrugged forwards. Kiana’s hands made loose fists from the electric current that ran through her body. Unfortunately, the shock didn’t bring her back.
With a few unsuccessful shocks out of the way, the team decided to resume chest compressions and push meds into Kiana’s IV line. Kiana’s chest was pumped violently but rhythmically for several minutes, but the compressions and 2 doses of meds failed to restart her heart. The team decided to defib Kiana again. The paddles were gelled, charged to 360, and she was shocked again. Kiana’s body twitched sharply in response to the shock, but her heart didn’t start back up. “again! Everyone…CLEAR!” Lindsay shouted, immediately shocking Kiana again. KA-THUMP! Kiana jolted violently on the table while her eyes remained open, staring up above with an expressionless gaze. Kiana was shocked unsuccessfully another 3 times after that and given another dose of meds, but v-fib was the clear winner of the battle up to that point.
Dr Lindsay was reluctant to give up on the beautiful young lady. However, the code became redundant the longer it went on. Kiana would receive a few shocks, then it was back to a few minutes of CPR and meds, rinse and repeat. At the 30 minute mark of the code, it was noted that Kiana’s pupils were fixed and dilated. Dr Lindsay knew she exhausted all possible options in this particular case. At that point, resuscitation efforts were ceased, and Kiana’s time of death was called at 4:48pm. The ambu bag was detached and the chirping, flashing v-fib monitors were turned off. The EKG electrodes were disconnected, and the defib pads were peeled off. The defb gel was wiped off of Kiana’s bruised, battered chest. Her eyes were gently shut for the final time, and her body was covered up. Lastly, a toe tag was filled out and placed on the big toe of her left foot. The tag dangled against the wrinkled soles of Kiana’s feet, signifying a sudden and tragic end for the beautiful young lady.
66 notes
·
View notes
Text
#1 New York Times Bestseller
Don’t panic—Mercury Stardust, AKA The Trans Handy Ma’am is here to help!
For too many people, the simple act of contacting a plumber or repair person can feel like a game of chance. As a transwoman and a professional maintenance technician, Mercury Stardust has discovered (the hard way) that we live in a world with much to fear. If you've ever felt panicked about opening your home to strangers in order to fix a maintenance issue, this book is for you.
Renting a home can be a complex process—from finding a safe and affordable space, to hiring help for moving in and out, and of course, managing any repairs that come up during your stay.
You deserve to feel empowered to take matters into your own hands—and it’s not as hard as you might think. In this book, Mercury will show you how to tackle the projects that need improvement in your home—from how to properly fix a clog in your bathroom sink and safely hang things on your walls to patching small and medium drywall holes.
Safe and Sound includes:
Guidance for over 50 simple home maintenance projects, such as replacing your showerhead and troubleshooting a faulty garbage disposal.
Chapters covering basic and handy repairs for your plumbing, electrical, carpentry, and safety needs.
Advice tailored to renters to minimize permanent changes.
Helpful illustrations and QR code links to videos to help you on your journey.
Remember—a little bit of knowledge can go a long way toward making you feel more safe and in control of your own life.
https://amzn.to/3TzY2Jh
70 notes
·
View notes
Text

Hi friends! We have a couple of updates to share.
Firstly, Seraj needs more than $3,300 to pull off his final Ramadan project before Eid. He wants to distribute it on the last day of Ramadan, which is in 3 days, so we need to get to $20k ASAP!
contribute at bit.ly/serajfund
The financial situation in Rah Fah continues to decline, with intermediaries taking a 15-17% cut when people get cash out. He is so hopeful that this project will work out! Helping others and bringing smiles to faces–especially those of children–is clearly one of Seraj’s passions.
Here are the project details, all thought up by Seraj himself. He has amazing ideas! 125-130 cash envelopes containing either 50 or 100 shekels each. Seraj will distribute them based on how large each family is. Seraj will also make 40 envelopes for kids, each containing 20 shekels.
Currently, Seraj’s plan is to distribute his envelopes on the last day of Ramadan, before Eid al-Fitr. Last time he tried to print something, the printer had no electricity. He has a plan this time for checking in early to make sure he has a chance to print.
Working with Seraj on his mutual aid projects has been such a tangible reminder that we reject the notion of charity (which is very rooted in the white savior complex and pity of Black and Brown folx), and even allyship (not enough action) instead are partners and collaborators with Seraj self directing, leading us, and constantly motivating us to to get to the next goal so he can achieve his vision!
Because Seraj and his family have managed to survive, he’s been able to give back. No NGOs or governments, just a 21-year-old young man helping as many of his neighbors as he can. In his words, “This is my duty, sisters, as long as I can help! Why don't I do that!”
Seraj is genuinely a superstar to everyone on our team. His generosity is humbling to us. We have so much to learn from Pale-eh -steinians.
Secondly, we have a date for our upcoming virtual dance party! Mark your calendars for Monday, April 29th in the evening (Pacific time). Sky is hosting this event to hype up our virtual auction for Seraj. Follow Sky on Instagram for more details @rebirthgarments or @radicalvisibilitycollective
If you’d still like to contribute items to the auction, go to bit.ly/fundraiserforseraj ! Seraj’s Support Soirée would like to offer an item or service for every budget. And we encourage a wide variety of dough-nation types! While many of them will be creative objects, they do not have to be.
Some examples:
a book you love or wrote
a framed photograph
a massage (local area bidders only)
a meditation session
a piñata
a tarot reading
a t-shirt you love or designed
stickers
a virtual lesson on social media marketing
visual art
a virtual dance lesson
Your items will be listed this week on Give Butter! (stay tuned for details!)
Our support soiree dance party will hype up the auction featuring selections from the archives of Rebirth Garments fashion performances while you can dance with Sky!
Thank you so much for being here for Seraj. He and his family are so deeply grateful for all of the ways folks have supported them and partnered with them to help others. And our team is so thankful for how you all have stepped up. Please share and contribute!
-Written by my team member Bex with additions by me!
[image Description: a flyer featuring a photo by Seraj of a small little kid with a blue plastic bag full of fresh fruits and vegetables. The kiddo has a heart emoji over their face and is smiling really big. They are wearing a red shirt that says “sleep time” with a sleeping bear on it. They are standing on a sandy ground in front of a tent. Text to the right of the photo on a red background reads: Gaza Sky
Seraj’s mutual aid project for
Ramadan in Rah-fah
For part 2 of Seraj’s Ramadan project, he gave out 32 food parcels for 32 families around him in the displacement camps.
Send support to his family + others!
bit.ly/serajfund “
Underneath is a QR code with the link. ]
#gaza strip#gaza genocide#gaza#free gaza#radicallyvisible#queerfashion#mutual aid#go fund me#fundraising#free palestine#gazaunderattack#palestine#stand with gaza#vetted#I personally vetted this fundraiser
35 notes
·
View notes
Note
Is there a way to safely mask my email address while sending an esim to those who are organizing?
This is one you’re probably going to get better info from googling. Encrypting your email is a bit too technically complex (for me) to explain here, but afaik there’s an org (gazaesims was an active group last i checked?? run by Gaza journalist Mirna El Helbawi I believe) with an email you can send the QR code.
#heads up tho#while i’m fairly tuned into this#i’m not an organiser by any means#and my info (and therefore advice) is often out of date because the situation changes so fast#ask#palestine
61 notes
·
View notes
Text
Posting this because I really want that classy cravat, while I also open it for a new cape. Though classy cravat is my main priority.
Classy Cravat: $4.99 (OPEN) - portrait
Days of Love Meteor Mantle: $17.99 (OPEN) - half body, full body, or two portraits






Info
Will only draw your skykids. Send me your skykid reference and tell me what pose you would like me to draw.
Can draw some sky creatures: mantas, birds, manatees, and crabs
Two choices of background: simple color or sky (see the examples)
Color backgrounds: one color or multi colors (tell me which colors you would like)
Sky backgrounds: day or night
No complex art
No NSFW
Send your QR code and I will unlock the friendship tree for you.
I will send you the sketch and will continue the piece once you improve it and send the iap.
Also, I will mostly draw on weekends. If you decide to commission me, I recommend you to dm me before that. (Btw I got the first three days of holidays this week)
#sky children of the light#sky cotl#that sky game#thatskygame#skyblr#sky cotl fanart#sky kid#sky kids#skykid#fanart#sky iap commission#sky iap commissions#sky cotl commissions#sky cotl commission#sky commissions#sky commission#commission#days of love
34 notes
·
View notes
Text
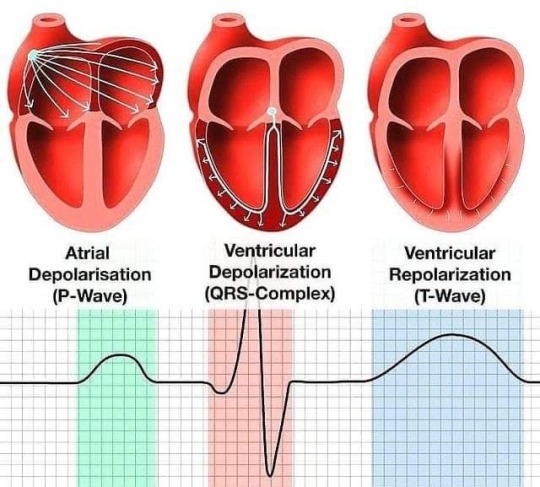
🫀Let's look into atrial depolarization (P wave), ventricle depolarization (QRS wave), and ventricular repolarization (T wave)
🔵 Atrial Depolarization - The P Wave 💙 At the heart's command, the P wave sets the stage, representing the initial electrical impulse that triggers the contraction of the atria. It's the starting point, a signal that initiates the beat, much like the ignition of a well-tuned engine.
⚡ Ventricle Depolarization - The QRS Wave ⚡ Moving deeper into the heart's rhythm, we encounter the QRS complex. This trio of waves illustrates the ventricles' forceful electrical activation, pushing blood out to our entire body. Think of it as the powerful engine revving up, propelling us forward with every heartbeat.
🌀 Ventricular Repolarization - The T Wave 🌀 As the heart cycle nears its end, the T wave emerges, symbolizing the ventricles' recovery and preparation for the next cycle. It's like the engine cooling down after a hard run, regaining composure before the next surge of activity.
109 notes
·
View notes
Last Seen Blogs

nataliavalas
Nataly
nataliavalas
Nataly

testinglayoutlikeaboss
The reason I like you,
Got millions millions millions

incorrect-tokyo-ghoul-quotes
incorrect-tokyo-ghoul-quotes

k0ra-kumori
Kora-Kumori