#new nursing student
Text

#study motivation#studyabroad#studyinspo#studyspiration#studyspo#studystudystudy#studyvisa#italy#student life#study aesthetic#studygram#studying#study blog#the case study of vanitas#character study#study night#study nook#study nursing in new zealand#study notes
496 notes
·
View notes
Text
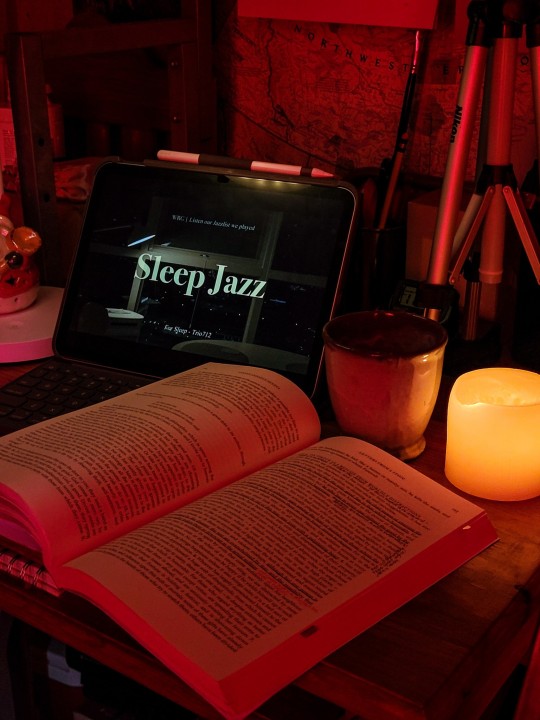
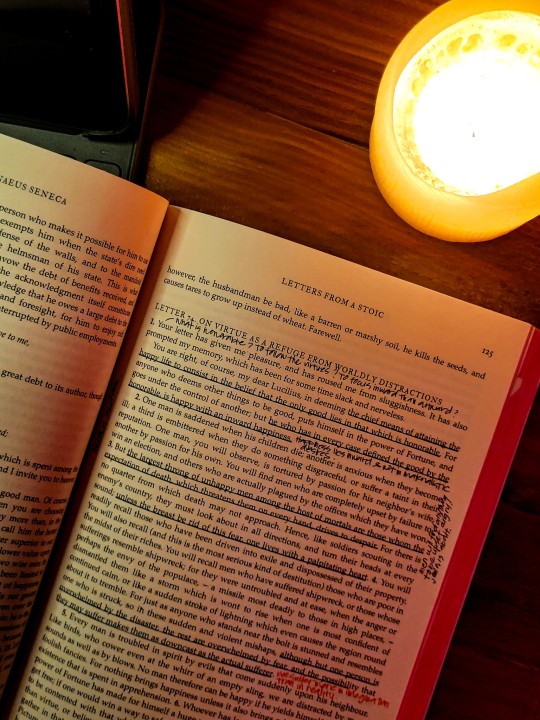
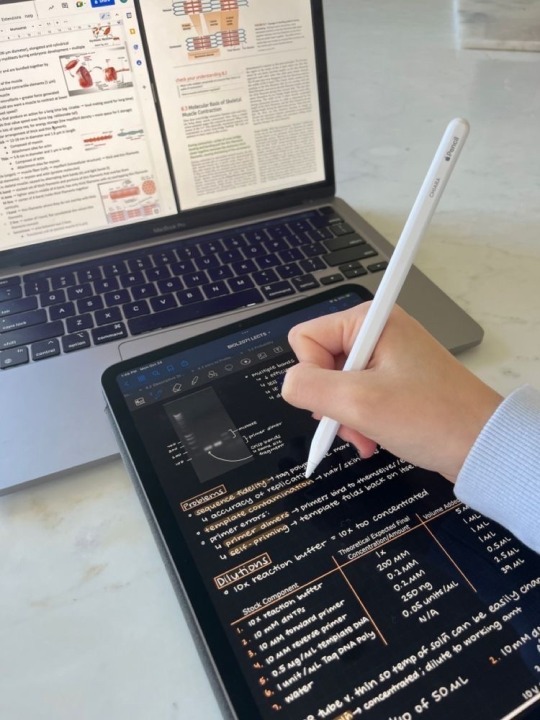
☕️ I brewed myself a cup of coffee and it tastes amazing - smooth, balanced, with a hint of chocolate. I’m annotating this passage from Letters From A Stoic, which I’ll be transferring to my Obsidian! I love how it allows me to link related notes and quotes. It’s quite helpful in looking back at previous notes + helps me get a bigger picture of a topic etc.
Not much tasks for today so I might just read (currently: Enchantment of Ravens), and probably watch Harry Potter. I’m kind of sad that my holiday break is almost over. But I feel like if it goes on, I’ll be bored to death!
🦋Grace
#Studyblr#New Studyblr#bookblr#Medblr#academia#100 days of productivity#chaotic academia#heydilli#myhoneststudyblr#aesthetic#Grace’s books#Books#Stoicism#Coffee#nursing student#living with adhd
102 notes
·
View notes
Text
Today marks the first day a nurse was so mean it made me cry.
Shoutout to the nice cleaning lady, my residents and my staff for making it more bearable ;-;
#I’m honestly surprised it took this long tbh#at least she doesn’t have any nursing students to torment#but i also saw her berating a new cna#and leaving another nurse alone with 16 patients for HOURS#lavanda speaks#personal
27 notes
·
View notes
Text

🩺 fall semester of sophomore year
manhattan, new york city
#studyblr#light academia#academiario#study mood#studyspo#study inspiration#nyc#nyclife#stem#pre nursing#dark academia#new york city#new york#studying#student#bujo#library#college#community college#study blog#study aesthetic#study motivation
289 notes
·
View notes
Text
i keep gettin degrees to procrastinate :3
#my school has an accelerated nursing program for graduate students#so u can get ur bachelors in 17 months#and i really think that’s my calling#so im going to apply to that#i feel like a whole loser bc ill be 24 w a degree that im not using#trying to get a new one lol but yeah#it’s going to be fucking tough but#i think i got it#idk#confused n scared n sad n lonely n anxious n all the things
15 notes
·
View notes
Text
if you are 1) currently in a university where your student healthcare covers hormone therapy, and 2) in a good financial, emotional, and social position to start hormone therapy, i would recommend pursuing it. because in my experience, it's a huge pain in the ass to get an endocrinologist once you're on your own
#unless you live near a planned parenthood or another equivalent to that#but in general you might as well take advantage of the mandatory student health insurance while you have it#it's also cheaper than you might expect. my vials cost $40 CAD for 4 months and then the injection materials are like a couple dollars each#for me i got a therapist with the university and asked them to recommend me to one of the uni's doctors#so i got to skip some of the waitlisting process yay#and then even after getting access to hormones i went to the clinic maybe 5 or 6 times because i needed a nurse to help me with injections#all of which was 'free' because it was with the university#now that i'm graduated though i need to find a new endocrinologist and it turns out the process is WAY more complicated on your own 🤡#of course your mileage may vary depending on how based your school is but it's definitely worth checking imo 🤷#beepbeep.txt#wanted to say this because i basically didn't use the uni health services until my last year and i was like 'wow#'i'm actually getting so much shit for free right now'#like i was seeing a therapist and a dietician and the endocrinologist and a nurse simultaneously at one point#and i might've missed out on all that if i didn't have someone tell me how easy it was to get help if you ask the right questions#so there's my word of wisdom for anyone who might benefit from it.......#also going to post tips about injections later because i think that would also help people out 👍
27 notes
·
View notes
Note
med student steve and nurse eddie who is sick of his shit please <3 from wip wednesday i know it's not wednesday anymore but plz
yessssss i love this AU so much because it's just me projecting onto steve and daydreaming about Eddie Munson, Certified Hot Nurse™
also don't worry i have very little free time and am also australian so for me, WIP wednesday is a state of mind, not an actual time frame lmao
Snippet for you under the cut!
Shaking off the black cloud currently hanging over him, Steve finally lays eyes on the person trying to get his attention. A nurse is leaning over the desk of the nurse’s station a few meters away to look straight at Steve, and– wow, okay. Steve knows damn well what his type is, the kind of person and style he goes weak in the knees for, but this guy is aggressively punching every single one of Steve’s buttons. He’s got dark, curly hair that’s done up in a bun, some small strands of hair hanging out to frame the guy’s face. It gives Steve an eyeful of the guy’s killer jawline and the jewellery glinting in his ears – studs, of course, they are on the job, but at a glance Steve can see at least a couple in each ear. The guy’s arms are spread out on the desk in front of him, and Steve can feel his brain freeze at the sight of dark ink poking out from under the guy’s scrubs. He forces himself to look up and away from those (tempting, deliciously tempting) arms and into the nurse’s face – and okay, that’s not much better. The way this guy is looking at him, big brown eyes locked onto Steve’s face, he feels like he’s getting sucked in.
“Sorry?” Steve says, taking a moment to blink and regain his composure. He hopes to God he doesn’t look as flustered and distressed as he feels. “Are you talking to me?”
“Yup,” the nurse says, popping the p. He gestures at the sample bag Steve’s holding, with a few different vials and one syringe of blood inside, as he continues. The smile he gives Steve is almost apologetic as he says, “Pathology isn’t going to take those bloods from you, sweetheart. Not like that, at least.”
“Excuse me?” Steve instinctively bristles at the pet name, the way it just drips off this guy’s tongue. Just like that, the black cloud is back. He crosses the distance over to the nurse’s desk. “What’s wrong with them? They’ve all been labelled properly, and signed.”
“Well…” The nurse says, drawing out the word. Steve feels himself start to frown, just the tiniest bit. “You left the needle on your blood gas.” With a couple of fingers, the nurse points to the offending syringe in Steve’s sample bag. Sure enough, the needle is still attached to the syringe full of blood, the sharp end embedded in a small piece of foam.
Steve frowns even deeper. “My intern told me it’s fine like this.”
“Yeah, that doesn’t surprise me.” The guy grins and rolls his eyes before giving Steve a ‘what can you do’ kind of expression. “It’s a common mistake to make, actually, since they don’t really explain this stuff officially, but-”
“Listen,” Steve interrupts, gritting out the word between his teeth. He’s sure this nurse, whoever he is, has more important things to do than patronize him. Steve sure as fuck isn’t going to stand here and be made fun of while this guy takes his sweet-ass time to get to his point. “I’m pretty sure my intern knows what they’re talking about, seeing as they’re, you know, a doctor. If you really want to be helpful”–Steve’s eyes flick down to read the nurse’s name badge–“Eddie, then you can point me in the direction of the specimen drop-off.”
Eddie actually rears back at that, straightening up and pulling his arms back so he’s holding on to the very edge of the desk instead of casually leaning over the top of it. If Steve were having a better day, he might feel bad about it. As it is, all Steve feels is a sick sense of satisfaction at the way Eddie’s face has shuttered off, his eyes no longer shining the way they were a moment ago.
“It’s that way,” Eddie says bluntly, pointing back in the direction Steve came. His voice has lost all the character, the theatricality that he spoke with a minute ago. “Turn left once you step out of this ward and follow that hallway straight down.”
“Thanks,” Steve says, trying very hard not to feel like an asshole. He almost succeeds.
Eddie just grunts in acknowledgement. He gives Steve a quick once-over and says, “Good talk,” in a tone that clearly states it was anything but.
As he strides off towards the specimen drop-off, Steve can’t help but agree.
#charlie writes things#medical steddie au#medical student steve harrington#nurse eddie munson#steddie#med student steve and nurse eddie au#<- haven't actually posted any snippets from this before so that's gonna be my new au tag#also i want to reassure you that steve is NOT trying to say doctors are smarter/better than nurses or anything like that#the point he's going for is 'surely someone who has graduated medical school after doing their schooling In This Hospital#knows what is and isn't allowed under the hospital policies'#and it gets. misconstrued *laughs evilly*#also this is not a 3 sentence snippet but as a wise individual once said 'fuck it we ball'
32 notes
·
View notes
Text
i don't think i should have to choose between burnout or barely scraping at the poverty line and yet. here we are
#this is not a new realization before anyone gets on my dick#i'm just currently moving from being a student with a side-gig to mostly being employed#so I'm more annoyed about it than usual#like yes i could work 40 hours/week and that'd give me like. maybe 300 bucks of disposable income#but also i don't hate myself that much#like. just. a 30-hour week should be livable#instead of making me consider taking on a second side-gig i can do from home#like generally for so-called 'unskilled' labour#but ESPECIALLY considering that I'm like. yk. a Social Worker/Nurse#ANYWAY#fuck capitalism etc etc#mona rambles
45 notes
·
View notes
Text
the truth is im not sure if any other towns with ivy leagues in them tend to have the hatred and resentment for the school that ppl from new haven often have for yale. id love to just sit down and chat with someone from another ivy league town bc like. is it just the combo of a school full of very rich prep school kids in one of the poorest areas in the state where our public schools literally does not have the funding or curriculum for a lot of students to qualify for the college in their own fucking town or is this a wider issue in other places
#a childhood friend of mine just started at yale and im happy for her#but it makes me want to scream bc her mom works at yale she’s from new haven and there is literally a program here that is supposed to#give severly reduced or free tuition to new haven residents but apperantly they stopped doing that shit in her lifetime#so she has to pay full price and theyre making her live on campus despite living pretty much on campus already#hhhh im so fucking tired of this shit#her mom sent my mom this letter they got about how they should be careful about their kids being in new haven because its so dangerous and#scary and theres homeless people here oh my god!! there was literally a skull and crossbones on it#im so tired of this culture of yaleies being like ‘we want to reduce the distance between yale students and new haven residents!!’ but we’re#not the fucking problem. im thrilled about how much money yale brings in. we get an ikea and nice resteraunts bc of it#and nice museums and theatres and shit#but still our school system is on the list of the poorest in the country#my mom’s school literally cannot afford a school nurse or a counceler#i feel like maybe if yale wants to bridge the gap they should make it possible for people from this city to attend there#like. maybe they could start a program where kids from new haven could get reduced yale tuition? wait they already did that and they fucking#got rid of it for no reason
19 notes
·
View notes
Photo

Student nurses at New York Hospital having tea on the roof of the Nurses' Residence, 1920s.
Photo: New York-Presbyterian Hospital via Artstor
#New York#NYC#vintage New York#1920s#nurses#student nurses#tea#roof#rooftop#afternoon tea#Washington Heights
174 notes
·
View notes
Text


#studyabroad#study motivation#italy#studyinspo#studyspiration#studyspo#studystudystudy#studyvisa#student life#study aesthetic#study japanese#study tips#studybrl#study studyblr#study nursing in new zealand#study korean#study blr#study in singapore#studyblr#study shows#study life#the case study of vanitas#study notes#study hard#studygram#studying#study blog#study journal#study beats#study bunny
240 notes
·
View notes
Text
Nothing in my day-to-day job shows me the limits of modern medicine like vancomycin does. And it makes me insane.
(extremely long, somewhat incoherent nerd rant below the cut)
See, vanc is really good at, like, three things: treating MRSA (when given IV), treating ampicillin-resistant enterococcus (when given IV), and treating c diff (when administered orally ONLY). Most every use outside of that, like when it’s used to treat methicillin-susceptible staph aureus for “penicillin allergic patients” (don’t get me started on PCN allergies), actually has data that it increases risk of morbidity and mortality (i.e. harm and DEATH).
Unfortunately, due to the prevalence of multi-drug resistant organisms, vancomycin is empiric therapy for a lot of presumed infections. And it's a lot more difficult to actually tell if someone has an infection than you'd think. A lot of medical conditions imitate each other and when time is of the essence to identify what's going on, the most ethical thing is to start an antibiotic and rule out infection as the hospitalization continues. Lab techniques have gotten a lot quicker: I can remember 8 years ago, it would take 3 days just to identify what microbe the patient had in their presumed infection. These days, anno domini 2023, PCR comes back in a matter of hours, identifying gram positive/gram negative staph/strep/bacilli/etc, and it's the sensitivities that take 2-3 days. (Don't get me started on contaminated cultures.) But even with improvements in lab technique, we might not culture any microbe at all or the provider might keep vancomycin on "just in case" because we don't know IF the patient is infected, WHAT they're infected with, or if the infection will get better with a different drug.
And vancomycin is terrible on kidneys. Extremely nephrotoxic. It isn’t as bad as the 80s when the drug first came out and was called Mississippi Mud colloquially, but it will fuck the patient up if not monitored closely.
But finding the correct dose for each patient in a timely manner is nigh impossible. This is because vancomycin is renally eliminated. We have to mathematically estimate how well the kidneys are working. Unfortunately, our mathematic equation is next to useless if you are:
-Less than 50 kg
-Shorter than 5 foot tall
-Have a BMI of more than 40
-Are an adult younger than 45 (twenty-year-olds get astronomical doses that would be destructive in an older patient)
-Are older than 65 (the official definition of 'geriatric', i'm relatively sure)
-Are female (this is really only applicable if the patient is less than 50 kg or older than 65 - think: little old frail lady - we have absolutely no fucking idea how their kidneys are doing until we order the serum drug level. It is next to impossible to accurately dose vancomycin in little old ladies on the first try.)
-Are missing limbs (lots of leg amputations in the older and impoverished diabetic population!!)
-Have a lot of muscle mass (think bodybuilder or really tall guys)
Fun fact: we estimate renal function by looking at height, weight, age, birth gender (few, if any, studies on trans patients taking HRT), and a lab value called serum creatinine. Creatinine is a byproduct of muscle metabolism, I don't know the fine details, but we can generally estimate how well kidneys are working by seeing how much creatinine is in the blood: low creatinine usually means kidneys are excreting it as they 'should' be. High creatinine means there's something wrong, the kidneys aren't able to excrete it as efficiently as they 'should' be. But the effect of low muscle mass and high muscle mass haven't been studied enough to be able to adjust our mathematical equation to compensate for them. And with high BMI: we often overestimate their renal function because we don't know how to estimate their muscle mass vs their body fat.
(I work out in the boonies. ~70% of our patients have diabetes. ~80% of our patients have a BMI of greater than 35. So what I'm trying to say here is: we are shooting in the fucking dark when we're estimating the renal function of the vast majority of our patients.)
Complicating this: vancomycin is useless until it reaches steady-state concentration in therapeutic range. On one side of this problem: a lot, if not most, medical providers assume that vancomycin starts working its magic from the first dose. So we sometimes get orders for "vancomycin 1 gram now and see how the patient is doing in the morning". That isn't going to solve jack shit! That's just going to increase the incidence of microbial resistance!!
OR, like in the multiple situations I dealt with this afternoon, you make an educated guess on what regimen is going to work for the patient. You get a level 48 hours after the dose starts. And you find out that you fucking guessed wrong and the patient is subtherapeutic. It has been two fucking days and the patient hasn't started being treated for their (presumed) infection yet!! And we've increased the possibility of microbial resistance! *muffled screaming in frustration*
So what I'm trying to say here is: on almost every presumed infection that comes into the hospital (which we're guessing like 30%? 50%? of the time), we're starting an extremely toxic drug, oftentimes 100% guessing what regimen will be therapeutic, only finding out in 2 days that it is not therapeutic, and it can sometimes take days and days to titrate the dose sufficiently to find a therapeutic regimen. And sometimes we're really fucking unlucky and we destroy the patient's kidneys temporarily (or permanently! but kidneys can be very resilient so that's thankfully rare) because we guessed a regimen that's too high!! This is a fucking nightmare!!!!!!!!
And if all of this wasn't bad enough, we don't really have any drugs that do what vancomycin does therapeutically. We have things that can be used to cover some of what vancomycin does, but nothing that's equivalent AND less toxic.
Like, to fix this situation, we need:
-Better education to providers on what drugs are appropriate empiric therapy for different presumed infections (we're working on it, we are working on it)
-Better ways to estimate kidney function (there needs to be more research on kidney function in patients with BMI greater than 35!! And little old ladies!! And patients with low body weight and high body weight and amputations and...)
-Better prognostic tools to tell 1. when the patient is infected (looking at you, sepsis!!!) 2. what they're infected with
-Less-toxic antibiotics AND/OR better ways to treat infection (this would be the evolution of medicine as we know it)
And I want to be clear: vancomycin isn't bad. It's an extremely effective tool when used correctly but we often either don't have enough data to use it correctly or the provider doesn't understand that this tool is fucking useless for the job they're trying to perform.
#some days i'm just smacked in the face by the limits of modern medicine#there is so much we don't know!!!#we're doing the best we can!!!#negativity#personal#us healthcare#i understand other hospitals will have a different experience than this#but my corporation is extremely stingy and we get all the new grads#so educating providers and nurses is a never-ending wheel at my facility#and we don't treat anything complicated except orthopedic surgeries#some days I just get overwhelmed by how little we know#if you can guess my profession on the first try please keep it to yourself i'm trying to maintain a low profile here okay#also if you ask me medical questions don't expect an answer#i was a Cs Get Degrees student all I know i've learned on the job and I don't know shit
6 notes
·
View notes
Text
i left my internship back in february and i feel soooo much better
#the environment got so toxic after the new student nurses came in at the end of last year i just couldn’t deal with it anymore#i’m back at my previous job until i can find something else but i’m in no rush#salo.exe
4 notes
·
View notes
Text
I have a pharmacology exam on Wednesday and I would love nothing more than to slip into the abyss (cool weather and cozy blankets, candles and soft rain) and still get an A on the exam tbh
#but no!!!#I just HAD to be an academic weapon#and had to choose an rigorous and challenging major#-> me when my challenging major is challenging me: :((#moral of the story is that there are so many drugs to help you start pooping or stop pooping. so many to choose from & so many to know#there are even MORE drugs to help you not be sad. SO MANY.#also! if you're at risk for thromboembolisms#good news for you buddy#there are also SEVERAL DRUGS TO CHOOSE FROM#(several drugs that nursing students have to learn)#sometimes I wanna talk to the dean and be like “have you considered this: I'm just a girl. I'm literally just a girl”#shut up lauren
2 notes
·
View notes
Text
nurses love me for my paper-mache skin and entirely visible cardiovascular system
#never been in this hospital before so I was once again flocked by student nurses#they always take so much blood 💀 anyway#some terrible news I need to have a cerebral angiogram#I do not even want to think about it I’m going to get mcdonalds and go home and nap
3 notes
·
View notes
Text
I'm actually disappointed that hospitals aren't haunted by benevolent spirits. Spirits that have no qualms about interacting with patients & staff. Spirits who know a living patient is gonna start circling the drain before any of the staff, and alert them. Spirits who died from a medical mistake warning nurses & doctors if they're going to make that mistake again. Spirits who show up to help hospice and dying patients transition without fear. And hell, even the curmudgeonly but harmless ghost of ol' Mr. George still occassionally setting the bed alarm off in one specific room & grumbling about having to pee even though he always had a Foley.
I just think that would be nice. As long as we don't have the ghost of Karen or Kyle hitting the call bell every 60 seconds & screaming they're out of ice while throwing the pitcher at you
#ghost doctors who didn't die at the hospital but were there so much their spirit is still attached to it#ghost ortho surgeon bros giving residents a hard time#kind ghost nurses helping precept students and new nurses#ghosts#haunting#haunted#nursing#nurse#medicine#medical#hospital#haunted hospital#friendly ghost#medical humor
7 notes
·
View notes
Last Seen Blogs

theamityelf
Take a deep breath; relax your shoulders

armn09
Untitled

phantom-angst-obsession
Ghost Torture but not the bad kind™

jacobjay91
welcome to my world of my feet, and other's too!

drugslaced
Untitled