#childhood psychiatry disorders
Photo
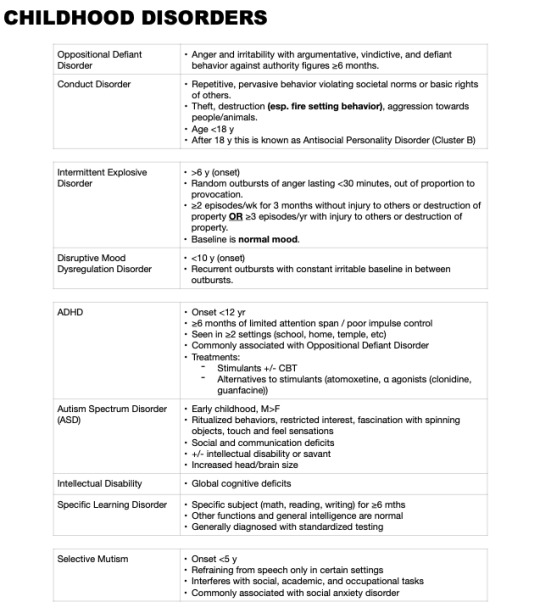
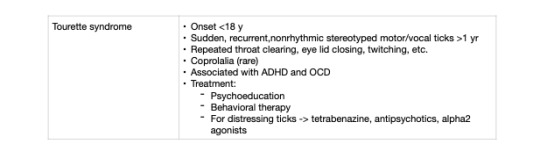
Childhood Psychiatry Disorders: High yield for USMLE
#USMLE#USMLE prep#usmlenotes#usmle notes#psych notes#psychiatry#medblr#medical school#medical notes#tourette syndrome#selective mutism#specific learning disorder#intellectual disability#autism#ADHD#Disruptive mood disregulation disorder#intermittent explosive disorder#Conduct disorder#oppositional defiant disorder#childhood psychiatry disorders#childhoodpsych
38 notes
·
View notes
Text
Before you define yourself as being anti-self-diagnosis and pro-psychiatry or therapy remember,
to search about psychiatric hospitals and how is the treatment of the disorders outside the US, in third-world countries (like where I live),
listen to people traumatized by therapy, especially kids,
and if possible search up the about how's education of neurodivergences and the approach of neurotypical to neurodivergent people in countries other than US again,
acknowledge that MANY therapists won't respect you and your choices, and they don't need to choose for you what you should and shouldn't do about your life choices, it makes some people suffer,
the majority of doctors and a lot of people even neurodivergent ones won't respect your spiritual beliefs if they're about how your neurodivergence originated and it's wrong because it also hurts people, and in countries other than US there are more types of religions/spiritualities that don't see some things as a disorder,
and in the end remember that no it's not because they're doctors that means that they're always right or know about your brain better than you, you should explore yourself more.
Do it all with empathy, sympathy, and kindness
#anti psychiatry#ableism#disability rights#disabilities#anti self diagnosis#neurodivergence#actually schizospec#schizospec#anti therapy#cluster b safe#aspd safe#speaking as a Brazilian people here have an old century view of neurodivergents#if you're to travel to here don't disclose your neurodivergence or persodivergence#childhood trauma#complex ptsd#post traumatic stress disorder#actually adhd#psychiatry#sanism#antipsych#intellectual disability#psychology#anti psych#pro self diagnosis#pro paraphile#pro recovery#self diagnosed autism#therapy
87 notes
·
View notes
Text
"Clinicians and researchers who deal with people with histories of chronic trauma are routinely confronted with fight, flight, ore freeze reactions. Our patients (and occasionally colleagues) easily take offense, and they often disorganize their (and our) lives by becoming too angry, too ashamed, and too frozen. Minor irritations easily turn into catastrophes; small failures of communication are difficult to gloss over and easily turn into dramatic interpersonal conflicts...human kindness...often fails to have a significant impact on the despair, rage, and terror of people with histories of trauma and abandonment.... Gradually we came to understand that the most severe dysregulation occurred in people who, as children, lacked a consistent caregiver. Emotional abuse, loss of caregivers, inconsistency, and chronic misattunement showed up as the principal contributions to a large variety of psychiatric problems (Dozier, Stovall, & Albus, 1999; Pianta, Egeland, & Adam, 1996). One of the most important discoveries in psychology, neuroscience, and psychiatry has been that failure in establishing secure early attachment bonds leads to a diminished capacity to regulate negative emotions.... Sadly, deficient affect regulation caused by early adverse experiences is compounded by the resulting off-putting behaviors in the face of stress, such as temper tantrums and emotional withdrawal (Shaver & Mikulincer, 2002). Dysregulated behavior alienates potential friends and partners and interferes with being able to garner support and accumulate restorative experiences. Lack of affect regulation thus runs the danger of becoming a vicious circle, where deficient self-control leads to abandonment, which in turn makes it even more difficult to regulate the negative mood states."
from The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation by Stephen W. Porges, Foreward by Bessel A van Der Kolk
#polyvagal theory#Bessel A van der Kolk#Stephen W. Porges#psychology#pysiology#psychiatry#mental health#emotions#nervous system#self help#depression#communication#bipolar#borderline personality disorder#ADHD#CPTSD#PTSD#chronic trauma#abandoned#psychosomatic#psychophysiology#physiological psychology#sympathetic nervous system#parasympathetic nervous system#enteric nervous system#eating disorder#pills#self diagnosis#autism#childhood trauma
4 notes
·
View notes
Text
“One of the things that’s really driven me in my work with children and abuse is you see how the general public have so much empathy and gushing sentimentality for abused children and these poor little three, four, five, six-year-olds. By their twenties and thirties, they’re alcoholic and they’re addicted to heroin. And suddenly the public have turned off their empathy switch, and we’ve forgotten the developmental roots of that. And so, as I moved in my own career away from child and adolescent psychiatry into adults’ addictions, what became patently clear was that these patients in their thirties, forties, fifties with alcohol and opioid addictions were the same cohort of little four, five, six-year-olds that I’d cared for in the past.”
Dr. Ben Sessa, in an interview from How to Change Your Mind by Michael Pollan
#dr Ben sessa#michael pollan#psychiatry#psychology#how to change your mind#addiction#substance use#substance use disorder#abuse#trauma#childhood trauma#alcoholism#heroin#opioid#child psychiatry#childhood development#devolopmental psychology
25 notes
·
View notes
Text
HFourth Stay in the psych ward. I am safe now. It doesn’t take long to go from manic to psychotic, but with the right help and medication I can get on top of it… Eventually.
I am in my mid- forties. I got a diagnosis of bipolar a few years ago, but this has been changed to schizoaffective disorder. This is why it is crucial to be as transparent as possible with one’s psychiatrist or psychologist. It wasn’t that I was withholding information, I just assumed a lot of information I had about myself and the happenings in my mind were normal and therefore irrelevant.
But normal could be a diagnosis just around the corner for you. You don’t understand why no matter how hard you try, your life is just passing you by, while you watch everyone else thrive. That’s me. Many half/downright said: oh she is taking the piss relying on her husband. I was…relying on my husband, and trying meant nothing because my enemy was my brain, the most powerful tool we conceive from and do everything with. When it is broken and you don’t know it, you keep hammering like everyone else, and while they make houses of stones, you see your beautiful sandcastle be washed out to sea one more time out of a million times.
The only real house I have ever had is the one who loves me, could be a cat… could even be a real man if I’m lucky. Till next time… Love, Shea.
#bipolar disorder#childhood abuse#depression and anxiety#schizoaffective disorder#trauma#poverty#homelessness#isolation#misunderstood#labeled#crazy#judged#discarded#different#Hopeful#psychology#psychiatry#Rape
3 notes
·
View notes
Text
Stress in Children
#psychotic diseases treatment in indore#de-addiction specialist indore#anxiety disorder treatment in indore#psychiatrist in indore#childhood psychiatry problems treatment in indore#mood disorder treatment in indore#addiction treatment in indore#childhood disorder treatment in indore
0 notes
Text
Dear Diary,
Growing up I would constantly get sick and my doctor’s would treat my symptoms but never found the root of the problem. My early twenties brought up a lot of changes for me and it was extremely overwhelming. i was diagnosed wirh type II diabetes, hypothyroidism, GAD, bipolar djsorder II, and chronic migraines.
As a child I was borderline diabetic but was able to get better and get it under control for years. My hypothyroidism was found when i felt nodules on my thyroids. GAD and my bipolar diagnosis was discovered when my primary said i was depressed and prescribed me zoloft unsupervised for over a year. i was getting worse and went to see a psychiatrist after desperation. Later on that year I attempted suicide by running to oncoming traffic. Fortunately for me my coworker was able to catch me and dragged me to his car for safety. That night I was numb and my family djdnt even notice; I never told them. Months later i had an episode before driving back to college that landed me in the psych ward. That was the lowest point of my life and I vowed I would never go back.
My migraines story isnt as dramatic but it was an issue I was dealing with my entire life. My pediatrician said they were just headaches because of my thick long hair. i would have sensitivity to light, sounds, and smells. I would always vomit for hours and I would always feel weak afterwords. As an adult the severity of those symptoms increased and would last days. Now when I get them I usually need to be hospitalized for the pain cocktail, nausea medicine, and fluids because of dehydration. i see a neurologist now and can only take medication for it through a nasal spray and dissolvable tablet.
This is just the beginning…
#psychiatry#bipolor#migraine#generalized anxiety disorder#diabetes#loneliest#depressing shit#hypomanic#me myself and i#my story#childhood cancer survivors
0 notes
Text
As a significant "feminised" category of mental illness, however, HPD [histrionic personality disorder] was superseded in the DSM-III by the introduction of the controversial BPD, a label which has been increasingly applied to women, with around 75 per cent of all cases estimated to be female. Seen as a milder form of schizophrenia and lying on the "borderline" between neuroses and psychoses, the concept has been used in psychiatry since 1938. Like other personality disorders, BPD has a notoriously low reliability level even by the generally poor standards of the DSM, and even within the profession is considered by many as yet another "wastebasket" category (though as Bourne ruefully remarks, the ambiguity of such personality disorders makes them particularly useful in policing deviance in the new century). One member of the DSM-III task force stated at the time of constructing BPD that "in my opinion, the borderline syndrome stands for everything that is wrong with psychiatry [and] the category should be eliminated". The chair of the task force, Robert Spitzer, admitted with the publication of DSM-III that BPD was only included in the manual due to pressures from psychoanalytically oriented clinicians who found it useful in their practices. Such practices have been documented by Luhrmann who describes psychiatrists' typical view of the BPD patient as "an angry, difficult woman—almost always a woman—given to intense, unstable relationships and a tendency to make suicide attempts as a call for help.' Bearing significant similarities to the feelings of nineteenth century psychiatrists towards hysterics, Luhrmann's study reveals psychiatrists' revulsion of those they label with a personality disorder: they are "patients you don't like, don't trust, don't want . . . One of the reasons you dislike them is an expungable sense that they are morally at fault because they choose to be different." Becker reinforces this general view of the BPD label when she states that "[t]here is no other diagnosis currently in use that has the intense pejorative connotations that have been attached to the borderline personality disorder diagnosis." A bitter irony for those labelled with BPD is that many are known to have experienced sexual abuse in childhood, something they share in common with many of those Freud labelled as hysterical a century earlier; a psychiatric pattern of depoliticising sexual abuse by ignoring the (usually) male perpetrator, and instead pathologising the survival mechanisms of the victim as abnormal.
By the mid-1980s, the hysteria diagnosis had disappeared from the clinical setting while BPD had become the most commonly diagnosed personality disorder. BPD is now the most important label which psychiatric hegemony invokes to serve capital and patriarchy through monitoring and controlling the modern woman, reinforcing expected gender roles within the more fluid, neoliberal environment. Nevertheless, as Jimenez (emphasis added) reminds us, the historical continuity from hysteria to BPD is clear: "Both diagnoses delimit appropriate behavior for women, and many of the criteria are stereotypically feminine. What distinguishes borderline personality disorder from hysteria is the inclusion of anger and other aggressive characteristics, such as shoplifting, reckless driving, and substance abuse. If the hysteric was a damaged woman, the borderline woman is a dangerous one."
Bruce M.Z. Cohen, Psychiatric Hegemony: A Marxist Theory of Mental Illness
3K notes
·
View notes
Text

Childhood PTSD vs Autism
#ptsd#childhood ptsd#trauma#autism#asd#autism spectrum disorder#psychcore#psych#psychiatry#psychology#psychotherapy
1 note
·
View note
Note
what are your thoughts on ocpd? i generally think these behaviors are harmless or at least not distressing and wouldn't benefit people much to have classified as a personality disorder.
hmmm i could post more nuance abt this at a later time so giving this response might be kicking a hornet's nest + leaving- please please please keep in mind that i believe all ppl's suffering is valid + in need of healing + i am questioning the history, purpose + impact of personality disorder dx, NOT the lived experiences of ppl diagnosed with them
while i think all psychiatric diagnosis is suspect, i find personality disorders in particular to be laughable, even by dsm standards. they are a hodgepodge of "types of ppl we think are bad". the words "unusual" + "dramatic" are used to describe supposedly objective pathologies. if anything, these disorders serve as a massive red flag that psychiatry is far less wedded to science than its proponents want to believe it is. i think our attempts to 'destigmatize' this absolutely dogshit collection of disorders instead of questioning their use or existence has been a horrible error within the mad community.
many of the criteria are absolutely seeping with moral judgements + christian ideology. several are blatant repurposings of hysteria. they are frequently diagnosed in ppl who have no desire to 'heal' from them (not viewing the behaviors as a problem is often part of the dx). things like disregarding the rights of others or exploiting others for your own gain are side by side with things like the desire to not be around ppl or intensely believing in aliens. most of them can be directly linked to traumatic experiences in childhood + yet they persist in portraying them as disorders of individual, unchangeable pathology. if ppl expanded their view of trauma, i'm willing to bet that basically all cluster b + c + a decent chunk of cluster a ppl would qualify as having experienced significant trauma.
fwiw, i definitely meet the ocpd criteria but i find the word ocd to be a more useful tool for me. my father also meets this criteria + i would say it has been a deeply destructive pattern of behavior in his life for himself + his loved ones. i can't say this is the case for everyone meeting this criteria, tho.
i just don't think the concept of diagnosing anyone with having a "disordered personality" is healing. some things classified as pds are extremely distressing experiences which ppl deserve support for, but i would like to see those placed in conversation with trauma, politics, + community. classifying intense trauma responses as permanent disorders of the self leaves a horrible taste of blood in my mouth. how many of us already believe that we are inherently broken because of what happened to us?
like u said, other things classified as pd diagnoses can be pretty harmless differences. i often see ppl in my communities responding to the widespread belief that ppl diagnosed with pds are immoral or evil (which is shitty!) by trying to 'destigmatize' them, but i propose, after a careful evaluation of the history + current usage of the diagnosis, that the concept of personality disorders was + is intended to classify ppl who are seen as morally corrupt or 'unusual' as being diseased. the original purpose of this diagnostic category was to stigmatize people. is this really the concept we want to seek liberation through, or can we find new ways of understanding any suffering that may come from the experiences currently labeled as personality disorders?
211 notes
·
View notes
Text
How Common is Neurodivergence?

[image id: poster of "How Common is Neurodivergence?.” There are 12 circles and five small images: an image of a brain, speech bubbles, an infinity sign, a person reading, and a person surrounded by arrows and balls. Each of the 12 circles has a percentage representing how common a particular form of neurodivergence is written in Open Dyslexic font. Full transcript, more information, and references under the cut.]
More Information
Forms of neurodivergence represented here are focused on neurodevelopmental disorders.
These percentages are representative of percentage in general population and do not reflect percentages within neurotypes which are often higher due to co-occurrence being the norm, rather than the exception, within neurodevelopmental disorders; for example, 33-45% of people with ADHD will also have dyslexia (Butterworth & Kovas, 2013), whereas only 10% of the general population are dyslexic (British Dyslexia Association [BDA], 2023).
Certain neurodivergencies are often underrepresented and under-reported, so the percentages are likely to be higher; for example, one study suggests that rates for FASD in the UK may be as high as 17% (McQuire et al., 2019).
Some of the neurodivergencies represented here are umbrella terms and percentages given are representative of all forms of neurodiversity belonging to that term; for example, SpLds include dyslexia which is at a rate of 10% (BDA, 2023) and dyscalculia which is at 3-7% (Haberstroh & Schulte-Körne., 2019). Tic Disorders at 1% are another example here, as this is inclusive of Tourette Syndrome which is at 0.6%, and around 1 in 5 individuals exhibit tics at some point during childhood (Cavanna et al., 2017).
______________
Transcript in Full
1% Intellectual Disability
10% Language Disorder
4% Speech Sound Disorder
5% Stuttering
7.5% Social (Pragmatic) Communication Disorder
1.7% Autism
5% ADHD
10% Specific Learning Disorder (SpLD)
5% Developmental Co-Ordination Disorder (DCD)
3-4% Stereotypic Movement Disorder
1% Tic Disorders
3.6% Fetal Alcohol Spectrum Disorders (FASD)
______________
Sources
American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders (5th Ed., Text Rev.).
Arvidsson, O., Gillberg, C., Lichtenstein, P., & Lundström, S. (2018). Secular changes in the symptom level of clinically diagnosed autism. Journal of Child Psychology and Psychiatry, 59(7), 744–751.
Attention-deficit/hyperactivity disorder (ADHD). PsychDB. (2022, November 29).
Autism spectrum disorder (ASD). PsychDB. (2022, May 19).
Butterworth, B., & Kovas, Y. (2013). Understanding neurocognitive developmental disorders can improve education for all. Science, 340(6130), 300–305.
Cavanna, A. E., Coffman, K.A., Cowley, H., Fahn, S., Franklin, M. E., Gilbert, D.L., Hershey, T.G., Jankovic, J., Jones, M., Leckman, J.F., Lehman, R., Mathews, C.A., Malaty, I., McNaught, K., Mink, J.W., Okun, M.S., Rowe, J.A., Scahill, L.D., Scharf, J.M., Schlaggar, B.L., Stewart, E., Walkup, J.T., Woods, D.W.. (2017). The spectrum of Tourette Syndrome and TIC disorders: A consensus by Scientific Advisors of the Tourette Association of America. Tourette Association of America.
British Dyslexia Association. (2023). Dyslexia. British Dyslexia Association.
Dyspraxia at a glance. Dyspraxia Foundation. (2023).
Haberstroh, S., & Schulte-Körne, G. (2019). The Diagnosis and Treatment of Dyscalculia. Deutsches Arzteblatt International, 116(7), 107–114.
Ketelaars, M. P., Cuperus, J. M., van Daal, J., Jansonius, K., & Verhoeven, L. (2009). Screening for pragmatic language impairment: The potential of the Children’s Communication Checklist. Research in Developmental Disabilities, 30(5), 952–960.
May, P. A., Baete, A., Russo, J., Elliott, A. J., Blankenship, J., Kalberg, W. O., Buckley, D., Brooks, M., Hasken, J., Abdul-Rahman, O., Adam, M. P., Robinson, L. K., Manning, M., & Hoyme, H. E. (2014). Prevalence and characteristics of fetal alcohol spectrum disorders. Pediatrics, 134(5), 855–866.
McQuire, C., Mukherjee, R., Hurt, L., Higgins, A., Greene, G., Farewell, D., Kemp, A., & Paranjothy, S. (2019). Screening prevalence of fetal alcohol spectrum disorders in a region of the United Kingdom: A population-based birth-cohort study. Preventive Medicine, 118, 344–351.
Norbury, C. F., Gooch, D., Wray, C., Baird, G., Charman, T., Simonoff, E., Vamvakas, G., & Pickles, A. (2016). The impact of nonverbal ability on prevalence and clinical presentation of language disorder: Evidence from a population study. Journal of Child Psychology and Psychiatry, 57(11), 1247–1257.
Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C., & Rohde, L. A. (2014). ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2), 434–442.
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The worldwide prevalence of ADHD: A systematic review and metaregression analysis. American Journal of Psychiatry, 164(6), 942–948.
Prevalence and Therapy Rates for Stuttering, Cluttering, and Developmental Disorders of Speech and Language: Evaluation of German Health Insurance Data. (2021). Frontiers in Human Neuroscience, 15(645292), 1–13.
Social (pragmatic) communication disorder. PsychDB. (2021, March 29).
Stereotypic movement disorder. United Brain Association. (2022, August 8).
Wren, Y., Miller, L. L., Peters, T. J., Emond, A., & Roulstone, S. (2016). Prevalence and predictors of persistent speech sound disorder at eight years old: Findings from a population cohort study. Journal of Speech, Language, and Hearing Research, 59(4), 647–673.
UCL. (2013, April 19). Learning disabilities affect up to 10 per cent of children. UCL News.
#neurodiversity#neurodiverse stuff#neurodivergent#neurodivergence#actually autistic#actually audhd#autism#audhd#adhd#dyspraxia#disability#disabilties#neurodevelopmental#intellectual disability#communication disorder#stuttering#asd#motor disorders#dcd#actually dyspraxic#dyspraxic#tics#tourettes#splds#dyslexia#dyscalculia#dysgraphia#fasd
354 notes
·
View notes
Note
What Psychiatry actually says: Most evidence we have points towards that DID and OSDD-1 are likely caused by early childhood trauma the majority of the time - however there are some exceptions where either trauma happened later or trauma history could not be identified. There are also people who demonstrate extremely similar symptoms, but that seem to be caused by cultural and spiritual practices rather than trauma, so these people should not be diagnosed. We still have a lot to learn about both these disorders and similar phenomenon, so we can't make any sweeping conclusions about how it develops and why.
What anti-endos say: Well actually, science says that it's literally physically impossible for systems to form any other way except for this specific type of trauma, so if you experience anything otherwise you're wrong and you're personally attacking me!
.
81 notes
·
View notes
Note
Hi! I have a question? I’m not sure if it’s potentially obtuse of me to ask or if it’s offensive, I’m really sorry if it is.
But I’m a little confused, because I keep trying to find NPD articles because my friend said they may have it. and I keep seeing articles where a lot of the info is like. Incredibly biased. I don’t know a lot about NPD besides like the really stupid stereotypes, and I was wondering if you could give me like a basic rundown?
Sorry if it’s a little long, the articles were pissing me off.
Thank you in advance and thank you in general!
Hey there.
Yeah, biased articles is something you're going to see all the time when handling anything regarding NPD. I'll share some with you. Some of them might sound a little annoying but they are as objective as it gets. I rather not link personal posts by people here. I assume you need scientific objectivity.
NPD is a highly stigmatized personality disorder with a high chance of being a result of childhood trauma/neglect/abuse. It's broadly split into vulnerable vs. grandiose NPD but this distinction isn't supported by every psychiatrist.
It's usually stated that pwNPD have low affective (reaction) and/or cognitive (comprehension) empathy, but studies on that have been pretty mixed. A common trait of NPD is a warped perception of yourself, your importance, and your value. PwNPD tend to have a need for "narcissistic supply", though I personally don't like the term & other psychiatry loosely based on Freud.
Here's a dry description from the NCBI website. Here's another article from NCBI with a more detailed look into comorbid factors that pwNPD experience. Both of these rather strictly focus on DSM-5 criteria for NPD. You might find that some pwNPD find DSM limiting and slightly biased.
This one talks about relation between childhood abuse and development of narcissism. Here's another article on how NPD develops as a protective strategy after early trauma. There's severe gender bias in diagnosing NPD: in cases of displaying the same symptoms, men are more likely to be diagnosed with NPD and women - with BPD. NPD is highly comorbid with other personality disorders, mainly BPD and HPD. An obvious TW but grandiose narcissists are more likely to plan out a successful suicide while vulnerable narcissists are more likely to attempt suicide.
Oh, also. "Narcissistic abuse" does not exist.
So, yeah. Maybe your friend can get a good therapist and/or check out some stuff on #actually npd (without fanaticism) to see if our experiences even relate to them. Good luck.
18 notes
·
View notes
Text
Impact of Age on Depression and the Role of Psychiatrists in Recovery
#best psychiatric doctor in indore#de-addiction specialist indore#anxiety disorder treatment in indore#childhood disorder treatment in indore#childhood psychiatry problems treatment in indore
0 notes
Note
Hi Magz! I see a lot of debate about if autism is a disorder, a disease, or a "way of being". You're nonverbal and DSM/psych-critical, so I want to know your thoughts on autism's classification (if/when you're able)
Was think about this for some days,
but epistemology n label stuff wrt neuro-psychiatry is bit magz weakness when try words it.
Am not very enlighten voice of autism, n am in own little world which often have consequence when Magz try communicate ideas early.
Like, this too early for proper...
Am also have different experience of autistic people that unable speak since toddler, n they should be listen to also. So with disclaimer.
Regardless, am try:
when people call autism "way of being" - it often attempt reclaim way medicalization have dehumanize autistic people
when make monster of us by say "autism" something can n should be remove from person
which result in medical abuse, psychiatric abuse, interpersonal n parental abuse.
high rates abuse from caretakers, medical staff, n parents - especially when unable / not allow advocate for self.
so "autism is way of being" is direct response to that history - n cannot be remove from psychiatric context.
the consequence of do "way of being" do embed parts psychiatry into it as essential aspect of person, but is understandable why happen at least.
Keep in mind is the language that often available for layperson go against common reasonings for abuse.
but even if was not "way of being", the abuse that normal happen when autistic - should not.
so we need pin idea center "regardless anything, abuse should never happen nor there be class of people it ok do to" and "there systems n ideas in place that make abuse seem 'necessary' n enforce it or pressure as thing should do, n this should not happen - but it do happen"
-
with "disease", it have even more negative connotation - as well, can reinforce the need of "cure". which, again, become reasonings for abuse.
so many autistics are against that way call it, "disease".
especially when what define "autism" is many traits how people experience world, or outsider perspective of how autistics seem like.
so would, in essence, *become* calling the person and their needs - a disease.
n is often language that lead to eugenics logic: something that need be cleansed from population or forced out of person.
-
with "disorder" - unfortunately the limits of language n its history, make it so.
autism - and previously "childhood onset schizophrenia" - was coined within the bounds of neuro-psychiatry. n is informed by it.
an observation of behaviors n difficulties of function in early 20th century to 21st century, with comparison how "normal" children act
have cemented the label autism, as neurodevelopmental "disorder" (Autism Spectrum Disorder)
the personal experience n difficulties of the autistic individual is real, in sense of any other neuro-socio-biological thing can be
but the way of acknowledge it is through that medicalization
the pick of what pool of 'symptoms' are autistic, the observance of toddlers n children behaviors to 'notice' autism, what is consider normal n what not normal
sociologically n culturally - creating the consequences of what "not normal" mean bit-by-bit in more rigid terms;
thus defining what "average normal child" not need accommodation of n 'should not act like' through "not being autistic, not {many other 'disorder'}"
n biological definings, by working backwards on what people these overlap symptoms have in common when try search it - whatever can -
brain scan, gastrointestinal issues, patterns of regression, comorbidity conditions ...
n we can acknowledge this self-reinforcing aspect, n the inherent medical environment what 'autism' label came from
but as long as we live in this type society, with its hostility to 'autism' n layered lore intertwined
- even with it reference these idea, it have its particular use in language for know what these various circumstance are refer to n these various experience (which not same everyone but it approximate some type idea)
n sometimes (usually "low support needs") people are overeager with their criticism of psychiatry n medicalization, to remove language terms entirely or be picky
while give nothing of alternative or way express experiences for the silenced stigmatized autistics they rarely hear from
or try shut down. cuz they call themselves "high support needs" n "low functioning" for describe their reality of disability
thus, the silencing n narrowing words reinforcing that sort ableism against disabled anyway.
when the point n goal is to empower the persons most hurt by these systems oppression psychiatric, without patronize or silence - in whatever method can.
usually by question these systems authority n narratives they hold, but priority is of the people.
still, am not trust psychiatrists n medical people n such,
they done much horrible things to Magz n seem project own ideas onto self while focus on whatever label n not own person that am, n how am experience personally, n how environment n people are affect
so this experience inform own view
that it. whatever. it not any of those,
but a reality we live by anyway. whatever we call it. but some the terms have more consequence than other.
and am not know how say what want say, cuz like half the words jumble. so. this the best gonna get for now.
n am prolly say lil bit something way wrong way say it, than what meant, cuz it happen often but what can do ?
28 notes
·
View notes
Last Seen Blogs

chesspnoi-eaa
CHESSPNOI

shadowyvn
Untitled

privatemirkwoodparty
private mirkwood party.

yuuzi
yuuzi

samedaydch0
2.2 sell house fast for cash