#speaking out
Text
Cinder feels kinda like this generations Morro so let’s see what happens
134 notes
·
View notes
Note
Thank you for everything, but in particular for fighting and exposing people that think that narcissistic abuse does not exist and that we're somehow ableist towards those absolute monsters!! They should be ashamed and go back to the sewers they belong in.
Never give up, because we won't either!! ♡
Haha okay I wouldn't say anyone needs to go to the sewers for being manipulated, if someone realizes they've been wrong about something, that's okay and it's okay to just say sorry and be forgiven.
I know it's really hard to deal with people who continually harass us for speaking out against abuse, but it's better to go against the source of the abuse, the narcissist, rather than to divert attention to those who've been naive and trusting enough to fall for their lies. The narcissists also prefer if people who've been manipulated by them get in fights, rather than uniting against the person who started all of the problems.
I also suspect a lot of these 'well meaning people telling us we're not allowed to speak about narcissistic abuse' were just narcissists themselves, acting. They love playing around with making multiple accounts and pretending there's this whole community of support for them, when it's just a bunch of sock puppets who scream very loudly. There's actually a lot more of us than there is of them, and if we stood strong together, we would easily dismantle their manipulation and remove the fear of harassment they've spread around the place.
I won't give up! Victims of narcissistic abuse deserve a safe space and not to be harassed for speaking out, or to be shamed and accused for watching out and trying to protect others from abuse.
36 notes
·
View notes
Text
I'm regards to my post of a Prothonotary Warbler I recently made a post on Instagram (@introvertedswimmer_photography) where I talked about this endangered species. Here's what I had to say:
Love these cute little Prothonotary Warblers. Despite them being an endangered species under Canada's Species at Risk Act and Ontario's Endangered Species Act, I have seen this bird multiple time in my over 10 years birding career. As someone who always looks forward to seeing this adorable bird yearly, I cannot imagine spring birding without it. Habitat destruction and the draining of the forested swamps is resulting in habitat loss and the decline in these birds. I am calling everyone to help to revive habitats for these beautiful cute birds to prevent them from going extinct and becoming just a memory. Please spread the message and talk to people about this habitat destruction.
#ontario#original photographers#nature#nature photography#beautiful#bird photography#walking in nature#birdblr#birding#birds of north america#bird watching#bird#birds#birdwatching#birbs#birbs of tumblr#birblr#endangered#awarness#speaking out#bird art#warbler#prothonotary warbler#endangered species#cute#love#spread the message
11 notes
·
View notes
Text
Speaking Out and Sharing my experiences with Robo/Morgyn/Sage in full (TW)
Hello everyone, this is a serious post so please take it very seriously!
Here, this will be the first time that I will publicly speak out fully of the truth about one of the most horrible people that I have met, Robo/Morgyn/Sage. I used to be friends with them, but they hurt me and many others, so I don't want to associate with the gang anymore. This is also the first time I have ever call out someone or expose them publicly and he and the gang are still out there somewhere, but most of us are DONE with them and we don't trust them anymore.
Since the post is a little long, I would recommend reading the important sections (Incidents, 26th May 2022, Aftermath, Finding Out the Truth and My Advice), but if you want to read the whole thing, you can.
If anything happens to anyone, I will take full responsibility since call outs are a big deal and I care about other people's safety and wellbeing and I'm putting my career and myself in danger for the truth to be officially out and hopefully, we can fully move on and forget and Robo/Morgyn/Sage and his gang will be hold accountable of what they have done to most of us, including myself.
#call out tw#call out post#speaking out#serious post#janae talks#janae speaks#cutejk123 talks#cutejk123
29 notes
·
View notes
Text
"I Was Told to Approve All Teen Gender Transitions. I Refused."
Via The Free Press:

Perhaps you read the long investigation about detransitioners published in this weekend’s New York Times. It is comprehensive and sober and we highly recommend it.
It’s also a piece we are confident would never have made it into the paper were it not for independent publications like ours taking the journalistic and reputational risk over the past few years to pursue the subject of “gender-affirming” care and the subsequent harms inflicted on vulnerable young people. In this, we are proud to stand alongside Hannah Barnes, Lisa Selin Davis, Hadley Freeman, Helen Joyce, Leor Sapir, Abigail Shrier, Jesse Singal, Kathleen Stock, Quillette and others, who took the arrows so that the mainstream press could finally start reporting on what’s really happening.
What is immensely clear is that individual testimonies—whistleblower accounts like those we’ve published by Jamie Reed and Dr. Riittakerttu Kaltiala—have made the change we are now beginning to see.
And that change is now impossible to deny: witness the arrival of lawsuits from young people who say they have suffered the consequences of these life-altering treatments.
Today, therapist Tamara Pietzke adds her voice to those of our other whistleblowers, and tells how she could no longer go along with the pressure to transition her patients.
By Tamara Pietzke
February 5, 2024
For six years I worked at a hospital that said all teenagers with gender dysphoria must be affirmed. I quit my job to blow the whistle.
I know from firsthand experience what hard times are. Though I had a happy childhood, raised as the middle child by working-class parents in Washington State, my mom died of ovarian cancer when I was 22.
After that, my family fell apart. I felt lost and alone.
I decided to become a therapist because I didn’t want anyone to go through what I had, feeling like no one on this planet cares about them. At least they can say their therapist does.
I earned my master’s in social work from the University of Washington in 2012, and I have worked as a therapist for over a decade in the Puget Sound area. Most recently, I was employed by MultiCare, one of the largest hospital systems in the state.
For the six years I was there, I worked with hundreds of clients. But in mid-January, I left my job because of what I will go on to describe.
The therapeutic relationship is a special one. We are the original “safe space,” where people are able to explore their darker feelings and painful experiences. The job of the therapist is to guide a patient to self-understanding and sound mental health. This is a process that requires careful assessment and time, not snap judgments and confirmation of a patient’s worldview.
But in the past year I noticed a concerning new trend in my field. I was getting the message from my supervisors that when a young person I was seeing expressed discomfort with their gender—the diagnostic term is gender dysphoria—I should throw out all my training. No matter the patient’s history or other mental health conditions that could be complicating the situation, I was simply to affirm that the patient was transgender, and even approve the start of a medical transition.
I believe this rise of “affirmative care” for young people with gender dysphoria challenges the very fundamentals of what therapy is supposed to provide.
I am a 36-year-old single mother of three young kids all under the age of six. I am terrified of speaking out, but that fear pales in comparison to my strong belief that we can no longer medicalize youth and cause them potentially irreversible harm. The three patients I describe below explain why I am taking the risk of coming forward.
Last spring, I started seeing a new client, who at 13 years old had one of the most extreme and heartbreaking life stories I’ve ever heard. (For the sake of clarity, I am referring to all patients by their biological sex.)
My patient’s mother has bipolar disorder and was so abusive to my patient that the mother was given a restraining order. My patient was sexually assaulted by an older cousin, by one of her mother’s boyfriends, and also once at school by a classmate. Her diagnoses include depression, PTSD, anxiety, intermittent explosive disorder, and autism. She is being raised by her mother’s ex-boyfriend (not the one who assaulted her).
The year before I started seeing her, when she was 11, she was hospitalized for talking about committing suicide. Later that year, a pediatrician diagnosed her with gender dysphoria after she started to question her gender. The pediatrician referred her to Mary Bridge Children’s Gender Health Clinic, whose clinicians recommended she take medicine to suppress her periods and that she think about starting testosterone.
Mary Bridge, MultiCare’s pediatric hospital, runs the gender clinic for minors and employs nurses, social workers, dietitians, and endocrinologists, who provide gender-affirming care, which includes prescribing hormones to young patients who question their gender. In order to get that prescription, patients first need a recommendation letter from a therapist. Because Mary Bridge is a part of MultiCare, their patients were often referred to therapists like me who were in their system.
In an April 2022 blog post, a Mary Bridge social worker wrote that the gender clinic’s referrals increased from less than five a month in 2019 to more than 35 a month in 2022. In May 2022, the clinic received a $100,000 donation from Patient-Centered Outcomes Research Institute “to study health care disparities” in transgender youth.
The clinic operates in Washington, one of the states with some of the most lenient legislation on gender transition for youth. In May 2023, the state legislature passed a law guaranteeing that youth seeking a medical gender transition can stay at Washington shelters—and the shelters are not required to notify their parents.
Because of my patient’s autism, it was difficult for us to engage in introspective conversations. During our first visit, she came over to my desk to show me extremely sadistic and graphic pornographic videos on her phone. She stood next to me, hunched over, hyper-fixated on the videos as she rocked back and forth. She told me during one session that she watched horror and porn movies growing up because they were the only ones available in her house.
She showed up to our therapy sessions in disheveled, loose-fitting clothes, her hair greasy, her eyes staring down at the ground, her face covered by a Covid mask almost like a protective layer. She went by a boy’s name, but she never raised gender dysphoria with me directly—though one time she told me she would get mad at the sound of her own voice because “it sounds too girly.” When I asked her how she felt about an upcoming appointment at the gender clinic, she told me she didn’t know she had one.
In between scrolling through videos on her phone, she told me how she cried every night in bed and felt “insane.” She described a time when she was eight years old and her mother nearly killed her sister. She remembered her mother being taken away. At times, she would “age-regress,” she told me, by watching Teletubbies and sucking on pacifiers.
When she started seeing me, she had recently threatened to “blow up the school,” which resulted in her expulsion.
I knew I couldn’t solve all of her problems, or make her feel better in just a few therapy sessions. My initial goal was to make her feel comfortable opening up to me, to make the therapy room a place where she was heard and felt safe. I also wanted to try to protect her from falling prey to outside influences from social media, her peers, or even the adults in her life.
With a patient like this, with so many intersecting and overwhelming problems, and with such a tragic history of abuse, it took our first three sessions to get her feeling more comfortable to even talk to me, and to understand the dimensions of her problems. But when I called her guardian last fall to schedule a fourth appointment, he asked me to write her a letter of recommendation for cross-sex hormone treatment. That is, at age 13, she was to start taking testosterone. Such a letter from me begins the process of medical transition for a patient.
In Washington State, that’s all it takes—a few visits with a therapist and a letter, often written using a template provided by one’s superiors—for minors to undergo the irreversible treatments that patients must take for a lifetime.
I was scared for this patient. She had so many overlapping problems that needed addressing it seemed like malpractice to abruptly begin her on a medical gender transition that could quickly produce permanent changes.
The MultiCare recommendation letter Tamara was given for approving the medical treatment of minors with gender dysphoria. I emailed a program manager in my department at MultiCare and outlined my concerns. She wrote back that my client’s trauma history has no bearing on whether or not she should receive hormone treatment.
“There is not valid, evidenced-based, peer-reviewed research that would indicate that gender dysphoria arises from anything other than gender (including trauma, autism, other mental health conditions, etc.),” she wrote.
She also warned that “there is the potential in causing harm to a client’s mental health when restricting access to gender-affirming care” and suggested I “examine [my] personal beliefs and biases about trans kids.”
When Tamara outlined her concerns about giving a patient testosterone to her manager at MultiCare, she was told to “examine your personal beliefs and biases about trans kids.” She then reported me to MultiCare’s risk management team, who removed my client from my care and placed her with a new therapist.
I shouldn’t have been surprised by this. Just a few months earlier, in September of last year, I was one of over 100 therapists and behavioral specialists at the MultiCare hospital system required to attend mandatory training on “gender-affirming care.”
As hard as it is to believe given my work, I hadn’t heard about gender-affirming care before that moment. I needed to know more. So each night in the week leading up to the training, I searched online for information about gender-affirming care. After putting my kids to bed, I sat glued to my computer screen, losing sleep, horrified at what I found.
I discovered that neither puberty blockers nor cross-sex hormones (testosterone or estrogen) were approved by the Food and Drug Administration as a treatment for gender dysphoria. In fact, prescribing these treatments to kids can have drastic side effects, including infertility, loss of sexual function, increased risk of heart attack, stroke, cardiovascular disease, cancer, bone density problems, blood clots, liver toxicity, cataracts, brain swelling, and even death.
While gender clinicians claim hormonal treatment improved their patients’ psychological health, the studies on this are few and highly disputed.
I found that those experiencing gender dysphoria are up to six times more likely to also be autistic, and they are also more likely to suffer from schizophrenia, trauma, and abuse.
A risk manager’s job is to minimize the hospital’s liability, but in my case, they deemed that my concerns posed a greater risk to my client than giving her a life-altering procedure with no proven long-term benefit.
I shouldn’t have been surprised by this. Just a few months earlier, in September of last year, I was one of over 100 therapists and behavioral specialists at the MultiCare hospital system required to attend mandatory training on “gender-affirming care.”
As hard as it is to believe given my work, I hadn’t heard about gender-affirming care before that moment. I needed to know more. So each night in the week leading up to the training, I searched online for information about gender-affirming care. After putting my kids to bed, I sat glued to my computer screen, losing sleep, horrified at what I found.
I discovered that neither puberty blockers nor cross-sex hormones (testosterone or estrogen) were approved by the Food and Drug Administration as a treatment for gender dysphoria. In fact, prescribing these treatments to kids can have drastic side effects, including infertility, loss of sexual function, increased risk of heart attack, stroke, cardiovascular disease, cancer, bone density problems, blood clots, liver toxicity, cataracts, brain swelling, and even death.
While gender clinicians claim hormonal treatment improved their patients’ psychological health, the studies on this are few and highly disputed.
I found that those experiencing gender dysphoria are up to six times more likely to also be autistic, and they are also more likely to suffer from schizophrenia, trauma, and abuse.
The research also implies that the dramatic rise in these diagnoses across the West likely have a strong element of social contagion. In children ages 6 to 17, there was a 70 percent increase in diagnoses of gender dysphoria in the U.S. from 2020 to 2021. In Sweden there was a 1,500 percent increase in these diagnoses among girls 13–17 from 2008 to 2018.
Yet, countries that were once the pioneers of gender transition medicine are now starting to backtrack. In 2022, England announced it will close its only gender clinic after an investigation uncovered subpar medical care, including findings that some patients were rushed toward gender transitions. Sweden and Finland undertook comprehensive analyses of the state of gender medicine and recommended restrictions on transition of minors.
I decided—though it was potentially dangerous to my career and to me—to ask questions about the findings I discovered.
The training I attended laid out an affirming model of gender care—from pronouns and “social transition” to hormone treatments and surgical intervention. In order for children to be diagnosed with gender dysphoria, the training stated, patients must meet six of eight characteristics, ranging from “a strong desire/insistence of being another gender” to “strong preference for cross-gender toys and games.”
Tamara and her MultiCare colleagues were trained to diagnose gender dysphoria among their young patients when they met six of the eight above characteristics. It was made abundantly clear to all in attendance that these recommendations were “best practice” at MultiCare, and that the hospital would not tolerate anything less.
When the leader of the training brought up hormone treatments, I shakily tapped the unmute button on Zoom and asked why 70 to 80 percent of female adolescents diagnosed with gender dysphoria have prior mental health diagnoses.
She flashed a look of disgust as she warned me against spreading “misinformation on trans kids.” Soon the chat box started blowing up with comments directed at me. One colleague stated it was not “appropriate to bring politics into this” and another wrote that I was “demonstrating a hostility toward trans folks which is [a] direct violation of the Hippocratic Oath,” and recommended I “seek additional support and information so as not to harm trans clients.”
In the training, gender-affirming treatment is presented as “suicide prevention.” As soon as I closed my laptop, I burst into tears. I care so deeply about my clients that even thinking about this now makes me cry. I couldn’t understand how my colleagues, who are supposed to be my teammates, could be so quick to villainize me. I also wondered if maybe my colleagues were right, and if I had gone insane.
Later, my boss reached out to me and told me it was “inappropriate” of me to raise these questions, telling me that a training session was not the proper forum. When I tried to present the evidence that caused me concern—the lack of long-term studies, the devastating side effects—she told me she didn’t have time to read it.
“I am speaking out because nothing will change unless people like me blow the whistle,” Tamara writes. “I am desperate to help my patients.” In retrospect, this ideology had been growing in power for a long time.
I remember in 2019 seeing signs of how gender dysphoria arose among many of my most vulnerable female clients, all of whom struggled with previous psychological problems.
In 2019, I started seeing a 16-year-old client after her pediatrician referred her to me for anxiety, depression, and ADHD. When I first met her, she had long blonde hair covering her eyes, to the point you could barely see her face. It was like she was going through the world trying to be invisible.
In 2020, during the pandemic, she told me she had started reading online a lot about gender, and said she started feeling like she wasn’t a girl anymore.
Around this time, her anxiety became so debilitating she couldn’t leave her house—not even to go to school. After taking a year off school during the pandemic, she enrolled in an alternative school for kids struggling with mental health. I was relieved that she was making friends for the first time, and seemed to be feeling a lot better.
Then she started using they/he pronouns, identified as pansexual, and replaced the skirts and fishnet stockings she often wore with disheveled and baggy clothes. Her long hair became shorter and shorter. She started wearing a binder to flatten her breasts. She tried out a few different names before settling on one that’s gender neutral.
The official diagnosis I gave her was “adjustment disorder”—an umbrella term often applied to young people who are having a hard time coping with difficult and stressful circumstances. It’s the type of diagnosis that doesn’t follow a child forever—it implies that mental distress among kids is often transient.
She came out as transgender to her family in 2021. Her mother was supportive, but her dad wasn’t. Regardless, she went to her pediatrician seeking a referral to a gender clinic.
In 2022, she went to Mary Bridge Children’s Gender Health Clinic for the first time, where the clinicians informed her and her parents that if she didn’t receive hormone replacement therapy, she could be “at increased risk for anxiety, depression, and worsening of mental health/psychological trauma,” according to her patient records. Her dad refused to start his daughter on testosterone, and so all the clinic could do was prescribe birth control to stop her period due to her “menstrual dysphoria,” or distress over getting her period. Which is something I thought all teenage girls experienced.
Five months later, she swallowed a bottle of pills and her mother had to rush her to the emergency room.
By early 2023, my client logged on to our weekly session, which we started doing by Zoom, and she told me she identified as a “wounded male dog.” She explained to me that this was her “xenogender,” a concept she had discovered online, which references gender identities that go “beyond the human understanding of gender.” She said she felt she didn’t have all of the right appendages, and that she wanted to start wearing ears and a tail to truly feel like herself.
I was stunned. All I could do was silently nod along.
After the session, I emailed my colleagues looking for advice. “I want to be accepting and inclusive and all of that,” I wrote, but “I guess I just don’t understand at what point, if ever, a person’s gender identity is indicative of a bigger issue.”
I asked them: “Is there ever a time where acceptance of a person’s identity isn’t freely given?”
The consensus from my colleagues was that it wasn’t a big deal.
“It sounds like this isn’t something that’s ‘broken,’ ” one colleague wrote me back, “so let’s not try to ‘fix’ it.”
“If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” she continued. “I might think it’s weird, but then again, not my life.”
After learning that one of Tamara’s patients identified as “a wounded male dog,” a colleague replied: “If someone told me they use a litterbox instead of a toilet and they were happy with it and it’s part of their life that brings them fulfillment, then great!” I was baffled and alarmed by her unquestioning affirmation. At what point does a change in identity represent a mental health concern, and not something to be celebrated and affirmed? Fortunately, my client never brought up her “xenogender” again. She also isn’t on testosterone due to her father’s disapproval. So I kept these thoughts to myself, and ultimately, in order to keep my job, I let it go.
Another female patient, who transitioned as a teen, serves as a warning of what happens when we passively accept the idea that gender transition will entirely resolve a patient’s mental health issues.
This client, who I started seeing in 2022, is now 23 and rarely leaves the house, spends most of the day in bed playing video games, and envisions no path to working or functioning in the outside world due to a variety of mental health problems. In 2016, this patient was diagnosed with autism, anxiety, and gender dysphoria. Later the diagnoses grew to include depression, Tourette syndrome, and a conversion disorder. In 2018, at age 17, the Mary Bridge Gender Health Clinic prescribed testosterone, despite the fact that this patient is diabetic and one of the hormone’s side effects is that it might increase insulin resistance. The patient’s mother, who has another transgender child, strongly encouraged it.
This patient now has a wispy mustache and a deepened voice, but does not pass as male. It turns out that testosterone, which will be prescribed for life, did not relieve the patient’s other mental illnesses.
My biggest fear about the gender-affirming practices my industry has blindly adopted is that they are causing irreversible damage to our clients. Especially as they are vulnerable people who come to us at their lowest moments in life, and who entrust us with their health and safety. And yet, instead of treating them as we would patients with any other mental health condition, we have been instructed—and even bullied—to abandon our professional judgment and training in favor of unquestioning affirmation.
I am speaking out because nothing will change unless people like me—who know the risks of medicalizing troubled young people—blow the whistle. I am desperate to help my patients.
And I believe, if I don’t speak out, I will have betrayed them.
(note: previously posted this with a lot of repetition because of copy/pasting. This is the fixed version. But if you see any repetition or mistakes please let me know!)
#trans#whistle blower#sex not gender#gender critical#lgb#speaking out#long post#long article#gender affirming madness#trans madness#trans and autism
11 notes
·
View notes
Text
"Only white jews are allowed to live in Israel"
Well
A Jewish sophomore at Colombia University:
Nigerian man in Tel Aviv:
Iraqi man (message of peace and support):
I know nothing about this person, honestly, but he explains
Israelis black life matter:
#israel#hamas#palestine#gaza#antisemitism#i/p#i/p conflict#jumblr#hamas is isis#free gaza from hamas#poc#jews of color#people of color#speaking out#Nigerian#iraqi#israeli arabs#Israeli#lybia#apartheid
11 notes
·
View notes
Text
My Thoughts on Palestine.
I am 22 years old. Born in Texas to a Christian family. I was raised in a church that is a god-fearing, hellfire, and damnation type of church. Growing up I was put in my church’s school and they taught me everything about the Bible. But I didn’t always listen in fact I would question everything since I had a curious mind. Sometimes they answered my questions and sometimes they didn’t. I was active in the church and tried to listen to sermons. I wanted to be a good Christian girl and listen.
There is one sermon that I remember. It was during the 9/11 memorial that my church had and my Pastor was speaking about 9/11 and then it turned to speaking about Muslims. I remember I was drawing, I know “good Christian girl”. I got a lil bored but I remember this. I was 6 years old, my pastor on the pulpit saying “The only way to save a Muslim is to give them a Bible or shoot them in the head.” I remember the other men in the church yelling “Amen! Amen!” I didn’t know what that meant until I got older.
I was raised with a strong hatred for Muslims. All Muslims. Any Muslims. “Remember 9/11, remember what they did.” Is what my father said like as if they personally attacked my family even though we lived in a suburban area in Houston, Texas. I hated anything to do with Muslims and the Muslim religion. When I was old enough to understand what was happening in Afghanistan, I was about 14 years old, I remember a student alongside me said “We should just blow up all the Muslims there.” And I thought “but what about the kids?” I didn’t say anything I just nodded my head and agreed with the student.
I got Instagram against my parents wishes. Scrolling through countless videos and then I saw some Muslims on there. Men, woman, and children. Just like me only different in religion. I still hated them but I wanted to learn about them. I still hated them but I wanted to understand them. I still hated them… I still hated them because I was taught to hate them. That little seed of “Why do I hate them?” Was growing.
Eventually I left that church when I was 16 years old which lead to me no longer be a Christian. Mind you not because I couldn’t stand what they believed about Muslims or because of the hypocrisy of my church. No I was no longer a Christian because I was bitter about my family divorcing.
Being on my own without the church breathing down my neck and telling me what I should or should not believe left me confused. So I started going on Instagram more and more and you know what got me to start thinking without the lenses of the church? Abortion and a woman’s right to choose. Argued a lot with my family until eventually my siblings started siding with me. It took a VERY long time for me to make my own choice, to make my own decisions of what I should believe. And that’s what has lead me to this point about Palestine.
Growing up in that church my Principal/Teacher/Pastor’s wife, yes she was all three, would talk about Israel. Talked about it so much that it came almost synonymous with America. I never once heard her or anyone talk about Palestine. In fact the only memory I have of Palestine is a video I saw on Instagram when I was about 17 years old. That little boy, maybe 13 or 15 years old also looked like his birthday, said on the mic “I give my life to Palestine.” And I thought “Palestine? What’s that?” I didn’t know what or who they were talking about so it went into the back of my mind. Never thought about it again.
Until October 7th, 2023, I was up late watching tiktok and I saw this picture with the Skyfall song by Adele playing. It showed a picture of the Iron Dome intercepting a missile. So immediately I go “Israel is under attack!” And I’ll be honest I didn’t care. Just another thing that didn’t matter in my life because I’m in Texas. A million miles away from the comfort of my home and warm bed, I could easily just swipe away or turn off. Until I saw the videos of Palestinian men, woman, and children.
I watched those videos and in my head I’m going “But they started it?” Because that’s what I was taught. “They’re Muslims trying to exterminate the Jews.” My thoughts echoing the words of my pastor, my teacher, my church, my dad. I’ll admit that a part of me was cheering for the Israel people, that I was condoning what was happening. I thought that Hamas was this powerful group and that Israel was weak because that’s what I was taught. Israel is this little country and defenseless, that’s what I was taught all my life. To pray for Israel’s peace and safety, that���s what I always did. It what I was taught to do.
The videos I saw though proved otherwise. Israel isn’t weak, Israel isn’t defenseless, Israel isn’t poor, Israel is… Israel is bombing civilians. Israel is bombing churches. Israel is bombing places that are supposed to be safe.
It’s like the wool was forcibly taken from my eyes. Like a person gripping my hair and making me look. At first I didn’t want to see. I was content in what I was taught. I was safe with not knowing. But I couldn’t do that anymore. I couldn’t just look and forget. I couldn’t. My turning point was my little brother, 13 years old and mind you hasn’t been raised in the church like I was. His worldview is his own because he was allowed to make his own views without the influence of the church. We were talking about it and this 13 year old kid starts talking about Palestine. And at first I was against it, at first I argued with him but he wasn’t backing down. And I thought “He’s caring about this so much. Why?”
So I read as much as I could on Palestine. I’ve been reading articles and watching videos. I’ve been trying to understand. It was hard, the hatred I had for Muslims and the love I had for Israel made it hard. I second guessed everything and tried to find the moment where I could go “Ah ha! See the Muslims and Palestine is lying!” But I couldn’t. I couldn’t find it.
My tiktok fyp was showing me videos of the men, woman, and children left and right. Again it was like the hand was gripping my hair and making me look. In time I didn’t fight it anymore. I stayed and I looked. Video after video, reel after reel, I watched. A silent witness until I couldn’t be silent anymore. I follow tiktok and Instagram accounts to keep up to date. I’m trying to cram as much knowledge in my head so I can speak out about this to my friends that I was raised with. To argue with my dad about this because he’s only parroting what his pastor is saying.
2 weeks I’ve been learning. 2 weeks I’ve been doing the bare minimum of educating myself on this.
Did you know that I thought Israel’s state was there for at least 200 years? Did you know that I had no idea about the open air prison of Gaza until 2 weeks ago? Did you know that I have been loyal to a state that didn’t even know my name only because I was raised to be loyal to them?
I’m ashamed. I’m ashamed of myself. I’m ashamed that I, who prides herself on learning history and facts did not know about Palestine. I’m ashamed that when I saw that video when I was 17 years old that I did not look into what Palestine is. I’m ashamed of my church. I’m ashamed of the state that I was so loyal to even though they wouldn’t even care about me. I’m ashamed that all I can do is speak and post.
But more than anything, I bare witness. I bare witness to the men, woman, and children that are suffering. I am their witness. I will speak out. I will post. I will comment. I will share. Because that is the very least that I can do.
To the Palestinians, I am so sorry that I hated you without even knowing you. That I saw you as Muslim and hated you because of it. I’m so sorry.
To the Muslims, I am so sorry that I hated you and your religion. I hated you without even thinking why? Without stopping and thinking why do I hate you when you’ve done nothing to me? I’m so sorry. I can never not be sorry.
I can never be sorry enough. I’m no saint. I’m no good person. But I will try to be good. I will try and do better. I will educate myself and help when I am able to. I will speak out. I will be another voice. Another shoulder to lean on. I’m sorry and I will do my part to help.
#palestine#free palestine#muslim#christianity#raisedchristian#figuring things out#speaking out#im sorry#palestinians#free gaza
8 notes
·
View notes
Note
What did Marty Scurll do?

Speaking Out Wiki Page
11 notes
·
View notes
Text
Psyche: Relationships (I) - Projection
Many of the traits we seek in others are, in fact, attributes within ourselves that we have disowned. Over time, it becomes apparent that the vitality or power we perceive to be residing in others is inherently within us. However, if our partner is unable or unwilling to relinquish that power, or if we continue to project our internal world onto them, true inner fulfillment may remain elusive.

Consider what you seek in a partner. Could these desirable traits be latent within you? The act of idealizing or deifying someone can spark the romantic phase of any relationship. Yet, once this period is over, the projection dissolves, revealing an unfiltered version of the person underneath. This can mark the beginning of substantial personal growth or the end of a relationship.
Projection is a constant element of human interaction, but awareness is the key to managing it. Relationships can serve as catalysts for spiritual advancement, yet such progression demands introspection and a commitment to change. This dynamic brings to light the conflict between the desires of the ego and the soul.
The ego seeks stability, comfort, and reliability, creating patterns of behavior that are meant to protect us. In order to perpetuate this, the ego casts a shadow of conflict and distress in the face of our soul with everything that runs contrary to its familiarity. These underlying issues are only made conscious through a deeper level of awareness that precedes and bears command over the ego.
To facilitate our development, the soul must expand to the extent which it can endure the discomfort of the ego while it pursues necessary transformation. This may involve difficult conversations and alterations in communication styles. In a relationship committed to growth, both individuals need the strength of their soul to tolerate the ego's distress, otherwise, interactions may devolve into conflicts driven by unresolved childhood issues.
Power struggles between partners often reflect unmet needs from their respective past. The real breakthrough happens when it becomes clear that the other person is not a projection of one's parents or anyone else. Achieving this understanding requires the ability of the soul to manage the ego's discomfort. If comfort and happiness are the sole pursuits, they will likely hinder the growth process within relationships committed to spiritual development, as this path often necessitates a certain level of discomfort.
While self-improvement is a significant component, it's also important to remember that self-deception can occur easily when one is left to their own devices. The dynamics of a relationship tend to reveal the issues we may avoid confronting within ourselves, especially when we have certain expectations. While setting standards for partners is vital, it's equally important to commit to embodying the qualities we aspire to find in others.
“So whenever your relationship is not working, whenever it brings out the "madness" in you and in your partner, be glad. What was unconscious is being brought up to the light. It is an opportunity for salvation. Every moment, hold the knowing of that moment, particularly of your inner state. If there is anger, know that there is anger. If there is jealousy, defensiveness, the urge to argue, the need to be right, an inner child demanding love and attention, or emotional pain of any kind whatever it is, know the reality of that moment and hold the knowing. The relationship then becomes your sadhana, your spiritual practice. If you observe unconscious behavior in your partner, hold it in the loving embrace of your knowing so that you won't react. Unconsciousness and knowing cannot coexist for long even if the knowing is only in the other person and not in the one who is acting out the unconsciousness. The energy form that lies behind hostility and attack finds the presence of love absolutely intolerable. If you react at all to your partner's unconsciousness, you become unconscious yourself. But if you then remember to know your reaction, nothing is lost... See if you can catch yourself complaining, in either speech or thought, about a situation you find yourself in, what other people do or say, your surroundings, your life situation, even the weather. To complain is always nonacceptance of what is. It invariably carries an unconscious negative charge. When you complain, you make yourself into a victim. When you speak out, you are in your power. So change the situation by taking action or by speaking out if necessary or possible; leave the situation or accept it. All else is madness.”
— Eckhart Tolle
#relationships#ego#soul#inner child#projections#blame#unconscious#cycles#patterns#acceptance#speaking out#change#boundaries#psychology#psyche
12 notes
·
View notes
Text
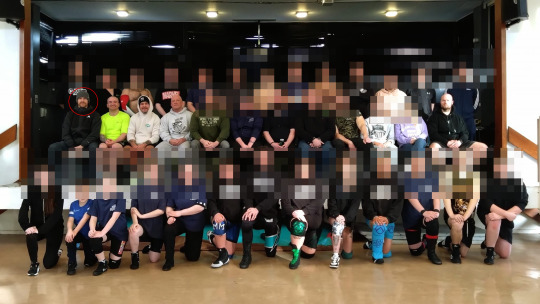
So i dont really know who else to tell this information but I would like it spread around as much as possible if you're going to wrestling shows here in Scotland, Kid Fite (the man circled) was named during speaking out for allegedly grooming a 16 year old and he's still working within the industry as seen here at the PBW training academy, i've blurred out everyone elses faces that isn't a wrestler (that i know of) but there are young women included in this.
I do know that he's still getting booking elsewhere here in Scotland, but the fact he's still "training" with younger people is absolutely fucking disgusting.
3 notes
·
View notes
Text
Years ago when i was preteen (young teen) i had a girl close a door on me in a room where there was only us, then walk towards me slightly mad. I walked back and my feet tripped on the bed so i fell back onto it sitting down. Then she sat on me continuing to be mad
I remember this vividly, and i was wondering what.... what the hell is it?
I didn't and still don't feel like its normal. I also don't think its important to mention i was really confused by the girl acting this way. She was the same age as me aswell.
Can anyone explain if this was ok? I feel like it wasn't but I'm confused about it
#please help#help#my experiences#life experiences#strange things#speaking out#talking about stuff#im serious
2 notes
·
View notes
Text
speaking out.
guys i find it rly hateful and offensive when i follow some of you coz we have like the same interests and stuff and yous don’t even follow me back like why aren’t you begging to be my mutual what happened to girls supporting girls this is rly rly aimed so from now on i’ll be blocking people who have the same interests as me coz it’s basically plagiarism idk
3 notes
·
View notes
Text
I'm sorry ahead of time, but apparently it's this kind of day, y'all 💀💀
SO
I just have to address this yet again, cause I really feel the strong need to today. I already said a few of my thoughts on this awhile ago, tacked onto someone else's post that I reblogged, but I'm just gonna talk about one specific moment.
I don't think this will be very long, but who knows
So, I wanna talk about a moment in the van scene between Will and Mike. Yes, yes, so much to unpack there. But more specifically, the moment when Will is crying and Mike turns to look at him for a moment before looking away.
I've heard so many things about this scene. But the most popular one, or at least the one that I come across the most, is that Mike knew that Will was crying and just purposely ignored him because he didn't care or because he's an asshole or whatever.
Guys, Will was facing the window when Mike turned to look at him. Mike saw the back of Will's head. Maybe he realized that Will was upset, but he had no idea what about, and Will was obviously trying to hide the fact that he was crying. IF Mike even realized that Will was crying, and that's a big if, he probably realized that Will didn't want anyone to know he was crying and decided he should leave Will alone.
I mean, personally, if I'm looking away from everyone else and trying to hide that I'm crying, then I'd prefer no one notice and start asking me questions about it. If I'm hiding something, I obviously don't want anyone else to know. That's the whole purpose of hiding something.
Will didn't know that Jonathan saw him crying, either. Jonathan knew but said nothing because he knew Will wouldn't want to be called out like that or have attention drawn to the fact that he was crying. Which, yes, some of you might point out that Jonathan also clearly knows exactly why Will was crying, and therefore, that's the real reason that he didn't point out Will crying. Soooo, what? Do any of you really believe that even if Jonathan didn't know why Will was crying, he still would've pointed it out? Just like, "Hey, Will, are you crying back there? What's up, buddy, are you okay?" In the middle of everything with both Argyle and Mike there to hear it? When Will clearly was trying to draw less attention to himself, not more? No, he wouldn't of done that. And Mike would've been the same way, had he known that Will was full on crying beside him.
Mike and Will are very different in a lot of ways. Where Mike is very outspoken and open, Will is very quiet and private. So while Mike is okay having that conversation about himself and his and El's relationship where other people can also hear, if the situation were flipped, Will would prefer to keep things a lot quieter, a lot more secluded, because he's not someone who's as okay with outsiders in the same area hearing a private conversation as Mike would be. Will hides things and prefers to keep a lot of things to himself, and Mike, being Will's best friend of nearly a decade, would know that. And Jonathan, having known Will all of Will's life, would also know that.
So, even if Mike realized that Will was crying, he wasn't ignoring Will because he didn't care. It was actually the opposite. He was allowing Will to have that moment by himself, just as Will would've preferred to. If it was up to Will, he'd be in a room by himself while he was crying, not in a van with 3 other people around.
So please, stop hating on Mike for that scene. He probably didn't realize that Will was crying and even if he did, he would've just wanted to give Will some privacy, as much as possible in their situation at the time. Mike doesn't deserve all of the hate he gets, guys. He's literally just being a 15 year old boy, living his life the best he can with everything that goes on in it. And again, I remind you all. You can't get mad at Mike for not noticing things that Will is actively trying to hide. It means that Will is successful in what he's trying to do, therefore, he wants it that way.
Anyways, that's the end of this post guys, thanking you for reading through all these thoughts in my head if you made it all the way here, I tried to make it all as understandable as it was in my head. Have a good day/night, y'all <3
#speaking out#cause these thoughts needed an outlet#sorry not sorry#it frustrates me down to my very core#leave mike alone#he's a sweet little beanpole that needs to be protected#mike wheeler protection squad#mike wheeler#will byers#st van#st v2 spoilers#st vol 2#stranger things#stranger things 4#st 4#stranger things volume 2#stranger things van scene#purple_strxnger#scene analysis#character analysis#st 4x08#stranger things 4x08#stranger things spoilers#stranger things 4 volume 2#stranger things 4 spoilers#st4 volume 2
24 notes
·
View notes
Text
Is it just me, or have those damn bots/porn blogs been recently going crazy (again)?
I'm so annoyed ... 😠
2 notes
·
View notes
Text
My Gift To Myself
So, on my 60th Birthday yesterday I gave myself a gift. I gave myself permission to stop enabling people, feeling sorry for them, caring for them, feeling as if I should accept their behaviours.
I had a fabulous birthday. RD made it so special. People at work sent so many lovely messages before I left work. Friends messaged me on my birthday eve, RD brought flowers, gifts. Love. Lovely…

View On WordPress
4 notes
·
View notes
Text
I am posting to vent really.. I feel as though I am stuck in this loop. I’ve worked 7 days a week for the past 3 months straight minus a week for getting the cold. And it’s really messing with my mental health. At first I thought I could handle it.. I was making some more money, I was active every day.. I thought it was making me more productive.
The other is a stable reliable job in the medical field, which I never wanted to be in. One that drains me the second I enter the door. One that is extremely stressful because, while it’s stable and the spot is secure and easy to get to, it pays way less. I’m a pharmacy technician with no schooling background or prior medical knowledge in a low income area. Someone’s always screaming and crying. We are constantly denying ppl there meds because of insurance issues and it’s just mentally a lot on my soul. Not to mention i dam near break down everytime someone asks me an array of questions I don’t know the answer to even after working here for 7months. Rightfully so since pharma n POC don’t have the most trusting relationship. They look at me and think they can trust me, which they can I try my best to fully assist anyone and use every method to help even ones my coworkers would “overlook”. But It’s a lot. I know nothing about pharmacology. I barely took Tylenol before this job. I thought it would be a good stable job to signify that I was finally getting my life in order, dropped the arts, which I love and got a “respectable” profession.
They said I didn’t need any prior knowledge and I’d pick it up as I go.. the only thing I know how to do by heart is fill pill bottles. And even then.. I can’t pronounce half of the pills. Someone ask me a question I have to tell them to hold on and ask someone else…. And they always side eye me. Like somehow I, who was hired with no prior knowledge at all.. should know things they did after years of schooling. If I had a headache I drank tea, I’m Caribbean🤣 I didn’t go buying 3 types of pain killers it’s not “common knowledge” to me. In any case I feel like I need to drop one. I’m so tired now. Bags under my eyes, skin a mess.. I have more money I suppose but not enough to keep running myself into the ground. I have no time for doc appts , hair appts , spend time with family or friends. Do any hobbies, I just sleep. I don’t eat properly anymore I just eat whatever is closest outside..lately I’ve felt the urge to randomly bursted into tears having to go to bathrooms to pull myself together.. I force and drag myself up every morning but especially to the medical job. & no I got no kids. I live with my disabled mother. I know I need to make a change.. But I’m not sure what to do. I don’t want to make the wrong decision & end up without a job. The first one is so finicky they could tell me that it’s not working out tomorrow and that would be it. The medical one is unionized. But tbh I suck at my job.I wanted to go back to school, but it’s been so long since I’ve dreamed of something to do that wasn’t just to survive...
In any case.. I feel like maybe I just stick with the pharmacy because it stable. I am looking for other jobs but there isn’t much luck. I still apply everyday to at least 5. My friends & family say follow my heart and care for my mind. But I don’t want to be the only person in my circle without an “adult” job. Or in school. I don’t want to be end up the broke or liability person, I don’t want to burden those around me, I don’t want to be 25 in my moms home still lost on where to start. I had a rough childhood, abuse of many kinds etc. I never thought I’d make it to 25.. now I’m here I’m grateful.. I just want to be able to take care of myself financially and also have time to care for myself in other ways, then care for my family. So.. yeah this is the first time in months I’ve said a word about how overwhelmed I feel. Sorry if it’s a lot or sounds like it’s not that deep.. it is to me.
And thanks for having a space I can release.
#mentalheathawareness#mental health#mentally tired#healing#indecisive#freedom#mentally drained#mentalwellness#today drained me#vent#vent post#advice#expore#releases#baggage#speaking out#understanding#love language#peace#inner thoughts#inner peace
2 notes
·
View notes
Last Seen Blogs


johnkatsmc5
return to the underground,the other side of music

luke-scavuzzo88
Luke Scavuzzo

brotmehipajaro90
brotmehi

lefufacodejo
Untitled