#mtds drawing
Text

It's almost as if he's still here 💔
#my hero academia#mha#bnha#all for one#boku no hero academia#afo#mtds drawing#mha afo#bnha afo#bnha all for one#digital art#digital drawing#mha manga#bnha manga#ofa vestiges#ofa#one for all
92 notes
·
View notes
Text

kwites bloonsona.
#inside joke#twitch#twink#bloons#mtd#kwite fanart#kwite#kwite my beloved#digital art#drawing#doodle#kwote#my art#fanart#character art#artwork#art#artists on tumblr#artist on tumblr#artstyle#aethestic#aethstetic#gay boi#gay culture#gay#gayboy#gay art#curvy and cute#cute art#bloons tower defense
12 notes
·
View notes
Text
man what if i just posted all my tf2 art here huh
i keep forgetting,,
#gryph.txt#joining the mtd redraw joining a new server otto's art the mtd being almost done#girl help i'm in the trenches (the trenches being my hyperfixation on tf2 coming back)#i also#have been thinking about trying to draw up my designs for the red/blu mercs nd stuff#because i've been thinking about them again#blu scout and red sniper are done i sketched them out on paper and then turned them digital i just#haven't done any of these guys in full really#verrrrry tempted to just ask for tf2 requests 'cause. they're so silly so fun to me#but i'm. somewhat busy#i dunno if anyone seeing this feel free to :]
3 notes
·
View notes
Note
Can Armand fly? Like does he have the ~Cloud Gift~ so to speak, or does he not? I can’t remember..
And he doesn’t seem to have/use the Fire Gift too right, or am I wrong?
Armand’s powers are so interesting to me, the way he can make life like illusions like no other (at least I can’t remember an Anne Rice vampire making that kind of illusions, maybe I’m wrong) is somehow so ‘compliant’ with his character.
I remember when Daniel is about to be turned, Armand creates this illusion for him and Daniel’s description is so haunting for some reason, like he can actually smell the flowers, he can see the stars, he can pick a leaf from a tree and he even sees Armand’s damp footprints on the ground(!) Imagine being able to conjure up an illusion like that.. jeez
And he seems to have been able to do it when he was a younger vampire too, right?
Like didn’t he draw mortals who were ready to die from their homes with some kind of illusion, so he could feed on them? (That is also so compliant with his character for some reason now I think about it)
God, he really is SUCH a good character I can’t get over him. I need to have his name tattooed on my body (like Armand definitely tried to convince Daniel to do. ‘Daniel, can’t you get this tattoo of my name on your arm? I want to see how it is done :3’)
Armand does have the Cloud Gift!
The very first mention of Armand being able to fly is in MtD, where Lestat seems rather surprised to realize that he can:
The steel buttons of his [Armand's] denim jacket were icy cold, as though he had come from some far worse winter in a very few moments of time. We are never entirely sure about each other's powers. It's all a game. I would no more have asked him how he got here, or in what manner, than I would ask a mortal man how precisely he made love to his wife. ~ Lestat, MtD
Unrelated but I'm always so thirsty for any insights as to how vampires view their relationships to each other within vampiric norms, and I think it's fascinating that even two vampires who've known each other for so long and have such a complex, intertwined history as Armand and Lestat do don't really know how powerful the other is and it would be taboo to ask. Scandalous!
Thank you to @thecactifindahome for reminding me that Armand actually has known how to fly for quite a while!
By my own will, and with the first explosion of my blood in the light of the morning sun, I had been driven upwards, as high perhaps as I could go. For centuries I'd known how to climb to airy heights and how to move there, but I'd never pushed it to a conceivable limit, but with my zeal for death, I had strained with all my available strength to move Heavenward. My fall had been from the greatest height. ~ Armand, TVA
Armand also has the Fire Gift, which is first noted in PL:
“You go to New York, my friend, and Armand will burn you to cinders,” said Killer. “Oh, not Benji or Sybelle, no, and maybe not even Louis ... but Armand will do it and they won’t bat an eye. And they can do it too. They have Marius’s blood in their veins, those two. Even Louis’s powerful now, got the blood of the older ones in him. But Armand is the one who kills. There are eight million people in Manhattan and four members of the Undead. I warn you, Antoine, they won’t listen to you. They won’t care that Lestat made you. Least I don’t think they will. Hell, you won’t even have a chance to tell them. Armand will hear you coming. Then he’ll kill you on sight. You do know they have to see you to burn you up, don’t you? They can’t do it unless they can see you. But Armand will hunt you down and you won’t be able to hide.” ~ Killer to Antoine, PL
Armand has always been incredibly powerful — even a newborn vampire — which I think is due to a few different factors:
Marius ensured that Armand received plenty of his blood during his turning
Prior to making Armand, Marius hadn't created another vampire since Pandora, some 1,500 years ago so the power in his blood was very potent
Marius's blood was so powerful to begin because of the regular infusions he received from Akasha, so the vampires in his line do tend to be powerful and gifted
This accounts for Armand's early strength and Mind Gift abilities (spellbinding and illusions).
Seeing as the Cloud Gift didn't come until after QotD, I headcanon Armand received a blood power-up from Marius (or perhaps another of the old ones, similar to how Maharet offered Louis her blood). Vampire powers evolve with time/age, surviving a burning, taking the blood of a much more powerful vampire.
Age gave him the Cloud Gift, and following his suicide attempt, Armand did drink from Lestat — so the combination of the burning and Lestat's blood likely contributed to him developing the Fire Gift soon afterwards.
Armand is also telekinetic:
I have most-powerful abilities to cast spells, to dislocate my vision, and to transmit my image over distances, and to affect matter both at close range and matter which is out of sight. ~ Armand, TVA
And last but not least, he may have the power to astral project although I don't believe it's explicitly spelled out but even as a mortal, he has an out of body experience witnessing himself dying, and later on when he's recounting his suicide attempt in TVA, he says this:
That is, having fallen on the roof, burnt and in unspeakable torment, I might have sought a desperate mental escape, projecting my image and my strength into Sybelle's apartment long enough to kill her brother. It certainly is possible for spirits to exert enough pressure on matter to change it. So perhaps that is exactly what I did-project myself in spirit form and lay hands upon the substance that was Fox, and kill him.
However, he doesn't actually believe that that's what happened in this particular instance, but it's the possibility that he is, in fact, powerful enough to do so. Armand was already so unique and "different" as a mortal child and adolescent (I would call this neurodivergent but that wasn't a term in the 15th century or anytime shortly after), that it makes sense his powers would be easily amplified and exceptional in their own right.
Re: his hunting style, it's described by Lestat when they first meet as:
He [Armand] had learned to summon those who truly wished to die. He had but to stand near the dwellings of mortals and call silently to see his victim appear. Old, young, wretched, diseased, the ugly or the beautiful, it did not matter because he did not choose. Dazzling visions he gave, if they should want to receive, but he did not move towards them nor even close his arms around them. Drawn inexorably towards him, it was they who embraced him. And when their warm living flesh touched him, when he opened his lips and felt the blood spill, he knew the only surcease from misery that he could know. It seemed to him in the best of these moments that his way was profoundly spiritual, uncontaminated by the appetites and confusions that made up the world, despite the carnal rapture of the kill. In that act the spiritual and the carnal came together, and it was the spiritual, he was convinced, that survived. Holy Communion it seemed to him, the Blood of the Children of Christ serving only to bring the essence of life itself into his understanding for the split second in which death occurred. ~ Lestat, TVL
Definitely within character, I agree :') for a character that to me reads as having been passively suicidal for most of his life, there is a bittersweet irony and perhaps even a misguided sense of mercy behind it.
AND YES YOU SHOULD ABSOLUTELY GET AN ARMAND TATTOO I WANT ONE SO BAD!!! character of all time, love of my life, etc etc you guys already know!!!!!
#you ask and hekate answers#i lost count of how many times i said the word 'powerful' in this post don't judge me it's tuesday morning#also where's my headcanon post of armand tattooing an A on daniel's lower half#armand#the vampire chronicles#quotes#vc
49 notes
·
View notes
Text
We were talking today about how Daniel and Armand seperated and how it took it's toll on them. Which inevitably led to talking about Armand's 'death' in MtD and...well, this is just pure angst.
It was also done in about ninety minutes flat so it's bound to be messy. I'll clean it up later.
Burnt Out
There’s a set of lights in the window across the way.
The pattern changes every few minutes, it’s on some kind of timer and Daniel thinks he can anticipate what’s coming. A three second blink, then change, then two together, the fade, the change which alternates between a blue and a green and he’s right about half the time when he stares at it.
They look like the lights off the coast of home, but if he starts to think of home, he’s pretty sure he’ll scream and that would draw attention to him. They’re not supposed to do that. The older ones keep the younger in line that way, wiping out the ones who can’t keep to the established order.
It used to be safe, but that was before. That was with Armand, and Armand can’t hear him anymore. Armand is somewhere else. Daniel was the one to leave, he knows that, but it was so hard to keep up with him now. Wasn’t it supposed to be easier now? It was easier years ago, when Armand would sigh put-upon that his errant fledgling liked to wander off and come with him.
It wasn’t supposed to be like this.
The lights are functionally useless – they aren’t bright enough to illuminate the sidewalks or whatever else was outside.
What was outside?
Surely he’d been outside before, he’d have to have been outside to come inside, so he must know. He just can’t remember and the thought is –
The thought is –
The lights go green this time, and not blue like he expected. An unexpected thrill of joy.
---
Look, it’s not like Daniel doesn’t know something’s wrong with him.
At first, it was just that things were so vivid, so fantastic that he couldn’t drag himself away. Louis had described such things, he’d seen Armand sit and stare for hours and this – this was normal, wasn’t it? It was the noise that hurt. There were so many living, breathing minds and the noise made his hands shake. He’d tried to control it, but it had gotten worse and he knew part of it was because he’d left Armand. It felt like there was nothing tethering him anymore, like he may simply float away if he didn’t find something to hold him there.
The lights were pretty. They were predictable and if he sat far enough away, the buzzing noise didn’t bother him.
It won’t last forever. It’ll pass, and when it passes, he can go home and he’ll be able to handle being around Armand again. Armand won’t look at him and see his mistake, the thing that tries his patience, the child who should never have been made at all, that’s what he’s thinking, Daniel knows it. If he could just stop the noise. If he could just focus his mind and not lose his shit, that would be fantastic.
There’s a payphone outside. He could make a call and go home right now, but he realises with trembling fingers, he doesn’t remember the number.
This wasn’t supposed to happen anymore. Daniel doesn’t remember tearing the telephone booth apart, it’s not like him to be violent with it, that was never him but the phone booth is in ruins and there’s glass in his hands.
It’ll be gone tomorrow night, so he doesn’t bother with it.
---
Hunger drives him away from the lights, so he ventures out. Drinks three, because he doesn’t know when he’ll remember to feed again.
Doesn’t remember what he did with the bodies. Fuck, that’s going to get him in trouble. He’s supposed to deal with that.
He doesn’t want to deal with it. He just wants to watch the lights, but there’s a lecture from Marius on the horizon if he starts leaving bodies around. He’s good at those. Maybe that’s where Armand went.
The reflection of the lights dance across his window, soothing in how predictable they are.
---
One of the bulbs has gone out and the sudden absence of it makes Daniel’s entire skin crawl.
It’s thrown the whole pattern off. He can’t sit and watch them anymore, so he takes to pacing back and forth, back and forth until he forgets about the bulb, looking out at the lights and it hits him with a fresh wave of grief over it’s burnt out darkness. It feels like he’s going to drown without it, he can’t breathe which is ridiculous, he’s a vampire, he doesn’t need to breathe.
Daniel laughs and the sound is deafening.
He’ll get used to the new pattern. He will. He can do this, because if he doesn’t, if he stops and thinks about it, then…
It’s just one little light. How can the loss of one little light impact everything so badly? But it’s black and burnt and broken and –
”Bear witness, this sinner dies for Him!" The light, the blinding light he’d left behind, swallows the voice and Lestat’s screaming Armand’s name, it’s so hard that it forces Daniel to his knees, he can’t be, he can’t he can’t he can’t
he can’t…
---
Daniel.
There’s been something pulling at his mind for days – nights – now, but this is so much louder. It’s the same voice, but the noise of it, shit, he’s going to throw up, can vampires throw up?
Daniel?
Maybe he should find somewhere dark to go to sleep for a while, that’s what Lestat had done when he felt broken, wasn’t it? But if he did that, he was going to be alone with his –
(”Armand!” The smell of the burning, the echoing anguish, and it’s screaming inside his skull. Maybe it’s Lestat but it sounds more like his own voice somehow.)
“Daniel, look at me.”
Daniel’s not so far gone that he doesn’t know that he should probably jump, because he doesn’t know when Marius got there and he really, really doesn’t like the look he’s giving him. He’s seen that look before, on the plane, in the garden full of stars. Distantly, he thinks that’s probably a bad sign and he opens his mouth to tell Marius that he knows that. He’s not crazy, he’s just – he just has to get this under control.
Instead, he hears himself tell Marius that the lights are broken.
Marius looks at him for a long moment, before turning to look at the reflection of the broken lights and merely nods. “Can you stand?”
What kind of question is that? Of course he can stand. Except…he can’t. Shit, he feels so weak, when did that happen?
I could feel your hunger streets away, comes Marius’ voice in his head. But you can’t go out like that, so let’s get you into some clean clothes.
These clothes are clean. No, they’re not. There’s two lines of red blood streaming down his shirt, splodges of it on his jeans and shoes. They’re brown, as if they’ve been through mud but he doesn’t know when he did that.
“I don’t know where my clothes are,” Daniel’s voice is hoarse, and he realises he can’t remember the last time he spoke aloud to anyone. He winces at the sound of it, that desire to curl up and watch the lights hitting him again. He doesn’t want to listen to the sound of his own voice. Who wants to sit and listen to a headcase like that?
There’s something – blood! It’s rich and thick and god, he hasn’t felt this desperate for it in so long. He’s drinking greedily, he knows, and he shouldn’t, he has to stop, that’s part of those rules too, don’t circle the drain.
I’m happy you remember that, Marius’ voice came again. Don’t worry for me, just take what you need and we’ll go.
It was Marius’s wrist he was cradling. Of course it was, he hadn’t gone anywhere, had he? But…
Go?
You left a trail here, Marius’ voice continues. The wound is already shut, and he’s still hungry. I’ve fixed it, but you can’t stay.
But the lights, Daniel tries to communicate.
There are lights at my home, Marius’ voice in his head has changed, it’s softer somehow. He can feel his hand brushing through his hair and shit, when was the last time he’d touched someone he hadn’t killed? Weeks? Months? More? There’s lots of things there, you remember, don’t you?
Daniel tries to picture it, but he can’t. There’s a panic rising in him but there’s Marius’ voie again.
It’ll come back to you, Marius’ voice continues as Daniel’s pulled to his feet. He doesn’t sway anymore. It’ll just take some time.
It’s not exactly going home, but it’s close enough that Daniel doesn’t put up a fight about it. As long as he has something to think about, then he’ll be alright. It’ll just take time, and that’s what he has now, isn’t it?
Nothing but time.
#pure unadulterated angst#daniel molloy#marius de romanus#vampire armand#vc#tw: armand's attempt to go into the sun is seen briefly#tw: mental illness#and HOW#the formatting here is atrocious but tumblr be like that
65 notes
·
View notes
Text
im starting to draw phighters with REAL EYES!1111111111 - mtd
4 notes
·
View notes
Note
5 and 11 for the writers ask thingy 😊
5. What's a piece of lore you haven't shown in your fic or don't think you'll be able to add in?
The aliens, LMAO. I'm sorry, I just can't. That part of canon does not exist in my brain and it never will.
I've been a fan of these books since before MtD came out and I've had to do a lot of re-adjusting and re-jiggering on my headcanons/fanon/thoughts as new books have come out and brought new information to the table. For the most part, I think I've done a good job rolling with the punches, but I draw the line at aliens. I have zero interest in it and would just rather pretend it's not a thing. I made a joke in a tag once that the only aliens in my fic will be Marius getting enraged at how wrong Ancient Aliens gets things, and that pretty much sums it up.
11. Is there anything important in your fic you think readers have missed/overlooked?
I don't think so. Sometimes there are lines or jokes that make me cackle that no one comments on and I wonder if those land for anyone else or if it's just me (the joke about Louis and moon dust in Night Out is one of my favs and no one has ever mentioned it!) But for the most part, I think people who read my fic tend to get what I'm doing. Or at least the ones who comment do! I have no idea what other people might think.
3 notes
·
View notes
Text
annie 🌒
hello, im annie ! im a lesbian who uses she/they/he pronouns.
my interests include but are not limited to:
musicals; falsettos/in trousers, the book of mormon, be more chill, ride the cyclone
omori and other indie games
writing and drawing
music (specifically piano)
i play multiple characters in the mtd roleplay server (limboverse) -- usually whizzer (falsettos), elder price (tbom), and jane doe (rtc)
other stuff:
my pronouns teehee
my carrd 😎👍
4 notes
·
View notes
Text
long story short: the plan (3) ✧ sam and colby
long story short ✧ a parallel universe snc au | ao3
disclaimer: i do not own any aspect of the karate kid universe. does not *totally* follow the karate kid canon (i’ve taken a few creative liberties).
summary: sam and colby enroll at west valley.
word count: 1,116
warning(s): arden’s a lil mean
“So, how are we going to enroll at this high school?” Sam asked.
“And are you sure no one can see my tattoos?” Colby added, rubbing his forearms. He’d been anxious ever since Arden put some sort of paste on his arms. Like she had said, the three of them were still able to see his tattoos, but he still wasn’t convinced that no one else could see them.
“I’m sure, Colby,” Arden said. “Now, quit askin’. Get out of the habit now before you ask in the school and people start thinkin’ you’re crazy.”
“Can you say it just one more time for my sake?”
Arden huffed as she pulled her clunky station wagon into a parking spot. She turned, looked him in the eye, and said without blinking, “No. One. Can. See. Your. Fuckin. Tattoos.”
“Thank you.”
Arden nodded, then turned back around and asked, “Now, anything else before we go in there?”
Sam stared at her, his eyes wide. Did she not listen to anything he had asked? Did she not think it important to tell them what’s going on? She said she was going to brief them in the morning, but all she had done was yell at them to get ready and herded them into her car. Nothing about a backstory, nothing about a plan. Nothing at all.
“Uh, yeah?” Sam said. “How are we enrolling at this school? What’s the plan? Why are there suddenly a bunch of new kids at school? Is that not going to draw attention?”
“Well, there’s only three new kids. You, Colby, and Daniel.”
“What?” Sam said.
Arden ignored him. “As for how you’ll be enrollin’, I know a thing or two about forgin’ documents.”
“Did the MTD teach you that?” Colby asked.
She turned to look at him, a smirk curling across her face. “If it helps you sleep better, sure. That’s where I learned it from.”
Colby’s brows furrowed together and he looked like he wanted to question her further, but he stopped himself. Perhaps that was for the best. This girl was…psychotic? Off her rocker? Dangerous? Whatever—Sam couldn’t pinpoint what she was, but he wasn’t about to say, ask, or do anything that could set her off. For now, she was an ally. And he knew better than to risk losing that in an unfamiliar universe when he and Colby were wholly reliant on her and her knowledge.
“As for why you’ve moved here. You two are step-brothers. Quick, decide who’s parents married who.”
“Uh, my mom married Sam’s dad,” Colby decided.
“You got that Sam?”
“My dad married Colby’s mom,” Sam repeated.
“Great. The reason that the two of you moved here was because they passed away. A horrible car accident. Now, for simplicity’s sake, Colby’s dad and your mom are out of the picture, too. Where did you two move from?”
“Kansas,” Sam said. “In our universe, we moved to LA from Kansas, so it’ll be easy to remember it if we kept the same story.”
“Good thinkin’, Sam,” Arden said. Wow, a compliment? He wasn’t expecting that. “Now, the two of you moved in with my parents. My mom, Judy, is a nurse and my dad, Garrett, is an accountant. Who are you livin’ with and what to do they do?”
“Aunt Judy is a nurse and Uncle Garrett is an accountant,” Sam and Colby repeated.
“Hey, I was wondering something,” Colby said.
“Yes?”
“What side of the family are you on?” he asked.
“Huh?” Arden’s brows furrowed together
“Like, are you related to my side or Sam’s side? Since we’re step-brothers and all.”
Arden looked impressed, like she hadn’t considered that before. “Because you asked, Judy and Garrett can be on your side of the family. Judy is your mom’s sister. Anything else?”
“Are you not enrolling here, too?” Sam asked. “Earlier, you said there was only three new students. Implying that you’re not enrolling.”
“Oh, I’m already a student here.”
“But I thought you were an agent in training for the MTD.”
She snorted. “Next you’re gonna to tell me that you believe Arden’s my real name.”
“Is…Is is not?”
She didn’t answer. Instead, she said, “We better be gettin’ to the front office. Need to get your schedules and all that jazz.”
She set the two of them to the front office of the school. It looked pretty standard. Potted plants were scattered around orange-flecked folding chairs. The room was bright, and Sam had to squint to see. A large counter cut the room in half, and three desks were behind the counter. One of the desks was being manned by an older women.
The woman looked up when the trio entered and approached her desk. “Can I help you?”
Arden put on a charming smile and said, “Hi, Angie! My cousins are here to pick up their schedules? They’re new here.”
“Of course,” Angie said. She typed away on her computer. “Give me just a second to print off your schedules.”
The printer beside her desk whirred as a series of papers came out. She pulled the papers from the tray and began highlighting something on two of the papers. She pushed the papers in front of the boys and said, “These are your schedules and a map of the school. I've highlighted the best routes to your each of your classes so you won't get lost.”
Sam and Colby took their respective schedules and maps.
“Now, would either of you like a tour of the school? One of the aides should be here soon.”
“Oh, that won’t be necessary, Angie!” Arden said. “I’ve got the tour covered for them.”
“Alright! Well, welcome to West Valley, boys. I’m sure you’ll have a grand time here.”
They left the office and Arden began to walk off. Sam and Colby jogged after her, Colby asking, “So? Are you going to give us a tour or what?”
She snorted. “Figure your own shit out.”
“Well, where are you going?” Colby asked. “We might have the same class together.”
“Biology with Rayburn.”
“Oh, I’m going there too,” Sam said.
“Then keep up, Golbach,” Arden said. To Colby, she said, “We’ll meet up at lunch and report anything we’ve found out. Then, we’ll put together a more solid plan. Got it?”
“Yes, ma’am.”
“Now, where are you headed?”
“Uhh, English with Salyers.”
“That’s the other side of the school. Better get a move on. And good luck.”
“Thanks, you too.”
And, as Colby walked away from Sam and Arden, Sam couldn’t help but think of how in over their heads they were. There was absolutely no way this was going to work. Was there?

#long story short: a parallel universe snc au#sam and colby#sam golbach#colby brock#snc#xplr#traphouse#trap house#traphouse 2.0#trap house 2.0#sam and colby fanfic#sam and colby imagine#sam and colby fanfiction#sam and colby fic#sam and colby fan fiction#sam and colby fan fic#sam golbach fanfic#sam golbach imagine#sam golbach fanfiction#sam golbach fic#sam golbach fan fiction#sam golbach fan fic#colby brock fanfic#colby brock imagine#colby brock fanfiction#colby brock fic#colby brock fan fiction#*written by: me#starrybrock
11 notes
·
View notes
Text
Errors Free Tax Reforms for Businesses and Self-Employed Tax Returns UK
The tax reforms key points are, the changes mean businesses will be taxed on profits arising in a tax year also it will align the way self-employed profits are taxed with other forms of income, such as property and investment.
Reforms to the tax system that aim to make it easier for self-employed workers and small businesses to fill out their returns have been announced by the Government.

The changes, which will come into force by 2023 and have been drawn-up alongside representatives of small businesses, will mean businesses will be taxed on profits arising in a tax year, rather than profits of accounts ending in the tax year.
It will align the way self-employed profits are taxed with other forms of income, such as property and investment income.
Under the current system, tax returns filed by the self-employed, sole traders and partnerships are based on a business’s set of accounts ending in the tax year (April 5). More complex rules apply when a business starts and draws up its accounts to a date different to the end of the tax year.
In those cases, taxpayers pay tax for their first tax year on the period to the end of the tax year, and then in subsequent years on the basis of their full accounting year, meaning profits are taxed twice and complex rules apply to relieve the double taxation when the business finishes.
Financial Secretary to the Treasury Jesse Norman said:
“These complex rules lead to thousands of errors and mistakes in self-employed tax returns every year.
“Simplifying them will allow self-employed people to spend less time doing tax admin and more time growing their business and creating jobs.”
The change to the time periods against which businesses report their tax will also reduce the number of times those with several sources of income will need to report their income under MTD for Income Tax.
Know more about changes in coronavirus government schemes for businesses and self-employed, get in touch with Morgan Reach Certified Chartered Accountants. We’ll guide you through what support is available for you or your business as well as the latest news that may affect you.
#tax reforms uk#uk tax reforms#tax return uk#small business tax return#self-employed tax return#tax system uk#accounting services#chartered accountants#bookkeeping services#filing accounts uk#corporate tax
2 notes
·
View notes
Text
Yo, I’m thinking of doing a stream if anyone is interested. I wanted to draw The Owl House stuff, if you stop by you can tell me what to draw!
I’ll be doing it 9/13 at 7:15pm mtd to probably 9pm mtd, that’s 9:15 EDT and 6:15pm PDT
twitch.tv/hope170gaming
Please come by and hang out!
#toh#the owl house#the owl lady#eda clawthorne#owl eda#lilith clawthorne#lumity#luz noceda#amity blight
25 notes
·
View notes
Text

Toga sketch ❤️
#my hero academia#mha#bnha#boku no hero academia#mtds drawing#toga himiko#himiko toga#mha toga#bnha art#digital drawing
26 notes
·
View notes
Text
Takahiro A. Kato et al., Multidimensional anatomy of ‘modern type depression’ in Japan: A proposal for a different diagnostic approach to depression beyond the DSM-5, 70 Psychiatry Clin Neurosci 7 (2016)
Abstract
Japan’s prototype of depression was traditionally a melancholic depression based on the premorbid personality known as shūchaku-kishitsu proposed by Mitsuzo Shimoda in the 1930s. However, since around 2000, a novel form of depression has emerged among Japanese youth. Called ‘modern type depression (MTD)’ by the mass media, the term has quickly gained popularity among the general public, though it has not been regarded as an official medical term. Likewise, lack of consensus guidelines for its diagnosis and treatment, and a dearth of scientific literature on MTD has led to confusion when dealing with it in clinical practice in Japan. In this review article, we summarize and discuss the present situation and issues regarding MTD by focusing on historical, diagnostic, psychosocial, and cultural perspectives. We also draw on international perspectives that begin to suggest that MTD is a phenomenon that may exist not only in Japan but also in many other countries with different sociocultural and historical backgrounds. It is therefore of interest to establish whether MTD is a culture-specific phenomenon in Japan or a syndrome that can be classified using international diagnostic criteria as contained in the ICD or the DSM. We propose a novel diagnostic approach for depression that addresses MTD in order to combat the current confusion about depression under the present diagnostic systems.
Clinical Picture
Case: male, 24 years old
Chief complaint: No desire to do anything
Medical history: No previous psychiatric disorder
Family history: Nothing of note
Developmental and social history: He is the first son, with an older sister. His father is a company employee, his mother a full-time homemaker. There was nothing particularly problematic during junior or senior high school, although apparently he sometimes deliberately did not apply himself to the subjects of teachers that he disliked. At university he took part in group activities and had a part-time job, just like other students. He was not terribly enthusiastic about searching for a job and aimed to become a civil servant. After graduation, he attended a vocational college for a year to prepare for the entrance exam to the civil service, and at the age of 23 started to work in the municipal government of a provincial city – he says he just happened to sit the exam and pass it.
History of present illness: He did not particularly dislike the work in the place he was assigned to after being hired, though he was not greatly interested in it either. However, he would occasionally be absent from work; he says this was because he had an annoying boss who he couldn’t stand the sight of. Nonetheless, it was not a case of being unable to go to work because he was depressed, and when he was absent from work he would play slot machines, go to the movies, or go shopping. In June 2010, a year after starting work, he married a female colleague from the same work-place with whom he had fallen in love. In May 2011, his first child was born. He was still halfhearted about his job, but also finding it hard to be at home, he would play slot machines or go to the movies. Raising the child proved to be very difficult, but his wife had stopped working and, together with both his mother and her own mother, managed the household very well.
In December 2011, his boss reprimanded him for his attitude toward his work. He had previously been given warnings on a number of occasions, but apparently this time the reprimand he received was very severe. He subsequently left work early, complaining of feeling unwell. He says that from that day on he was unable to sleep at night. He became easily irritated and tended to have feelings of desperation. Even though, he went to work properly every day. Whilst at work, he had no motivation to do anything and had no energy. He would become angry and did not feel like attending work social events, such as the year-end party or the New Year party. He would tend to stay out of his boss’s sight. He would feel a little more cheerful only when he played slot machines and when spending time in an Internet cafe, but when he went home he would again slip into gloom because, he says, he found it boring. His anger was not toward himself but others, such as his boss and his wife. He sometimes would feel valueless himself; however, he could alleviate such unpleasant feelings by his devotion toward his hobbies. His sleep was constantly mildly disturbed but not severely, and sometimes he would have trouble getting to sleep and fail to get up in the morning. Therefore, from around the middle of January he started to fail to go into his office once/twice a week and during this absence he would surf the net to relax or go out to play slot machines.
In March of 2012, he found a site on the Internet called ‘Mind medicine cures your Depression!!’ which contained a checklist for depression, and he quickly came to believe that he himself must have ‘depression.’ The following day, he decided to go to a local psychiatric clinic for a prescription of antidepressants. He entered the examination room, greeting the doctor politely, then he voluntarily read out his life history and medical history from a memo he had prepared. When he finished, he handed the psychiatrist in charge a depression checklist, which he had found on the Internet, and requested a particular medicine by himself: ‘Doctor, as I have just mentioned, these diagnostic criteria apply to me. I heard that selective serotonin re-uptake inhibitors are effective.’ Based on his examination, his score on the Hamilton Rating Scale for Depression1,2 was 17 (mild depressive level); he met the DSM-IV criteria for a major depressive episode (based on the handbook, entitled Quick Reference to the Diagnostic Criteria from DSM-IV-TR3) and was diagnosed as suffering from depression. He requested a medical certificate then and there. Additional clinical history revealed that he did not meet the diagnostic criteria for avoidant personality disorder, schizoid personality disorder, or narcissistic personality disorder. Also, according to information supplied by his wife, who was present when he was examined, there was nothing particular in the symptoms to suggest that the illness was feigned.
This clinical picture was originally used for the symposium during the 109th annual meeting of The Japanese Society of Psychiatry and Neurology in Fukuoka, 2013.
Introduction
Cases like the above have emerged in Japan since around 2000, and these cases have been called ‘modern type depression (MTD)’ – a novel form of depression. This catchy ‘modern’ name has quickly and widely spread to the public via Japan’s mass-media and Internet-related media, while the name itself has not been regarded as an official medical term, and there is no consensus guideline for its diagnosis and treatments, which has led to confusion when dealing with MTD in clinical practice. Scientific literature about MTD remains very limited. In this review paper, we summarize and discuss the present situation and issues regarding MTD – focusing on historical, diagnostic, sociocultural and international perspectives, by referring to our recent international survey.4 Is MTD a phenomenon limited to Japan? The pilot survey has indicated that MTD may exist not only in Japan but also in many other countries with different sociocultural and historical backgrounds. It is therefore of interest to establish whether MTD is a cultural phenomenon specific to Japan or a syndrome that can be classified using the present international diagnostic criteria of the ICD/DSM. Finally, we propose a novel diagnostic system of depression including MTD in order to combat current confusion regarding the diagnosis of depression under the present ICD/DSM diagnostic systems.
Historical Background
Just since the beginning of the 21st century, Japanese psychiatrists have increasingly reported patients with a type of depression that does not seem to fit the criteria of the ICD-10 and the DSM-IV, and which is widely denoted as MTD among Japanese psychiatrists. The Japanese psychiatrist/psychopathologist Shin Tarumi reported the increasing occurrence of MTD and he labeled MTD as Dysthymia-gata utsu-byo (dysthymic type of depression) in the Japanese literature.5,6 Tarumi described the associated premorbid personality as Typus dysthymicus (TD) and compared it with Japan’s traditional type of depression.5,6 Tarumi defined the characteristics of MTD with TD as follows: (i) younger generation; (ii) attachment to oneself with less loyalty for social structures; (iii) feeling distressed about rules/order; (iv) negative feelings about social order/models; (v) vague sense of omnipotence; and (vi) not hard-working by nature (Table 1).6–17 MTD is also characterized by (a) distress and reluctance to accept prevailing social norms; and (b) avoidance of effort and any strenuous work.4,18 Most sufferers of MTD are born after 1970, that is, the generation growing up with home video games in the era of Japan’s high economic growth. Youths with MTD tend to feel depressed only when they are at work; otherwise, they can enjoy the virtual world of the Internet, video games, and pachinko (Japanese pinball). Therefore, sufferers of MTD have difficulties in adapting to work/school and participating in the labor market.
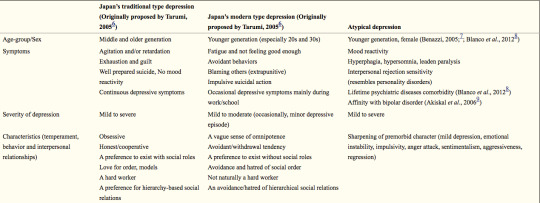
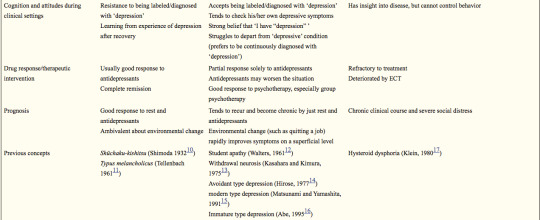
Table 1. Comparison between Japan’s traditional type depression, Tarumi’s Japan’s modern type depression and atypical depression
This table is a proposed comparison between Japan’s traditional type depression, Japan’s modern type depression and atypical depression according to Tarumi 2005,6 Tarumi & Kanba 2005,5 and Kato et al. 2011.4 Data, especially the section on ‘Drug response/Therapeutic intervention,’ has not yet been validated. ECT, electroconvulsive therapy.
Formerly, the melancholic type of depression had been regarded as a typical form of depression amongst the Japanese population, whose premorbid personality was defined as shūchaku-kishitsu (SK) by the Japanese psychiatrist Mitsuzo Shimoda.10,19 Shimoda characterized SK as: (i) middle aged; (ii) strong loyalty to society and community and one’s role within these structures; (iii) a preference for rules and order; (iv) positive feelings about social order/models; (v) attentive and diligent; and (vi) fundamentally hardworking.10,19,20 SK has been discussed in a similar context to Tellenbach’s Typus melancholicus (TM), which was identified amongst Germans after World War II.11 Tellenbach described the premorbid personality of patients with unipolar endogenous depression as orderly, devoted to duty and to family members, and scrupulous.11 Such types of depression based on SK and TM are considerably different from MTD. On the other hand, since the 1970s, different types of depression have been reported by Japanese psychiatrists and psychopathologists, such as taikyaku shinkei-sho (withdrawal neurosis);13 tohi-gata utsu-byo (avoidant type of depression);14 gendai-gata utsu-byo (modern type of depression);15 and mizyuku-gata utsu-byo (immature type of depression).16 Commonalities between the above types of depression and the currently emerging MTD have been pointed out. The former (taikyaku shinkei-sho, tohi-gata utsu-byo, gendai-gata utsu-byo and mizyuku-gata utsu-byo) was limited to highly educated youth, but MTD has been known to affect youth regardless of educational backgrounds.4
The 24-year-old man presented in the above clinical picture expressed moderate depressive symptoms just after a stressful event at his workplace. He came to regard himself as having severe depression, and finally he asked a doctor for sick leave in order to take a rest. His depressive symptoms mainly emerged during working time, and his symptoms were relieved in other situations. His characteristics, including behaviors and interpersonal relationships, contained the following features: not naturally a hard worker; an avoidance/hatred of hierarchical social relations; a preference to exist without social roles; extrapunitive type; and a vague sense of omnipotence. These features are exactly matched with MTD proposed by Tarumi.5,6
Diagnostic Issues of MTD
MTD has not been regarded as an official medical term, and various diagnoses have been applied based on ICD-10 and DSM-IV criteria. Our case vignette survey among Japanese psychiatrists suggests that MTD tends to be diagnosed as a variety of psychiatric disorders, such as mood disorder (296, code of DSM-IV; the same shall apply hereafter), dysthymic disorder (300.4), adjustment disorder (309) and adjustment disorder with depressed mood (309.0) by Japanese psychiatrists.4 Interestingly, some Japanese psychiatrists reported that categorical diagnostic systems, such as the ICD-10 and the DSM-IV, are not applicable to MTD. The case vignette survey was also administered to foreign psychiatrists at the same time, which revealed that they tend to diagnose the MTD case as mood disorder (296), dysthymic disorder (300.4), adjustment disorder (309), adjustment disorder with depressed mood (309.0) and adjustment disorder with mixed anxiety and depressed mood (309.28). Based on the reports and our clinical experiences in Japan, it is challenging to differentiate between MTD and other types of depression, such as atypical depression (AD) and dysthymia.
Atypical depression
It is often difficult to differentiate MTD from AD due to some overlap of their clinical features, including young onset, impulsivity, aggression toward others, behavioral symptoms similar to personality disorders, being refractory to treatment, and severe social disability caused by a chronic clinical course.7,8,21
Patients with MTD tend to have specific features of personality or characteristics, while patients with AD have no such features. However, it is also well known that the characteristics of AD patients would alter dramatically around the onset of AD, showing its aggressive and impulsive aspects. Around the onset of AD, the characteristics in patients with AD often sharpen, and their emotions become unstable. The features and alterations of characteristics in patients with both AD and MTD often lead to interpersonal rejection sensitivity and social disability. Formerly, Klein suggested the concept of ‘hysteroid dysphoria’ in regards to the disease concept related to AD,17 and recently, AD has been suggested to have the affinity of characteristics or symptoms with bipolar II disorder.9 In the present stage, there exists no specific markers to differentiate MTD from AD, but specific symptoms of AD (hyperphagia, hypersomnia, leaden paralysis, and mood reactivity) seem to be useful for the differentiation.
Dysthymia
Dysthymia is also on the differential diagnosis for MTD, because both show a chronic clinical course and less severe depressive symptoms. In regards to this differentiation, the Japanese psychiatrist Shin Tarumi did not refer to the distinct difference between the two diseases and just stated ‘MTD has not completely become dysthymia yet.’5,6
In DSM-5, dysthymia (dysthymic disorder) was combined with chronic major depressive disorder under the name of persistent depressive disorder.22 The DSM-5 diagnostic criteria for persistent depressive disorder still characteristically include subjective superior symptoms, but not some objective depressive symptoms, such as psychomotor agitation/inhibition and suicidal ideation. These would be common features of MTD. Needless to say, the concept of dysthymia itself has not been clearly defined, which makes the differentiation between MTD and dysthymia more difficult.
Previously, Akiskal developed a framework of soft bipolar from subaffective dysthymia to character-spectrum disorders by therapeutic reactions.23 Similar to soft bipolar, the present situation has suggested that MTD might be heterogeneous. Therefore, further studies are needed to clarify the syndrome of MTD, which has important implications for the selection of appropriate interventions.
Personality disorder
Tarumi did not include the comorbidity of personality disorders (avoidant personality disorder, schizoid personality disorder, or narcissistic personality disorder) in clinical case descriptions of MTD in his original paper.5 However, the international case vignette survey by Kato et al. in 2011 has suggested that personality problem is the most highly influential factor for MTD, and a variety of personality disorders are suggested to be comorbid with MTD.4 The underlying features of personality have yet to been clarified, while psychopathologists have highlighted the temperamental features of MTD syndrome as narcissism (omnipotence) and avoidance.5,6,24 In addition, immaturity may be an important factor.25 People who originally have a tendency toward an immature and narcissistic personality may easily develop depression and evasive behaviors when confronted with stressful situations at school and in the work-place (Fig. 1).
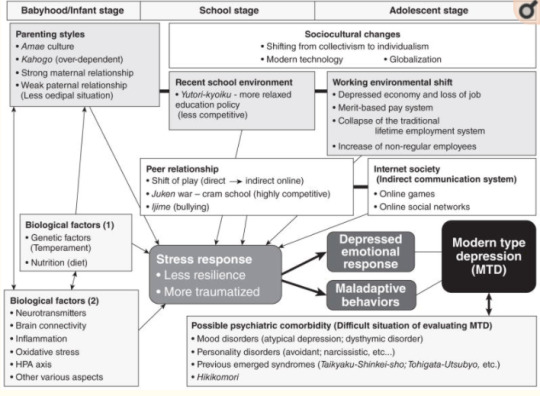
Figure 1. Multidimensional understandings of Japan’s modern type depression (MTD). A variety of psychosocial factors, from the early stages of life through to adolescence, have been suggested to contribute to the onset of MTD. Especially important are childrearing, school and later workplace environments. Within this, parent–child relationships, and how/whether good-enough relationships between peers and friends have been established is vital. The establishment of these bonds can facilitate smooth relationships with workplace colleagues and superiors later in life. However, in MTD, the establishment of such fundamental interpersonal skills during the early stages of life may be insufficient, which can induce vulnerability to stress, meaning that mental dysfunctions are more likely to develop. In other words, lower resilience and the greater possibility of experiencing stress traumatically. Regarding the sociocultural impact in Japan, along with modernization and globalization, there has been a continuing shift away from the hitherto respected and venerated ‘group mentality’ to an ‘individualism’ in which individual achievements are pursued and this shift has resulted in rapid changes in school and work environments. In addition, we suppose that such sociocultural factors are occurring along with an interrelated biological basis, and it is important not to ignore underlying biological factors. With regards to diagnosis and evaluation of MTD, we are in a transitional period and a differential method to distinguish from existing psychiatric diagnoses is warranted. HPA, hypothalamic–pituitary–adrenal.
On the other hand, in the case vignette survey, only Japanese psychiatrists disregarded the factor of personality – SK, that is, immodithymia – as a component cause of Japan’s traditional type of depression, while many psychiatrists in other countries believed that the SK personality strongly affects the onset of depression as a pathological factor. Generally speaking, the Japanese are regarded to be a diligent, scrupulous and hard-working people, and such personality traits have been positively accepted and moreover encouraged in Japanese society over a long period of history since the Samurai era.26 However, these personality traits are not always considered to be positive but as a cause of illness, such as obsessional personality, by experts, including psychiatrists, anthropologists and sociologists in Japan and other countries.27,28 Therefore, Japanese psychiatrists’ opinions in the case vignette survey indicate that not only lay people but also psychiatrists in Japan have been influenced by such Japanese cultural contexts.4
Interestingly, a Japanese clinical study, published in 1997, suggested that TM, which is similar to SK, is not the premorbid personality trait of unipolar (endogenous) depression in Japan.29 This result might have predicted the recently suggested prototype shift of depression in Japan from TM to TD.30
On the other hand, Kotov et al. performed a meta-analysis regarding the association between the personality traits in the Big Three model (negative emotionality, positive emotionality, and disinhibition vs constraint) and Big Five model (neuroticism, extraversion, conscientiousness, agreeableness, and openness), and common psychiatric disorders, such as depression, anxiety and substance abuse disorders.31 The meta-analysis revealed that these common psychiatric disorders are strongly connected to personality. Both major depressive disorder (MDD) and dysthymic disorder showed a similar tendency for high neuroticism and low conscientiousness. Dysthymic disorder showed the most pathological profile. Actually, more than other ailments, dysthymic disorder showed extremely negative extraversion, negative conscientiousness, and positive disinhibition. There is a fairly small number of studies but this outcome is consistent with the argument that dysthymic disorder may be best seen as a form of personality disorder.32 Indeed, dysthymic disorder tends to be chronic and is often lifelong.33 Hence, prominent personality disturbance can be expected to manifest in dysthymic disorder. Surprisingly, the connection between MDD and extraversion was unexpectedly weak. On the other hand, low extraversion was revealed to play an important role in dysthymic disorder. Prospective studies are extremely rare in this field and a causal relationship is yet to be elucidated. Moreover, there are only a few longitudinal studies, the problem of comorbidity, and other limitations (Japanese clinical data seem not to be included in this meta-analysis). In spite of these limitations, this meta-analysis is an important resource when considering the relationship between MTD and personality.
Further clinical, psychopathological and epidemiological studies are needed to clarify underlying personalities, temperaments and characteristics of depression and MTD among particular cultural groups.
Sociocultural Aspects
Psychiatric disorders are strongly influenced by culture, society, history and region.34,35 In any case, much attention should be paid to any medical culture that allows for an immediate diagnosis and the dispensation of medicines in such cases. Japan’s rapid socioeconomic and cultural changes have affected the lifestyle, behavior and mentality of people of all ages in Japan,36 and new types of psychiatric disorders or behavioral disorders have recently appeared in Japan. Tarumi suggested that MTD is caused by the unique Japanese cultural background and sociocultural changes in Japan.5,6 Tarumi regarded MTD as the byproduct of Japan’s historical socioeconomical shifts; beginning with World War II, the following period of high and rapid economic growth (1960–1980s), the economic crisis (1990s), and the diversity and complexity of modern society in the 21st century.5,6 Traditionally, Japanese society has greatly encouraged immodithymia, but modernization, globalization and the introduction of Western culture have led to a mixture of cultures and the celebration of individualism in Japan. The effects of changes in the education system and a move from its traditional disciplinarian base to Yutori education, a system that emphasizes the individual and freedom, may have been great. In the corporate world, the collapse of the traditional nenkō joretsu or seniority-based promotion system will also have had an effect. With the disintegration of the seniority system, there has been an evolution to an intensely competitive society and a distancing from the traditionally harmonious Japanese sense of group belonging.37 It has been suggested that a lack of a sense of belonging could be behind the increase in middle–older-age suicide.38,39 With regards to MTD, the problem of such a sense of belonging may be another major consideration. In the corporate world, younger employees who do not have such a sense of belonging and exhibit aspects of depression at work are often able to function normally and happily with such a sense on weekends, at places of leisure and/or online (Facebook, etc.), and this may reflect that very lack of a sense of belonging within the traditional Japanese organizations. According to the analysis by Takahashi et al.,40 the Japanese corporate organization gave a sense of belonging and community to workers because of its long-term-based relationship under the systems of seniority and permanent employment. After the burst of the bubble economy in the 1990s, however, these traditional systems collapsed and this organization no longer provides a sense of community or belonging.
Unfortunately, Japanese society had not prepared for the effects of this transition. Thus, patients with symptoms of MTD may have often been judged as lazy or ‘sloths’ because one of the most highlighted characteristics of MTD is the tendency to feel depressed only during work or at school.4,18
MTD and hikikomori based on amae
While the psychopathology of MTD is not well understood, it has been suggested that it is related to amae and other Japanese forms of mentality, a suggestion that raises the possibility of MTD as a cultural syndrome or form of psychopathology that predominates in Japan.28
Takeo Doi, a psychiatrist and psychoanalyst, described Japanese dependent behaviors with the word amae.28 The person who is acting amae may beg or plead, or alternatively act selfishly and indulgently, while secure in the knowledge that the caregiver will forgive this. The behavior of children towards their parents is the most typical example of amae. Doi argued that child-rearing practices in Western society seek to stop this kind of dependence in children, whereas in Japan it persists into adulthood in all kinds of social relationships.28 Even now, compared to Western societies, in Asian societies, including Japan, Korea and Taiwan, young people tend to be more economically dependent on their parents, and this phenomenon seems to be one of the expressed forms of amae.41 Hikikomori, a form of social withdrawal characterized by persistent isolation in one’s home for more than 6 months, may be indirectly promoted by amae to the extent that parents accept their child staying at home for prolonged periods of time.41 Even though the concept of amae was originally considered to be uniquely Japanese, contemporary opinions suggest that amae is actually more universal in nature.42 Thus, there is an interesting parallel to hikikomori that has been thought of as unique to Japan but, as our preliminary results show, is perceived by psychiatrists as occurring in a variety of other countries.41 In addition, our international clinical investigations have revealed real hikikomori persons in different countries, including the USA.43,44 These facts suggest that hikikomori and/or MTD could also be a universally observed psychiatric problem.
Cultural/social psychological understandings of MTD and hikikomori
The sociocultural background and tradition of amae is related to hikikomori and MTD. On the other hand, as another research stream, cultural psychologists and social psychologists have focused on the cultural uniqueness of inter-dependence with experiment and quantitative methods.45–49 A common argument being that East Asians are more collectivistic and/or more inter-dependent than Westerners.50–52 In a collectivist culture, inter-dependence is emphasized and in an individualist culture, independence has more value than inter-dependence. A common traditional assumption of these concepts is that collectivistic people tend to prefer harmonious inter-dependence to individual motivation or self-interest. This means that collectivists are ‘harmony seekers.’ On the other hand, Hashimoto and Yamagishi have claimed that the above assumption is not necessarily true, and have recently proposed a novel dimension, namely ‘dis-engaging inter-dependence.’53 They have claimed that the conventional distinction has focused only on dis-engaging independence and engaging interdependence, and relatively ignored the opposite (engaging independence and dis-engaging interdependence). Engaging independence is characterized as voluntary formation of interaction relationships with others to find desirable interaction partners and to prove to others that one is a desirable interaction partner. Hence, individualistic and harmonious. On the other hand, dis-engaging interdependence is characterized as ‘rejection avoidance’ to try to confirm qualification of informal membership in a given social group by following the group norm and informal rules. It is not voluntary adaptation for the group, but motivated to avoid being ostracized by other group members. Hence, collectivistic but not harmonious.
Of these categories, dis-engaging inter-dependence may be deeply related to MTD and also hikikomori. Patients with MTD tend to avoid many interpersonal relationships because they are so afraid of being hurt and humiliated by others. They are always scared of potential psychological attack from others. In particular, hikikomori persons do not want to leave their homes. For them, their family is the only group that they are convinced will not hurt them. This is consistent with the characteristics of dis-engaging interdependence. Although an empirical demonstration has yet to be carried out, it would be plausible to consider MTD patients as having much higher levels of dis-engaging inter-dependence than normal and healthy people. According to Hashimoto and Yamagishi,53,54 comparing student samples from the USA and Japan, the Japanese showed significantly higher scores on dis-engaging inter-dependence than Americans. This may be indirect evidence that it can be related to MTD because currently MTD is frequently observed among youth in Japan. Interestingly, a recent review article by Li and Wong has indicated the interaction between hikikomori and inter-dependence.55 It is necessary to conduct systematic empirical research to investigate the relationship (and/or causality) between MTD and dis-engaging inter-dependence.
Biological Factors
While the biological foundation of MTD is unknown, some specific biological mechanisms are worth speculation. The frequently observed clinical viewpoint that treatment with only the standard pharmacological therapies for depression is not successful for patients with MTD has strongly suggested that a different biological mechanism from traditional depression may exist in the biological features of MTD.
Abnormal function of the hypothalamic–pituitary–adrenal (HPA) axis has long been proposed as a candidate biological foundation of depression.56 A number of studies using the dexamethasone (DEX)/corticotrophin-releasing hormone (CRH) test have been conducted for the assessment of HPA axis function in patients with depression, while these outcomes have been inconsistent.57 The inconsistency may result from the heterogeneity of depression. Hori et al. have reported key findings in elucidating the heterogeneity of depression using the DEX/CRH test and the Temperament and Character Inventory in patients with MDD.58 MDD patients with high cooperativeness showed exaggerated cortisol reactivity; on the contrary, patients with low cooperativeness and high reward dependence showed blunted cortisol reactivity.58 In addition, Hori et al. revealed that MDD patients with escape-avoidance coping showed blunted cortisol reactivity.59 On the other hand, schizotypal personality traits60 and low novelty-seeking with harm avoidance61 in healthy adults are reported to be correlated with exaggerated cortisol reactivity, which proposes the possibility that functions of the HPA axis differ with character and temperament. Low cooperativeness and escape-avoidance coping coincide with the features of MTD, thus the biological foundation of MTD may, at least to some extent, result from abnormal functions of the HPA axis. While not MTD, abnormal function of the HPA axis (abnormal cortisol reactivity in DEX/CRH test) has also been observed in patients with borderline personality disorder62 and atypical depression.63 Based on the above data, Kunugi et al. has recently proposed a classification of depression focusing on the HPA axis functions.64
Interestingly, a recent clinical research regarding atypical depression has suggested a significantly higher comorbidity with metabolic syndrome.65 Metabolic syndrome has recently been suggested to be related to oxidative stress and inflammation.66 Our pilot study has indicated a correlation between serum proinflammatory cytokines and depressive symptoms/personality traits in Japanese university students (unpub. data). We propose an inflammation hypothesis of psychiatric diseases, including depression, via microglia, brain immune cells.67–71 These data may suggest that inflammation and oxidative stress may link to MTD. Further translational studies are needed to clarify the biological foundation of MTD.
Therapeutic Approach
No systematic data have been reported regarding therapeutic interventions of MTD. While our previous case vignette survey has suggested that both psychotherapy and pharmacotherapy were recommended to treat MTD, psychotherapy was especially preferred by psychiatrists in all countries.4 Interestingly, Japanese psychiatrists seemed to hesitate to recommend pharmacotherapy for MTD. In addition, some Japanese psychiatrists hesitated to treat MTD at all. These data have indicated that Japanese psychiatrists, at least to some extent, regard MTD as a non-medical condition. This was in contrast to most psychiatrists in other countries endorsing the need for active treatments to MTD.4 Why is there a discrepancy in psychiatrists’ attitudes toward MTD? These findings may suggest that Japanese psychiatrists themselves are bound to their own socio-cultural and historical contexts.4
The arrival of new antidepressants to Japan in 1999 has also been suggested to have influenced the public view toward depression,72 and may have led to a similar phenomenon occurring in Western countries.73 Previously, depressed persons had tended to hesitate to visit psychiatrists, and Japanese psychiatrists had tended to equate depression only with the traditional melancholic type. Perhaps with the introduction of public awareness campaigns for depression and antidepressants, people who considered themselves depressed began to feel less self-conscious about visiting psychiatrists. This may have been a contributing factor leading to increasing numbers of visits of depressed persons to psychiatrists in Japan.4 However, as the case vignette survey implies, this popular shift has not been accompanied by similar changes in the perception of Japanese psychiatrists, who have very much remained deeply bound to earlier, more traditional conceptions of depression. On the other hand, the results of the case vignette survey indicate that psychotherapy was regarded to be of importance for MTD patients with Japanese psychiatrists who did not see a role for pharmacotherapy.4 Therefore, public education about depression and psychotherapy as a treatment should also be considered as one of the possible solutions to alleviate this discrepancy between the general population and psychiatrists in Japan.
Therapeutic strategies regarding MTD based on pathophysiological understandings should be established. We hypothesize that child and adolescent development has been impacted by rapid environmental changes, which may cause the novel phenomenon. The ways of ‘playing’ among children and adolescents have dramatically shifted from ‘direct playing’ (direct communication in a physical space, such as outdoors or in parks) to ‘indirect playing’ (indirect virtual communication via video games and Internet-related materials) within the past decades.36 People who have grown up in such new environments may become confused and depressed when they enter the traditional workforce and encounter the need for real direct communication. Therefore, psychoeducation and (group) psychotherapy may be the recommended approaches in order to develop skills of direct communication, which may lead to a smoother adjustment to adult communication environments. In addition, pharmacological and social approaches may also be effective. Clinical research to measure therapeutic responses should be performed to dig up the appropriate intervention.
How to Solve the Issues Associated with MTD
Blind-spots of the DSM system
Recently, early-career psychiatrists in Japan have considered that it is possible to make diagnoses based solely on the abbreviated pocket-sized DSM-IV-TR. This book, entitled the Quick Reference to the Diagnostic Criteria from DSM-IV-TR,3 states that it is intended to be used in combination with the unabridged version of the DSM-IV-TR (which is 900+ pages in length).74 In fact, the DSM-IV-TR also states in an introductory section entitled ‘Cautionary Statement’ that ‘the proper use of these criteria requires specialized clinical training that provides both body of knowledge and clinical skills.’ Many early-career psychiatrists seem to be unaware of these facts. The DSM-IV-TR includes detailed explanations of diagnostic criteria, diagnostic features, and differential diagnoses for each disorder. However, even in the unabridged version, there is no mention of which examinations should be performed in the garnering of information for each disorder. This can only be achieved through not only reading of psychiatric textbooks but also the accumulation of real clinical experiences with supervisory psychiatrists involving the joint examination of patients in a hospital/clinic setting. However, in reality, early-career psychiatrists who are actually willing to accumulate such valuable experiences are on the decline. In addition, there are some problems based on the nature of operational diagnosis in DSM. Parker indicated that operational criteria of the depression dimensional model in DSM has made it easy to diagnose depression, and also resulted in loose diagnostic practice blunting clarification of causes and treatment specificity of depression.75
On the other hand, the Structured Clinical Interview for DSM-IV (SCID) is considered the best available method for diagnosis of psychiatric disorders, but in reality there are limitations to its applicability. When applying the systematic diagnostic criteria for MDD based on the DSM-IV (and also DSM-5), whilst being relevant, a difficulty arises when strictly applying the criteria. In particular, within the definition of MDD, a continuous depressed mood of more than 2 weeks is one of the criteria for diagnosis, and in reality it is difficult to judge whether this criteria has been met for this continuous period for almost every day for 2 weeks. Furthermore, ambiguity exists regarding the extent at which ‘continuous’ may be defined. In MTD, depressive symptoms are exhibited at work or at school but during weekend rest times or when at home these symptoms are not exhibited. In such cases, are the DSM criteria of ‘for more than 2 weeks’ met? Depending on the psychiatrist, there are those who would diagnose MDD and others who would not. In Japanese clinical settings, for such cases and similar cases where symptoms are even less frequent, there is still a high probability that a diagnosis of MDD will eventuate.
Proposing a novel diagnostic approach to depression
The greatest difficulty in the evaluation and diagnosis of depression is the gap between subjective patient symptoms and objective realities. It is a well-known given among experienced psychiatrists that information garnered from the individual only is not enough in the diagnosis of depression. Information regarding psychiatric symptoms from an individual is no more than ‘subjective symptoms’ and in many cases differs from objective realities. It is particularly difficult for inexperienced psychiatrists to reach a diagnosis for depression based on information garnered solely from the individual but it is also often the case that treatment is commenced without understanding this reality. Moreover, it is important to note that recently not only psychiatrists but also physicians are diagnosing depression and tend to prescribe antidepressants. In order to improve this situation, changes must be made to allow for a more detailed assessment of the individual’s situation. Along with the individual, the collection of information from family members and other third parties is incredibly important (Fig. 2). When an individual claims to be depressed, an objective assessment is required that cannot be limited to the individual. Because of this, when the only obtainable information is from the individual, a diagnosis of ‘possible’ depression may be preferable. This aspect has not been included in many guidelines of depression; however, it must be of great importance, especially in diagnosing MTD.
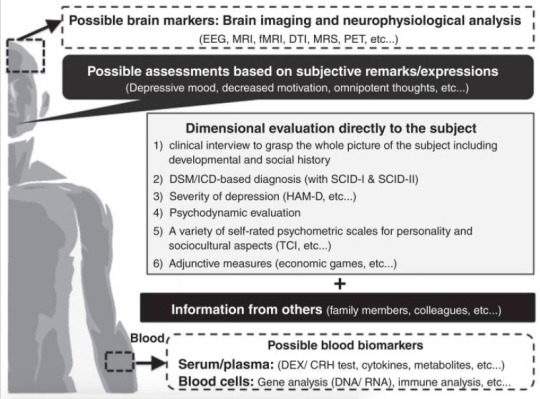
Figure 2. Multi-axial assessments of modern type depression (MTD). In order to evaluate MTD, we recommend utilizing the 1–6 assessment methods directly to depressed persons. In addition, information from others is essential to evaluate such persons. Objective biomarkers of MTD have not been developed until now. Some biomarkers of MTD may overlap with major depressive disorder and other psychiatric diagnosis/syndromes, while some data from brain imaging/neurophysiological analysis and peripheral blood analysis may help to distinguish MTD from other psychiatric conditions. Further investigations should be developed to dig up such biomarkers. CRH, corticotrophin-releasing hormone; DEX, dexamethasone; DTI, diffusion tensor imaging; EEG, electroencephalography; HAM-D, Hamilton Rating Scale for Depression; fMRI, functional magnetic resonance imaging; MRI, magnetic resonance imaging; MRS, magnetic resonance spectroscopy; PET, positron emission tomography; SCID, Structured Clinical Interview for DSM-IV; TCI, Temperament and Character Inventory.
Using a three-tier diagnostic system (possible/probable/definite)
Here, we propose a novel criteria that can make evaluation/diagnosis of depression understandable even for less experienced psychiatrists.76 Along the lines of a diagnostic system for many physical illnesses (cancer, etc ) and dementia, we propose that diagnosis of depression should be divided into the three tiers of ‘possible,’ ‘probable’ and ‘definite.’ The first tier (possible) would be ‘diagnosis based on information from the subject only,’ the second tier (probable) would be ‘diagnosis based on the information from the subject and other sources (family or colleagues, etc.),’ and the third tier (definite) would be ‘diagnosis based on information from the subject + (family, colleagues, etc.) + (intensive clinical examination during outpatient clinic and/or hospitalization).’ Furthermore, we believe that each tier should have a different treatment guideline.77 By utilizing this novel diagnostic system, we can avoid the tendency to overdiagnose depression in persons with MTD tendencies (Fig. 2).
Investigating research into adjunctive measures, such as economic games
In addition, economic games, such as the trust game, have been utilized to evaluate real-world interpersonal relationships as a novel candidate for psychiatric evaluations. Economic games have been developed in the field of social psychology and economics, and have been proposed as a novel tool for evaluating interpersonal psychiatric problems. Clinical studies using economic games (prisoner’s dilemma, the public goods game, the ultimatum game and the trust game) have revealed some difficulties of social decision-making in individuals with MDD and personality disorders.77–80 The trust game, an economic game, has been widely used to evaluate a person’s trust toward others.81 In this two-person game, the first player has to make a risky financial decision depending on how much s/he would trust the second player (partner). Recent studies have examined whether other factors, such as personality and psychiatric conditions, influence trusting behaviors and cooperation.79,80,82–84 As a pilot study, we recently conducted a trust game experiment with 81 Japanese university students.85 Clinical case reports have indicated that people with MTD and hikikomori have difficulties in developing trust among family members, and colleagues in schools and working places.86–88 Therefore, a common feature of modern psychiatric syndromes may be induced through difficulty in trusting others, and these features may not be limited to patients but also to the wider contemporary populations, especially the young. In the economic experiment, participants made a risky financial decision about whether to trust each of 40 photographed partners.85 Participants then answered a set of questionnaires, including the Patient Health Questionnaire (PHQ)-9. Regression analysis revealed that item 8 of the PHQ-9 (subjective agitation and/or retardation) for female participants was associated with participants’ trusting behaviors. Women with higher subjective agitation (and/or retardation) gave less money to men and highly attractive women, but more to less attractive women in interpersonal relationships. This indicates that women with high subjective agitation may tend to make more defensive and cautious decisions in daily life, which may cause difficulties in various social interactions. These data indicate the possible impact of economic games in psychiatric research and clinical practice, including MTD, and further validation should be investigated.
Conclusion
In this review paper, we introduced MTD, citing the few scientific reports available and offered our collective experiences and perspectives on its diagnosis and treatment. In Japan, MTD refers to a syndrome with predominant symptoms of depression and withdrawal that has rapidly increased among youth since around 2000. It is worth recalling that the phenotype of mental illness – be it the appearance of late-19th century hysteria, the appearance of post-1950 eating disorders, or post-1970 borderline personality disorders – is transforming along with society. Despite the lack of agreement upon diagnostic criteria of MTD, it may be considered that cultural, social, and biological factors are all involved in its development and Japanese cultural and social influences may be creating MTD (Fig. 1). In Japan, along with MTD, social withdrawal syndrome (i.e. hikikomori) is concurrently prevalent amongst youth and is considered a great social problem. We hypothesize that the onset of MTD and a prolonged maladaptive social situation may be one of the causal factors of hikikomori. As we may consider ‘withdrawal/avoidance’ to be a common factor in both syndromes, further research regarding shared psychopathology and risk factors in modern society is necessary. We believe that combating MTD may also rescue hikikomori. Differentiation of MTD from other psychiatric disorders has not been established under the present situation, while we have newly classified MTD and related psychiatric disorders (syndromes) from the following two aspects: maturation of personality and ability for social interaction (Fig. 3).
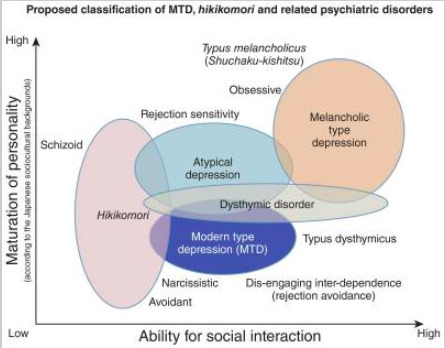
Figure 3. Proposed classification of modern type depression (MTD), hikikomori and related psychiatric disorders. Based on the maturation of personality and ability of social interaction, we have classified the five psychiatric disorders (syndromes), including MTD and hikikomori. The level of personality maturation in this figure is based on the Japanese sociocultural contexts. In Japan, melancholic personality (Typus melancholicus or Shūchaku-kishitsu) has long been regarded as matured personality, while this perspective may not be applied in other countries with different sociocultural backgrounds.
We have suggested the necessity for the introduction of novel methods of evaluation, not only limited to the diagnosis of MTD but to depressive disorders in general, as we consider the modern usage of psychiatric tools that rely on subjective claims by patients to be insufficient. In particular, we recommend the addition of: third-party evaluations to the diagnostic criteria; the usage of economic game experiments and the like; and the evaluation of actual behavioral characteristics. It is hoped that through the introduction of these tools, a more accurate diagnosis of depressive disorders will become possible. The development of a new multi-axial evaluation and diagnostic tool that incorporates such new tools is required (Fig. 2). As the nosology of MTD has not been validated, we need to keep in mind that the presented data shown in the ‘biological factors’ and ‘therapeutic approach’ sections does not directly provide the findings of MTD (mixed with issues regarding major depression in general). In order to advance MTD research, we have proposed research-based draft operational criteria for MTD (Table 2). The draft operational criteria are limited to research use at the present stage. We hope that in the near future, a breakthrough diagnostic and treatment methodology for MTD will be developed based on these draft criteria.
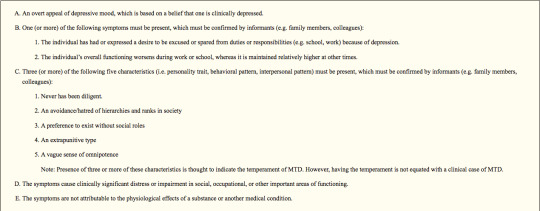
Table 2. Proposed research-based operational criteria and intervention for ‘modern type depression (MTD)’: Provisional –recommended only for research use.
In order to advance MTD research, MTD should be defined with more systematic methodology. Thus, we herein propose operational criteria for MTD based on the present knowledge of MTD. The draft operational criteria are for research use at the present stage. Based on research with the draft criteria, clinically useful operational criteria should be developed in the near future. Of note, five components are listed as representative of MTD in Item C. In order to evaluate the temperament of MTD, the person must be comprehensively assessed, including personality, development, life history and present status. In order to help conduct the assessment more efficiently, a self-report questionnaire (‘MTD-trait scale’) for evaluation of MTD temperament is being developed (Kato et al. unpub. material). HAM-D, Hamilton Rating Scale for Depression; MDD, major depressive disorder; MTD, modern type depression.
References
1. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960; 23:56–62. [PubMed: 14399272]
2. Furukawa TA, Streiner DL, Azuma H, et al. Cross-cultural equivalence in depression assessment: Japan-Europe-North American study. Acta Psychiatr Scand. 2005; 112:279–285. [PubMed: 16156835]
3. American Psychiatric Publishing. Quick Reference to the Diagnostic Criteria from DSM-IV-TR. American Psychiatric Publishing, Inc; Arlington, VA: 2000.
4. Kato TA, Shinfuku N, Fujisawa D, et al. Introducing the concept of modern depression in Japan: An international case vignette survey. J Affect Disord. 2011; 135:66–76. [PubMed: 21782250]
5. Tarumi S, Kanba S. Sociocultural approach toward depression – Dysthymic type depression. Jpn Bull Soc Psychiatr. 2005; 13:129–136. (in Japanese).
6. Tarumi S. The ‘new’ variant of depression: The dysthymic type. Jpn J Clin Psychiatr. 2005; 34:687– 694. (in Japanese).
7. Benazzi F. Testing atypical depression definitions. Int J Methods Psychiatr Res. 2005; 14:82–91. [PubMed: 16175877]
8. Blanco C, Vesga-Lopez O, Stewart JW, Liu SM, Grant BF, Hasin DS. Epidemiology of major depression with atypical features: Results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). J Clin Psychiatry. 2012; 73:224–232. [PubMed: 21939615]
9. Akiskal HS, Akiskal KK, Perugi G, Toni C, Ruffolo G, Tusini G. Bipolar II and anxious reactive ‘comorbidity’: Toward better phenotypic characterization suitable for genotyping. J Affect Disord. 2006; 96:239–247. [PubMed: 16973219]
10. Shimoda M. On the treatment of involutional depression in my department. Taiwan Igaku Zasshi. 1932; 31:113–115. (in Japanese).
11. Tellenbach, H. Melancholie. Springer; Berlin: 1961.
12. Walters, PA, Jr. Student apathy. In: Blame, GB., Jr, McArthur, CC., editors. Emotional problems of the student. Appleton-Century-Crofts; New York: 1961. p. 129-147.
13. Kasahara Y, Kimura B. Utsu-byo no rinshoteki-bunrui ni kansuru kenkyu. Seishin Shinkeigaku Zasshi. 1975; 77:715–735. (in Japanese). [PubMed: 1243687]
14. Hirose, T. Tohi-gata utsu-byo ni tsuite. In: Miyamoto, T., editor. Sou-utsu-byo no seishin-byori 2 [Psychopathology of Manic-Depressive Illness 2]. Kobundo, Tokyo: 1977. p. 61-86.
15. Matsunami K, Yamashita Y. Syakai-hendo to utsu-byo [Social changes and depression]. Jpn Bull Soc Psychiatr. 1991; 14:193–200. (in Japanese).
16. Abe T, Otsuka K, Nagano M, Kato S, Miyamoto T. A consideration on ‘Immature Type of Depression’: Premorbid personalities and clinical pictures of depression from the structural- dynamic viewpoint (W. Janzarik). Jpn Clin Psychopathol. 1995; 16:239–248. (in Japanese).
17. Klein DF, Liebowitz MR. Hysteroid dysphoria. Am J Psychiatry. 1982; 139:1520–1521. [PubMed: 7137409]
18. Kato TA, Shinfuku N, Sartorius N, Kanba S. Are Japan’s hikikomori and depression in young people spreading abroad? Lancet. 2011; 378:1070. [PubMed: 21924990]
19. Shimoda M. Shuchaku-kishitsu ni tsuite. Yonago Igaku Zasshi. 1950; 2:1–2. (in Japanese).
20. Kanba S. Modern interpretation of Shimoda’s shuchaku-kishitsu. Kyushu Neuro-Psychiatry. 2006; 52:79–88. (in Japanese).
21. Ohmae S. The modern concept of atypical depression: Four definitions. Seishin Shinkeigaku Zasshi. 2010; 112:3–22. (in Japanese). [PubMed: 20184236]
22. American Psychiatric Publishing. Diagnostic and Statistical Manual of Mental Disorders. 5. American Psychiatric Publishing; Arlington, VA: 2013.
Psychiatry Clin Neurosci. Author manuscript; available in PMC 2017 August 17.
VA Author Manuscript VA Author Manuscript VA Author Manuscript
Kato et al.
Page 16
23. Akiskal HS. Dysthymic disorder: Psychopathology of proposed chronic depressive subtypes. Am J Psychiatry. 1983; 140:11–20. [PubMed: 6336637]
24. Hirose T. Depression of avoidant type compared with depression of dysthymic type. Jpn J Clin Psychiatr. 2008; 37:1179–1182. (in Japanese).
25. Abe T. Depression from the viewpoint of life stage: Diagnosis and treatment. Jpn J Psychosom Med. 2009; 49:987–993. (in Japanese).
26. Nitobe, I. Bushido: The Soul of Japan. G. P. Putnam’s Sons; New York: 1906.
27. Benedict, RF. The Chrysanthemum and the Sword: Patterns of Japanese Culture. Houghton Mifflin; Boston, MA: 1946.
28. Doi, T. The Anatomy of Dependence. Kodensha International; Tokyo: 1973.
29. Furukawa T, Nakanishi M, Hamanaka T. Typus melancholicus is not the premorbid personality trait of unipolar (endogenous) depression. Psychiatry Clin Neurosci. 1997; 51:197–202. [PubMed: 9316163]
30. Kanba S, Kano R, Eguchi S, Utsumi T, Abe T. Has the prototype of depression been shifted? Jpn J Clin Psychiatr. 2008; 37:1091–1109. (in Japanese).
31. Kotov R, Gamez W, Schmidt F, Watson D. Linking ‘big’ personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychol Bull. 2010; 136:768–821. [PubMed: 20804236]
32. Watson D, Clark LA. Depression and the melancholic temperament. Eur J Pers. 1995; 9:351–366.
33. Klein DN, Shankman SA, Rose S. Ten-year prospective follow-up study of the naturalistic course of dysthymic disorder and double depression. Am J Psychiatry. 2006; 163:872–880. [PubMed: 16648329]
34. Tseng, WS. Handbook of Cultural Psychiatry. Academic Press; San Diego, CA: 2001.
35. Alarcon RD. Culture, cultural factors and psychiatric diagnosis: Review and projections. World Psychiatry. 2009; 8:131–139. [PubMed: 19812742]
36. Ogata Y, Izumi Y, Kitaike T. Mobile-phone e-mail use, social networks, and loneliness among Japanese high school students. Nippon Koshu Eisei Zasshi. 2006; 53:480–492. (in Japanese). [PubMed: 16944832]
37. Watabe, M. Social exchange; transition from ‘embedded long-term relationships’ to ‘voluntary short-term relationships’. In: Hibino, A.Watabe, M., Ishii, K., editors. Disconnected Society (Tsunagarenai Shakai). Nakanishiya, Kyoto: 2014.
38. Hatcher S, Stubbersfield O. Sense of belonging and suicide: A systematic review. Can J Psychiatry. 2013; 58:432–436. [PubMed: 23870726]
39. Kim SY, Kim MH, Kawachi I, Cho Y. Comparative epidemiology of suicide sin South Korea and Japan: Effects of age, gender and suicide methods. Crisis. 2011; 32:5–14. [PubMed: 21371965]
40. Takahashi, K., Kawai, D., Nagata, M., Watabe, M. Fukigen na shokuba [Unpleasant Workplace]. Kodansha, Tokyo: 2008.
41. Kato TA, Tateno M, Shinfuku N, et al. Does the ‘hikikomori’ syndrome of social withdrawal exist outside Japan? A preliminary international investigation. Soc Psychiatry Psychiatr Epidemiol. 2012; 47:1061–1075. [PubMed: 21706238]
42. Niiya Y, Ellsworth PC, Yamaguchi S. Amae in Japan and the United States: An exploration of a ‘culturally unique’ emotion. Emotion. 2006; 6:279–295. [PubMed: 16768560]
43. Teo AR, Stufflebam K, Saha S, et al. Psychopathology associated with social withdrawal: Idiopathic and comorbid presentations. Psychiatry Res. 2015; 228:182–183. [PubMed: 25977071]
44. Teo AR, Fetters MD, Stufflebam K, et al. Identification of the hikikomori syndrome of social withdrawal: Psychosocial features and treatment preferences in four countries. Int J Soc Psychiatry. 2015; 61:64–72. [PubMed: 24869848]
45. Heine, SJ. Cultural Psychology. W. W. Norton & Company; New York: 2011.
46. Yamagishi, T. Trust – The Evolutionary Game of Mind and Society. Springer Tokyo; Tokyo: 2011. 47. Yamagishi T, Cook KS, Watabe M. Uncertainty, trust, and commitment formation in the United
States and Japan. Am J Sociol. 1998; 104:165–194.
48. Cross SE, Hardin EE, Gercek-Swing B. The what, how, why, and where of self-construal. Pers Soc Psychol Rev. 2011; 15:142–179. [PubMed: 20716643]
49. Markus HR, Kitayama S. Culture and the self: Implications for cognition, emotion, and motivation. Psychol Rev. 1991; 98:224–253.
50. Oyserman D, Coon HM, Kemmelmeier M. Rethinking individualism and collectivism: Evaluation of theoretical assumptions and meta-analyses. Psychol Bull. 2002; 128:3–72. [PubMed: 11843547]
51. Matsumoto D. Culture and self: An empirical assessment of Markus and Kitayama’s theory of independent and interdependent self-construals. Asian J Soc Psychol. 1999; 2:289–310.
52. Levine TR, Bresnahan MJ, Park HS, et al. Self-construal scales lack validity. Hum Commun Res. 2003; 29:210–252.
53. Hashimoto, H., Yamagishi, T. Center for the Study of Cultural and Ecological Foundations of the Mind Working Paper Series. Hokkaido University; 2014. Engaging and disengaging aspects of independence and interdependence: An adaptationist perspective.
54. Hashimoto H, Yamagishi T. Two faces of interdependence: Harmony seeking and rejection avoidance. Asian J Soc Psychol. 2013; 16:142–151.
55. Li TM, Wong PW. Youth social withdrawal behavior (hikikomori): A systematic review of qualitative and quantitative studies. Aust N Z J Psychiatry. 2015; 49:595–609. [PubMed: 25861794]
56. Holsboer F. The corticosteroid receptor hypothesis of depression. Neuropsychopharmacology. 2000; 23:477–501. [PubMed: 11027914]
57. Holsboer F, von Bardeleben U, Wiedemann K, Muller OA, Stalla GK. Serial assessment of corticotropin-releasing hormone response after dexamethasone in depression. Implications for pathophysiology of DST nonsuppression. Biol Psychiatry. 1987; 22:228–234. [PubMed: 3028512]
58. Hori H, Teraishi T, Sasayama D, et al. Relationship of temperament and character with cortisol reactivity to the combined dexamethasone/CRH test in depressed outpatients. J Affect Disord. 2013; 147:128–136. [PubMed: 23178186]
59. Hori H, Teraishi T, Ota M, et al. Psychological coping in depressed outpatients: Association with cortisol response to the combined dexamethasone/CRH test. J Affect Disord. 2014; 152–154:441– 447.
60. Hori H, Teraishi T, Ozeki Y, et al. Schizotypal personality in healthy adults is related to blunted cortisol responses to the combined dexamethasone/corticotropin-releasing hormone test. Neuropsychobiology. 2011; 63:232–241. [PubMed: 21494051]
61. Tyrka AR, Wier LM, Price LH, et al. Cortisol and ACTH responses to the Dex/CRH test: Influence of temperament. Horm Behav. 2008; 53:518–525. [PubMed: 18294637]
62. Rinne T, de Kloet ER, Wouters L, Goekoop JG, DeRijk RH, van den Brink W. Hyperresponsiveness of hypothalamic-pituitary-adrenal axis to combined dexamethasone/ corticotropin-releasing hormone challenge in female borderline personality disorder subjects with a history of sustained childhood abuse. Biol Psychiatry. 2002; 52:1102–1112. [PubMed: 12460693]
63. Gold PW, Chrousos GP. The endocrinology of melancholic and atypical depression: Relation to neurocircuitry and somatic consequences. Proc Assoc Am Physicians. 1999; 111:22–34. [PubMed: 9893154]
64. Kunugi H, Hori H, Ogawa S. Biochemical markers subtyping major depressive disorder. Psychiatry Clin Neurosci. 2015; 69:597–608. [PubMed: 25825158]
65. Takeuchi T, Nakao M, Kachi Y, Yano E. Association of metabolic syndrome with atypical features of depression in Japanese people. Psychiatry Clin Neurosci. 2013; 67:532–539. [PubMed: 24152284]
66. Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006; 444:860–867. [PubMed: 17167474]
67. Horikawa H, Kato TA, Mizoguchi Y, et al. Inhibitory effects of SSRIs on IFN-gamma induced microglial activation through the regulation of intracellular calcium. Prog Neuropsychopharmacol Biol Psychiatry. 2010; 34:1306–1316. [PubMed: 20654672]
68. Kato TA, Monji A, Mizoguchi Y, et al. Anti-inflammatory properties of antipsychotics via microglia modulations: Are antipsychotics a ‘fire extinguisher’ in the brain of schizophrenia? Mini Rev Med Chem. 2011; 11:565–574. [PubMed: 21699487]
69. Kato TA, Yamauchi Y, Horikawa H, et al. Neurotransmitters, psychotropic drugs and microglia: Clinical implications for psychiatry. Curr Med Chem. 2013; 20:331–344. [PubMed: 23157624]
70. Mizoguchi Y, Kato TA, Seki Y, et al. Brain-derived neurotrophic factor (BDNF) induces sustained intracellular Ca2+ elevation through the up-regulation of surface transient receptor potential 3 (TRPC3) channels in rodent microglia. J Biol Chem. 2014; 289:18549–18555. [PubMed: 24811179]
71. Monji A, Kato T, Kanba S. Cytokines and schizophrenia: Microglia hypothesis of schizophrenia. Psychiatry Clin Neurosci. 2009; 63:257–265. [PubMed: 19579286]
72. Schulz, K. New York Times. 2004. Did antidepressants depress Japan?.
73. Healy, D. The Antidepressant Era. Harvard University Press; Cambridge, MA: 1997.
74. American Psychiatric Publishing. Diagnostic and Statistical Manual of Mental Disorders. 4. American Psychiatric Publishing; Arlington, VA: 2000. text rev
75. Parker G. Is depression overdiagnosed? Yes. BMJ. 2007; 335:328. [PubMed: 17703040]
76. Hashimoto R, Yasuda Y, Yamamori H, et al. Is it possible to make a diagnosis of major depression based solely on the medical interview of the patient? Seishinka. 2013; 22:243–249.
77. Wang Y, Zhou Y, Li S, Wang P, Wu GW, Liu ZN. Impaired social decision making in patients with major depressive disorder. BMC Psychiatry. 2014; 14:18. [PubMed: 24450703]
78. Zhang HJ, Sun D, Lee TM. Impaired social decision making in patients with major depressive disorder. Brain Behav. 2012; 2:415–423. [PubMed: 22950045]
79. Brendan Clark C, Thorne CB, Hardy S, Cropsey KL. Cooperation and depressive symptoms. J Affect Disord. 2013; 150:1184–1187. [PubMed: 23726777]
80. King-Casas B, Sharp C, Lomax-Bream L, Lohrenz T, Fonagy P, Montague PR. The rupture and repair of cooperation in borderline personality disorder. Science. 2008; 321:806–810. [PubMed: 18687957]
81. Berg J, Dickhaut J, McCabe K. Trust, reciprocity, and social history. Games Econ Behav. 1995; 10:122–142.
82. Chiu PH, Kayali MA, Kishida KT, et al. Self responses along cingulate cortex reveal quantitative neural phenotype for high-functioning autism. Neuron. 2008; 57:463–473. [PubMed: 18255038]
83. Kato TA, Watabe M, Tsuboi S, et al. Minocycline modulates human social decision-making: Possible impact of microglia on personality-oriented social behaviors. PLoS ONE. 2012; 7:e40461. [PubMed: 22808165]
84. Watabe M, Kato TA, Monji A, Horikawa H, Kanba S. Does minocycline, an antibiotic with inhibitory effects on microglial activation, sharpen a sense of trust in social interaction? Psychopharmacology. 2012; 220:551–557. [PubMed: 21956241]
85. Watabe M, Kato TA, Teo AR, et al. Relationship between trusting behaviors and psychometrics associated with social network and depression among young generation: A pilot study. PLoS ONE. 2015; 10:e0120183. [PubMed: 25836972]
86. Nakano M. How supervisors deal with subordinates who have characteristics of ‘new-type depression’. Rinsho-Shinrigaku. 2014; 14:235–243.
87. Tsujii H, Natsuhori K, Uozumi E. Nursing care for an adolescent hikikomori case with domestic violence: A case report. Nihon Seishinka Kangogaku Kaishi. 2010; 52:72–76.
88. Nakagama H. Integration of individual and family conjoint interview: A case study of a social withdrawal adolescent and his family members. Kazoku-Shinrigaku-Kenkyu. 2008; 22:28–41.
#psychiatry#global psychiatry#cross-cultural psychiatry#atypical depression#mental illness#DSM-5#depression#major depressive disorder#shūchaku-kishitsu#diagnosis#diagnostic symptoms#modern type depression#dysthymia#classification#hikikomori
1 note
·
View note
Text
Claywood House Hampshire low-carbon home
Claywood House, Hampshire low-carbon home, English Luxury Property, Architecture, ACG Building Images
Claywood House Hampshire low-carbon property
19 January 2022
Architects: Ayre Chamberlain Gaunt (ACG)
Location: Hampshire, South of England, UK
Photos below by Andy Matthews
Claywood House in Hampshire
Claywood House, a new 5-bedroom low-carbon home has been designed to meet the needs of a wheelchair dependant client and to create spaces that allow her to live independently. The new building is located within the orchard of the client’s previous home – a multi levelled building unsuitable for conversion (but retained and sold). The house is designed as a counterpoint to the original and with an architecture of contrast reflecting a ‘fresh start’ for the client and her family.
The design celebrates the beautiful setting and builds into the landscape itself. The shape of the building responds to the complex geometry of the topography and the site boundary and works with the slope of the site to reduce the visual impact to the surrounding area. The house is cut away to direct views across the garden and away from the former home, creating sheltered living spaces and establishing a clear entrance. A privately accessed guest annex is located to the south of the site.
Drawing inspiration from the nearby historic brickworks and clay pits, the earth bound ‘plinth’ is formed from a pale coloured, long-format brick. Chamfers and deep reveals express the depth and solidity of the ground floor, which contains the main living spaces, garage and pool area.
A ‘lightweight’ slatted timber-clad form supported on the ‘heavy’ brick plinth, contains the bedrooms areas and annex. This element emerges from the trees with gaps that open in the slatted timber to reveal windows on the east and west façades. The timber slats are arranged in a rhythmic pattern designed to mimic the vertical trunks of the trees in the woodland opposite.
Spaces have been designed to offer moments of delight for the whole family. Inclusive design features include specifically placed floor to ceiling and low windows which allow views into the gardens whether standing or seated. Wide corridors upstairs mean casual passing is easy, while recesses give ample room for extra wide turning circles and a place to rest and enjoy the morning sun.
Flush thresholds blur the boundaries between inside and outside space, at the same time allowing for easy wheelchair access into the landscaped garden. Extra-large garage and generous storage areas keep wheelchairs easily accessed and tucked away. The new building is fully accessible with a lift and provides facilities for the specialist care required by the client including a physiotherapy pool, gym and carer’s suite.
The house incorporates a ground source heat pump, a 12kw Photovoltaic array and a mechanical heat recovery ventilation system. Further, the building envelope is extremely well insulated and airtight thereby creating a highly sustainable new building.
Photos below by Jim Stephenson
Claywood House Hampshire – building Information
Location: Hampshire, southern England, United Kingdom
Type of property: Contemporary self-build
Bedrooms: 5
Project started: March 2017
Project finished: October 2020
Size of house: 750 sqm
PROJECT TEAM:
Architect: Ayre Chamberlain Gaunt (acgarchitects.co.uk)
Structural Engineers: Eckersley O’Callaghan (eocengineers.com)
Contractor: R Durtnell & Sons until their demise in July 2019. Then client managed with site manager Larry Martin.
Sustainability & MEP: Mesh (www.mesh-engergu.com)
STRUCTURE:
Steel works: Clarke Construction Essex (ccel.org.uk)
Groundworks: MTD Formwork (mtdformwork.co.uk)
Brickwork: Randers Tegal Ultima from Taylor Maxwell
Energy services: Mesh Energy (mesh-energy.com)
Swimming Pool: Pools by Design (poolsbydesign.co.uk)
Ground Source Heat Pump: WDS Green energy (wdsgreenenergy.co.uk)
Solar PV panels: Spirit Energy (spiritenergy.co.uk)
Final surfaces: Georgian Complete Finishings (gcfinishings.co.uk)
Plumbing: Tugwell Heating Co (tugwellheating.co.uk)
Electrics: TMS Electrical Contractors (tmselectrical.com)
Windows: IQ Glass (iqglassuk.com)
Garden Design & Build: Catherine MacDonald and Landform Consultants (landformconsultants.co.uk)
Driveway tarmac & bonded resin: L.A.Kattenhorn & Partners (kattenhornsurfacing.co.uk)
Gates: Penchards (penchardsuk.com)
Garage doors: Deuren (deuren.co.uk)
Door automation: Dormakaba (dormakabagroup.com)
FIXTURES & FITTINGS:
Accessible kitchen design: Adam Thomas Consultancy (adamthomasconsultancy.com)
Kitchen build: Myers Touch (themyerstouch.co.uk)
Bathrooms: Motionspot (motionspot.co.uk)
Lift: Aritco (aritco.com); installed by Platinum Lifts (platinumlifts.co.uk)
Stoves: Focus Stoves (focusstoves.co.uk)
Tiles: Minoli (minoli.co.uk)
FURNITURE & ACCESSORIES:
Living room rug & hall wall hanging: Helen Yardley (helenyardley.com)
Dining table: &Bespoke (01264 783103)
Sofas: Hitch Mylius (hitchmylius.co.uk)
Photographers: Andy Matthews and Jim Stephenson
Claywood House Hampshire low-carbon home images / information received 190122 from Architects Ayre Chamberlain Gaunt (ACG)
Location: Hampshire, southern England UK
Hampshire Houses
Contemporary Hampshire Houses – recent property selection
The Pines, Beaulieu Estate, The New Forest National Park
Design: AR Design Studio, Architects
visual : Nu.Ma
The Pines House in New Forest National Park
The Orchard House, Wickham Conservation Area, Winchester
Design: AR Design Studio, Architects
photographer : Martin Gardners
The Orchard House
Holly Cottage Extension, Meonstoke, South Downs National Park
Design: Studio B.A.D Architects
image courtesy of architects practice
Meonstoke House
Mayfly Cottage
Architects: Stiff + Trevillion
photography © Kilian O’Sullivan
Cottage in Hampshire
The Well House in Shawford, Winchester
Architects: AR Design Studio
image courtesy of AR Design Studio
New Property in Shawford, Winchester
The Elements House
Architects: AR Design Studio
photo © Martin Gardner
The Elements House
Downley House, Petersfield, south west Hampshire
Design: Birds Portchmouth Russum Architects
photo : Nick Kane
New House in south west Hampshire
House in Brockenhurst
New House in Winchester
Hampshire Buildings
Hampshire Architecture Designs
Hampshire Buildings
West Downs Centre, University of Winchester
Architect: Design Engine Architects
photo : Jim Stephenson
University of Winchester West Downs Building
Bedales School Art and Design Building, Steep, Petersfield
Design: Feilden Clegg Bradley Studios
photograph © Hufton+Crow
Art and Design Building, Bedales School
Comments / photos for the Claywood House Hampshire low-carbon home design by Ayre Chamberlain Gaunt Architects (ACG) page welcome
The post Claywood House Hampshire low-carbon home appeared first on e-architect.
0 notes
Note
🗝 Give me a reverse AU scenario for lesmand!
✏️If you could change one thing from canon, what would it be and why?
🗝 Give me a reverse AU scenario for lesmand!
I had to percolate on this one for a bit! Okay, imagine a newborn vampire Armand meeting three hundred year old, charismatic cult leader Lestat. 🫢 Ngl, I think cult!Lestat would have been far more successful at drawing Armand into his dark little netherworld than canon Armand was with Lestat in TVL.
I just wonder how deep we go with this one in the reverse AU? Do we swap their makers as well? Their entire backgrounds? I think it would take a lot for Lestat to be broken down enough to where he would believe he had no other option. So I think we'd have to go all the way back and put him through the same or equivalent trauma Armand went through in TVA. This would require some hybrid of TotBT-Lestat, IWTV-Lestat, and a third worse thing I have not yet conceived of.
They would hook up almost immediately though. Armand wouldn't have had to wait 200+ years just to get the tip. 😔
✏️If you could change one thing from canon, what would it be and why?
Buddy, I've been in a state ever since remembering that there could've been a world where David died in MtD and Armand lived. So that. I want Armand and Lestat walking together in Central Park! I want another book from Armand's point of view! Although, I don't know if we would have gotten a TVA if Anne had gone this route with MtD. 🫠
BUT YEAH.
16 notes
·
View notes
Text
Global Commercial Lawn Mower Market Research 2020 - Industry Scenario, Strategies, Growth Factors and Forecast 2030 || Deere and Company, Honda Motor Company, Husqvarna Group
The Global Commercial Lawn Mower market analysis is intended to provide all participants and vendors with pertinent specifics about growth factors, risks, and lucrative business opportunities that the market is expected to reveal in the upcoming years. This intelligence study also contains the revenue share, market size, market potential, and rate of consumption to draw insights pertaining to the rivalry to gain control of a large part of the market share. The Commercial Lawn Mower industry is extremely competitive and consolidated because of the existence of several designated companies that are adopting different marketing strategies to grow their market share. The vendors hired in the sector are outlined found on their geographic reach, financial performance, strategic moves, and product portfolio. The vendors are slowly enlarging their strategic actions, along with customer interaction.
The primary objective of the Commercial Lawn Mower market is to assemble vital data about product definition, applications, classification, industry chain structure. Furthermore, the Commercial Lawn Mower report targets the company’s elementary data including product picture, considerable market share, company profiles, specifications, and contact details.
To Know more Market Challenges and Industry Growth analysis on Commercial Lawn Mower - Get Free Sample Here https://market.us/report/commercial-lawn-mower-market/request-sample
In addition, the report presents quantitative as well as the qualitative narration of the global Commercial Lawn Mower market. The research report is beneficial for researchers, strategy managers, academic institutions, and analysts. Thus report helps all types of users to determine the strategic enterprises so that they can understand how to expand the global Commercial Lawn Mower market business across the globe for product development. Moreover, the research report provides an in-depth analysis of all the segments that can impact market growth. The Commercial Lawn Mower segment is slated to expand as the fastest-growing segment. The commercial and industrial segment is slated to expand as the fastest-growing segment.
The Enterprise seems to be evenly competitive to examine any market with clarity the market is divided into segments, such as its product type, application, technology, end-use industry, etc. Segmenting the market into smaller segments makes it easier in understanding the dynamics of the market with more clearness. Data is displayed with the help of tables and figures that consist of a visual representation of the numbers in the form of histograms, bar graphs, pie charts, etc. Another key component that is integrated with the report is the regional analysis to assess the global presence of the Commercial Lawn Mower market.
Main Market Perceptions Consist of The Following:
1. The survey of Commercial Lawn Mower delivers market size and growth rate for the forecast period 2021-2030.
2. It presents detailed understandings of ongoing industry movements, trend forecasts, and growth drivers.
3. It offers a separate review of market sectors and the local perspective.
The important applications and probable business areas are also specified in this report.
Get more insights about the Global Commercial Lawn Mower Market - Click Here for More Inquiry https://market.us/report/commercial-lawn-mower-market/#inquiry
Top Leading Key Players:
Deere and Company Honda Motor Company Husqvarna Group Kubota Toro MTD Products Ariens Company Bobcat BOSCH Group Briggs and Stratton Hustler Turf Equipment Scag Power Equipment Swisher Acquisition Inc.
Commercial Lawn Mower report is segmented into types, key geographical regions, and applications. The major key vendors, types, applications, and regions of the Commercial Lawn Mower market are given in below.
By Types:
Battery powered Electric Gas Powered
By Applications:
Online Offline

By Regions:
North America (The US, Canada, and Mexico)
Europe (France, Germany, the UK, and Rest of the World)
Asia Pacific (Japan, China, India, and Rest of Asia Pacific)
Latin America (Brazil and Latin America)
Middle East & Africa (Saudi Arabia, the UAE, South Africa, and Rest of the Middle East & Africa)
Years Considered to Estimate the Market Size:
History Year: 2012-2019
Base Year: 2020
Estimated Year: 2021
Forecast Year: 2021-2030
Important highlights of this Commercial Lawn Mower market report:
1. COVID-19 impact on the revenue Streams of the Commercial Lawn Mower market players.
2. Statistics of the total sales amount And general market returns.
3. Enterprise trends types of research.
4. The estimated growth rate of the Commercial Lawn Mower Market.
5. Pros and cons of the direct and indirect sales media.
6. In-depth information about the major Distributors, traders, and traders.
Reasons you should buy this report:
1. The Commercial Lawn Mower market is keeping a track of the market since 2012 and has added the necessary historical data & analysis in the research report.
2. It also offers a complete assessment of the common behavior about the coming market and changing market system.
3. This report delivers several strategic business processes to support you in making those determinations.
4. Industry professionals and research judges have worked much to prepare the research report which will help you to give that additional edge in the competitive market.
5. The market research report can be customized according to your requirements. This means that The Commercial Lawn Mower market can cover a particular product, application, or a company can provide a detailed analysis in the report. You can also buy a different report for a specific area.
Get Link for Purchase Report @ https://market.us/purchase-report/?report_id=39528
TOC (Table of Content)
1. Market Overview.
1.1 Commercial Lawn Mower Analysis
1.2 Market Objective
1.3 Primary Summary
2. Commercial Lawn Mower Sample Reports.
2.1 Statistics
2.2 Market estimates
3. Commercial Lawn Mower Market Perceptions
3.1 Survey of Commercial Lawn Mower
3.2 Ongoing industry movements
4. Commercial Lawn Mower Key Players
5. Types
6. Applications
7. Regions
8. Market Size
9. Important Highlights of Commercial Lawn Mower
9.1 Reports Guidelines and policies
10. Reasons you should buy Commercial Lawn Mower Report
10.1 Necessary historical data
10.2 Strategic business methodologies
10.3 Detailed analysis of the report
CONTACT US :
Mr. Benni Johnson
Market.us (Powered By Prudour Pvt. Ltd.)
Email: [email protected]
Address:
420 Lexington Avenue,
Suite 300 New York City,
NY 10170, United States,
Tel: +1 718 618 4351
Website: https://market.us
0 notes
Last Seen Blogs

daily--cats
♡ What greater gift than the love of a cat ♡

veiligheidsglaslatenplaatsen
Vincent Hendriks

heavenly-sights
Untitled
notsaltyaesthetic
notsaltyaesthetic

wanderstarr
most sane puppet enjoyer (debatable)