#affirm or suicide
Text
By: Mary Harrington
Published: Feb 19, 2024
A new study challenges the common assertion that gender-dysphoric youth are at elevated risk of suicide if not treated with “gender affirming” medical interventions. If it’s true, it ought to have a seismic impact on the accepted medical approach to gender-confused youth.
Reported in the BMJ, the study examines data on a Finnish cohort of gender-referred adolescents between 1996 and 2019, and compares their rates of all-cause and suicide mortality against a control group. While suicide rates in the gender-referred group studied were higher than in the control group, the difference was not large: 0.3% versus 0.1%. And — importantly — this difference disappeared when the two groups were controlled for mental health issues severe enough to require specialist psychiatric help.
In other words: while transgender identity does seem to be associated with elevated suicide risk, the link is not very strong. What’s more, the causality may not work the way activists claim.
The association between gender dysphoria and mental illness is well-documented by both providers of “gender-affirming care” and trans advocacy groups and clinical psychology research. But one less well-evidenced claim, based on this association, is that these difficulties are caused not by being transgender, but by the political and social stigma associated with it. Gender dysphoria, we are to understand, is not in itself a mental health issue. What causes mental health issues in transgender youth — up to and including suicide — is the wider world’s rejection of their identity, and of the metaphysical frame of “gender identity” as such.
This is the root of the oft-repeated social media assertion that anyone who demurs about trans identity, however mildly, is complicit in “trans genocide”. The same assertion that invalidating trans youth makes them kill themselves is also behind the rhetorical question routinely used to browbeat parents into consenting to social and medical transition for their gender-confused offspring: “Would you rather have a live daughter or a dead son?”
It’s behind the prohibition on “trans conversion therapy” already in force in several countries, and promised by the Labour Party in England too. Such measures forbid therapists from exploring with their clients whether there is any link between their gender dysphoria and — for example — life trauma or other mental health issues. For logically, if the cause of distress and suicidality in trans people is not being accepted for who they are, any therapist who seeks to explore links between gender dysphoria and other biographic or psychiatric issues is complicit in just this kind of non-acceptance, and is thus not helping but harming their client.
But as the study puts it: “Clinical gender dysphoria does not appear to be predictive of all-cause nor suicide mortality when psychiatric treatment history is accounted for.” Rather, what predicts risk in this population is “psychiatric morbidity”. And contra the activists, transitioning does nothing to reduce it: “medical gender reassignment does not have an impact on suicide risk.”
Every suicide is a tragedy, and leaves grieving loved ones behind. No one wants to be complicit in pushing a young person down that path. So the suggestion that questioning someone’s gender beliefs may have this effect serves as a powerful emotional cudgel. But if the Finnish study is correct, this whole rhetorical, legislative, and medical edifice may be built on sand. If the elevated risk of suicidality in trans youth disappears when you control for other psychiatric difficulties, this suggests strongly that trans youth are not more at risk due to transphobia or invalidation, but due to the well-documented fact that gender dysphoria tends to occur in people who are disturbed and unhappy more generally.
It ought to follow from this that the way to manage suicide risk in trans-identified young people is not to affirm their gender identity and whisk them off for medical interventions, but to watch for and treat psychiatric comorbidities. Ultimately, though, the claims of gender ideology are less scientific than metaphysical. So don’t expect scientific evidence that contradicts its prescriptions to have much impact on trans advocates. Even if “following the science” would make a real difference to suicide risk in gender-dysphoric youth.
==
History will view "gender affirming care" advocates the same way we view lobotomy advocates.
#Mary Harrington#affirm or suicide#suicide narrative#trans or suicide#suicide#gender affirming care#gender affirming healthcare#gender affirmation#affirmation model#medical corruption#medical scandal#medical malpractice#gender lobotomy#pseudoscience#medical experimentation#religion is a mental illness
197 notes
·
View notes
Text
A new landmark study has found that access to gender-affirming healthcare significantly reduces rates of depression, gender dysphoria, and suicidality among transgender people.
While it’s no secret that providing gender-affirming care to transgender individuals who ask for it can greatly benefit their well-being, an increase in transphobic rhetoric and bans on gender-affirming healthcare has prompted thorough medical studies into the impact of such care.
Now, brand new research conducted in Melbourne, Australia, has found that allowing transgender people to access the care they’re after can reduce suicidality by a stunning 55%.
As part of the first-ever randomized controlled trial (RCT) on gender-affirming care, researchers took 64 transgender and gender-diverse adults who had been looking to start testosterone therapy and randomly split them into a treatment group and a control group.
While the treatment group was allowed to begin hormone therapy that week, the control group waited three months for their treatment to begin.
Before the study began, both groups were evaluated on depression, gender dysphoria, and suicidality. Three months later, the two groups were evaluated again.
RCTs for medical care can often be hard to conduct due to practical and ethical concerns. However, researchers of this study found a way to hold an RCT for this study by incorporating a shorter follow-up period. Rather than giving the control group a placebo drug, or no treatment at all, they were simply given a longer wait time.
The results showed a notable decrease in gender dysphoria, depression, and – most significantly – suicidality.
The group that received gender-affirming care right away saw a 55% reduction in suicidality compared to a 5% drop within the control group.
Depression scores in the treatment group decreased by half, while gender dysphoria rates also significantly decreased.
Breaking down their findings, researchers Brendan J. Nolan MBBS, Sav Zwickl, PhD, and Peter Locke wrote: “There was a statistically significant decrease in gender dysphoria in individuals with immediate [access to gender-affirming care] compared with delayed initiation of testosterone therapy.”
“A clinically significant decrease in depression and a decrease in suicidality also occurred with immediate testosterone therapy.”
“The findings of this trial suggest that testosterone therapy significantly decreases gender dysphoria, depression, and suicidality in transgender and gender-diverse individuals desiring testosterone therapy.”

Of course, this isn’t the first time that research has shown significant drops in depression and suicide rates among transgender individuals who receive gender-affirming care.
A 2022 medical study showed that young transgender people who have access to puberty blockers are 73% less at risk of suicide and report improved well-being.
But, as anti-trans activists advocate for further bans on gender-affirming care, one of the key arguments is that the evidence in support of the care isn’t up to scratch with GRADE (Grades of Recommendation, Assessment, Development, and Evaluation) standards.
So research like this landmark RCT is so significant to the transgender community and its allies as the fight for their healthcare rights rumbles on.
#us politics#news#pinknews#2023#gender affirming care#gender affirming healthcare#transgender healthcare#transgender#trans rights#trans healthcare#suicidality#depression#gender dysphoria#Australia#randomized controlled trial#trust the science#Brendan J. Nolan#Sav Zwickl#Peter Locke#testosterone therapy#Grades of Recommendation Assessment Development and Evaluation#lgbtqia+#lgbtqia+ rights
449 notes
·
View notes







Text
It is absolutely wild to me how Republican news outlets and politicians try to sensationalize things that don't even exist. Yet these fabricated issues are having serious disastrous effects on real-life people's health and safety. B was just talking to one of his old "friends" and he was trying to convince us to donate to the campaign of a governor whose platform rests primarily on anti-trans legislation. And B was like...no?? Are you aware of his platform? And this guy says, with absolute confidence, that this governor's platform is about protecting kids. Because it's ok if an adult wants to mutilate their body, but we shouldn't be allowing doctors to surgically change children's bodies. Which is why gender-affirming care should be illegal.
The mental gymnastics. Except he genuinely thought that "gender-affirming care" was synonymous with "surgical intervention." Gender-affirming care for a 10-year-old is therapy and support and letting them wear the clothes and use the pronouns/name they want. Gender-affirming care for a teenager might also include blockers and/or hormone therapy (or not! I've only known one person who started hormones before they turned 18, and I specifically worked with queer kids when I was a professor/teacher). For some people, gender-affirming care is solely external and doesn't involve physical intervention at all. And it is so, extremely, rare for someone to receive surgery as part of gender-affirming care when they are a minor. Yet this is what so many people seem to think gender-affirming care means. Surgery.
This is not an accident. This is targeted and malicious. This is misdirection by people who know better trying to sway the opinions of people who don't. Listen. I don't know what my point is, here. I just needed to vent. I guess it just goes to show that, now more than ever, if you're going to get into a debate with someone, make sure you understand what they mean when they use certain terminology or you're certain to get nowhere. Because this man was so confident he knew what he was talking about until we did a quick vocabulary backtrack. And when confronted with the fact that maybe he hadn't, actually, been fed the truth, he suddenly had a lot less to say. Ugh.
#gender-affirming care#doug burgum#lgbtq#trans rights are human rights#gender-affirming care is suicide prevention#us politics
396 notes
·
View notes
Text
Here's to those who have had self-inflicted trauma.
Many, many traumatized individuals end up feeling like they are partly or completely to blame for their trauma. Regardless of reason, you are not responsible. Even if it was something you did to yourself or others, I firmly believe you were a victim of circumstance; genetic factors, predisposition, lack of knowing it was dangerous, adult influence, etc... there were things out of your control. So, today? We're here to appreciate you.
Shoutout to those who:
Went through SA, CSA, COCSA, and/or NCCSA
Were forced to do traumatizing acts to another child/person
Had/have an eating disorder
Had/have an addiction, even the "mild" or "uncommon" ones
Experienced self-harm or suicide attempts
Otherwise had a near-death experience
Were hospitalized for their mental health
And anyone else who just feels like it's their fault. Because I promise, it isn't.
It's going to be ok. I know how hard things can get. I've had my own run-ins with crises before, but... the important thing is that you're here. You have so, so much value and brightness inside you. I don't want you to think you have to take drastic measures to feel better. Because, you didn't get to write the beginning of your story... but you can definitely write the rest. And I'm excited to see how it turns out.
Please stick around, ok?
🖤💜💙💚💛
#tw csa#tw cocsa#tw nccsa#tw hospitalization#tw suicide mention#tw suicide#tw sh#tw self harm#tw ed#tw eating disorder#tw addiction#multiplicity#plural#pluralgang#plural affirmations#actually multiple#actually plural#did#requests#did osdd
57 notes
·
View notes
Text
What makes me lose my mind a bit about Season 2 Kendall is that like— Logan is trying to fully break his will and control him, and Kendall is trying to break his own will in a lot of ways through guilt and self-destructive behaviours, but there’s this tiny stubborn part of him, this desire for self-preservation, that they can’t kill no matter how hard they try. There’s this little instinctual, human voice inside him saying no, I want to live, I want to fight back, I don’t want to be his puppet, I don’t want to drown. Like initially he wants to save Vaulter, and oppose Logan on buying Pierce. Each time he goes up to the roof in “Safe Room”, he comes back down. He confronts Logan when Logan’s getting too cozy with Rhea in “Return”. He seeks out some form of happiness with Naomi (obviously that is self-destructive too given that he knows her presence will enable his drug abuse, but he also does seek connection and joy out of their relationship). But every time this desire to care about himself and fight back rears its head, either he or Logan smothers it. He submits to Logan’s orders regarding Vaulter (“because my dad told me to”) and Pierce. He goes back up onto the roof multiple times. After the confrontation about Rhea, Logan takes him to the waiter’s house, reminding him of his guilt and powerlessness. Seeing that Kendall finds escape in his relationship with Naomi, Logan sends her off the yacht.
So when Logan tells Kendall he is going to be sacrificed in “This Is Not for Tears”, Kendall has reached a point where he obeys without a single protest. “I deserve it. Maybe I deserve it”. But — crucially — Logan disagrees, saying that Kendall has nothing to be guilty about regarding the waiter’s death. Logan’s lines here are really important, because (in my interpretation??) they ignite Kendall’s repressed urge to fight back that has been slowly eroded this entire season, which leads to his decision at the end of the episode. If Logan had responded “yes, you do deserve it”, then Kendall would have walked to his own destruction willingly, giving up, maybe even feeling a sense of righteousness that he was being punished. But Logan doesn’t say that. Instead, he says: “Nah, nah. Not that. NRPI. You’re the best. Don’t beat yourself up. No real person involved. You know, it’s… it’s nothing.“ It’s nothing.
I think Kendall has a realization in this moment which is very similar to the one Rhea has in “DC”, when she says to Logan, “I can’t see the bottom of the pool. I don’t know if you care about anything. And that scares me”. Kendall’s conscience has been eating him up from the inside — but Logan doesn’t have it. He just doesn’t care. The waiter’s death has been weighing on Kendall as the basis for his self-destructiveness (and submission to Logan’s control), but Logan dismisses it so flippantly, almost as if it is irrelevant, since the moral value of that event is currently not related to his own self-interest in using Kendall as a tool. Which is all this ever was. To Logan, it was never about the waiter. It was never some form of “deserved” punishment. It was always just a part of Logan’s game, convenient to him, serving his aims.
So that tiny stubborn part of Kendall comes to life a bit inside him. It says no, no I don’t want to lie down and let you do this to me. I’m not sure he listens to it right away. But it’s there, and it grows bit by bit. No I want to live, no I want to escape, no I want to fight back, no my father is a malignant presence, a bully, and a liar, and this is the day his reign ends
#and obv this is all just my personal interpretation since logan and Kendall’s decision making is soooo subjective —#what is their reasoning??#and at what point/based on what do they make those choices??#u could look at it a million ways…#stopping myself from writing ‘in my opinion’ before every sentence of this post was a harrowing experience#anyway#i am very normal about kendall roy daily affirmation#i watched 2x10 recently and. yeah ughghmm it was immensely distressing#logan roy#kendall roy#succession season 2#succession 2x10#succession#ruby (unfortunately) watches succession#suicidal thoughts tw#addiction tw
174 notes
·
View notes
Text
say it with me people
trans kids deserve to live, gender affirming health care saves lives, leave us trans people alone you dickwads, queer education is suicide prevention
#delusion speaks#transgender#trans#queer#canada#queer education is suicide prevention#can you tell i'm angry?#because i'm fucking furious#gender affirming healthcare#saves lives#leave trans people alone#lgbtq+#lgbtq community#lgbtqia#lgbtq#lgbtqplus#trans rights are human rights#trans kids deserve to get to adulthood#don't mind me i'm crying
40 notes
·
View notes
Text
me, myself and I have the control, i can do whatever i want and i wont fail.
#coquette moodboard#lana del rey#coquette#ultraviolence#vintage coquette#born to die#doellette#vintage americana#messy moodboard#sylvia plath#loa affirmations#manifesting#manifesation#that girl#it girl#dollette#my year of rest and relaxation#the bell jar#virgin suicides#lux lisbon#fashion#american psycho#marie antoinette#lizzy grant#femcel#female rage#female histeria#female hysteria#black swan#natalie portman
58 notes
·
View notes
Text
CHICAS I MADE A SUBLIMINAL THE OTHER DAY AND IT LITERALLY WORKS
I JUST FOUND CASH ON THE FLOOR ON MY WAY TO THE METRO
(shameless promo)😘👇
youtube
#girlblogging#i’m just a girl#lana del rey#real#girl blogger#slay#relatable#fiona apple#lizzy grant#taylor swift#sofia coppola#the virgin suicides#lux lisbon#kirsten dunst#this is what makes us girls#this is a girlblog#hell is a teenage girl#locally hated#girl interrupted syndrome#girlhood is a spectrum#subliminals#affirmations#90s model#adriana lima#money subliminal#model subliminal#coquette#dollette#vintage americana#Youtube
9 notes
·
View notes
Text
Having Cheese, who's such a kind and patient character, admit that he's angry at Daniel for committing suicide was such a shocking and powerful moment.
#everyone dealt with their grief differently. and throughout the show I think we're supposed to assume Cheese made peace with it#He was always putting everyone before himself and always talked highly of Daniel#and for him to say that he was angry because of Daniel's death is something I think a lot of people will find affirming#anger is such an overlooked stage of mourning#and to show that someone can be kind and patient and loving while also dealing with those ugly emotions is so so so important#reservation dogs#suicide mention#death mention
167 notes
·
View notes
Text
"i'm feeling supersonic / give me gin and tonic" has done damage to my psyche but i think it's reparable
#i'll be like well i'm feeling supersonic i think there's no reason not to have a bit of gin and tonic!!! pass me the bottle#honestly i never was the life-affirming type.#so i might as well blame it on someone else that i act like this + don't fantasize about suicide. it's not like me#kata.txt
7 notes
·
View notes
Text
By: Prisha Mosley
Published: Apr 4, 2023
The transgender community of today is built upon its cult-like tactics of brainwashing, information control, and deception. It has grown so big because of these lies and the control they can take over young minds, and the minds of the mentally ill.
I hope that by discussing some of these lies I can shed light upon them and allow people to see more truth and a different narrative than what is being pushed by the media and transgender community.
1. Transition or Suicide
“Would you rather have a dead daughter or a living son?” This is what my WPATH certified therapist asked my parents in front of me on my very first appointment. This is the narrative among doctors and the community. However, research has shown that rates of suicide actually increase in transgender patients after they receive treatment. Nonetheless, the idea that if anyone, particularly a child, does not receive “gender-affirming care” they will kill themselves.
This is a myth. A lie. No one will die if they are denied access to experimental, mutilating, sterilizing surgeries and drugs.
We can rebut this argument with simple facts. If transgender people have always existed, which is another narrative the trans community pushes, then there would have been droves of child and teenage suicides throughout history we would be able to look back at and refer to. These children would be killing themselves because they didn't have access to “gender affirming care, because it did not exist.” But this did not happen. This is a brand new medicine, which people have never wanted or needed before now, because it was never accessible before.
Transition is not a cure for suicidality, anyway. It won't make suicidal thoughts or ideation go away. In fact, as mentioned above, suicide rates actually increase after transition.
Suicide is a multifaceted issue, and multiple factors are required for a completed suicide. There is no such thing as “trans children not given hormones will kill themselves.” “Misgendering” someone will not cause them to kill themselves. Suicide requires four things, including hopelessness and a lack of support, and will not happen without all four factors being present.
Sources are below.
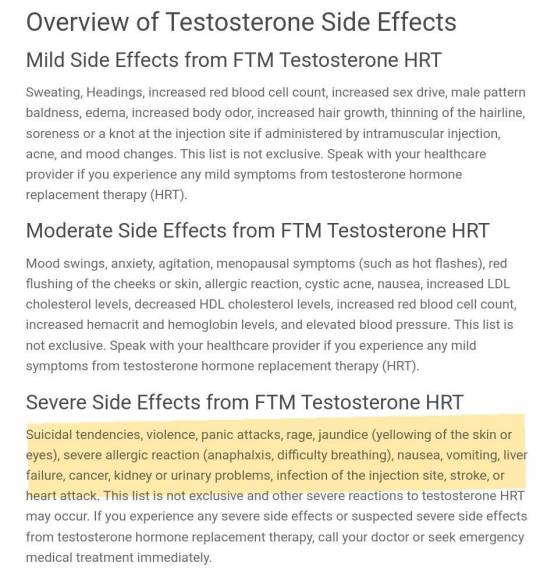
Finally, the effects of hormones, especially testosterone, can increase suicidality just like completing surgery does.
2. Trans Genocide
Another common with being pushed is that a transgender genocide is going on right now. This is also false.
Claiming that there is a genocide happening when there is none is incredibly disrespectful to people's who are victims of genocide.
Genocide is defined as the purposeful killing of a large group of people with the purpose of erasing that group or people.
No one is going out in droves killing transgender people, at least not in Western society where the ideology is being pushed.
Being denied access to women's spaces will not kill any trans-identifying male. The same goes for their sports. Hearing your birth name will not kill a person either.
I have also heard claims that the laws being rolled out to protect children are genocidal, and will cause people to kill themselves, a part of the genocide… This is also false, and as mentioned above, the CDC made a statement about the four factors required for suicide. None of them included “anti-trans bills.”
3. It's Reversible
This is one of the biggest lies they tell, most commonly to naïve, impressionable children. Trans-influencers even make videos saying that you can just go on “T” (testosterone) for a little while and essentially pick and choose which side effects you would like to experience. This is false. Testosterone effects everyone, and every woman, differently. You don't know what side effects will come first, you don't know what will happen when you stop, and there is no way to know until it happens. At that point, the effects are irreversible and unchangeable.
This goes the same for estrogen abuse in males. The effects, such as atrophy, and the growth of male breasts, will not go away. They are irreversible side effects, and they are life-lasting.
When I am testifying on bills, I often hear that puberty blockers are reversible, too. This is another lie for more reasons than one. Puberty blockers have not been studied for their use in completely ending puberty in a young person. Their use has only been studied for things like cancer, sterilizing pedophiles, and use in children with precocious puberty. In the case of precocious puberty, they are used for a very short period of time, and are not meant to completely stop puberty, but rather simply delay it so it can be experienced at a normal time.
Everything that is meant to develop and change during puberty will stop when puberty blockers are in use, and time is not reversible. You will never get back the time you lost when you were supposed to be growing your bone density, and developing your brain. And there is no information about what happens mentally to a child who is on puberty blockers, and if there is irreversible damage to mental health and the development of the personality.
Surgery, of course, is irreversible. There is no going back once you have lost body parts, or put in fake implants, or destroyed your sexual organs.
Reconstruction is almost impossible, will not be covered by insurance, and cost tens of thousands of dollars. It is also difficult to have follow-up surgeries after such mutilating procedures. It is traumatic on the body, and mentally and emotionally as well.
For myself, breast reconstruction will consist of at least three surgeries, and I may lose my nipples altogether. They have to be grafted once again, and are not extremely likely to survive the procedure.
First, I have to endure a tissue expander. An implant-like bag will be placed in my chest, and I will have to go to the surgeon every week for a period of at least 6 months to have the bags injected with saline through my skin. This is so that I will grow more skin, because my flesh was taken during the surgery and my chest is tight.
After my skin has regrown, I will have to remove the tissue expanders and heal for a while. After that, the implants as well as some fat, which will be taken from my stomach and thighs with liposuction, can be put into my chest beneath the loose skin. Once this is completed, after I have healed again, we can attempt to surgery to graft my nipples again, but there is a chance they will not survive. I may lose my nipples completely.
The cost of these procedures is an estimated $35,000, and is not covered by insurance. Even still, I will never be able to breastfeed. I lost that ability forever as a teenager.
4. Rapid Onset Gender Dysphoria isn't Real
This is another lie which I hear when I'm testifying. I remember in Texas, a doctor laughed when she was asked about ROGD.
Rapid on set gender dysphoria is gender dysphoria which is experienced suddenly and usually at the onset of puberty or right after a trauma.
Most common patient seen at a gender clinic is experiencing rapid onset gender dysphoria. According to the Journal of Adolescent Health, many parents are reporting that their parents are experiencing ROGD.
I experienced ROGD after a sexual assault. I became disconnected from my gender, and I blamed all of my problems on it. I believed that only girls were sexually assaulted, and believed that if I remained one, it would happen again.
Another common reason youths, particularly girls, experience ROGD, is porn. Porn shows girls a sexualized version of femininity which is degraded and abused for the sake of men. My early exposure to porn also contributed to my ROGD. I have seen many young “trans-men” claim that they are transitioning to escape sexualization.
My story is not uncommon.
6. Gender Euphoria
“Gender euphoria” is advertised by the trans community a lot, but it's another lie.

No one experiences euphoria about their sex. Autogynophiles experience sexual euphoria and gratification when they are perceived as women, and wrong sex hormones have steroid-like effects, but that is all. The high that trans-identifying people are chasing is either sexual gratification or a literal high from drugs.
There is no such thing as gender euphoria. You can be comfortable and satisfied in your sex, and experience sex based pleasure, but gender euphoria isn’t real. Despite its non-existence, however, people suffering with gender dysphoria are set on the path to chase this high. This is how life-long medicalization happens.
7. The Male and Female Brain
There is talk within the trans community about “female vs male brains” and the claim that transgender people have the brain of the opposite sex.
According to a study written about my ScienceDaily, (linked below), "Men and women's brains do differ slightly, but the key finding is that these distinctions are due to brain size, not sex or gender," Dr. Eliot said. "Sex differences in the brain are tiny and inconsistent, once individuals' head size is accounted for."
There is not only no evidence that trans-identifying people have the brain of the opposite sex, but actually, evidence to the contrary. Despite this, the trans community, and even doctors, will tell gender dysphoric people that they actually have the brain of the opposite sex. This is diabolical, as differences between the brains of the different sexes do not exist.
8. There is no Social Contagion
The presence of ROGD and the 4400% increase in minors who with trans-identifying, this myth is easy to blow out of the water. Many trans-identifying people are minors, specifically girls, the most demographic most vulnerable to social contagions. According to a study done by the UCLA, “Nearly one in five people who identify as transgender are ages 13-17.”
The social contagion theory was first suggested by concerned mothers of ROGD teens. ROGD is a subset of gender dysphoria specifically picked up and shared by teens, and as mentioned previously, usually at the onset of puberty of following a serious trauma.
The moms have gotten together and created support groups wherein the parents come up with other solutions for gender dysphoria than drugs and surgery. They have been touted as “hateful” and “anti-trans",” however, and face a lot of backlash. Despite the success the mothers have had with helping their gender dysphoric kids, WPATH says that “-all persons— especially adolescents—are deserving of gender-affirmative evidence-based care.”
9. No Surgeries are Happening on Minors
This is yet another false claim. I won’t horrify you with photos of nude minors with their breasts cut off, mostly because I think it is wrong and exploitative to share those photos, but I will tell you that it happens, and is continuing to happen.
If you would like to find this information for yourself, search for gender clinics near you, tell them that you have a 15 or 13 year old trans-identifying daughter and that she needs “top surgery” and see what happens.
Many lawsuits are beginning to come out by detransitioners, most of whom were minors when they were medicalized. Chloe Cole is a shining example of one of these young children.
Finally, WPATH has lifted all age restrictions on surgery for trans-identifying minors under their gross and negligent guidelines.
10. Informed Consent
“Informed consent,” is a form of gaining consent on paper which is signed by the patient to verify that they fully understand all of the consequences and side effects of the treatment which they are being given. This is another delusion, however, and for two reasons.
The first reason is that children cannot consent. Children do not have the mental or emotional capacity to consent to sterilization, or understand what life long medicalization means. I could not even grasp the meaning of the words “vaginal atrophy” when they were said to me, and without being trauma informed, my doctors did not know that I said yes because my understanding of atrophy made me believe that it would make it impossible for me to be raped again. This is the way a child thinks. Children cannot conceptualize what will happen to them if they undergo puberty blockers, wrong sex hormones, or undergo surgery.
The second reason is that the doctors cannot give proper informed consent because they do not know everything that happens when a patient takes wrong sex hormones, or what complications they may have from surgery. This is brand new and experimental medicine which has not been researched in the long term.
Puberty blockers have only been studied for their use in things like precocious puberty and their long term use remains unstudied. Wrong sex hormones have almost never been studied, and the studies that we do have are short term, not peer reviewed, and abysmal. Brand new surgeries seems to be coming out every month or so, like experimental clavicle shortening for trans-identifying males. There is no way for any research or long-term follow up to have been done on this.
11. “Trans Hate” is at an All Time High
At a time when the president is visiting with newly trans-identified men and writing them personal letters of congratulations, and trans-identifying people are all over the media with sponsorship deals and being influencers, and with acceptance higher than it ever has been before, there is the claim that “hate” is at an all time high.
This is said usually in response to the recent bills to protect children from “gender affirming care.” These are not anti-trans bills, but they are pro-women and pro-children bills.
In fact, with the rate of acceptance, there are more trans-identifying people than ever, and the trans community will tell you this themselves. This is how they defend against the social contagion argument. Their theory is that there have always been this many trans-identifying people throughout history, and that it is because of acceptance that they are able to come out and be public about their identities. I thought there was a genocide happening, though? So is acceptance high or low? They can’t keep the narrative straight.
--
Sources:
Suicide:
https://www.cdc.gov/mmwr/preview/mmwrhtml/00031539.htm
https://twitter.com/LeorSapir/status/1631030625397252101
ROGD:
https://www.jahonline.org/article/S1054-139X(16)30765-0/fulltext
https://www.parentsofrogdkids.com/
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0202330
Male/Female Brain:
https://www.sciencedaily.com/releases/2021/03/210325115316.htm
Social Contagion:
https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/
https://thepostmillennial.com/new-study-supports-social-contagion-theory-for-surge-in-teen-girls-identifying-as-transgender
Surgeries on Minors:
https://www.nytimes.com/2022/09/26/health/top-surgery-transgender-teenagers.html
https://mercatornet.com/chloe-cole-gender-transition/80073/
https://news.northwestern.edu/stories/2022/09/age-restriction-lifted-for-gender-affirming-surgery-in-new-international-guidelines/?fj=1
==
Prisha Mosley is suing the doctors and therapists who pushed her through the transition conveyor belt. She has testified at several hearings about her ongoing medical problems resulting directly from this medical malpractice.
Reminder: suicide is itself a socially contagious phenomenon.
https://www.city-journal.org/article/reckless-and-irresponsible
Decades of research suggest that suicide is a socially contagious behavior, especially in youth. In 1994, the Centers for Disease Control and Prevention published a document titled “Suicide Contagion and the Reporting of Suicide: Recommendations from a National Workshop.” In a section titled “Aspects of News Coverage That Can Promote Suicide Contagion,” the CDC cautioned against “[p]resenting simplistic explanations for suicide.” Suicide, it explained, “is never the result of a single factor or event, but rather results from a complex interaction of many factors and usually involves a history of psychosocial problems.”
Those pushing the narrative should already know this, and those reporting it already do know this. It almost seems like they want it to happen to justify their activism...
#Prisha Mosley#gender ideology#queer theory#genderwant#affirm or suicide#manipulation#gender cult#religion is a mental illness
20 notes
·
View notes
Text
It kinda irks me when i see ppl talking about guiltying prisoners because it'll "have a better impact on them" or will "help them more than an inno vote" because we've got 4 prisoners already guiltied who haven't been benefited at all. Fuuta is probably our best, as she no longer thinks she was right for the murder, but she's also now permanently disabled and probably getting indoctrinated into a cult. Even ignoring Kotoko's attacks, they're still being tortured psychologically. They're hallucinating, paranoid and suicidal. How could subjecting someone to that hell be any better for them than forgiving them
#chernikocore#i get why ppl thought this trial 1. but why are we still thinking like this please look at our already guiltied prisoners#not just about kazui ive seen ppl say this about yuno ALOT#the only guilty vote ive agreed with so far is haruka because of the restraints TT but even that wouldn't have been necessary if not for muu#idk i dont wanna come off as rude but. how are ppl thinking this about kazui...#''this man wasnt affected by an inno vote because he hates himself too much. maybe if we make him hallucinate voices blaming him for his#wifes suicide and affirming the idea he has that he should have kept lying‚ he'll feel better :)''#orz
24 notes
·
View notes
Note
You asked to see me..? About my loss of interests..?
- Aziraphale
Yes, thank you for coming to see me Aziraphale. Would you. mind telling me a bit more about it? Do you feel like your ability to be interested in things faded slowly, or disappeared more suddenly? Are there things you still do find pleasure or enjoyment in? I'm hoping to help root out what is causing this change for you, so that we can figure out how best to address it and help get you back to fully enjoying your existence again.
//IRL this week marks National Suicide Prevention week in the US. If you or someone you know is struggling with significant changes in their mental health - including loss of enjoyment/interest, hopelessness, changes in sleep or appetite, anxiety, despair, self-endangering behavior, or any other worrying change, please seek help. I promise it can and will get better, and the world needs you more than you know.
// For mental health crisis help in the US, dial 988 or text HOME to 741741 for immediate, confidential assistance.
//For crisis support specifically tailored to gender diverse folks, contact Trans Lifeline https://translifeline.org/
//For LGBTQIA+ youth, there is also The Trevor Project https://www.thetrevorproject.org/get-help/
#good omens therapy#the angel aziraphale#mental health#mental heath support#suicide prevention#lgbtqia#gender affirming care#queer youth
16 notes
·
View notes
Text

This Fucking Guy.
#negative affirmations <333#ace attorney#aa#ace attorney fanart#miles edgeworth#miles edgeworth fanart#reiji mitsurugi#fanart#digital art#my art :D#art#he sucks soooooo bad <3333 i want him.#suicide mention#remember that time he came back from his year long suicidal trip only to go to court#and tell his own witness that he doesn't care if she kills herself? noone does it like him im afraid.#king of zero self awareness <33
48 notes
·
View notes
Text
Here's to adaptive systems.
Adaptive systems are defined as "systems which formed in response to trauma or other adversity". [via Pluralpedia]
So, here's to systems who formed from trauma, isolation, neglect, bullying, stress, disability, or just simply identify as adaptive.
Shoutout to:
Adaptive systems currently in actively traumatizing situations
Those who are processing past traumas
The ones who have found peace, but still acknowledge how they were impacted by their past
Systems who are adaptive as well as some other label to describe themselves
Those who are in therapy, on medication, in an outpatient program, have been hospitalized, or otherwise require professional assistance to help them function
Those who struggle with a dissociative disorder, self harm, suicidal ideation, depression, anxiety, personality disorders, or another condition that affects them often
We love you so much. You shouldn't have had to have been strong or resilient, but I'm glad you're still here regardless. You're so valued and important to your communities, plural or otherwise.
Please know you've got someone thinking of you. ❤️
🖤💜💙💚💛
#multiplicity#plural#pluralgang#plural affirmations#actually multiple#actually plural#requests#did#did osdd#tw sh mention#tw suicide mention#tw neglect#tw bullying#tw abuse#tw hospitalization#tw trauma#adaptive system#adaptive systems
26 notes
·
View notes
Last Seen Blogs

greetea
Untitled
americanmarketplace
AMERICAN MARKET PLACE

raposabranca
Raposa Branca Art

exploreeducation
Explore Education

justasimplesinner
peace was never an option