#cw meth
Text




Highschool creepypasta AU but it’s realistic and just the pastas being dweebs. They’re 13 and 14 and in algebra class
#creepypasta#horror.jpg#creepypasta art#ben drowned#jeff the killer#sillyposting#having a highschool au after not being in hs is the best#cus instead of it being a romanticized version of hs#it’s just having characters be shithead teenagers instead#benjeff#cw meth
{kind=link}
867 notes
·
View notes
Text
NEIL put the meth down im coming over
8 notes
·
View notes
Text
this song is for the people who tell their families that they're sorry for things they can't and won't feel sorry for
you can read this through a queer lens. as a queer person I am tempted to feel this way, too. but it doesn't sit quite right with me.
this is the Meth Album about people who are "either dead or in prison now". this song is for the junkies who threw their lives away and honestly can't say that they were sorry for doing it, because they're not. but they're saying sorry anyway. why?
queerphobia does run deep. I won't brush that aside. a lot of people are forced to atone for being queer. but queerness is something a sizeable chunk of Americans agree you shouldn't feel sorry for, and one that doesn't carry a prison sentence anymore. there's a mass cultural movement about not being sorry. there are parades about it.
being an addict is something that an overwhelming majority, especially people with addicts in their lives, feel is a moral failing—and one you must apologize for to move on with your life. the 12 Steps are nearly universally paraded and have apology or "making amends" built into them.
this song is for the (former) drug users don't want to apologize for their addictions but feel forced to even when they don't mean it. broadly speaking, they are forced to—medical and legal punishments are immense if they don't do recovery or do it the way the state wants them to.
dissimilar to queerness, there is nearly universal cultural pressure to apologize for using drugs. being seen and loved in the absence of an apology for being an addict feels like a more radical statement, and that deserves acknowledgement.
6 notes
·
View notes
Text
Cw substance/
The time I made Walter White and Jesse Pinkman into grumpuses


PLESSSSEE ABAJAHQHAH ?/!-?:!
#cw meth#cw drugs#tw drugs#tw meth#breaking bad#jesse pinkman#walter white#bugsnax#bugsnax fanart#breaking bad fanart#why did i draw this
2 notes
·
View notes
Note
CJ DOES METH
Idk why you're coming into my inbox and saying true things in all caps but sure, I mean he's a 52 year old politically incorrect queer man from rural america who we know is involved in criminal activites and he acts... like that tm. he is meth coded.
Whether you're comfortable with that or not is another question
You want to know a funny thing tho. In every modern au I've written I've had CJ textually abuse stimulants, except in the fic where Ed and Izzy are literally running drugs. granted that is only twice (heathers AU and Stizzy fake dating AU) but its weird that I haven't given him drugs in the divorce court au.
Disclaimer: I recognize that drug abuse is a serious issue and that some people are uncomfortable with it. My experience with illicit drugs so far has been rather casual and complication free so maybe thats why I feel comfortable joking about it. I promise this will be the only meth blorbo anon I respond to.
#ofmd#cw meth#I have done meth. I rate it 4/10#it only gets as high as a 4 because it didn't ruin my life and the withdrawls were non existant#my dare officer hyped this drug up and then it was just kinda... blegh#CJ would like it tho
1 note
·
View note
Text

and his four walls declared him insane
#drugblr#tumblog#drugcore#grunge#druggie#weirdcore#girls with tattoos#girls with piercings#girls who smoke weed#junkie girls#girls on drugs#lines#tattoed girls#drugs cw#tw drugs#sex and drugs#drug junkie#meth junkie#crystal mdma#pure mdma#mdmazing#girls who do pills#tumblr girls#alt girls#girls who do hard drugs#drug girls#girls who snort#snorting meth#methamphematine#girls who blow meth
72 notes
·
View notes
Text

#drugs#tw drugs#sex and drugs#drugstore beauty#drugs cw#drugstore makeup#drugs and cash seized as part of investigation into organised crime in tipperary as arrest made#drugsandresearch#drugs tw#marijuana#cocaine#snorting cocaine#mum whose baby son died with cocaine in his system after she’d been snorting it with partner avoids jail#snorting opioids#snoring sounds#im snorting#snorting meth#herion#crystal mdma#mdma trip#pure mdma#mdmazing#mdma party#from molly & tommy to gemma and gorka: the a list couples who ditched tinder for tv and are still going strong#molly#drugs of tumblr#meth friends#slamming meth#injection#injecting drugs
69 notes
·
View notes
Photo

175 notes
·
View notes
Text


Faces vs. asses
#drugs and society#drugs cw#drugs tw#drugstore#drugs mention#gimme drugs#iv drugs#love and other drugs#narcotics drugs#prescription drugs#drugs#sex and drugs#drug abuse#blowing spun#spun texas#meth spun#alternative goth#gothic#soft goth#gothgoth#goth girl#gothstyle#emo kid#emo girl#tattoos#sexy tattoed women#tattoed girls#tatted up#pretty girls#fat girls
77 notes
·
View notes
Text
"All Nazis Are Methheads"







#nazisploitation#sacha baron cohen accuses tiktok of ‘biggest antisemitism movement since the nazis’#nazis#nazigate#nazi#methamphematine#meth and fuck#crystal methamphetamine#meth and spun#meth spun#meth friends#sex meth#girls who blow meth#meth#cnc drugging#tw drugs#sex and drugs#drugs cw#drugstore beauty#drugstore makeup#drugs#drug rehab#drug detox#drug#ausgov#politas#auspol#tasgov#taspol#australia
13 notes
·
View notes
Text
Today i discovered that Tumblr people consider hating pitbulls a right wing thing, what the fuck.
#tumbrl#average tumblr user#pitbull#anti pitbull#just ban that breed#they kill more people than any other dog breed#and cats and rodents#and animals#and children#other dogs#they just like to maul injury and kill stuff#the only people i have ever saw owning one were naziskins and meth addicts#it was litterally bred to kill stuff i don't care if yours seems fine#keep it away from smaller animals and other people#calling yourself a leftist and owning a dog that is an hazard to other people is ridiculus#tw animal abuse#cw animal cruelty#cw animal abuse#somebody may call that at least
20 notes
·
View notes
Text
roll the pipe just right
watch the smoke fill up
don't let it out of sight
it's like water -- fill your cup
god stop talking about it
and yes you are still high
fuck could they tell I was lit
it wasn't me -- it was a lie
I get bored so I get high
I get bored so I get sober
I get high 'cause I can't die
I get high 'cause it's October
and I keep doing anything
or nothing at all
to try to find what's missing
or I'll become small
write it down so it's true
make it nice, make it pretty
don't fade into the blue
I don't want them to pity
-ash
#writing#writer#poemsbyme#poetry#poets on tumblr#poems and poetry#sad poems#sad poetry#drug addiction#narcotics drugs#trigger warning drugs#cw drugs#meth#tina#drug recovery#we do recover
16 notes
·
View notes
Text
in the newest edition of skinny bitch audacity (fatphobia):
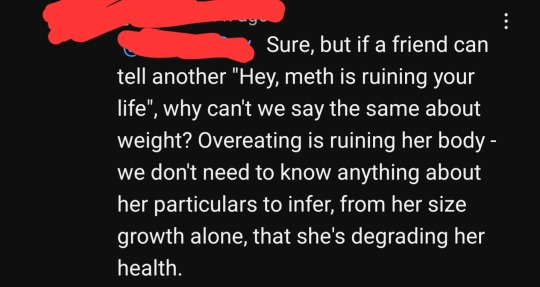
comparing weight gain to... being a meth addict. and that you can look at someone and be qualified to say theyre degrading their health if they arent a small enough size for you to be attracted to them/be 'acceptable'
[IF YOU SHAME ADDICTS ON THIS POST YOURE GETTING BLOCKED. IF YOU SHAME FAT PEOPLE ON THIS POST YOURE GETTING BLOCKED. I WILL NOT WARN YOU TWICE.]
#literally as someone who put a small hole in my nose from snorting pills i stole and destroyed an oven making meth#i think my eating disorder is and always will be the biggest health issue i have subjected myself too#people treated me better when i was skinnier and diluting drain killer and throwing up on myself after attempting suicide#then being fat and more gentle to my body despite my surroundings#im disabled and not the healthiest vs walking 30 miles a day before but... i was fucking destroying my organs and had no personality#that isnt healthy!!!!#this is the same mindset that encourages eating disorders! that encourages and excuses doctors dismissing fat people's problems and blaming#it on weight when that isnt a factor! the same mindset that kills thousands!! get a life get a personality and stay out of peoples business!#thats not even going into how fatphobia as a whole has racist origins and how it still upholds to this day!#educate yourself and liberate yourself instead of still upholding this bullshit that harms millions#i hate skinny bitches you owe me 500 dollars and the decency to shut the fuck up for forever#ransom note#cw fatphobia#also adding that note at the end like. this site loves being hostile to fat people AND addicts and im not entertaining your audacity either
18 notes
·
View notes
Text
Experimenting with drugs, i.e. cannabis and nicotine, and alcohol in adolescence and young adulthood has its risks but it does not automatically make you an addict. Drinking at a party just because alcohol is available does not automatically make you irresponsible and untrustworthy. Smoking weed because you’re bored and have nothing else to do does not automatically make you dependent. Trying one cigarette, even a whole pack of cigarettes (not all at once ofc), will not doom you.
Experimentation is normal, it is expected, it is demonstrably FINE.
You can have the responsibility not to drive, you can have the responsibility to eat something and drink water, you can have the responsibility to take care of others at parties, you can have the responsibility to spend money on groceries and rent before buying some booze, you can have the responsibility to smoke outside so your room doesn’t smell, you can have the responsibility to know the symptoms of overdose and the responsibility to DO something when you see someone has overdosed, you can have the responsibility to know how these drugs and your medications interact, you can have the responsibility to know the symptoms of addiction and seek help if you experience them.
An addiction is much, much different than curiosity. In all likelihood, if you use responsibly, you will figure out what you like and don’t like, how much is enough, and what the best practices are. And you will still not have an addiction.
#obligatory do not do meth or heroin#obligatory I am not an expert#I am also still a young adult#but I’m learning to cut myself some slack#human beings have always liked the funny plants and rotten fruit juice#anyways quit scaremongering#that won’t solve anything#I am sure there are many people out there more knowledgeable than me#cw addiction
21 notes
·
View notes
Note
SOOOO CHENYA WHAT IF I SAY THAT CHESSIE HAD CATNIP NOW SHE'S STARTING TO SEE RAINBOWS? :3
Ahhhh, catnip! *grins*
Is it her first time on catnip? I wish her well! She’s in for a fun time! Rainbows are a fun treat!

#the fun thing about catnip is that even though it’s a drug for us kitties it’s also just… a plant#so while of course we shouldn’t have too much of a good thing it isn’t going to HURT us by any means#in other words - all of the ‘fun’ of regular drugs with NONE of the horrible side effects#that make regular drugs things you should NEVER partake in#this of course does not include prescribed medications or recreational drugs 👍#I’m talking about like LSD or heroin or meth#don’t do drugs kids#but catnip is fine! 😸#che’nya chats#twst rp#che’nya rp#Cheshire Cat family reunion#tw drugs#cw drugs#<- ooc: just because of the tags oop#ooc: also I have no idea the difference between cw and tw so they both go on sorry 😭
9 notes
·
View notes
Text
4/28/24
Really, really proud of my team today. Beyond excellent response to a potential disaster scenario this morning.
Turns out overnight we got an admission to our unit who was just banned from, apparently, every other hospital in the area. At an outside hospital we occasionally accept patients from, he assaulted 3+ staff members; multiple new assault charges against him. They didn't want him anymore, so they sent him to us in 4 point restraints. He was knocked out from a sedative the night before, currently sleeping in his room.
Always fun to hear someone say "Yeah they just seriously attacked like four or five other people. Alright Gomdy, it's your turn!" As soon as report was over, I updated the security guard on the situation, called the security department to be aware of the pending need for backup, and very, very politely informed the doctor on call of the very, very important need for his prn injection to be strong enough. We were not taking any chances.
Guy wakes up an hour after report is over, walks into the hall, asks me where he is. I calmly answer his question, he shouts "FUCK!" and goes back into his room. Security and I are already watching each other closely, and he calls for back up just in case.
For the next twenty five minutes, the guy is just asleep in his room. I hear him cough and hock a loogie, so I walk in and talk to him a bit. Denies knowing why he's in any hospital to begin with, says the police kidnapped him. He agrees to breakfast. I bring it to him in his room. I am not fucking around with "No, you need to eat out here with everyone else." Not today, not like this. Someone who gets special privileges on the acute psych unit is someone who is not doing well.
While all this is going down, I'm constantly, constantly keeping everyone in the loop. Resident doctor? Let him rest, come back when he's ready for her. House Sup? Meets us in person to discuss the security risk. The security officer present at the time is the same guy who was hurt several months ago with one of my other patients, so he deserved to see that I was doing everything I could to make sure there wasn't going to be an event, and if there was, that it would be quick and decisive.
After I bring the patient his tray, what, fifteen minutes pass? And i hear a clatter. I go in there and find his food half eaten and spread lying against the wall, a few feet from him, clearly thrown. I ask him what happened, he says "I dropped the tray." Yeah okay. I ask him "Will you help me clean it up so I can get it out of here?"
The thing some people may not realize is, that's a valid assessment question, and his answer was "yeah." He immediately started helping me pick the food up off the floor and put back onto the tray so I can take it to the dirty food cart thing. I ask him if there's anything I can help him with; he wants to speak with "whoever's in charge." I tell him I'll contact the doctors, etc.
That was the moment I started suspecting it; that "emotional outburst" syndrome, or whatever its called. Where someone has a brief episode of losing their shit completely, and then regains control again soon after. That comes before the probable meth addiction. As far as I'm concerned, if he didn't have the former, he wouldn't have the latter.
But that's getting away from myself. Someone calls, and it's his mom. She asks me if we have a patient with his exact name and description; I put her on hold, and check if he knows the lady; He does. I quickly and quietly ask him to file the form that says she's allowed to know who he is and why he's here, and what does he do? He complies! Perfectly cooperative, he rights himself, takes my pen, signs the form, plops back down in bed.
I go back and tell his mom "Yeah he's here." She's quieting down a cat in her house, then asking me for details. "Assaulted a bunch of staff members." That gets an "oh, oh, ohhhh oh dear," from her, the kind only a little old lady can give. She's gotta be his enabler, I think to myself.
This whole morning, he's got that standard affect I've come to find in men with severe anxiety disorders and drug addictions; brief, one word answers, feigned lack of knowledge of a subject, guarded/masked disclosures, and desperation to discharge. All his interactions with me, when they're cooperative, are filled with desperate and practiced self control. One that doesn't come with a deeper feeling of inner peace, but instead from having learned "if I lose my cool now, I will be worse off for it."
The resident and the head physician come by, and as soon as they're on the unit I make sure the security guard calls for back up. Once the two doctors are ready to go talk to the guy I tell them, "Hold on, I've been building a rapport with him. Let me go in there first, and let me introduce you two."
And they do it. We go in, and he's talking with them from his hospital bed. All the standard questions anyone wants to know when they're an involuntary admission. "What's going on? Why am I here?" The doctors start asking him what he remembers, and he reveals he of course knows a little bit more than he let on. He remembers feeling "parasites" all over his skin, and telling his mom he wants to die. He fully well remembers all of it, I'm sure. Just doesn't want to admit it, out of fear of being punished. And at one point he asks "And my cat! Where is my cat?" That was when I interrupted the doctors. "I spoke with your mom briefly on the phone this morning, and she was quieting down a cat who was mewing loudly. Does that sound like your cat?" Immediately, the guy's face relaxes. My god, I think to myself, that was a really fucking lucky phonecall.
"When can I leave?" That last one is the one that tests everyone, and I don't envy them for being asked it. They tell him "Not today," and "we'll see how you respond to treatment," or something like that. Guy's already clearly desperately controlling himself. Asks for permission to go use the patient phone on the unit. They tell him "yes," and he gets up to go use the phone.
At this point, I've been watching him closely enough to go "Okay, yeah, that phone call is not going to go well." I take the opportunity to warn another nurse, who's already watching, what I'm sure is about to happen, and then go pull meds from the med room. While I'm in there, I hear an unmistakable banging sound; Guy's smashing the phone against the receiver. Yup, needs something to calm down before he attacks.
I thought that morning when I called the doctor to ask for a stronger dose I got one, but the head doctor on the unit who saw him stopped me and told me "No, up the haldol dose. Make it stronger." Kinda surprised me, but in a good way. They understood exactly what I was trying to avoid. I had to go back and get more haldol in a syringe, but whatever works.
I had two syringes of sedatives ready pretty quickly all things considered, but we still waited for more security to arrive before doing anything. The patient had already gone back to his room after getting whatever bad news he heard on the phone, it turns out, so we were just preparing for the worst before doing anything.
It ended up being a party of, what, eight people? Three nurses, a technician, and four security guards to go into this guy's room. Each of the guards agree on what limb they would grab if it came to that. But I stopped them up front and said "Hey, before anything happens, let me do the talking. I'm gonna go in there, introduce myself and explain what we're here for, and we'll go from there."
So, when we went in there, I politely explained "I see you want to calm down, we have some medication to help you with that." And what does he do? He willfully complies! Just rolls over onto one side and exposes his shoulder for me. I give the injection pretty quick, apply my bandaid, and allow the other nurse to get his other shoulder. The guy was clearly forcing himself to manage his anxiety in the moment, but he wasn't attacking anyone or screaming. Nobody even needed to lay a hand on him.
And he just slept like that for the rest of the shift! Not totally sleeping, mind. I'd leave lunch and dinner trays in his room, and come back an hour or two later to find them half eaten. He knew food was there, he knew we were letting him rest, and he wasn't fighting us on it. No violent outbursts, no nothing. Just some angry phone treatment and food to clean up off the floor.
This event could have so easily been another security guard out on leave, or a nurse out, or what. But it wasn't, because everyone communicated and worked together. Completely avoided any events entirely. I don't want to pretend we did better than that other hospital did, because I'm pretty sure we were on the latter half of withdrawal, but I won't deny we displayed some true skill in our interventions this morning. I know it's going to happen eventually, but so far I've never been assaulted on this job.
I don't want to write all this without talking about the patient, though. I think the root issue with guys with his presentation is basically, the anxiety. They don't have an internal locus of control, beyond "Shut up and calm down." They can't examine themselves effectively; it's either not part of their thought process or its too painful. So when they've got a thought, or a feeling, or a situation, causing them so much pain and fear, they can only tell themselves "I can't lose my shit right now" to get through it. Nobody can survive on "just keep it together" forever.
Without any understanding or guidance, they're just going to stay in a bad situation as it gets worse. Eventually turning to drugs like meth to try to make the pain go away, which of course only makes everything exponentially worse. Eventually they snap, in whatever form that takes. But when they regain control, they don't experience that release of tension, or fear. They just go back to keeping that internal storm barely under control.
My heart goes out to this population. I don't know how to help them, beyond my job. And my job is really only to help him through the withdrawal and get him out of the crisis state of wanting to kill himself or hurt anyone else. After he leaves here, If the social worker can't help him effectively, he goes right back to whatever resources he has available to him. And he's in this situation because those have already failed him. Lots of people say "patients in these situations don't get better until they accept that they need to get better." But how does someone like him reach that point?
Hey, but that security guard has come to appreciate me a lot though. He frequently tells me he likes working with me, because I'm so "By the book." Well damn dude, I'm so thankful you're here to let me do my job safely! Can't believe administration tried to tell us we didn't need a full time security presence on this unit. Buncha fuckin chumps.
#nursing#psych#psychiatry#dear diary#diary entry#psychosis#nurse#schizophrenia#cw: drugs#cw: addiction#cw: meth#amphetamine#mental health#addiction#assault
4 notes
·
View notes
Last Seen Blogs

glitterbomb-dave
Saeglopur
gregpostok
Greg Postol

nephrologistpatna
Nephrologist In Patna

nenedip
DipnDots

jorylaj6134
Capture The Moment