#anankastia
Text
would it confuse people too much if i started calling OCPD “anankastic PD”? maybe abbreviated to AKPD? (since OCPD doesn’t actually have obsessions or compulsions, and i want to normalise ICD [and PDM] models of disorders as much as the DSM has been online (it’s the americanisation of the internet btw))
13 notes
·
View notes
Text
Need anankastia headcanons
0 notes
Note
For the ask meme, 1, 2, 4, 5, 6, 23, 24. I'd do more but that is all I can remember.
What are your personality disorder(s)? If you have multiple, do you think you have a “main” one?
I have anankastic personality disorder (the DSM likes to call it "OCPD"; I don't think it's a particularly fitting name given how psych currently defines obsessions and compulsions and OCD and those don't particularly fit), NPD, and ASPD. I don't think I have a "main" one per se; some are worse/a larger part of my thinking/feeling/action at different times and they fluctuate. I used to think a lot about which of my disorders I'd get rid of first if I magically had the option one day. My answer has varied greatly over time, and I don't think I can pin down a consistent one. They all suck.
2. Do you have mental illnesses besides personality disorders? Do you think them or your personality disorders affect you more?
I have ADHD (I consider mine a disorder) and C-PTSD. I may also have some degree of OCD symptoms (leftover?), though I've always tried to bury them/ignore that they exist/pretend they're not that bad actually, and I don't think I can really accurately measure how badly it affects me, and trying to do so or just try to explain it in general/talk about how I experience it would require thinking about it which is always unpleasant to some degree. I usually just try to forget they exist.
My ADHD affects my ability to survive under capitalism fulfilling capitalist demands. It impacts my actions and decision-making and perceptions and behaviors 24/7. It's the reason why I know I will never be able to fully do the things I want to do which my anankastia requires me to do and why I fail at everything which requires skills, why I forget everything, why I'm answering this ask from 8/11 a month and a half later because I just Couldn't anytime earlier, why I'm still struggling hard and feel constant existential despair at the overwhelming workload in front of me which will never fully disappear, why I forget everything and why I'm a total mess.
I've only recently come to terms with the fact that I have C-PTSD, mostly because I didn't really understand that all the things I experienced/am experiencing were/are traumatic, and was in heavy denial and didn't really think my symptoms "counted" (was working off very normative models/explanations of what it looks like). For the past few months I've been examining myself more, including my subconscious physical and psychological reactions to certain things and their patterns and my difficulties doing certain things because of certain mental blocks and feelings those produce and how it is in fact woven into every aspect of everything I do too and how it has awful negative effects on me.
I don't know how to say which affects me "more." It would be like comparing apples and oranges. They all affect different aspects of me and my life (a great deal).
4. What would you like mentally ill people without personality disorders to understand?
That 1) you being misdiagnosed with a PD you don't have by saneists isn't an excuse to center yourself in discussions about our PDs rather than us, 2) yes the current psychiatric paradigms and diagnostic criteria are based on statist fallacies conflating current social/external harm/ongoing trauma with inherent harm/trauma and that needs to be corrected, 3) no that doesn't mean our PDs don't exist at all or that none of us would experience inherent distress post-revolution, 4) it does in fact also require paternalism to so arrogantly demand that you know what our minds are like more than we do, 5) in fact everyone who isn't us can shut up with your assumptions about what our minds must be like most of them are laughably simplistic and totally awful and completely off and make huge sweeping generalizations, 6) yes our experiences are in fact nuanced and complex and messy and often not what you expect including our relationships with compassion, empathy, kindness, anger, authoritarianism, entitlement, violence, victimization, and abuse, having them, not having them, perpetrating them, and/or fighting against them, 6) psychiatry is bad actually and please use your critical thinking and learn how to actually critique things even if they're part of the status quo, 7) no you cannot in fact predict with 100% accuracy someone's internal psychological profile based on some external behaviors you need to unlearn your impulse to do so and following the threads of your beliefs to their origins in carceral culture and start holding authoritarians accountable, 8) please learn what a disorder is, no it's not "when someone is abnormal," no it's not "when someone hurts others," 9) it costs you $0 to not use ableist/saneist slurs or insults or armchair-diagnosing there are literally dozens of other actually accurate things you could say, 10) someone fighting back against you oppressing/victimizing them is not "evil boundary-violating" or "gaslighting" or "abuse."
5. What would you like people with your personality disorder(s) to understand?
Fuck psych. They'll only get worse. Not worth it. Your instincts are right about them being full of bullshit and unable to understand much less help. Learn and cope and heal outside of authorities' radar.
Also, anankastia is incredibly misunderstood and erased, even among other people with PDs, and it sucks, and no one ever talks about it ever, and the few people who do talk about it usually just discuss more shallow surface-level versions of it which I have never been able to fully relate to at all given (what I feel is) the severity of my symptoms and their messiness and how deeply it is woven into every aspect of my life and mind and how tightly they all lock into each other in a way I don't think I can extricate myself from ever (pre-transhumanism, at least). I would appreciate more nuanced discussions and acknowledgment and advocacy for cases like mine (the hopeless ones that don't get happy-ending stories about the magical successes of DBT turning their entire life around and fixing all their problems).
Also, you don't have to be an edgelord to get NPD and ASPD destigmatized or accepted. You don't have to brag about being pro abuse or abusing others or assaulting others or dangerous or whatever. You do have agency and nuanced experiences. Also, it's okay to be cringe, and if you cringe at pastel uwu positivity then it's not for you but that doesn't mean it's objectively bad, wrong, or harmful. Also, fakeclaiming others/training yourself to hyper-scrutinize/fakeclaim others is not going to make you seem more valid/real/correct in the eyes of the neurotypicals. Best to deconstruct that early. Also, the pushback against "allowing minors to dx with PDs" is entirely based on numerous pseudoscientific and ageist fallacies which would appear obviously incorrect if you used a single moment of genuine critical thinking and analysis.
6. What would you want a mentally ill person who’s really struggling today to know?
I don't know. That there are people out there in the world fighting for liberation? That some of us have hopes and dreams and plans of totally eradicating our unwanted pain? Options for direct action, ways to contact people who can get you out of an abusive/unsafe situation? That trying is still worth it? That later/tomorrow will be better? That your brain is wrong and everything's okay and you're still okay? You're right and you're valid? I don't know.
23. What are your hardest mental illness symptoms?
When I was 6-11 years old I would probably say the anankastia, the absolute total overwhelming need for [X] to be [Y] way or to do [A] in [B] way despite that being physically impossible and the overwhelming fear of that happening and the intense pain/discomfort which would follow, and the intense pain/discomfort if I did do it correctly anyway because it was time-consuming and exhausting and extremely stressful trying to get it perfectly right all the time and punishing myself if I didn't get it exactly right and arguing with myself trying to figure out what Counted as "Right" in the first place.
When I was 12/13 I would probably say the NPD symptoms which were already showing up and the total paranoia of being criticized/being viewed as less "Good" at all in any way and going to drastic and hugely time-consuming measures trying to prevent that and trying to perfect that the need for which caused me intense constant stress and fear, and being criticized for harming others in an attempt to preserve my own self-esteem/sense of superiority which I need(ed) above all else and caused a major collapse in me and total despair and I couldn't cope with that, and I could hardly cope with any of my other mistakes/failures either.
Or maybe my intense self-hatred regarding my body influenced by my other disorders to cause a horrible eating disorder for several years(?) (recovered now dw).
In 2021 I would say "my overwhelming feeling of need to hurt/abuse/exploit/do injustices to others in order to get things right/feel psychological/emotional fulfillment/not-empty-and-feeling-like-nothing's-there and feeling like I can't/shouldn't hold to my ethical principles (what ethical principles?)/not considering the feelings of others and the horrible shit that would result from my plans which I singlemindedly pursued because I need it so badly and feel like I have no other option and if I don't do them I have nothing and oh shit things actually have consequences."
Right now? I'm not sure. I'm even more of a mess, and everything's too hard, and the last few nights I've successively had breakdowns after feeling significant existential despair. I'm still way better than I was in 2021 though, that was a total trainwreck.
24. What do you do to get over mental health slumps?
I cross my fingers and wait until I get lucky and they go away on their own. Apart from that, meds. My "coping skills" are nonexistent.
#ask#anon#late answer#ask games#pd#ocpd#anankastia#npd#aspd#ocd#c-ptsd#adhd#personal#about iris#iris's mental health#ok to rb
1 note
·
View note
Text
Hannibal Fic Rec
Anankastia by trixiethenerd42
Summary
“I know a relaxation method that will make you sleep better,” Hannibal said shamelessly.
“And what is this method?” Will already had something in mind, but all his neurons told him that it wasn't real. He swallowed hard and didn't move an inch, curious to know what would happen next.
“I think you already know, Will."
Between Shadows and Savor by trixiethenerd42
Summary
"Are you thinking about what we did, Will?" He said, his eyes fixed on the man in front of him.
Will looked away as he usually did. "I'm thinking of what we are, Hannibal. Of the strange connection we share."
Hannibal smiled serenely. "Don't worry about yesterday. We were just two souls, bound by a shared darkness, finding solace in the warmth of each other's company."
"Does that mean we're not anymore?" What if Will wanted to share Hannibal's warmth? What if he wanted that closeness again?
"Do you want us to be, Will?" The simple question was enough to make him panic.
Yes, he wanted to.
Symphony of Doubts and Desires by trixiethenerd42
Summary
Seeing that Will didn't respond, Hannibal insisted. "Tell me what you dream about."
"You." He responded quickly. "I often dream that I'm killing you."
Hannibal leaned back in his chair, his eyes sparkling with interest. "And how do you do that?"
"With my own hands. I strangle you until the breath of life leaves your body."
A smirk. "How does it feel to do this?"
The answer was simple and short. “Fucking fantastic.”
In the dim light of the office, Hannibal stood up, surprising Will.
"Come on, Will. Strangle me."
Or
How Hannibal and Will went from friends to something more complex.
#hannibal#nbc hannibal#nbc hannigram#hannibal nbc#hannigram#hannibal lecter#will graham#murder husbands#fic rec#ao3#ao3 fanfic#fanfic#fanfiction#archive of our own
21 notes
·
View notes
Link
1 note
·
View note
Photo

Why You Need to Understand the Latest Personality Trait: Anankastia
0 notes
Text
does anyone have a link to a reblog of anankastia’s post on how conduct disorder is a bad diagnosis? their account is gone and as such I can’t see the original post
1 note
·
View note
Text
hi if youre a narcissist, a histrionic, an antisocial, a borderline, a dependent, an avoidant, an anankastic, a paranoid, a schizoid, and/or a schizotypal, i love you ♡
#anankastia = ocpd#dogpost#misc#personality disorders#npd#hpd#aspd#bpd#stpd#szpd#ppd#ocpd#anankastia#dpd#avpd
78 notes
·
View notes
Text
// TW : ableism, ableist language, NPD stigma, antisemitic rhetoric, invalidation of autism and BPD
I would suggest you block this person. Please don't interact or argue with them, they're not worth it. Just block them.
Note : they go by they/them. Please respect their pronouns.
Screenshots :

First they claim "empaths" are the ones being oppressed while people with NPD are "endlessly defended". Then they say people with NPD are "the worst kind of abusers".
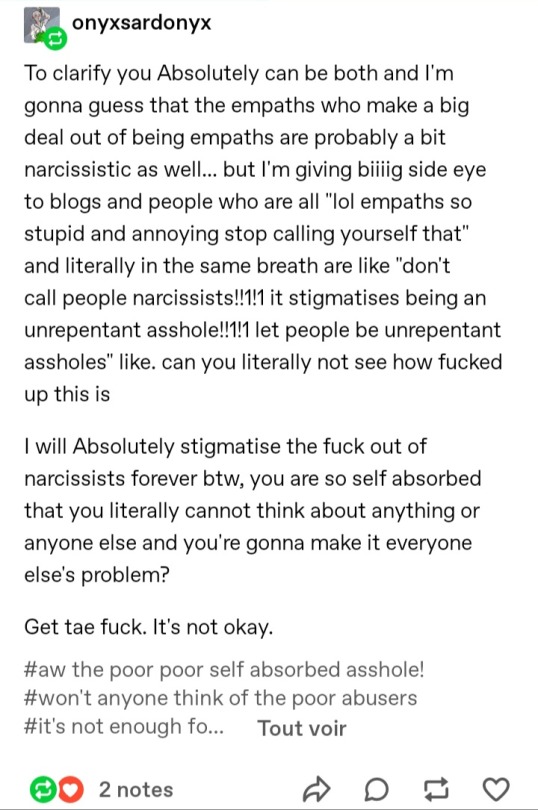
They go on to call people with NPD "unrepentant @ssholes" and equate an actual disorder with parapsychology (empaths).
The rest of the tags :
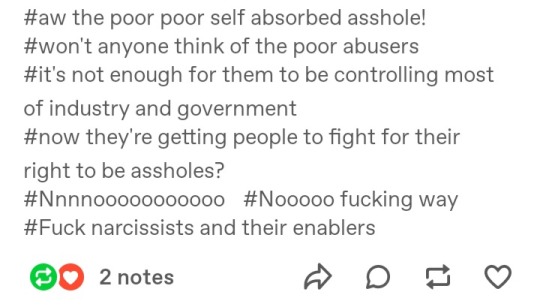
They also believe that people with NPD are "controlling most of the government", an ableist conspiracy theory with antisemitic origins.
At first i though they could be talking about narcissism the personality trait, not the disorder. But the tags on this reblog proved me wrong :
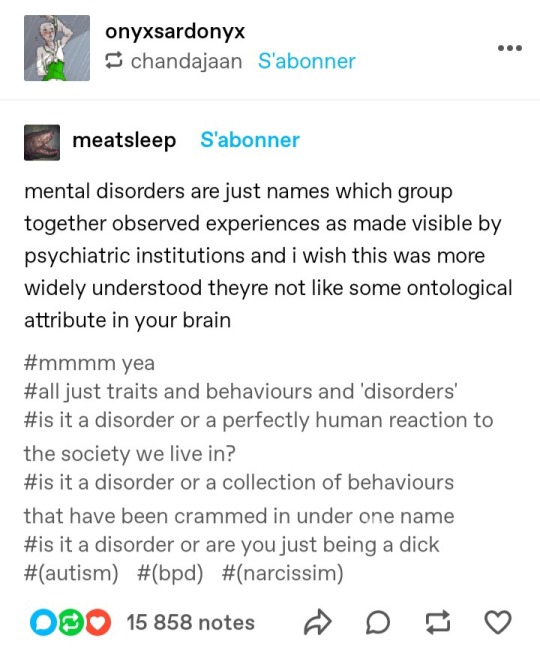
As shown by the order of the tags in parentheses, the third tag refers to autism, the fourth to BPD, and the fifth to NPD.
In addition to calling people with NPD "d*cks", they argue against the validity of disorder labels, including autism, BPD and NPD.
They call autism a "perfectly human reaction to the world we live in". They sound like the kind of ableist who downplays autistic struggles and claims that "everyone's a little autistic" or that autistic people are "the next step in human evolution".
- - - - - - - -
#please check anankastia's reblog in the notes for more info on the ableist conspiracy theory#ableism#ableism tw#npd#npd stigma#blocklist#ableist language#autism#bpd#antisemitism#ableist rhetoric#antisemitic rhetoric#empaths#narcissism#parapsychology#pop psychology
151 notes
·
View notes
Text
Personality Disorder Traits

Anankastia: The core feature of the Anankastia trait domain is a narrow focus on one’s rigid standard of perfection and of right and wrong, and on controlling one’s own and others’ behaviour and controlling situations to ensure conformity to these standards. The colors come from the OCPD flag that this is based off of.
Borderline pattern: The Borderline pattern descriptor may be applied to individuals whose pattern of personality disturbance is characterized by a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity. The colors come from the BPD flag that this is based off of.

Detachment: The core feature of the Detachment trait domain is the tendency to maintain interpersonal distance (social detachment) and emotional distance (emotional detachment). The colors come from the SPD flag that this is based off of.

Disinhibition: The core feature of the Disinhibition trait domain is the tendency to act rashly based on immediate external or internal stimuli (i.e., sensations, emotions, thoughts), without consideration of potential negative consequences. The pattern of light and dark mirrors that of the dissociality flag.

Dissociality: The core feature of the Dissociality trait domain is disregard for the rights and feelings of others, encompassing both self-centeredness and lack of empathy. The colors come from the ASPD flag that this is based off of.
These definitions of were taken from the ICD-11, which are used in classifying the singular “personality disorder.”
60 notes
·
View notes
Text
are the names of PDs actually good?
in this post i’m discussing each personality disorder’s name and alternatives (used in academia, not community based) and rating thembased on the following criteria:
✅ is it accurate?
✅ is it unique?
✅ is it easy to learn and read?
‼️ is it stigmatising or have stigma attached?
Antisocial
accurate ❓ unique ✅ easy ✅ stigma ‼️
“antisocial” refers to criminal or harmful behaviour; not every person with ASPD acts that way
on the other hand, many people with ASPD tend to be misanthropic so maybe it’s not entirely inaccurate
easy to read
stigmatising, though more because of the stigma surrounding ASPD itself than the name
rating: 2.5/4
Alt: Dissocial / Dyssocial
accurate ❓ unique ✅ easy ❌ stigma ‼️
same as above, except “dyssocial” looses a point for being difficult to read
rating: 1/4
Alt: Psychopathy / Sociopathy
accurate ❌ unique ❌ easy ❓ stigma ‼️
psychopathy & sociopathy aren’t the same thing, and neither are the same as ASPD
huge amount of stigma attached to these
can be difficult to read/spell
rating: 0/4
Avoidant
accurate ✅ unique ✅ easy ✅ stigma ❌
it’s accurate, unique, easy and doesn’t have stigma attached (largely because AVPD isn’t well known)
rating: 4/4
Alt: Anxious-Avoidant & Phobic
accurate ❌ unique ✅ easy ❌ stigma ❌
inaccurate - many avoidants don’t have social anxiety / phobia
too long
no stigma (again because of it being unknown)
rating: 1/4
Borderline
accurate ✅ unique ❌ easy ✅ stigma ‼️
it is accurate but not many know what “borderline” actually means
the most known PD, carries a lot of stigma and sexism
easily confused with “borderline functioning” and similar terms in psychology
rating: 2/4
Alt: Emotionally Unstable
accurate ❓ unique ❌ easy ✅ stigma ‼️
not accurate as instability is not a feature of every borderline’s symptoms
not unique - also an alt. name for HPD
stigmatising
rating: 1/4
Dependent
accurate ✅ unique ✅ easy ✅ stigma ❓
accurate, unique, easy
possibly could be seen as stigmatising
rating: 3.5/4
Histrionic
accurate ❌ unique ✅ easy ❌ stigma ‼️
who actually knows what “histrionic” means?
apparently it comes from a word meaning an actor who is exaggeratedly false, which isn’t accurate for people with HPD
unique, but not easy to read
stigmatising, but again, no one knows what it means
rating: 1/4
Alt: Hysteric / Hysteric-Histrionic
accurate ❌ unique ✅ easy ❌ stigma ‼️
inaccurate - people with HPD aren’t “hysteric” (in the modern use of the word)
too long
“hysteria” is sexist & stigmatising
rating: 1/4
Alt: Emotionally Unstable
accurate ❌ unique ❌ easy ✅ stigma ‼️
inaccurate - emotional instability can be part of HPD, but not for all histrionics
not unique, already an alt. name for BPD
stigmatising
rating: 1/4
Narcissistic
accurate ✅ unique ✅ easy ❓ stigma ‼️
accurate, unique
might not be easy to spell
stigmatising, though more because of the stigma surrounding NPD itself than the name
rating: 2.5/4
Obsessive-Compulsive
accurate ❌ unique ❌ easy ✅ stigma ❓
inaccurate: people with OCPD don’t have obsessions or compulsions
not unique: too easily confused with OCD
easy to spell
potentially stigmatising
rating: 1/4
Alt: Compulsive
accurate ❌ unique ❓ easy ✅ stigma ❌
inaccurate for the same reasons OCPD is
technically unique but still not great for same reason OCPD isn’t (re: OCD)
rating: 1/4
Alt: Anankastic
accurate ❌ unique ✅ easy ❌ stigma ❌
unique, but no one knows what “anankastia” means
it means obsessive, so has the same problems as OCPD & compulsive
better than the others because it’s not easily confused with OCD
not easy to spell
not stigmatising, because it’s not known
rating: 1/4
Paranoid
accurate ✅ unique ❓ easy ✅ stigma ❓
accurate, easy to spell
possibly confusing with paranoid schizophrenia
potentially stigmatising
rating: 2/4
Schizoid
accurate ❓ unique ✅ easy ❌ stigma ❓
hard to tell if it’s accurate or not, because there’s no real definition of “schizoid” outside of SZPD
unique, but could be hard to spell
possibly stigmatising
rating: 1/4
Schizotypal
accurate ✅ unique ❌ easy ❌ stigma ❓
accurate, but easily confused with the concept of schizotypy
difficult to spell
potentially stigmatising
rating: 1/4
feel free to add on / criticise!
#congrats avpd you're the only name that gets full marks#dogpost#can i tag this as 'informational shitposting'?#personality disorders#no bold
19 notes
·
View notes
Text
Anankastia i anankaści. Czym jest osobowość anankastyczna?
„Może wszystko już wiesz
Może wszystko już masz
Jesteś pewny, że to szczęście
Nie masz czasu na sen
Nie masz czasu na seks
Wciąż od życia chcąc więcej
Zachłanna jest ta gwiazda
Dla której gubisz radość chwil
Liczy się wciąż niepewność
Którą przynoszą dni”
Bajm – „O Tobie”
[z płyty „Szklanka wody”, 2000 r.]
Anankastic Personality Disorder
[F60.5 w klasyfikacji ICD-10]
Temat, który poruszam w niniejszym artykule, jest niezwykle bliski mojemu sercu, ponieważ sama mam zdiagnozowane anankastyczno-unikające zaburzenie osobowości (OCPD + AvPD). O osobowości unikającej wspominałam już w moim poprzednim tekście zatytułowanym „Schizoidia i schizoidzi. Czym jest osobowość schizoidalna?”. Teraz wypadałoby wyjaśnić, o co chodzi z anankastią i anankastami. Na początek należy odnotować, że interesujące nas zaburzenie psychiczne posiada wiele nazw, które wprowadzają pewien zamęt pojęciowy. W międzynarodowej klasyfikacji chorób ICD-10 (stosowanej m.in. w Polsce od lat 90. XX wieku) używa się terminu „anankastic personality disorder” – „anankastyczne zaburzenie osobowości”. W podręczniku diagnostyczno-statystycznym DSM-5 (obowiązującym w Stanach Zjednoczonych Ameryki od 18 maja 2013 r.) występuje zaś określenie „obsessive-compulsive personality disorder” – „obsesyjno-kompulsywne zaburzenie osobowości”. Podręczniki DSM-I (1952) i DSM-III (1980) podsuwały zwięzłą nazwę „compulsive personality disorder” – „kompulsywne zaburzenie osobowości”. O tym, że warto promować wyraz „anankastyczny”, świadczy fakt, iż wielu Anglosasów myli „obsesyjno-kompulsywne zaburzenie osobowości” (OCPD) z „zaburzeniem obsesyjno-kompulsywnym” (OCD). Ten ostatni fenomen to po prostu nerwica natręctw, czyli odprawianie kuriozalnych rytuałów w celu odparcia nawracających myśli o niepokojącej treści. Osobowość anankastyczna NIE jest tożsama z owym uciążliwym schorzeniem psychicznym. To ekstremalna anankastia – rodzaj patologii ludzkiego charakteru.
Kryteria diagnostyczne ICD-10
[cyt. za: polskojęzyczna Wikipedia]
1. „nadmiar wątpliwości i ostrożności”
2. „pochłonięcie przez szczegóły, regulaminy, inwentaryzowanie, porządkowanie, organizowanie lub schematy postępowania”
3. „perfekcjonizm (przeszkadza w wypełnianiu zadań)”
4. „nadmierna sumienność z zaniedbaniem przyjemności i relacji interpersonalnych”
5. „przesadna pedanteria i przestrzeganie konwencji społecznych”
6. „sztywność i upór”
7. „irracjonalne sądzenie, że inni dokładnie podporządkują swe działania sposobom działania pacjenta lub nieracjonalna niechęć do przyzwalania innym na działanie”
8. „natarczywe, niechciane myśli i impulsy”
Człowiek z zasadami
Dr n. med. Sławomir Murawiec poświęcił osobom anankastycznym jeden ze swoich artykułów zamieszczonych na stronie internetowej „Medycyna Praktyczna” (MP.pl). W tekście tym możemy przeczytać, że anankasta już na pierwszy rzut oka sprawia wrażenie kogoś surowego i drobiazgowego. Jego twarz emanuje wiecznym skupieniem, a mowa ciała wskazuje na permanentną samokontrolę i brak spontaniczności. Osobnik dotknięty F60.5 zwykle stara się zachowywać w sposób niebudzący żadnych zastrzeżeń. Jest powściągliwy w okazywaniu emocji, uważny podczas wypełniania codziennych obowiązków oraz niesłychanie wrażliwy na to, jak inni ludzie oceniają jego działania tudzież osiągnięcia. Człowiek anankastyczny poważnie podchodzi do życia i wykonywanej pracy, chętnie snuje „plany awaryjne” na wypadek wszelkich nieszczęść. W swoim otoczeniu uchodzi za pedanta/perfekcjonistę z tendencją do pracoholizmu. Przywiązuje ogromną wagę do szczegółów – nie spocznie, dopóki nie poczuje, iż wszystko zostało dopięte na ostatni guzik. Anankasta to typowy fundamentalista moralny, który przestrzega swoich zasad bez względu na okoliczności zewnętrzne. I tutaj sielanka się kończy. Według dr. S. Murawca, jednostka z omawianym zaburzeniem psychicznym „stara się mieć wszystko pod kontrolą, zarówno w stosunku do samej siebie, jak i w zakresie (…) oczekiwań dotyczących postępowania innych osób. (…) Natomiast ci, którzy nie są równie sumienni i nie przejmują się tak normami postępowania, mogą wywołać u osoby anankastycznej dużą złość i chęć wpasowania ich postępowania w obowiązujące reguły”.
Prawie jak autyzm
Naomi Fineberg, MRCPsych – brytyjska lekarka ze specjalizacją z psychiatrii – opowiada o ludziach anankastycznych w swoim krótkim wywiadzie dla amerykańskiego psychiatry Erica Hollandera, MD (YouTube.com/user/SpectrumNeuroscience). Mówi tam, że skrajna anankastia może być cnotą, lecz i przywarą osoby cierpiącej na tę przypadłość. Wiele cech anankastycznych (choćby staranność i dokładność) jest mile widzianych w kulturze euroatlantyckiej oraz preferowanych przez ambitnych rekruterów. Niestety, istnieje też druga strona medalu: jednostki anankastyczne tak bardzo dbają o detale, że pracują w żółwim tempie i nierzadko mają problem z finalizacją misternego projektu. Co więcej, koncentrują się na wykonywanym zleceniu do tego stopnia, iż nie potrafią równolegle realizować innych zadań (brakuje im elastyczności koniecznej do efektywnego wypełniania licznych obowiązków). Kiedy zostają oddelegowane do zrobienia czegoś ważnego, oczekują, że wszystko pójdzie zgodnie z założeniem, a warunki umowy nie ulegną nawet najmniejszej korekcie. Jeśli jednak dochodzi do niespodziewanej zmiany planów, czują się totalnie zbite z tropu. Odczuwają wtedy lęk i złość, które można porównać tylko do frustracji osób z zespołem Aspergera – łagodnym zaburzeniem ze spektrum autyzmu. Anankaści nienawidzą wszystkiego, co niepełne i niedoskonałe, nie tolerują chaosu w żadnej formie. Gdy spotykają kogoś, kto w ich mniemaniu zachowuje się zbyt swobodnie, arbitralnie go dyskredytują. Są sztywni, niereformowalni, zatwardziali. Mają intruzywne myśli i multum rozterek wewnętrznych.
Ułomność czy supermoc?
Todd L. Grande, Ph.D (profesor nadzwyczajny Wilmington University w amerykańskim stanie Delaware, autor wyjątkowo merytorycznego wideobloga o zagadnieniach psychiatrycznych – YouTube.com/user/RioGrande51) opisuje skrajną anankastię jako jedyne zaburzenie osobowości, które z definicji przynosi choremu sporo korzyści. Jest to równocześnie strategia adaptacyjna, która na pozór wygląda zupełnie niegroźnie dla postronnego obserwatora. Osobowość anankastyczna wydaje się zjawiskiem społecznie akceptowalnym, ponieważ współczesna cywilizacja faworyzuje ludzi produktywnych i dobrze zorganizowanych. W wielu środowiskach ceni się takie atrybuty, jak dystans emocjonalny czy umiejętność panowania nad własnymi reakcjami. Pomagają one przecież w budowaniu wizerunku rzetelnego profesjonalisty. Jeżeli ktoś ma skłonność do pracoholizmu, to jest wymarzonym najemnikiem dla każdego wyzyskiwacza, gdyż dobrowolnie zrezygnuje z niejednego urlopu. A jeśli stawia obowiązki służbowe ponad relacjami interpersonalnymi, raczej nie przyniesie firmie wstydu w postaci jakiejś seksafery. Dodatkowe zalety anankastów: punktualność, puryzm językowy, szanowanie powagi sytuacji. Cóż może być złego w takim „pozytywnym” zaburzeniu psychicznym?! Otóż jednostki anankastyczne są niezbyt koleżeńskie, mają piekielne braki w dziedzinie komunikacji niewerbalnej oraz ciężko znoszą słowa krytyki. Empatia zdecydowanie nie jest ich mocną stroną. Osoby dotknięte F60.5 bywają bardzo nietolerancyjne względem ludzi epikurejskich i ekstrawertycznych. Nie aprobują żadnych zachowań impulsywnych.
Ofiarny fanatyk
Kati Morton, LMFT (psycholog kliniczna, terapeutka małżeńsko-rodzinna prowadząca swój gabinet w kalifornijskim mieście Santa Monica, a zarazem właścicielka poradnikowego kanału YouTube.com/user/KatiMorton) twierdzi, że jednostki anankastyczne odczuwają przymus robienia wszystkiego w „jedyny słuszny sposób”. Mają swoje ulubione metody postępowania, których trzymają się jak rzep psiego ogona i nie rezygnują z nich nawet wówczas, gdy inni ludzie postępują inaczej albo proponują sensowne alternatywy. Z punktu widzenia otoczenia anankaści są zamkniętymi umysłowo „betonami”, z którymi trudno się żyje, a jeszcze trudniej kooperuje. Czasem tak bardzo „fiksują się” na preferowanych zasadach działania, że zapominają, po co właściwie je stosują. Kiedy przygotowują jakieś dzieło, poprawiają je mnóstwo razy, ale nigdy nie są zadowoleni z efektu końcowego. Można powiedzieć, iż szukają dziury w całym. Anankasta to człowiek obowiązku – jeśli wierzy, że jest do czegoś zobligowany, na pewno to uczyni. W imię tego, co uznaje za swoją misję, wyrzeknie się każdej przyjemności, choćby zasłużonego odpoczynku i ciepłych relacji z najbliższymi osobami. Tutaj dochodzimy do kolejnej cechy jednostek anankastycznych, czyli do pryncypializmu w kwestiach etycznych bądź ideologicznych. Ortodoksja ta nie wypływa bezpośrednio z norm przyjętych w danej kulturze lub religii. Modelowy pacjent z F60.5 myśli samodzielnie. Jeżeli zostaje nieugiętym radykałem, to dlatego, że tak mu podpowiada własna intuicja. Opinia współwyznawców czy towarzyszy partyjnych nie ma tu znaczenia.
Dyktator i dusigrosz
Ramani Durvasula, Ph.D (psycholog kliniczna, wykładowczyni California State University w Los Angeles, niezastąpiona gwiazda wirtualnej telewizji „MedCircle” – YouTube.com/channel/UCyGOloOIJWt8NlE4tnejQeA) uważa, iż sednem anankastycznego zaburzenia osobowości jest pragnienie, aby uzyskać pełną kontrolę nad własnym życiem. A ponieważ życie składa się z wielu różnorodnych elementów, anankasta próbuje kontrolować wszelkie aspekty swojego istnienia – zarówno wewnętrzne (myśli, emocje, popędy), jak i zewnętrzne (porządek w mieszkaniu, zawartość lodówki, pory spożywania posiłków). Z tej przemożnej potrzeby stabilizacji wynika dążenie do „ustawienia” wszystkich i wszystkiego zgodnie z subiektywnym poczuciem doskonałości. To zaś często spotyka się z oporem innych ludzi, którzy prędzej czy później zaczynają postrzegać chorego jako apodyktycznego narcyza. Relacje osoby anankastycznej z resztą świata – współmałżonkiem, dorastającą latoroślą, przyjaciółmi, sąsiadami – bywają zatem napięte. Jednostki dotknięte F60.5 przejawiają specyficzny stosunek do dóbr materialnych. W ich mniemaniu pieniądze są po to, by je odkładać na czarną godzinę. Nieuchronną konsekwencją takiego rozumowania jest powielanie błędów Ebenezera Scrooge’a z „Opowieści wigilijnej” Charlesa Dickensa (1843). Bohater przywołanego utworu dysponował imponującymi oszczędnościami, lecz był zbyt skąpy, żeby z nich skorzystać albo oddać je biednym. Człowiek anankastyczny może uznawać każdy niekonieczny wydatek za zgubną rozrzutność. Dotyczy to nawet drobnych upominków dla kogoś umiłowanego.
OCPD vs OCD
Wróćmy na chwilę do podobieństw i różnic między osobowością anankastyczną (obsesyjno-kompulsywnym zaburzeniem osobowości, OCPD) a nerwicą natręctw (zaburzeniem obsesyjno-kompulsywnym, OCD). Wypada pochylić się nad tą kwestią, bo – jak zauważył dr T.L. Grande – około 25% „natręctwowców” wykazuje także symptomy F60.5. Tracey Marks, MD (afroamerykańska lekarka, specjalistka w dziedzinie psychiatrii, gospodyni edukacyjnego profilu YouTube.com/user/MarksPsych) tłumaczy, że perturbacje osobowościowe tkwią w samym rdzeniu ludzkiego „ja”. Są one czymś, z czym dana osoba zwyczajnie się identyfikuje. Wpływają bowiem na to, kim ktoś jest, za kogo się uważa, jaką ścieżką podąża oraz w jaki sposób buduje więzi ze światem zewnętrznym. Patologie osobowości stanowią cząstkę „natury” konkretnego człowieka. Natomiast zaburzenia lękowe – chociażby nerwica natręctw – są powierzchowne i dają się pacjentowi odczuć jako coś obcego, kłopotliwego, niepożądanego. Gdy dopadają swoją ofiarę, dręczą ją bez litości. Jednostka anankastyczna i osobnik z natręctwami mogą zachowywać się podobnie, ale za tymi działaniami stoją całkiem inne motywy. Jeśli anankasta długo się myje i sprawdza wszystko kilkanaście razy, to dlatego, iż po prostu preferuje taką nadgorliwość. Tymczasem „natręctwowiec” czyni tak z powodu horrendalnego lęku i niepohamowanego przymusu wewnętrznego. Znerwicowana osoba męczy się ze swoimi obsesjami i kompulsjami, jednak nie potrafi ich w pełni kontrolować. Nie lubi tego, co sama robi. Wie, że postępuje absurdalnie, lecz jakoś nie może się powstrzymać.
Brenda aka Terminator
Dr Todd L. Grande opisywał kiedyś casus anankastycznej księgowej z nerwicą natręctw (OCPD + OCD), której współpracownicy nadali przezwisko „Terminator” ze względu na nieokazywanie uczuć, niebranie urlopów, ślepe przestrzeganie dyscypliny tudzież efektywność w ustalaniu nieprawidłowości finansowych. Była to wykształcona dama po pięćdziesiątce, stara panna, która od dziecka kochała weryfikować, czy „kasa się zgadza” i czy dobra ruchome są bezpieczne. Dyrekcja chwaliła ją za solidność i skrupulatność, a szeregowi pracownicy – postrzegali jako wyrachowane i antypatyczne indywiduum. Brenda (bo takim imieniem „ochrzcił” ją dr Grande) nie znosiła rzeczy w jakimkolwiek stopniu uszkodzonych. Pewnego dnia jej samochód został naruszony wskutek parkingowej stłuczki. Cóż kobieta wówczas uczyniła? W ciągu tygodnia wymieniła auto na zupełnie nowe: kupiła ten sam model w tym samym kolorze! Gdy terapeutka Brendy poznała ów motoryzacyjny sekret, zapewne nie posiadała się ze zdumienia… Pełną historię „Terminatora” można usłyszeć w filmiku „Obsessive-Compulsive Disorder & OCPD Presentation Analysis” (YouTube). Ciekawostka: bezceremonialne wyrzucanie podniszczonych przedmiotów NIE jest objawem charakterystycznym dla skrajnej anankastii. Osoby z tym syndromem zdradzają raczej tendencję do szaleńczego zbieractwa – syllogomanii. Wstrzymują się z usuwaniem nawet zawadzających rupieci, ponieważ „wszystko może się jeszcze przydać”. Takie chomikowanie doskonale koresponduje z typowo anankastycznym skąpstwem, drastycznym ograniczaniem wydatków na siebie i bliźnich.
Cluster „C” (DSM-5)
Ehsan Gharadjedaghi, Psy.D (psycholog kliniczny osiadły w kalifornijskim hrabstwie Orange, pomysłodawca branżowego projektu „TherapyCable” – YouTube.com/user/TherapyCable) omawia F60.5 w kontekście tzw. klastra „C” wyodrębnionego w amerykańskim podręczniku diagnostyczno-statystycznym DSM-5. Chodzi tutaj o trzy zaburzenia osobowości, które zostały uznane przez tamtejszych psychiatrów za „lękliwe” i „strachliwe”. Są to: osobowość unikająca („avoidant” – AvPD), osobowość zależna („dependent” – DPD) i osobowość anankastyczna („obsessive-compulsive” – OCPD). Nieszczęśnicy dotknięci przypadłościami z wiązki „C” egzystują w chronicznej trwodze. Jednostki unikające boją się upokorzenia i odrzucenia, toteż wolą tkwić w permanentnej izolacji społecznej niż wyjść do ludzi i doświadczyć spodziewanej krytyki. Z obawy przed wyśmianiem/potępieniem usiłują nie zwracać na siebie uwagi, ale w głębi serca tęsknią za zwykłymi interakcjami społecznymi. Jednostki zależne odczuwają strach przed samodzielnością i podejmowaniem ryzyka. Uwielbiają być wyręczane w dokonywaniu codziennych wyborów, dzięki czemu mogą uniknąć ponoszenia odpowiedzialności za swoje decyzje. Robią z siebie niezaradne dzieci, którym stale trzeba „matkować” lub „ojcować”. Jednostki anankastyczne lękają się utraty panowania nad własnym losem. Przeraża je przyszłość – ta wielka niewiadoma, która może przynieść dużo frasunku. W miarę możliwości próbują więc być przewidujące: przygotowują się psychicznie i materialnie na przyszłe kryzysy oraz niedostatki. Wykazują iście surwiwalową mentalność.
Oszukać przeznaczenie
Zajrzyjmy teraz do artykułu „Osobowość anankastyczna” opatrzonego stopką redakcyjną „opr. aw/aw”. Tekst ten, opublikowany w rzymskokatolickim serwisie Opoka.org.pl, bazuje na książce „Oblicza lęku. Studium z psychologii lęku” niemieckiego psychologa i psychoanalityka Fritza Riemanna (wydanie oryginalne – Monachium 1961, wydanie polskie – Warszawa 2005). Z lektury owego artykułu wynika, że człowiek anankastyczny szczególnie boi się przemijania, czyli upływu czasu niosącego za sobą nieuchronne zmiany we wszystkich sferach ludzkiego istnienia. Świadomość faktu, iż w życiu nie ma nic stałego, doprowadza anankastę do frustracji i rozpaczliwych prób zatrzymania rzeczy znanych. Dochowywanie wierności starym zwyczajom jest wyrazem buntu przeciwko efemeryczności ziemskich spraw – budowaniem domu na skale, który ma trwać pomimo niszczycielskiego działania sił przyrody. Upieranie się przy tym, co sprawdzone i umiłowane, daje wszak namiastkę ponadczasowości. Niestety, takie postępowanie wiąże się również z licznymi skutkami ubocznymi, a zwłaszcza z zaprzepaszczeniem wielu szans na korzystne przeobrażenia. Jeśli wyrobiliśmy w sobie nawyk odrzucania nawet rozsądnych sugestii, to sami podcinamy sobie skrzydła. Mroczne są ponadto konsekwencje ciągłego niezdecydowania. Bywa, że anankasta tak długo zwleka z podjęciem jakiejś decyzji, iż rozważana przezeń opcja przestaje być aktualna. Zdaniem Fritza Riemanna, za anankastyczną niechęcią do zmian kryje się… wyolbrzymiony strach przed śmiercią. Walka z przemijaniem to nieświadome dążenie do nieśmiertelności.
Gombrowiczowska symetria
Jeszcze inny obraz F60.5 wyłania się z naukowego opracowania „Niedojrzałość emocjonalna i moralna a zaburzenia osobowości” pochodzącego z periodyku „Studia Psychologica”, nr 5/2004 (cyfrową wersję tej publikacji udostępniono w elektronicznym archiwum Bazhum.muzhp.pl). Twórca artykułu – dr Włodzimierz Strus z Uniwersytetu Kardynała Stefana Wyszyńskiego w Warszawie – przedstawia osobowość anankastyczną jako absolutne przeciwieństwo osobowości dyssocjalnej (F60.2). Według badacza, skrajna anankastia i socjopatia/psychopatia są względem siebie symetryczne niczym dwie strony tego samego medalu. Zarówno jednostki anankastyczne, jak i dyssocjalne mają ogromny problem z własnym superego. Sęk w tym, że u tych pierwszych jest ono zbyt rozbudowane, a u tych drugich – prowizoryczne. O ile anankasta ujawnia „skrupulanckie” sumienie i nadwrażliwość moralną, o tyle socjopata/psychopata wydaje się pozbawiony hamulców i nieczuły wobec zastanych norm społecznych. Człowiek cierpiący na F60.5 nadmiernie się kontroluje, żyje w nieustannej obawie przed konsekwencjami swoich poczynań. Delikwent z F60.2 działa pod wpływem impulsu, nie bierze na siebie żadnej odpowiedzialności i nie odczuwa strachu przed karą za swoje przewinienia. Jednostka anankastyczna wstydzi się własnej seksualności, próbuje ją trzymać na wodzy. Jednostka dyssocjalna nie zna takich dylematów – jest po prostu hedonistyczna. Anankaści i socjopaci/psychopaci różnią się niczym Filidor i Anty-Filidor z „Ferdydurke” Witolda Gombrowicza (1937). Ale obie grupy ludności są niedojrzałe emocjonalnie.
3 x M
Kiedy myślę o anankastycznym zaburzeniu osobowości, natychmiast przychodzi mi do głowy Maryla Cuthbert – adopcyjna matka Ani z Zielonego Wzgórza. Bohaterka ta została wykreowana przez Lucy Maud Montgomery w 1908 r. „Maryla była to wysoka i szczupła kobieta o ostrych konturach członków. Jej ciemne włosy o niewielu siwych pasmach zwinięte były stale w gruby węzeł, w morderczy sposób przeszyty dwiema metalowemi szpilkami. Czyniła wrażenie osoby o ciasnym poglądzie na świat i bardzo wymagającej. Jednakże nieznaczny jakiś rys wokoło ust, leciutko tylko naznaczony, wskazywał, że gdyby był cokolwiek bardziej rozwinięty, zdradzałby niewątpliwie skłonność do wesołej ironji” – czytamy w pierwszym rozdziale powieści (tłum. Rozalia Bernsztajnowa, Warszawa 1921, pisownia oryginalna, cyt. za: Pl.wikisource.org). Osobą dotkniętą F60.5 była też zapewne Mildred Ratched, despotyczna pielęgniarka oddziałowa z książki „Lot nad kukułczym gniazdem” Kena Keseya (1962) i oscarowego filmu Milosa Formana pod tym samym tytułem (1975). Fabuła „Lotu…” ukazuje historię konfliktu między tą pedantyczną pracownicą szpitala psychiatrycznego a zbuntowanym, socjopatycznym pacjentem o nazwisku Randle Patrick McMurphy. Cech anankastycznych można by się także doszukiwać u prof. Minerwy McGonagall, opiekunki Gryffindoru w szkole magii Hogwart. Wspomniana postać występuje w powieściach o Harrym Potterze autorstwa Joanne Kathleen Rowling (1997-2007) i w kinowych adaptacjach tego cyklu prozatorskiego (2001-2011). McGonagall to bardzo mądra czarownica, lecz surowa i restrykcyjna.
Żelazna dziewica
Urodziłam się 19 lutego 1991 r. na Kielecczyźnie. Jako nastolatka byłam „czarną owcą” w moim środowisku rówieśniczym. Nie tylko dlatego, że chętnie ubierałam się na czarno, ale przede wszystkim dlatego, iż zachowywałam się inaczej niż większość moich znajomych. Zawsze pilnie się uczyłam, odrabiałam lekcje i respektowałam grono pedagogiczne. Co gorsza, nie chodziłam na imprezy, nie podrywałam chłopaków i nie oglądałam materiałów XXX. Te wszystkie „zbrodnie” wystarczały, żeby być „na cenzurowanym” od końca podstawówki aż do egzaminu maturalnego. Na studiach wypruwałam sobie żyły, aby zaliczyć komplet przedmiotów z najwyższym możliwym dla mnie wynikiem. Dzięki swojej determinacji trzykrotnie pobierałam stypendium rektora za wysoką średnią ocen: dwa razy na Uniwersytecie Jana Kochanowskiego w Kielcach (500 zł miesięcznie) i raz na Uniwersytecie Warszawskim (550 zł miesięcznie). Co zrobiłam z zarobionymi pieniędzmi? Nie, nie roztrwoniłam ich na luksusy/hulanki. Umieściłam je na lokacie bankowej, żeby się powoli mnożyły i zabezpieczały finansowo moją przyszłość. Nigdy nie umówiłam się z nikim na randkę ani nie poszłam z nikim do łóżka. Nie uznaję seksu przedmałżeńskiego i nie popełniłabym takiego czynu nawet dla „niewinnego” eksperymentu. Hołduję tradycyjnej zasadzie „jak kocha, to poczeka” (min. 3 lata). Nie chcę mieć nieślubnych dzieci, więc nie dopuszczam się głupstw, których skutkiem mogłaby być ciąża i oddanie noworodka do okna życia. Jestem dumna, zimna, przezorna i zapobiegliwa. Irracjonalne „błędy młodości” omijają mnie szerokim łukiem.
Natalia Julia Nowak,
grudzień-styczeń 2019/2020
PS 1. Z tymi „Terminatorami” to faktycznie jest coś na rzeczy. Osobowość anankastyczna została u mnie zdiagnozowana w 2009 r., osobowość unikająca – w 2019 r. Kiedyś na studiach licencjackich (2010-2013) życzliwa koleżanka wyjawiła mi, że studentka X w prywatnych konwersacjach nazywa mnie robotem. Później sama usłyszałam to określenie („robot”) na własne uszy. Hmmm…
PS 2. Funkcjonuje ciekawy wideoblog poświęcony w 100% osobowości anankastycznej, czyli północnoamerykańskiemu „obsesyjno-kompulsywnemu zaburzeniu osobowości”. Projekt nosi tytuł „OCPD: My Life in Debris”, co w tłumaczeniu na polszczyznę oznacza „OCPD: Moje Życie w Gruzach” (YouTube.com/ocpdmylifeindebris). Założycielem tego vloga jest niejaki Darryl – prawdziwy anankasta ze Stanów Zjednoczonych. O swoim OCPD wielokrotnie opowiadała też znerwicowana, kanadyjska wideoblogerka Emma, właścicielka amatorskiego kanału „EmmAnxiety” (YouTube.com/channel/UCWwm_9iH0k3inBrknkE9oag). Inna anankastka zamieszczająca swoje audiowizualne miniprodukcje na YT: „Let’s Talk Mental Health” – „Porozmawiajmy o Zdrowiu Psychicznym” (YouTube.com/channel/UC9LuPdpWmojRJqSzKPgm0ag).
PS 3. W akapicie „Gombrowiczowska symetria” pisałam o rozbieżnościach między osobowością anankastyczną a osobowością dyssocjalną. Nie zaszkodzi odnotować, że ta ostatnia jest znana w USA jako „antyspołeczne zaburzenie osobowości” (ASPD – „antisocial personality disorder”). Twórcy podręcznika DSM-5 przyporządkowali dyssocjalność/antyspołeczność do klastra „B”. Obejmuje on cztery zaburzenia osobowości, które na pierwszy rzut oka sprawiają wrażenie „dramatycznych”, „emocjonalnych” i/lub „niekonsekwentnych” (oto ich lista: ASPD – osobowość antyspołeczna, NPD – osobowość narcystyczna, HPD – osobowość histrioniczna, BPD – osobowość pograniczna/borderline). Ludzie dyssocjalni bywają nieoficjalnie dzieleni na socjopatów i psychopatów. W serwisie YouTube znajdziemy wiele krótkich filmików demaskujących podobieństwa i różnice między socjopatami a psychopatami, np. „What is the Difference Between Sociopathy and Psychopathy?” (YouTube.com/user/RioGrande51), „Sociopath vs Psychopath: What’s the Difference?” (YouTube.com/user/Psych2GoTv), „Sociopath vs Psychopath – What’s The Difference?” (YouTube.com/user/TheInfographicsShow), „Difference between a psychopath and a sociopath” (YouTube.com/user/businessinsider).
PS 4. Jeśli wierzyć anglojęzycznej Wikipedii powołującej się na badania Belindy Board i Katariny Fritzon z University of Surrey (południowo-wschodnia Anglia), istnieją trzy perturbacje osobowościowe, które częściej spotyka się u Brytyjczyków na stanowiskach kierowniczych niż u pacjentów Broadmoor Hospital – pilnie strzeżonego zakładu dla niepoczytalnych przestępców. Tymi trzema „elitarnymi” patologiami są: osobowość narcystyczna, osobowość histrioniczna i osobowość anankastyczna. Chyba nikogo to nie dziwi!
PS 5. Nurtuje mnie następujące pytanie… Czy Władysław Gomułka, pierwszy sekretarz Komitetu Centralnego PZPR w latach 1956-1970, nie był jednym z sukcesywnych anankastów? Do takich refleksji skłania mnie seans fabularyzowanego dokumentu „Towarzysz Wiesław. Od agitatora do dyktatora” (reż. Piotr Boruszkowski, TVP 2014). Co się tyczy spisu fikcyjnych postaci z F60.5, należałoby do niego dodać Artura, protagonistę sztuki teatralnej „Tango” Sławomira Mrożka (1964). Zauważmy, że antagonistą tego autorytarnego młodzieńca jest lokalny degenerat Edek – socjopata, osobnik dyssocjalny/antyspołeczny.
1 note
·
View note
Text
this interaction has solidified my stance against assimilation-thru-academia. possibly the final pt tipping me over. but not sure how to explain verbally/in normie-friendly terms. how to explain to a white dude that ability is not the problem. not accuracy or precision. not even innovation/insight. but the subject matter thereof. not “insecurity.” not insecurity or self-deprecation when i say i am disabled or weird or not normal but factual descriptors. trying to explain something that wasn’t grasped. failing. not anti-intellectualism or self-deprecation or undervaluation of own skills when i say i will never get Published-published. not the idea of an academy itself or intellect or rigorous examination or contact w/academics but The academy, this Academy in this particular location and in this particular time period under this particular system. radical theory cannot be truly “academic.” have already said too much. cant dismantle the system w/the system’s power, cant explain my problems w/the system to the system’s agents. why do i ever bother. just dont invest. then no losses. why the need.
4 notes
·
View notes
Text
Personality Disorder in the ICD-11
I tried to put the ICD-11 diagnostic guidelines of PD in a checklist instead of a text
Note: in the ICD-11, the concept of multiple distinctly defined PDs has been abolished. There is one personality disorder that is diagnosed with a specifier of severity. A specifier noting what traits are associated with the PD can also be used
Personality Disorder
A. Problems in one or both of the following areas:
Functioning of aspects of the self
Interpersonal functioning
B. The disturbance has persisted for at least two years
C. The disturbance is manifest in patterns of cognition, emotional experience, emotional expression, and behaviour that are maladaptive (e.g., inflexible or poorly regulated)
D. The disturbance is present across a range of personal and social situations
E. The patterns of behaviour characterizing the disturbance cannot be explained by normal development or by social or cultural factors, including socio-political conflict
F. The disturbance is associated with substantial distress or significant impairment in personal, family, social, educational, occupational or other important areas of functioning
Personality Functioning:
1. Areas of functioning of aspects of the self include:
identity
self-worth
accuracy of self-view
self-direction
2. Areas of interpersonal functioning include:
ability to develop and maintain close and mutually satisfying relationships
ability to understand others’ perspectives and to manage conflict in relationships
Severity
Mild:
Disturbances affect some areas of personality functioning but not others and may not be apparent in some contexts
There are problems in many interpersonal relationships and/or in performance of expected occupational and social roles, but some relationships are maintained and/or some roles carried out
Not likely to be associated with substantial harm to self or others
Distress and functional impairment are either limited to circumscribed areas or present in more areas but milder
Moderate:
Disturbances affect multiple areas of personality functioning though some areas may be less affected than others
There are marked problems in most interpersonal relationships and the performance of most expected social and occupational roles are compromised to some degree. Relationships are likely to be characterized by conflict, avoidance, withdrawal, or extreme dependency
May or may not be associated with harm to self or others
Marked functional impairment in many areas of life
Severe:
Most, if not all areas of personality functioning are affected. There is severe impairment in both interpersonal functioning and functioning of aspects of the self
Problems in interpersonal functioning seriously affect virtually all relationships and the ability and willingness to perform expected social and occupational roles is absent or severely compromised
Likely to be associated with harm to self or others
Functional impairment is severe and present in all or nearly all areas of life
Traits
None of these traits are inherently maladaptive. They're only a disorder if they're diagnosed as a specifier to personality disorder. Most can also be part of a diagnosis of a personality difficulty.
Negative Affectivity:
The disturbance is characterized by a tendency to experience a broad range of negative emotions
Common manifestations include:
experiencing a broad range of negative emotions with a frequency and intensity out of proportion to the situation
emotional lability and poor emotion regulation
negativistic attitudes
low self-esteem and self-confidence
mistrustfulness
(Compare: Dependent PD, Avoidant PD)
Detachment:
The disturbance is characterized by a tendency to maintain interpersonal and emotional distance
Common manifestations include:
avoidance of social interactions
lack of friendships
avoidance of intimacy
reserve
aloofness
limited emotional expression and experience
(Compare: Schizoid PD)
Dissociality:
Disturbance is characterized by a disregard for the rights and feelings of others, encompassing both self-centeredness and lack of empathy
Common manifestations of include:
sense of entitlement
expectation of others’ admiration
positive or negative attention-seeking behaviours
concern with one's own needs, desires and comfort and not those of others
indifference to whether one’s actions inconvenience hurt others
being deceptive, manipulative, and exploitative of others, being mean and physically aggressive
callousness in response to others' suffering
ruthlessness in obtaining one’s goals
(Compare: Antisocial PD, Narcissistic PD)
Dininhibition:
Disturbance is characterized by a tendency to act rashly based on immediate external or internal stimuli, without consideration of potential negative consequences
Common manifestations include:
impulsivity, distractibility, irresponsibility, recklessness, lack of planning
Anankastia:
The disturbance is characterized by a narrow focus on one’s rigid standard of perfection and of right and wrong, and by controlling one’s own and others’ behaviour and controlling situations to ensure conformity to these standards
Common manifestations include:
concern with social rules, obligations, and norms of right and wrong, scrupulous attention to detail, rigid, systematic, day-to-day routines, hyper-scheduling and planfulness, emphasis on organization, orderliness, and neatness, rigid control over emotional expression, stubbornness and inflexibility, risk-avoidance, perseveration, and deliberativeness
(Compare: Obsessive-Compulsive PD)
Borderline Pattern:
Personality Disorder is characterized by a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, as indicated by many of the following:
frantic efforts to avoid real or imagined abandonment, a pattern of unstable and intense interpersonal relationships, identity disturbance, manifested in markedly and persistently unstable self-image or sense of self, a tendency to act rashly in states of high negative affect, leading to potentially self-damaging behaviours, recurrent episodes of self-harm, emotional instability due to marked reactivity of mood, chronic feelings of emptiness, Inappropriate intense anger or difficulty controlling anger, transient dissociative symptoms or psychotic-like features in situations of high affective arousal
(Compare: Borderline PD)
(Tumblr didn't allow me more paragraphs so I had to improvise with colors; purple seemed like the easiest to read)
51 notes
·
View notes
Photo

Why You Need to Understand the Latest Personality Trait: Anankastia
0 notes
Text
ICD-11 model for personality disorders
In the new edition of the ICD, personality disorders have been collapsed into one singular disorder, specified further by trait domains. A person would be diagnosed only with ‘Dissociality in personality disorder or personality difficulty’ instead of ‘Dissocial Personality Disorder’. (Personality difficulty is a sub-threshold level of personality disorder traits).
The five traits are:
Negative Affectivity
Detachment (vaguely equivalent to DSM 5′s Schizoid PD)
Dissociality (equivalent to Antisocial PD)
Disinhibition
Anankastia (equivalent to Obsessive-Compulsive PD)
‘Borderline pattern’ is an optional specifier and ideally should be used in conjunction with other traits. (Equivalent to and essentially the same criteria as Borderline PD).
Negative affectivity
The core feature of the Negative Affectivity trait domain is the tendency to experience a broad range of negative emotions. Common manifestations of Negative Affectivity, not all of which may be present in a given individual at a given time, include: experiencing a broad range of negative emotions with a frequency and intensity out of proportion to the situation; emotional lability and poor emotion regulation; negativistic attitudes; low self-esteem and self-confidence; and mistrustfulness.
Detachment
The core feature of the Detachment trait domain is the tendency to maintain interpersonal distance (social detachment) and emotional distance (emotional detachment). Common manifestations of Detachment, not all of which may be present in a given individual at a given time, include: social detachment (avoidance of social interactions, lack of friendships, and avoidance of intimacy); and emotional detachment (reserve, aloofness, and limited emotional expression and experience).
Dissociality
The core feature of the Dissociality trait domain is disregard for the rights and feelings of others, encompassing both self-centeredness and lack of empathy. Common manifestations of Dissociality, not all of which may be present in a given individual at a given time, include: self-centeredness (e.g., sense of entitlement, expectation of others’ admiration, positive or negative attention-seeking behaviours, concern with one's own needs, desires and comfort and not those of others); and lack of empathy (i.e., indifference to whether one’s actions inconvenience or hurt others, which may include being deceptive, manipulative, and exploitative of others, being mean and physically aggressive, callousness in response to others' suffering, and ruthlessness in obtaining one’s goals).
Disinhibition
The core feature of the Disinhibition trait domain is the tendency to act rashly based on immediate external or internal stimuli (i.e., sensations, emotions, thoughts), without consideration of potential negative consequences. Common manifestations of Disinhibition, not all of which may be present in a given individual at a given time, include: impulsivity; distractibility; irresponsibility; recklessness; and lack of planning.
Anankastia
The core feature of the Anankastia trait domain is a narrow focus on one’s rigid standard of perfection and of right and wrong, and on controlling one’s own and others’ behaviour and controlling situations to ensure conformity to these standards. Common manifestations of Anankastia, not all of which may be present in a given individual at a given time, include: perfectionism (e.g., concern with social rules, obligations, and norms of right and wrong, scrupulous attention to detail, rigid, systematic, day-to-day routines, hyper-scheduling and planfulness, emphasis on organisation, orderliness, and neatness); and emotional and behavioural constraint (e.g., rigid control over emotional expression, stubbornness and inflexibility, risk-avoidance, perseveration, and deliberativeness).
Borderline pattern
The Borderline pattern specifier may be applied to individuals whose pattern of personality disturbance is characterised by a pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity, as indicated by many of the following: Frantic efforts to avoid real or imagined abandonment; A pattern of unstable and intense interpersonal relationships; Identity disturbance, manifested in markedly and persistently unstable self-image or sense of self; A tendency to act rashly in states of high negative affect, leading to potentially self-damaging behaviours; Recurrent episodes of self-harm; Emotional instability due to marked reactivity of mood; Chronic feelings of emptiness; Inappropriate intense anger or difficulty controlling anger; Transient dissociative symptoms or psychotic-like features in situations of high affective arousal.
#icd#icd-11#personality disorders#negative affectivity#detachment#dissociality#disinhibition#anankastia#borderline pattern#not a fan of this model; i like the dsm's alt model the best#dogpost#pd info#introduction to
25 notes
·
View notes
Last Seen Blogs
jilldraws90
JillDraws

crunchcrunchteacakes
For The Mission

groovybry
blindDude

los-santos-project-d
Red Suns in Los Santos

thekidd4929
Untitled